Full text - Learnblock
advertisement

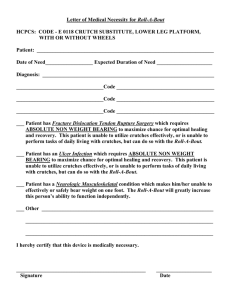
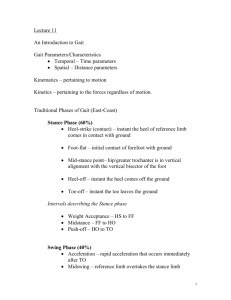
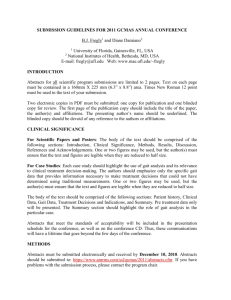
Chirurgia Narządów Ruchu i Ortopedia Polska, 76(5), 305-312, 2011 Three point crutch gait from the perspective of biomechanics and kinesiology. State of knowledge and idea behind the research Lechosław B. Dworak 1,2,3, Michał Murawa 1, Marek Owsian 2, Jacek Mączyński 1, Jarosław Kabaciński 1, Agata Rzepnicka 1 1 Department of Biomechanics, University School of Physical Education in Poznan 2 3 Department of Bionics, University of Arts in Poznań, Faculty of Physiotherapy, Poznan University of Medical Sciences Summary The study characterizes the idea behind the research project which consists in biomechanical and kinesiological analysis of three point crutch gait. The structure of the study is in part similar to an earlier publication of the authors [1], which discussed swing through gait. By defining the three point crutch gait and describing its general kinematic structure as well as synthetically analyzing the state of knowledge, the authors formulated the purpose of the study, the adopted research model – including the description of the modern and integrated measurement systems that were used and which consisted of: 2 AMTI force plates integrated into a measurement walkway, a set of 6 optoelectronic cameras of the BTS System as well as a multichannel kinesiological electromyography performed with the use of the NORAXON System. All phases of the research were characterized, presenting the adopted research protocol in its entirety. Key words: three point crutch gait, biomechanics, kinesiology, kinematic structure, conception and research model Chód trójpunktowy o kulach z perspektywy biomechaniki i kinezjologii. Stan wiedzy i koncepcja badań Streszczenie W pracy scharakteryzowano koncepcję projektu badawczego ukierunkowanego na biomechaniczną i kinezjologiczną analizę chodu trójpunktowego o kulach (three point crutch gait). Struktura pracy jest częściowo podobna do wcześniejszej publikacji autorów [1], odnoszącej się jednak do chodu kangurowego (swing through gait). Poprzez, definicję i ogólną strukturę kinematyczną chodu trójpunktowego o kulach oraz syntetyczną analizę stanu wiedzy, sformułowano cele pracy, przyjętą metodykę badań – w tym opis zastosowanych nowoczesnych i zintegrowanych torów pomiarowych, które składały się z: 2 platform dynamometrycznych AMTI wbudowanych w pomost pomiarowy, zestawu 6 kamer optoelektronicznych Systemu BTS, wielokanałowej elektromiografii kinezjologicznej z użyciem Telemetrycznego Systemu NORAXON. Scharakteryzowano także wszystkie etapy badań laboratoryjnych, ukazując całościowo przyjęty protokół pomiarowy. Słowa kluczowe: chód trójpunktowy, biomechanika, kinezjologia, struktura kinematyczna, koncepcja i model badań Problem formulation The genesis of interest in biomechanical, kinesiological and ergonomic aspects of crutch gait is related to several previous works of this paper’s author team [2-7], inspired among others by lectures given to physiotherapy as well as architecture and design students. It is, however, particularly related to two research projects of the Polish Ministry of Science and Higher Education (No N N404 1973 33 and No N N404 2715 40), realized in form of supervisor’s grants: Biomechanical analysis of three-point crutch gait in patients after lower limb injuries [8], Biomechanical and kinesiological analysis of swing-through gait in patients after lower limb injuries [9]. Crutch gait may be defined as a form of overland cyclical limb locomotion characterized by the fact that the supporting and propelling phases do not only occur during support with lower limbs (limb) but also with upper limbs holding mobility aids [1]. This paper discusses one of the types of crutch gait – the three point crutch gait. In Dega and Senger’s systematics of gait [10], it is categorized in the group of two-dimensional gaits. Three point crutch gait is one of the most frequently used crutch gaits. It is recommended because of symmetrical movement of crutches during the swing and stance phases, which is easy to learn as far as coordination is concerned. It is characterized by the possibility to partly (significantly) relieve weight bearing from the diseased lower limb [11-17]. Three point crutch gait: kinematic description from the perspective of biomechanics and kinesiology In their attempt to characterize biomechanically and kinesiologically three point crutch gait, the authors used widely accepted criteria for describing the kinematics and kinetics of locomotion movements, applying them to gait cycle and its phases [18-21]. Three point crutch gait is divided into two phases, both for the diseased limb and the crutches: stance and swing. Electronic PDF security powered by ISL-science.com 306 L. B. Dworak et al. Fig. 1. Schematic diagram of three point crutch gait cycle kinematics. Adaptation and modification on the basis of www.walkeasy.com. Ryc. 1. Schemat kinematyki cyklu chodu trójpunktowego o kulach. Adaptacja i modyfikacja na podstawie www.walkeasy.com. Assumptions The following assumptions have been made in order to define the biokinematic structure of three point crutch gait: 1. One lower limb is diseased (D) and requires support (in our case it will be the left limb; Fig. 1 and Fig. 2); 3. The swing phases of crutches and the diseased limb are performed with pendular motion, simultaneously (symmetry in time); 4. The patient moves with alternating step, crossing the front line of the supporting foot. According to this convention, three point crutch gait cycle begins and ends with the first contact of the diseased limb foot and crutches with the ground (Fig. 1). Descriptive kinematic structure of correct three point crutch gait cycle 1. The stance phase of the diseased limb and crutches (stance phase, StPh) It begins with the first contact of the diseased limb foot and crutches with the ground (initial contact, IC) and ends the moment this limb and crutches loose contact with ground (initial swing). It is divided into 3 microphases characteristic to the movement sequence of the body. 1.1. Shifting body weight onto the diseased limb foot and crutches (loading response, LR). Fig. 2. Sequence of characteristic foot and crutch positions during the cycle phases of three point crutch gait. Assumption: left limb diseased (D), right limb healthy (H). Grey and black colors signify part and full load on the limb respectively. Symbols " and ! represent the positions of crutches during stance (loaded) and swing phases respectively. Arrows placed on the projections of feet of D and H limb represent the swing phases of these limbs. Ryc. 2. Sekwencje charakterystycznych położeń stóp i kul w fazach cyklu chodu trójpunktowego o kulach. Założenie: lewa kończyna chora (D), prawa zdrowa (H). Barwa szara lub czerń oznaczają odpowiednio częściowe lub pełne obciążenie kończyny. Symbole " i ! oznaczają kolejno położenie kul w fazach podporowych (obciążenia) i wymachowych. Strzałki umieszczone w rzutach stóp kończyny D i H oznaczają fazy wymachowe tych kończyn. 2. The stance phases of the diseased limb and crutches happen simultaneously (symmetry in time) and as a result one achieves the unweighting of this limb; Its main qualities are simultaneous loading of crutches with patient's body mass and reduction of load on the diseased limb, related to shifting the COM forward from rear position. It is characterized by 4 points of support (both crutches and both feet are in contact with ground). In this sense it is a phase of double support of lower limbs as well as lower limbs and crutches (double support, DS). The equivalent of this in figure 2 are sequences 1 and 2. 1.2. Mid stance (MS). It can be distinguished by the loading of crutches with patient’s body mass and reduction of the load on the diseased limb. It is characterized by 3 points of support (three point crutch gait), as both crutches and the diseased limb foot are in contact with ground, because the healthy limb begins and continues its forward swing phase. The name of the three point crutch gait is derived from this characteristic locomotion sequence. Electronic PDF security powered by ISL-science.com Three point crutch gait biomechanics and kinesiology 1.3. Terminal stance (TS) It can be distinguished by increased loading of the diseased limb, in preparation for the swing phase that follows it, and by generation of COM propelling forces during the stance phase. 2. The swing phase of the diseased limb and crutches (SwPh) It begins when the diseased limb foot and crutches loose contact with the ground (simultaneously), and ends the moment the diseased limb foot and crutches enter in contact with ground. Similarly to the stance phase, it divides into 3 microphases. 2.1. Initial swing (IS) It is marked by the moment the diseased limb foot and crutches loose contact with ground initiating their symmetrical swing (diseased limb and crutches). In the supporting sense, during this microphase the body has only 1 point of support (healthy limb foot is loaded). 2.2. Mid swing (MS) It is characterized by symmetrical forward transfer of the diseased limb and crutches with pendular motion in the mid zone of this microphase. Analogically to the previous microphase, this sequence has only 1 point of support (healthy limb foot). 2.3. Terminal swing (TS) It begins when the swing of the diseased limb and crutches is beginning to stop, and ends, as in the beginning of the cycle, with the first contact of the diseased limb foot and crutches with ground (initial contact, IC). Similarly to the two previous swing microphases, this sequence also incorporates only 1 point of support (healthy limb foot). Critical analysis of the state of knowledge – synthetic perspective In their attempt to analyze the few available publications on three point crutch gait, the authors concentrated on those which present the problem from the perspective of biomechanics and kinesiology. The issue of grading the weight-bearing on the diseased lower limb and teaching patients to relieve weight-bearing as recommended (by a physician or physiotherapist) during locomotion with three point crutch gait was addressed by such researchers (and their associates) as Gray, Li, Tveit, Woolson, Hurkmans, Malviya, Youdas, Nowotny-Czupryna, Vasarhelyi, Eng, Hol [13, 22-31]. Li et al. [13], in their study of three point crutch gait addressed the variability of dynamic (in the values of 307 ground reaction force) and kinematic parameters. The experimental group consisted of 12 healthy persons whose task was to simulate (on a measurement walkway) three point crutch gait pattern so as to relieve weight-bearing on the diseased limb by 10% during the first, by 50% during the second, and by 90% during the third trial. The authors found that participants were not able to “feign” the proper level of weight-bearing relief in the first (10% weight-bearing relief) and the third (90% weight-bearing relief) case, whereas being relatively accurate in achieving 50% weightbearing relief. During crutch gait, they observed shorter stance phase and longer swing phase on the diseased side as compared to the healthy side. The main goal of the research carried out by Youdas et al. [27] was evaluation of whether participants of the experiment were able to relieve their right lower limb by a specific value (50% BW) during ambulation with three point crutch gait using axillary crutches, forearm crutches, a cane and a walker. Ten healthy subjects participated in the experiment. Each of them was instructed and trained by physiotherapists on how to properly unload their right lower limb with the use of bathroom scale. The results of the experiment demonstrated that after proper training it is possible to repeatedly relieve lower limb by 50% with the use of axillary crutches and by 56% with the use of forearm crutches. Whereas in case of ambulation with the use of a walker, participants were only able to achieve vertical loading of the lower limb of 64% BW and with the use of a cane of 76% BW. Tveit et al. [23], used in their research a system of prototype footwear measurement insoles, which made it possible to record pressure under feet when walking witch crutches. Six men and nine women who underwent hip arthroplasty were studied. They were instructed to load the operated limb with 30% BW when walking. The authors concluded that none of the participants was able to recreate the recommended amount of weight bearing on the operated limb, calling into question the practice of recommending patients specific values of weight bearing on the operated limb. Similar goal, concerning evaluation of whether partial weight bearing of lower limb may be reproducible, was set by Malviya et al. [26]. This time the experimental group consisted of healthy persons, who were trained in partial weight bearing of lower limb (25% BW) – with the use of a bathroom scale. Participants were to recreate indicated level of weight (25% BW), statically on a force plate, immediately after and 60 minutes after the end of the training. The results of the study show that using bathroom scales in order to learn to partially load a lower limb is effective. Partly contradictory research results, as well as studies mostly carried out with healthy participants and using methods that do not allow approaching the problem completely, inspired the authors of this study to form a broader research project. Electronic PDF security powered by ISL-science.com L. B. Dworak et al. 308 Purpose of the study and research hypotheses The scientific goal of the research project The main purpose of this research project is to identify and evaluate biomechanical kinematic and dynamic parameters of three point crutch gait with partial weight bearing of one (diseased) lower limb, used e.g. by patients after complete unilateral endoprosthetic hip joint reconstruction. H2: H3: Specific goals Specific goals are targeted at the following issues and concern the cycle of the studied gait type: Group of kinematic parameters: 1) Identify peak angular values and angular ranges in hip joints, knee joints and ankle joints. 2) Determine angular ranges of pelvis displacement. 3) Describe angular ranges of crutch motion. 4) Determine stance, swing and double support phase duration. 5) Determine length and width of a step and gait cycle length. 6) Identify the average optimal gait velocity and step frequency. 7) Determine the degree of reproducibility of parameters. Group of dynamic parameters 1) Identify the values of the vertical component, the horizontal anterior-posterior component, as well as horizontal medial-lateral component of ground reaction forces to lower limbs. 2) Determine the value of the vertical component of ground reaction force to crutches. 3) Identify real load on the lower limb of the operated side. 4) Determine weight bearing asymmetry of the crutch on the healthy side and operated side. 5) Determine statistically significant relationship between selected kinematic and dynamic parameters. 6) Determine percentage distribution of body weight on the healthy and the diseased lower limb during a static trial consisting in free standing. Group of electromyographic parameters 1) Identification of time structure of electromyographic activity in selected muscles of lower limbs, standardized for gait cycle. Research hypotheses Considering the state of biomechanical knowledge related to the research project on three point crutch gait, as well as personal experience and intuition on the subject, the authors formulated several research hypotheses which will further undergo verification: H1: It is expected that there will be significant difference in ground reaction forces between the ope- H4: H5: rated and the healthy limb during gait, which will prove the presence of significant weight-bearing relief of the limb with hip joint endoprosthesis. It is expected that asymmetrical loading of lower limbs with the vertical component of ground reaction force during the static trial (trials on a stabilometric platform) will be notably higher in comparison to the dynamic trials (during gait over two dynamometric platforms). It is expected that during gait trials, there will be significant asymmetric loading of the crutches, with predominance of the healthy limb side. It is expected that the values of characteristic kinematic parameters describing motion in (main) joints of lower limbs will be significantly higher on the healthy limb side as compared to the operated limb side. It is expected that the studied group of patients will show high degree of reproducibility of kinematic parameters, resulting from stable velocity of locomotion and effective mastering of three point crutch gait technique. Research materials and methods The authors have received consent from the Bioethical Commission of the Poznan University of Medical Sciences, (resolution no 618/09) for carrying out this research project. Materials The trials were carried out on patients, who were diagnosed with primary unilateral coxarthrosis. The patients were recruited from several orthopedic wards in Poznan, Poland, after consulting their senior registrars. The main criteria for their selection for final analysis and statistical calculations were: type of undergone surgical procedure, time from surgery to the trials, type of used crutch gait. Patients after the surgical procedure of complete unilateral endoprosthetic hip joint reconstruction were used in the experiment. Fifteen persons were admitted to the final study. Methods The trials were carried out in the Biomechanical-Kinesiological Laboratory of the Department of Biomechanics at USPE in Poznan. Laboratory possesses the ISO 9001:2008 quality management system certificate. Many research methods were used in this project. They are illustrated in Figure 3. This research project used the most modern measurement equipment, similar to that used in leading scientific centers performing this kind of motion analysis. The entire measurement system has been integrated to form a joint Electronic PDF security powered by ISL-science.com Three point crutch gait biomechanics and kinesiology 309 Fig. 3. Block diagram of the used measurement model. Ryc. 3. Schemat blokowy zastosowanego modelu badań. measurement track for simultaneous observation of kinematic, kinetic and electromyographic parameters; thus creating conditions for significantly innovative research. Measurements were carried out in several phases: C 1st phase consisted of a static balance test, where percentage distribution of body weight on the diseased and healthy lower limb was recorded; C 2nd phase consisted of anthropometric measurements of patients and their preparation for the main trials (placing markers on their bodies according to the Vaughan – Davis model [32] and putting electrodes on selected muscles, according to SENIAM guidelines) (www.seniam.org) – Figure 4. C 3rd phase consisted of the most important measurement for this research project – the measurement of kinematic, dynamic as well as electromyographic parameters during patient locomotion over a specially designed measurement walkway – Figure 5 and Figure 6. Fig. 4. Vaughan–Davis model extended by additional 6 markers placed on the surface of the crutches (source – BTS Analyzer software). Ryc. 4. Model Vaughan–Davis zmodyfikowany o dodatkowych 6 markerów umieszczonych na powierzchni kul (źródło – program BTS Analyzer). The study analyzes several tens of kinematic and dynamic parameters of three point crutch gait (Tab. I), extending it with anthropometric measurements (essential in using the adopted Vaughan–Davis model). The above listing does not mention the group of electromyographic parameters, which described symmetrically measured muscles of: vastus medialis, vastus lateralis, tibialis anterior, gastrocnemius medialis, semitendinosus, biceps femoris. Fig. 5. Schematic diagram of the testing method: integrated measurement stand and measurement tracks for recording kinematic, kinetic and electromyographic characteristics of three point crutch gait. Ryc. 5. Schemat ideowy realizowanej metody badań: zintegrowane stanowisko i tory pomiarowe do rejestracji kinematycznych, kinetycznych i elektromiograficznych charakterystyk chodu trójpunktowego o kulach. Electronic PDF security powered by ISL-science.com L. B. Dworak et al. 310 Fig. 6. Diagram of the measurement walkway with two integrated AMTI force plates (measurements in cm). Ryc. 6. Schemat pomostu pomiarowego z wbudowanymi dwoma platformami dynamometrycznymi AMTI (wymiary liniowe w cm). Table I. Some of the studied and calculated parameters, their meaning and applied units Tabela I. Niektóre badane-obliczane parametry, ich znaczenia oraz jednostki Name Symbol Unit H cm Anthropometric parameters: body height body mass m kg pelvis width WP cm pelvis depth (right, left side) DP(l,r) cm knee width (right, left) WK(l,r) cm ankle width (right, left) WA(l,r) cm lower limb length (right, left) LLE(l,r) cm vertical RZ BW anterior and posterior RY BW lateral RX BW QL, QR BW stance phase duration (left, right) TST PH(l,r) %GC swing phase duration (left, right) TSW PH(l,r) %GC TDO SU %GC F Hz step length LS m step width WS m gait cycle length LGC m V m/s crutch-crutch cycle length Lcr-cr m crutch positioning width Wcr-cr m distance between ankle joint center in the diseased lower limb and the crutch on the same side (ipsilaterally) Lcr-A m HFE deg AFD-FP deg forward/backward tilt PT deg rising dropping PO deg intern./extern. rotation PR deg sagittal plane CrT deg frontal CrO deg transverse CrR deg Ground reaction force parameters body weight distribution on left, right limb (in postural stability static tests) Kinematic parameters: a) time and space for lower limbs double support phase duration step frequency gait velocity b) time and space for crutches c) range of motion of lower limb joints during the gait cycle hip joint talocrural d) range of motion of pelvis e) range of motion during gait cycle for crutch motion in three planes Electronic PDF security powered by ISL-science.com Three point crutch gait biomechanics and kinesiology Summary This conceptual study presents a research project, which aims at analyzing biomechanically and kinesiologically three point crutch gait in patients after complete unilateral endoprosthetic hip joint reconstruction. In their attempt to describe (from the perspective of biomechanics and kinesiology) the kinematics of three point crutch gait against the background of current knowledge, the authors formulated their goals and research hypotheses. They also characterized the measurement track they used and listed analyzed parameters. The results of most of the trials carried out as part of this project were presented in the doctoral thesis Biomechanical analysis of three-point crutch gait in patients after lower limb injuries” [33]. They will be successively presented in a series of publications prepared by the author and his team. The study was financed in stages from the following sources: supervisor’s grant from the Polish Ministry of Science and Higher Education No N N404 1973 33, a grant for the statutory activity of the Chair of Biomechanics, USPE in Poznan and of the Department of Bionics at the University of Fine Arts in Poznan. The authors would like to thank their colleague Krzysztof Kmiecik, MEng for the preparation of illustrations. [9] [10] [11] [12] [13] [14] [15] [16] [17] [18] [19] [20] [21] References [22] [1] Dworak L.B., Rzepnicka A., Murawa M., Mączyński J., Buszko P.: Swing-through gait from the perspective of biomechanics and kinesiology. Critical analysis of the current state of knowledge and the idea behind the research. Swing-through gait from the perspective of biomechanics and kinesiology. Critical analysis of the current state of knowledge and the idea behind the research. Chir. Narzadow Ruchu Ortop. Pol., 2010; 75(6): 392-398. [2] Dworak L.B., Mączyński J., Kręgielski T.: Relationship between ground reaction forces and velocity in standard human locomotion - the gait. Scientific Papers of the Faculty of Mechanical Engineering and Machine Building of Wroclaw University of Technology. Series: Conferences, No 21. Oficyna Wydawnicza Politechniki Wrocławskiej, 1994: 82-85. [3] Dworak L.B., Mączyński J.: Pathomechanics of selected types of locomotion - initial study. Post. Rehab., 1995; 9(2): 61-71. [4] Dworak L.B., Kmiecik K., Mączyński J.: Dynamic overloads during marching past gait. Acta Bioengin. Biomech., 2000; 2(1): 71-77. [5] Dworak L.B., Murawa M., Kabaciński, J.: Rehabilitation aids for human locomotion – Present trends in construction and ergonomics. In: Ergonomics for Disabled Persons, ed. J. Lewandowski, J. Lecewicz-Bartoszewska. Technical University of Lodz, 2005: 102-113. [6] Dworak L.B., Murawa M., Mączyński J.: Biomechanical analysis of two-point alternate crutch gait - comparison to standard gait. Fizjoter. Pol., 2006; 6(4): 310-316. [7] Murawa M.: Biomechanical analysis of two-point alternate crutch gait, case study of physiotherapy teachers and students. Master's thesis USPE in Poznan. Typescript , 2004: 63. [8] Dworak L.B., Murawa M.: Research project titled Biomechanical analysis of three-point crutch gait in patients after lower limb injuries, submitted to the Polish Ministry of Science and Higher Education for the 20th supervisor's research grant com- [23] [24] [25] [26] [27] [28] [29] [30] [31] 311 petition. Registration No XXXX, USPE in Poznan. Typescript 2007: 25. Dworak L.B., Rzepnicka A.: Research project titled Biomechanical and kinesiological analysis of swing-through crutch gait in patients after lower limb injuries, submitted to the Polish Ministry of Science and Higher Education for the 40th supervisor's research grant competition. Registration no 99846. USPE in Poznan, Typescript 2010: 39. Dega W., Senger A.: Ortopedia i Rehabilitacja, Vol. 1. PZWL, Warsaw: 1996: 83-90; 163-171. Winter G., Pederson M.: Complete Guide to Sports Injuries: How to Treat Fractures, Bruises, Sprains, Strains, Dislocations, Head Injuries, Perigee Books, 1997. Stewart K.B.: How to use crutches correctly. Nursing, 1997; 27(5): 20-22. Li S., Armstrong C.W., Cipriani D.: Three-point gait crutch walking: variability in ground reaction force during weight bearing. Arch. Phys. Med. Rehabil., 2001; 82: 86-92. Love C.: Using assisted walking devices. J. Orthop. Nurs., 2001; 5: 45-53. Van Hook F.W.: Ambulatory Devices for Chronic Gait Disorders in the Elderly. Amer. Family Phys., 2003; 67(8): 1717-1724. Timby B.K.,: Fundamental Nursing Skills and Concepts. Lippincott Williams & Wilkins; 2004; 26: 545-565. Southall V.H.: Guidelines for Specialized Health Care Procedures. Richmond: Virginia Department of Health, 2004. Inman V.T., Ralston H.J., Todd F.: Human Walking. Williams and Wilkins, Baltimore/London, 1981. Perry J.: Gait analysis. Normal and Pathological Function. SLACK Incorporated. NJ, 1992. Winter D.: The Biomechanics and Motor Control of Human Gait: Normal, Elderly and Pathological. University of Waterloo, 1998. Simoneau G.G.: Kinesiology of Walking. In: Kinesiology of the Musculoskeletal System. Foundations for Physical Rehabilitation. Ed. Neumann D.A., Mosby, St Louis 2002: 523-569. Gray F. B., Gray C., McClanahan J. W.: Assessing the accuracy of partial weight-bearing instruction. Am. J. Orthop., 1998; 27: 558-560. Tveit M., Karrholm J.: Low effectiveness of prescribed partial weight bearing. Continuous recording of vertical loads using a new pressure-sensitive insole. J. Rehabil. Med., 2001; 33, 42-46. Woolson S.T., Adler N.S.: The effect of partial or full weight bearing ambulation after cementless total hip arthroplasty. J. Arthropl., 2002; 17(7): 820-825. Hurkmans H.L.P., Bussmann J.B.J., Benda E., Verhaar J.A.N., Stam H.J.: Techniques for measuring weight bearing during standing and walking. Clin. Biomech., 2003; 18: 576-589. Malviya A., Richards J., Jones R.K., Udwadia A., Doyle J.: Reproducibility of partial weight bearing. Injury Int. J. Care Injured., 2005; 36: 556-559. Youdas J.W., Kotajarvi B.J., Padgett D.J., Kaufman K.R.: Partial weight – bearing gait using conventional assistive devices. Arch. Phys. Med. Rehabil., 2005; 86: 394-398. Nowotny-Czupryna O., Nowotny J., Sołtys J., Brzęk A., Czupryna K., Dąbrowska J.: Possibility of unloading one lower limb during crutch gait. Fizjoterapia, 2005; 13(3): 48-56. Vasarhelyi A., Baumert T., Fritsch C., Hopfenmuller W., Gradl G., Mittlmeier T.: Partial weight bearing after surgery for fractures of the lower extremity – is it achievable? Gait & Posture, 2006; 23: 99-105. Eng K., Ran R., Hozack W.J., Sharkey P.: Is partial weight bearing essential after uncemented total hip arthroplasty? J. Arthropl. Abstracts from the AAHKS Seventh Annual Meeting, 2008. Hol A.M., Grinsven S., Lucas C., Susante J. L.C., Loon C.J.M.: Partial versus unrestricted weight bearing after an uncemented femoral stem in total hip arthroplasty: recommendation of a concise rehabilitation protocol from a systematic review of the literature, Arch. Orthop. Trauma. Surg., 2010; 130: 547-555. Electronic PDF security powered by ISL-science.com 312 L. B. Dworak et al. [32] Vaughan C., Davis B., O’Connor J.: Dynamics of human gait. Kiboho Publishers, Cape Town, 1992. [33] Murawa M.: Biomechanical analysis of three-point crutch gait in patients after lower limb injuries. Doctoral thesis. USPE in Poznan. Typescript , 2011: 107. www.walkeasy.com www.seniam.org Contact address: dworak@man.poznan.pl Electronic PDF security powered by ISL-science.com