Assessment of radiolucent lines around the Oxford
advertisement

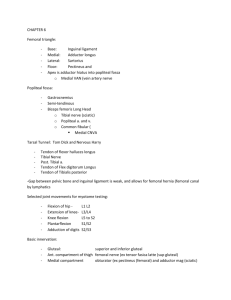
KNEE Assessment of radiolucent lines around the Oxford unicompartmental knee replacement SENSITIVITY AND SPECIFICITY FOR LOOSENING S. Kalra, T. O. Smith, B. Berko, N. P. Walton From Norfolk and Norwich University Hospital Trust, Norwich, England S. Kalra, MA, MBChB, FRCS(Tr&Orth), Specialist Registrar B. Berko, MBChB, Research Fellow N. P. Walton, FRCS(Tr&Orth), Consultant Orthopaedic Surgeon Norfolk and Norwich University Hospital, Colney Lane, Norwich NR4 7UY, UK. T. O. Smith, MSc, BSc(Hons), MCSP, University Lecturer Faculty of Medicine and Health Sciences University of East Anglia, Norwich NR4 7TJ, UK. Correspondence should be sent to Mr S. Kalra; e-mail: sanjaykalra20@gmail.com ©2011 British Editorial Society of Bone and Joint Surgery doi:10.1302/0301-620X.93B6. 26062 $2.00 J Bone Joint Surg [Br] 2011;93-B:777-81. Received 14 October 2010; Accepted after revision 4 February 2011 VOL. 93-B, No. 6, JUNE 2011 The Oxford unicompartmental knee replacement gives good results in patients with symptomatic osteoarthritis of the medial compartment. Previous studies have suggested that the presence of radiolucent lines (RLLs) does not reflect a poor outcome in such patients. However, the reliability and validity of this assessment have not been determined. Our aim was to assess the intra- and interobserver reliability and the sensitivity and specificity of the assessment of RLLs around both tibial and femoral components using standard radiographs. Two reviewers assessed the radiographs of 45 patients who had loosening of the tibial or femoral component confirmed at revision surgery and compared them with those of a series of 45 asymptomatic patients matched for age and gender. The results suggested that, using standard radiographs, tibial RLLs were 63.6% sensitive and 94.4% specific and femoral RLLs 63.9% sensitive and 72.7% specific for loosening. Overall intra- and interobserver reliability was highly variable, but zonal analysis showed that lucency at the tip of the femoral peg was significantly associated with loosening of the femoral component. Fluoroscopically guided radiographs may improve the zonal reliability of the assessment of RLLs, but further independent and comparative studies are required. In the meantime, the innocence of the physiological RLLs detected by standard radiographs should be viewed with caution. The Oxford medial phase-3 unicompartmental knee replacement (UKR; Biomet, Swindon, United Kingdom) comprises a keeled tibial tray with a flat upper surface and a pegged spherical femoral component. It uses an unconstrained mobile bearing which is congruent with the femoral component throughout the range of movement. Both tibial and femoral components are cemented. The implant has been advocated for use in painful isolated anteromedial osteoarthritis1 with an intact anterior cruciate ligament and correctable varus deformity (< 15°).2 The Oxford group have recently reported good results at a mean of 5.6 years for 1000 UKRs.3 Peri-prosthetic radiolucent lines (RLLs) after joint replacement surgery are usually considered to be indicative or predictive of loosening of the component. The presence of RLLs associated with the Oxford medial UKR is well documented, but their aetiology and significance are poorly understood. In 1984, Tibrewal, Grant and Goodfellow4 reported an incidence of tibial radiolucency of 96% in 80 phase-1 UKRs at one year. In 2006, Pandit et al5 described an incidence of 70% in 688 phase-3 UKRs at five years. Despite these radiological abnormalities, other series have shown a good survival and clinical outcome at ten and 20 years.6-11 Goodfellow et al2 subdivided tibial RLLs into two subtypes: physiological and pathological. Physiological RLLs were classified as those < 2 mm thick, well defined, with an accompanying parallel radiodense line. By contrast, pathological RLLs were > 2 mm thick, poorly defined, and not accompanied by radiodensity. Gulati et al12 reported an incidence of 62% of physiological RLLs around the tibial component and concluded that the presence of these lines was neither related to symptoms nor indicative or predictive of loosening. We are unaware of any previous studies which have investigated RLLs around the femoral component. The incidence, distribution and significance of these remain unknown. Recently, a much lower incidence of RLLs has been reported with the cementless Oxford medial UKR,13 which is thought to represent 777 778 S. KALRA, T. O. SMITH, B. BERKO, N. P. WALTON bone incorporation within the prosthesis. While several hypotheses have been proposed to explain the RLLs observed with the cemented prosthesis,4 the favoured theory is formation of a layer of fibrocartilage as a result of the compressive loading which occurs under the tibial plateau.14 The importance of fluoroscopically guided radiographs in the assessment of the tibial component has been emphasised in numerous studies,4,12,15 but their accuracy and validity, both alone and in comparison with standard radiographs, has never been formally investigated. No independent group has yet investigated the radiological assessment of the Oxford UKR. Consequently, it is unclear whether the use of fluoroscopically guided radiographs is common practice and their general adoption for the assessment of tibial RLLs in UKR is debatable. Fluoroscopically guided radiographs are not recommended for assessment of the femoral component. Our aim therefore was to evaluate two issues related to the radiological assessment of UKR. We wished firstly to determine how common is the use of fluoroscopically guided radiographs in joint replacement centres for assessing UKR and secondly, to evaluate the reliability, sensitivity and specificity of tibial and femoral RLLs using standard radiographs. Patients and Methods National survey. We carried out a telephone survey of all acute hospital trusts in the NHS which have an orthopaedic department, in order to determine how often they use fluoroscopically guided radiographs. The NHS website was accessed to identify all 110 eligible hospitals. Each hospital’s Superintendent Radiographer (or equivalent) was contacted through the hospital switchboard and was asked about local protocols for the post-operative radiological assessment of patients with UKR. In addition, they were directly questioned about the use of fluoroscopically guided radiographs in this group of patients. Radiological assessment. Our study was carried out in a University Teaching Hospital with a prospective database which included over 1200 operations performed over the last 12 years using the Oxford UKRs, mostly by a single surgeon. Since 2000, 949 phase-3 UKRs had been logged. For each, the database included the clinical outcome score, range of movement and complications. The incidence of revision surgery was also recorded including the intra-operative findings in each case. In total, 92 patients (9.7%) required revision surgery. Table I summarises the reasons for revision. In our study, our revision series included only those 45 cases in which loosening of either the tibial or femoral component had been confirmed intra-operatively. We identified 90 patients who had an Oxford phase-3 UKR performed between January 1, 2000 and December 1, 2008. Of these, 45 had required revision because of sus- Table I. Reasons for revision surgery in the 92 revisions of 949 Oxford phase-3 procedures. Only those 45 with loosening of a component were included into our revision series Reason Number of cases Femoral loosening Tibial loosening Bearing dislocation Unexplained pain Progression of lateral disease Fracture Infection Total 35 10 14 10 10 8 5 92 pected loosening which had subsequently been confirmed at revision and in whom details of the loose component were recorded (Table I). As Table II shows, these patients were approximately matched by age, gender and knee with 45 patients who had a UKR performed with an uncomplicated follow-up and who did not require revision. The clinical details of both groups are presented in Table II. There were 43 men and 47 women with a mean age of 69.5 years (51 to 91) at the time of radiological examination. In the revision series, ten patients had revision for loosening of the tibial component and 35 for loosening of the femoral component as determined intraoperatively. The radiographs of the revision group were the last taken before revision, at a mean follow-up of 26.8 months (3 to 90). Those of the non-revision group were approximately matched for period of follow-up (26.2 months (1 to 71)). All radiographs were reviewed by two assessors (SK, BB) who were blinded as to whether the patient had or had not undergone revision for loosening after the radiographs were taken. By this means it was possible to assess the sensitivity and specificity of each RLL measurement without assessor bias affecting the results. Both assessors had read the previous literature regarding RLL subtypes and the assessment of tibial RLLs.12 Both the tibial and femoral components were assessed for each patient by each assessor. One assessor (SK) then repeated his review of both the tibial and femoral implants after a period of three months. All the radiographs were reviewed on the institute’s Picture Archiving and Communication System and digitally measured. Tibial RLLs were assessed using the same zonal method described previously by Gulati et al12 (Fig. 1a). On anteroposterior (AP) view, the tibial component was divided into six zones. Each zone was assessed for the presence of RLLs and the subtype recorded. For femoral RLLs, we developed a system of dividing the lateral cross-table view of the femoral component into six zones (Fig. 1b). Each zone was assessed for the presence of RLLs and the subtype recorded. THE JOURNAL OF BONE AND JOINT SURGERY ASSESSMENT OF RADIOLUCENT LINES AROUND THE OXFORD UNICOMPARTMENTAL KNEE REPLACEMENT 779 Fig. 1b Fig. 1a The zonal assessment for radiolucent lines. Figure 1a – anteroposterior radiograph showing the six zones of the tibial component originally described by Gulati et al.12 Figure 1b – lateral cross-table radiograph showing the six zones of the femoral component. Table II. Details of the 90 patients included in our series Revision (n = 45) Non-revision (n = 45) Total (n = 90) Male (%) Female (%) Mean age (range) at radiography in years 23 (51.1) 20 (44.4) 22 (48.9) 25 (55.6) 69.6 (52 to 91) 69.3 (51 to 84) 43 (47.8) 47 (52.2) 69.5 (51 to 91) Side (%) Left Right 18 (40.0) 27 (60.0) 36 (40.0) 54 (60.0) Frequency of intra-operative tibial loosening (%) 10 (22.2) Frequency of intra-operative femoral loosening (%) 35 (77.8) The non-revision series had a mean Oxford knee score16 of 30 (19 to 47) and a mean SF-1217 score of 38 (18 to 60) at the time of the radiological examination. Statistical analysis. The clinical details including gender, side of implant, age at radiological examination, and frequency of tibial or femoral loosening were assessed using descriptive statistics consisting of mean, range values and frequences reported as percentages. An assessment of the difference in the frequency of occurrence of physiological and pathological RLLs was compared between the revision and non-revision series at each RLL zone using Fisher’s exact test, and for all zones using the chi-squared test. This was carried out for both tibial and femoral implants in both the revision and nonrevision series. A p-value < 0.05 was considered to be statistically significant The sensitivity and specificity of the femoral and tibial RLL assessments were also made as described by Bland.18 Interobserver reliability was assessed by comparing the femoral and tibial RLL assessments between the two assessors and intra-observer reliability by the assessments of one assessor on two separate occasions. These were VOL. 93-B, No. 6, JUNE 2011 18 (40.0) 27 (60.0) 10 (11.1) 35 (38.9) calculated using a weighted kappa analysis,19 and interpreted using the agreement recommendations of Landis and Koch.20 Results National survey. Of the 110 eligible hospitals, 109 were contacted. The Nuffield Orthopaedic Centre, Oxford, was not contacted since it had previously reported the fact that it used fluoroscopically guided radiographs.12 The senior radiographer from each of the remaining 109 stated that the hospital used standard weight-bearing AP and crosstable lateral radiographs in the follow-up of UKR. None reported the use of fluoroscopic guidance. Radiological assessment Comparison of tibial radiolucency. There was a greater frequency of pathological tibial lucency in the non-revision compared with the revision group (Table III). However, this was not statistically significant either overall (p =0.37) or when individual zones were compared (between p = 0.62 and p = 0.79 for the six zones, Fisher’s exact test). There was a higher incidence of tibial physiological lucency in the revision compared with the non-revision 780 S. KALRA, T. O. SMITH, B. BERKO, N. P. WALTON Table III. Radiological assessment of pathological tibial lucency Radiolucent zone Revision Non-revision p-value* 1 2 3 4 5 6 Total 3 6 4 5 5 5 28 19 17 17 4 10 9 76 0.79 0.70 0.79 0.73 0.73 0.62 0.37† * p-value calculated by Fisher’s exact test unless otherwise stated † chi-squared test Table IV. Radiological assessment of physiological tibial lucency Radiolucent zone Revision Non-revision p-value* 1 2 3 4 5 6 Total 15 9 2 2 1 3 32 8 5 3 2 3 2 23 0.98 0.54 0.59 0.66 0.64 0.76 0.52† * p-value calculated by Fisher’s exact test unless otherwise stated † chi-squared test Table V. Radiological assessment of pathological femoral lucency Radiolucent zone Revision Non-revision p-value* 1 2 3 4 5 6 Total 7 9 7 9 6 12 50 3 3 0 2 2 6 16 0.35 0.22 0.65 0.58 0.48 0.10 0.69† * p-value calculated by Fisher’s exact test unless otherwise stated † chi-squared test Table VI. Radiological assessment of physiological femoral lucency Radiolucent zone Revision Non-revision p-value* 1 2 3 4 5 6 Total 8 15 10 14 8 20 75 4 6 2 7 7 12 38 0.38 0.34 0.03 0.08 0.90 0.55 0.01† * p-value calculated by Fisher’s exact test unless otherwise stated † chi-squared test group (Table IV). However, there was no significant difference in the frequency of physiological lucency between the revision and non-revision groups either overall (p = 0.52) or in individual zones (p = 0.54 to p = 0.98, Fisher’s exact test). Comparison of femoral radiolucency. There was a greater frequency of pathological lucency in the revision compared with the non-revision group for each femoral zone (Table V). Statistical analysis showed that this trend was not significant between the revision and non-revision series either overall (p = 0.69) or for individual zones (p = 0.10 to p = 0.65, Fisher’s exact test). Table VI shows that while there was a greater number of physiological femoral RLLs in the revised compared with non-revised patients, this difference was not significantly different for zones 1, 2, 4, 5 and 6 (p = 0.08 to p = 0.90, Fisher’s exact test). However, there was a statistically significant difference between the groups in detecting RLLs in femoral zone 3 (p = 0.03, Fisher’s exact test) as well as an overall difference between the revision and non-revision groups (p = 0.01, chi-squared test). Diagnostic accuracy. The sensitivity and specificity of the tibial RLLs for detecting loosening of the component were 63.6% and 94.4%, respectively. The femoral RLLs were 63.9% sensitive and 72.7% specific. The results of the interobserver reliability indicated that the assessment of tibial pathological loosening ranged from fair to substantial agreement between the two reviewers. However, the interobserver reliability was, at best, moderate for femoral pathological RLLs indicating that this method of assessing RLLs may vary between assessors. Similarly, the assessment of intra-observer reliability indicated poor to good agreement between radiological assessments for both tibial and femoral components suggesting a lack of consistency between the first and second time that they were studied by the same assessor. Discussion Our findings indicate that while the sensitivity and specificity of RLLs using standard radiographs appear to be acceptable, their intra- and interobserver reliability is poor. Although the Oxford group have suggested that RLLs should be assessed using fluoroscopically guided radiographs,12 the national survey conducted in our study has indicated that this is not routine practice in the United Kingdom. Instead, standard non-fluoroscopically guided radiographs are generally obtained. Our findings agreed with those of previous studies reporting a high incidence of RLLs around the tibial component of the Oxford UKR.4,5,12 We have also shown a high incidence of RLLs around the femoral component. The aetiology of these is unknown and their reported lack of significance in predicting or indicating loosening of the components remains unexplained.4,12 We acknowledge that our small sample size may have been insufficient to detect a statistically significant radiological difference between those components which were found to be loose at revision and those which were not, except in femoral zone 3 (at the tip of the peg of the femoral component). However, physiological RLLs were present in greater numbers in the revision group, thereby bringing their lack of significance into question, as suggested by Gulati et al.12 Conversely, pathological RLLs were also present in large numbers in the non-revision THE JOURNAL OF BONE AND JOINT SURGERY ASSESSMENT OF RADIOLUCENT LINES AROUND THE OXFORD UNICOMPARTMENTAL KNEE REPLACEMENT group, although the difference in incidence was not statistically significant (p = 0.05). The difference shown in femoral zone 3 may be a representation of the pistoning phenomenon which has been described in a knee with a loose femoral component during flexion and extension of the knee.21 Lucency in this area may represent a genuinely loose component according to our results. Therefore we recommend that particular attention should be paid to femoral zone 3 when reviewing radiographs. Our results suggest that it is difficult to distinguish between physiological and pathological RLLs around both tibial and femoral components using standard radiographs. With respect to the tibial component, this may be because their characteristic features are obscured by a non-parallel x-ray beam, thereby causing RLLs to be missed unless fluoroscopic control is used, as suggested by the Oxford group.12 By contrast, the geometry of the femoral component may prevent the acquisition of a good view of the interface even if the x-ray beam is parallel. The Oxford group have reported an inter- and intra-observer correlation of more than 0.98 for physiological tibial RLLs when using fluoroscopically guided radiographs.12 It therefore follows that fluoroscopically guided radiographs may improve the agreement between assessors and therefore make it easier to distinguish between pathological and physiological RLLs, increasing the reliability of diagnosis and the monitoring of progression of loosening. When standard radiographs are used, which is standard procedure in most hospitals, a RLL around the femoral peg is likely to represent loosening of the femoral component. Further studies are required to evaluate the role of fluoroscopically guided radiographs in distinguishing between physiological and pathological RLLs, as are comparative studies to show a clear improvement in the assessment of UKR between fluoroscopically guided and standard radiographs. Listen live Listen to the abstract of this article at www.jbjs.org.uk/interactive/audio Supplementary material A table detailing the intra- and interobserver reliability of the assessment of radiological pathological loosening of each zone of the femoral and tibial components is available with the electronic version of this article on our website at www.jbjs.org.uk VOL. 93-B, No. 6, JUNE 2011 781 The authors would like to thank Mr M. Glasgow, as the surgeon who performed most of the operations. No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. References 1. White SH, Ludkowski PF, Goodfellow JW. Anteromedial osteoarthritis of the knee. J Bone Joint Surg [Br] 1991;73-B:582-6. 2. Goodfellow JW, O’Connor JJ, Dodd CA, Murray DW. Unicompartmental arthroplasty with the Oxford knee. Oxford: Oxford University Press, 2006:117-28. 3. Pandit H, Jenkins C, Gill HS, et al. Minimally invasive Oxford phase 3 unicompartmental knee replacement: results of 1000 cases. J Bone Joint Surg [Br] 2011;93B:198-204. 4. Tibrewal SB, Grant KA, Goodfellow JW. The radiolucent line beneath the tibial components of the Oxford meniscal knee. J Bone Joint Surg [Br] 1984;66-B:523-8. 5. Pandit H, Jenkins C, Barker K, Dodd CA, Murray DW. The Oxford medial unicompartmental knee replacement using a minimally-invasive approach. J Bone Joint Surg [Br] 2006;88-B:54-60. 6. Murray DW, Goodfellow JW, O’Connor JJ. The Oxford medial unicompartmental arthroplasty: a ten-year survival study. J Bone Joint Surg [Br] 1998;80-B:983-9. 7. Svärd UC, Price AJ. Oxford medial unicompartmental knee arthroplasty: a survival analysis of an independent series. J Bone Joint Surg [Br] 2001;83-B:191-4. 8. Price AJ, Short A, Kellett C, et al. Ten-year in vivo wear measurement of a fully congruent mobile bearing unicompartmental knee arthroplasty. J Bone Joint Surg [Br] 2005;87-B:1493-7. 9. Emerson RH Jr, Higgins LL. Unicompartmental knee arthroplasty with the Oxford prosthesis in patients with medial compartment arthritis. J Bone Joint Surg [Am] 2008;90-A:118-22. 10. Price AJ, Dodd CA, Svärd UG, Murray DW. Oxford medial unicompartmental knee arthroplasty in patients younger and older than 60 years of age. J Bone Joint Surg [Br] 2005;87-B:1488-92. 11. Price AJ, Waite JC, Svard U. Long-term clinical results of the medial Oxford unicompartmental knee arthroplasty. Clin Orthop 2005;435:171-80. 12. Gulati A, Chau R, Pandit HG, et al. The incidence of physiological radiolucency following Oxford unicompartmental knee replacement and its relationship to outcome. J Bone Joint Surg [Br] 2009;91-B:896-902. 13. Pandit H, Jenkins C, Beard DJ, et al. Cementless Oxford unicompartmental knee replacement shows reduced radiolucency at one year. J Bone Joint Surg [Br] 2009;91B:185-9. 14. Simpson DJ, Price AJ, Gulati A, Murray DW, Gill HS. Elevated proximal tibial strains following unicompartmental knee replacement: a possible cause of pain. Med Eng Phys 2009;31:752-7. 15. Mukherjee K, Pandit H, Dodd CA, Ostlere S, Murray DW. The Oxford unicompartmental knee arthroplasty: a radiological perspective. Clin Radiol 2008;63:116976. 16. Dawson J, Fitzpatrick R, Murray D, Carr A. Questionnaire on the perceptions of patients about total knee replacement. J Bone Joint Surg [Br] 1988;80-B:63-9. 17. Ware J Jr, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996;34:22033. 18. Bland M. An introduction to medical statistics. Third ed. London: Oxford University Press, 2006:275-9. 19. Altman DG. Practical statistics for medical research. London: Chapman & Hall, 1991:403-9. 20. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;33:159-74. 21. Monk AP, Keys GW, Murray DW. Loosening of the femoral component after unicompartmental knee replacement. J Bone Joint Surg [Br] 2009;91-B:405-8.