The British Association of Plastic Surgeons (2003) 56, 623–629
The fascial planes of the temple and face: an enbloc anatomical study and a plea for consistency
J.J. Accioli de Vasconcellosa, J.A. Brittob, D. Heninc, C. Vachera,d,*
a
Service de Chirurgie Maxillo-Faciale, Hopital Beaujon, AP-HP, 100 Bd du Général Leclerc, Clichy 92118,
France
b
Royal Free and University College Hospitals, London, UK
c
Service de’Anatomie Pathologique, Hopital Bichat, 56 Rue Henri Huchard, 75018 Paris, AP-HP, Paris.
Faculté Bichat, Université Paris VII, France
d
Faculté Bichat, Université Paris VII, Institut d’Anatomie de Paris, France
Received 20 January 2003; accepted 24 June 2003
KEYWORDS
Anatomy; Superficial
musculo-aponeurotic
system; Face; Temporal
region
Summary Many investigators have detailed the soft tissue anatomy of the face.
Despite the broad reference base, confusion remains about the consistent nature of
the fascial anatomy of the craniofacial soft tissue envelope in relation to the muscular,
neurovascular and specialised structures. This confusion is compounded by the lack of
consistent terminology. This study presents a coherent account of the fascial planes of
the temple and midface. Ten fresh cadaveric facial halves were dissected, in a levelby-level approach, to display the fascial anatomy of the midface and temporal region.
The contralateral 10 facial halves were coronally sectioned through the zygomatic
arch at a consistent point anterior to the tragus. These sections were histologically
prepared to demonstrate the fascial anatomy en-bloc with the skeletal and specialised
soft tissues. Three generic subcutaneous fascial layers consistently characterise the
face and temporal regions, and remain in continuity across the zygomatic arch. These
three layers are the superficial musculo-aponeurotic system (SMAS), the innominate
fascia, and the muscular fasciae. The many inconsistent names previously given to
these layers reflect their regional specialisation in the temple, zygomatic area, and
midface. Appreciation of the consistency of these layers, which are in continuity with
the layers of the scalp, greatly facilitates an understanding of applied craniofacial soft
tissue anatomy.
Q 2003 The British Association of Plastic Surgeons. Published by Elsevier Ltd. All rights
reserved.
The subcutaneous layers of the scalp have been
learned by generations of medical students according to the mnemonic SCALP, where S ¼ skin,
C ¼ connective tissue, A ¼ aponeurosis, L ¼ loose
*Corresponding author. Tel.: þ33-1-408-7571.
E-mail address: christian.vacher@bjn.ap-hop-paris.fr
areolar tissue, P ¼ pericranium. This mnemonic has
been extremely useful in demonstrating the generic
simplicity of the soft tissue layers of the scalp, as
well as acting as an aide memoire. By contrast, the
fascial anatomy of the temple and midface have
caused great confusion to many students and
surgical trainees alike. The perceived complexities
S0007-1226/03/$ - see front matter Q 2003 The British Association of Plastic Surgeons. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/S0007-1226(03)00310-2
624
J.J. Accioli de Vasconcellos et al.
have been generated in part by the large number of
published anatomical and clinical studies, each
giving a separate nomenclature to the consistent
anatomical structure. An understanding of craniofacial soft tissue anatomy is, of course, a prerequisite to understanding both reconstructive and
aesthetic surgical procedures in this area. The
purpose of this report is to simplify the craniofacial
fascial layers and provide a generic account of the
fasciae of the temple and midface, within the
context of their regional specialisation around
skeletal, muscular, glandular and neurovascular
structures.
Materials and methods
Ten fresh cadaveric heads were used for this study.
Ten hemifacial specimens were subjected to a
level-by-level planar dissection of the subcutaneous fasciae from skin to bone or muscle. The
contralateral hemiface in each case was subjected
to excision of an 8 cm coronal strip of tissue, taken
at the junction of the posterior and middle thirds of
the zygomatic arch. Each strip was incised down to
temporalis muscle above and masseter muscle
below, thereby including a segment of the zygomatic arch. Each strip was fixed in 10% neutral
formalin and then subjected to coronal section.
Having been paraffin-embedded, these blocks were
cut at 5m and stained with haematoxylin, eosin and
saffron.
Results
The fascial anatomy of the temple
The generic fascial anatomy of the temple is
demonstrated in Fig. 1. The scalp and subcutaneous
fat and connective tissue have been reflected
anteriorly to show the layers of fasciae beneath.
The most superficial layer is the temporoparietal
fascia, which often demonstrates muscle fibres in
surgical dissections. This is the generic aponeurotic
fascia, and it continues cranially as the galea of the
scalp (SCALP), and anteriorly as the orbital and
most superficial part of the orbicularis oculi muscle.
The second layer is a loose fascial layer, highly
vascularised, and rather fragile, continuing cranially as the subgaleal fascia,1 or the alternatively
named ‘loose connective tissue’ layer of the
mnemonic SCALP. In generic terms, this second
layer of vascularised fascia is the innominate
fascia.2 The deepest layer is the tough, thick,
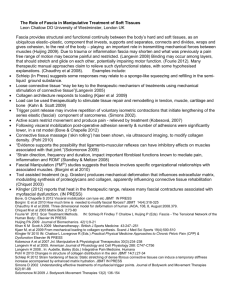
Fig. 1 The fascial layers of the temple. The aponeurotic
(temporoparietal fascia) layer is well defined and often
contains muscle fibres (A). The innominate layer is a loose
and areolar layer, but well defined as a fascial plane (L).
Temporalis muscle fascia (deep temporal fascia) is a
thick, white, plane, applied to the muscle (P). At the
level of the orbital roof, it divides into two planes, the
more superficial of which has been somewhat confusingly
called an ‘intermediate temporal fascia’ (Ramirez PRS
109, 329, 2002).
white temporalis muscle fascia, which continues
cranially as the cranial periosteum (SCALP), in
continuity at the temporal crest where temporalis
takes its cranial origin.
This anatomy, as demonstrated in planar dissection, is corroborated by en-bloc histological section
(Fig. 2). The five layers of the scalp, containing
three generic fascial layers, are all represented in
the temple. The temporoparietal fascia is the
aponeurotic layer. Beneath this is the ‘loose
connective tissue’ layer, or innominate fascia, and
in histological section it retains its multilaminate or
‘loose areolar’ structure as in the SCALP. It is highly
vascularised and not merely an avascular subfascial
space as has been previously suggested.3,4 The third
layer is the temporalis muscle (or deep temporal)
fascia. This fascia splits into a thin superficial layer
and a deeper, thicker and more fibrous layer, at the
level of the supraorbital margin. The superficial
lamina of the temporalis muscle fascia (deep
The fascial planes of the temple and face: an en-bloc anatomical study and a plea for consistency
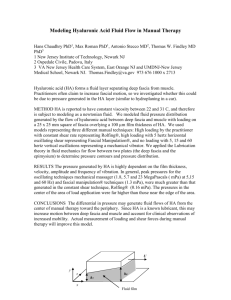
Fig. 2 The coronal section shows the planar anatomy of
the temple. The SMAS layer is a single subcutaneous layer
(A). The innominate layer is a multilaminate, highly
vascularised structure, and this explains the ‘loose,
areolar’ description of the surgical anatomy (L). The
superficial fat pad (sfp) separates the innominate fascia
from the superficial lamina of the temporalis muscle
fascia (P), and is a surgical guide to the proximity of the
temporal branches of the facial nerve (VII n). Surgical
approaches to the zygomatic arch (ZmA) cleave the
superficial lamina of the temporalis muscle (T·m) fascia
and enter the intermediate temporal fat pad (ifp).
Masseter muscle (M·m) takes origin from the posterior
surface of the zygomatic arch periosteum. The fascia
overlying temporalis (deep temporal fascia) is a thick
defined fascia deep to and independent from the
zygomatic arch (P, deep limb).
temporal fascia) is continuous with the unified
temporalis muscle fascia above the level of the
orbit, and with pericranium above the level of the
temporal crest. It has been called the intermediate
temporal fascia,5 but in generic terms, the temporalis muscle fascia is the deepest layer of the
mnemonic SCALP. The splitting of the temporalis
muscle fascia into two laminae, separated by the
(‘middle’ or ‘intermediate’) temporal fat pad, in
functional terms allows the powerful contraction of
temporalis muscle to be dissociated from tethering
the temple.
The histological appearance of the innominate
fascia of the temple is a potential source of
confusion in considering the generic anatomy of
the craniofacial fasciae. There appear to be
multiple laminae, enclosing vascular planes. In the
surgical approach, however, a single vascularised,
innominate fascia is dissected (Fig. 3). The innominate fascia, richly vascularised by branches of the
superficial temporal artery, can be raised as an
ultrathin fascial flap for eyelid or auricular cover6 or
as a free vascularised fascial bilayer transfer in the
coverage of exposed tendons.6 It is a delicate flap in
625
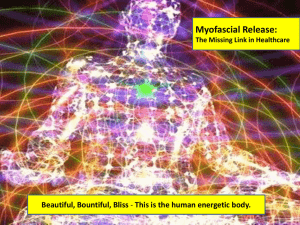
Fig. 3 (A and B) Planar, level-by-level dissections of the
fasciae of the temple. (A) The innominate fascia (L) is a
well-defined, vascularised surgical plane deep to the
temporoparietal fascia (A), which has vessels ramifying
on its superficial and deep surfaces. (B) The innominate
and temporoparietal fascial flaps raised as a pedicled
bilayer fascial flap (Bilayer F.f) to easily reach the eyelids
and auricle, protecting the frontal branch of the
superficial temporal artery (F.br STA). A possible third
layer, the superficial lamina of the temporalis muscle
fascia might be included in the flap, raised on the middle
temporal branch of the superficial temporal artery.
clinical use and should be raised with temporoparietal fascia in its caudal third to guard its blood
supply. This bilayer fascial flap is a different entity
from that described by several authors,3,7 – 9 which
consists of a bilayer of the superficial lamina of the
temporalis muscle fascia, vascularised by the
middle temporal branch of the superficial temporal
artery, and the innominate and temporoparietal
fasciae raised together on the ascending branch of
the superficial temporal artery. In theory, a multilayer fascial flap could be raised, containing the
three laminae as separate vascularised layers in
pedicled or free tissue transfer.10
626
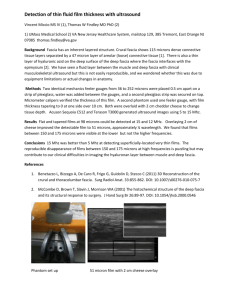
Fig. 4 Two plates from different subject cadavers
showing that the aponeurotic and innominate fascial
layers cross the zygomatic arch without attachment to it.
The temporal branches of the facial nerve (VII) are deep
to the innominate fascia (L) at this level, and in the roof
of the superficial temporal fat pad (sfp). Safe surgical
approaches to the zygomatic arch from the temple should
ideally be in the subperiosteal plane, necessarily cleaving
the superficial lamina of the temporalis muscle fascia
(circled) and exposing the intermediate temporal fat pad
(ifp). (ZMA—zygomatic arch; M·m—masseter muscle; ifp—
intermediate fat pad; A—SMAS layer; P—pericranial,
temporalis muscle (deep temporal) fascial layer).
The fascial anatomy across the zygomatic
arch
En-bloc histological section across the zygomatic
arch indicates that the generic structure of the
craniofacial fascial envelope is maintained (Fig. 4).
The temporoparietal fascia crosses the arch as the
aponeurotic layer, deep to which is the loose
areolar innominate layer. Despite previous reports
to the contrary4,11 neither of these layers attaches
to the zygomatic arch periosteum, and both are in
continuity with the corresponding generic layers in
the temple. The frontal (temporal) branches of the
J.J. Accioli de Vasconcellos et al.
facial nerve lie immediately deep to the innominate
fascia, between this and the zygomatic arch
periosteum. This is entirely consistent with their
course from the substance of the parotid gland, to
eventually lie deep to the musculo-aponeurotic
layer, within which the majority of the associated
muscles are innervated by the VII nerve from their
deep surface. This plane is characterised by a
superficial temporal fat pad12 a ‘wafer-thin’13
entity separating the innominate fascia from the
zygomatic arch periosteum. In this context the fat
pad which lies between the superficial and deep
laminae of the temporalis muscle fasciae is the
‘middle’ or ‘intermediate’ fat pad. The deep
temporal fat pad, often described as enveloping
the temporalis tendon caudal to the zygomatic
arch, was not seen in histological cross-section. It
may be, that as this structure dives deeply below
the arch it was out of the plane of our coronal cut
samples. Alternatively, this deep temporal fat pad,
also described as a temporal extension of the
buccal fat pad14 may have descended out of the
plane of our study in these cadavers as a consequence of the midfacial descent of normal ageing.
The zygomatic arch periosteum is in continuity
with the superficial lamina of the temporalis muscle
(deep temporal) fascia, and is, in generic terms, the
deepest layer described by the mnemonic SCALP.
The deep lamina of the temporalis muscle fascia
(deep temporal fascia) remains intimately related
to the temporalis muscle as it passes deep to the
zygomatic arch, and does not attach to the arch
periosteum (in contrast to the findings of Anderson
and Lo15). Temporalis muscle contraction is thereby
unimpeded by attachment to the zygomatic arch.
The fascial anatomy of the midface
Caudal to the zygomatic arch, and overlying the
region of the parotid gland, the aponeurotic layer of
the midface is dissected as the superficial musculoaponeurotic layer (SMAS) (Fig. 5), originally
described by Mitz and Peyronie.16 This layer is
continuous cranially as the temporoparietal fascia
and galea, and caudally as the platysma. Deep to a
SMAS flap, a glistening innominate fascia can be
demonstrated as an independent layer, overlying
the parotid gland, and continuing anteriorly to
protect the parotid duct and branches of the facial
nerve deep to it. In the midface, the innominate
fascia is a single, thin sheet, and ‘plasters’ the
parotid duct and emerging branches of the VII nerve
deep to it in the mid-anterior cheek as the
dissection proceeds anteriorly. When this layer is
incised and raised, the parotid gland and duct are
released into the wound, and facial nerve branches
The fascial planes of the temple and face: an en-bloc anatomical study and a plea for consistency
Fig. 5 The superficial musculoaponeurotic system
(SMAS) in the face can be raised as an adipofascial flap
in the parotid area (SMAS) to leave a thin glistening
innominate fascia overlying the parotid. Unlike in the
temple, this layer is adherent and thin over underlying
structures (the parotid). The innominate fascia (IF)
remains intact anteriorly, overlying the parotid duct,
branches of the facial nerve and the transverse facial
artery. It peters out towards the lip.
can be dissected freely. The floor of this ‘space’ is
the masseteric fascia. The parotid duct gains the
mouth by winding around the anterior border of
masseter and traversing the buccal fat pad (Fig. 6).
In the midlateral cheek, the more proximal course
of the VII nerve branches are protected deep to a
SMAS flap by the innominate fascia and substance of
the parotid gland. Careful dissection of a SMAS flap
in this area leaves the innominate fascia intact over
the parotid gland.
The deepest fascial layer, continuing caudally
from the zygomatic arch periosteum, is the masseter muscle fascia, generically the same layer as
the temporalis muscle fascia, and the scalp
pericranium. This is demonstrated in histological
section (Fig. 7). The SMAS and innominate fascia,
now attenuated to a single layer, overly the
parotid, whereas the masseter muscle fascia
remains applied to the muscle and is deep to the
parotid gland and, more anteriorly, the parotid
627
Fig. 6 The innominate fascia (IF) as an intact layer has a
glistening light reflex in the sub SMAS plane. When this
layer is breached, the parotid duct (Pd) and facial nerve
branches are released into the wound. The floor of this
space is the masseteric muscle (Mm) fascia, and more
anteriorly, the buccal fat pad (BFP).
duct. The parotid gland is not enveloped by a single
fascial layer that splits around it, but is a
specialisation of regional anatomy that is accommodated within the generic structure of the
craniofacial fasciae.
Discussion
The aim of this article is to present a simplified
means of addressing a region of important surgical
anatomy that is often misunderstood, and frequently confused in the surgical literature. There
are three fascial layers in the craniofacial soft
tissue envelope (Fig. 8). The deepest layer is the
fasciae of temporalis and masseter, which is in
continuity with periosteum at the bony attachments of these muscles. In the temple, this fascia is
split and this facilitates the unimpeded powerful
contraction of temporalis muscle.
The intermediate layer is the innominate fascia,
which in the temple, may in future have a useful
628
Fig. 7 Two plates from independent cadaveric subjects
showing that the generic consistency of the fascial layers
of the craniofacial soft tissue envelope are maintained in
the midface. The SMAS (A) and innominate fasciae (L) are
thin layers overlying the parotid gland (PG) and cranially
continuous up over the zygomatic arch. The masseter
muscle (M·m) fascia (P) is deep to the parotid gland and
continuous with zygomatic arch periosteum (circled).
There is no separate ‘investing fascia’ of the parotid
gland. (VII—temporal branch of facial nerve).
surgical application as an ultrathin pedicled flap for
eyelid or auricular cover. We have noted in our
dissections that the blood supply of this fascia is
attenuated in its caudal aspect, and easily separable from its blood supply from branches of the
superficial temporal artery. We would agree with
Carstens and colleagues6 that the innominate
fascial flap should be dissected in its caudal few
centimetres with the temporoparietal– aponeurotic
layer for pedicle safety. There is also potential for a
combined innominate – temporoparietal fascial flap,
supplied by the ascending branch of the superficial
temporal artery, for use in free flap tendon cover of
the distal extremity to provide a vascularised
bilayer as a gliding surface and to support a skin
graft.
The innominate fascia is the roof of the potential
J.J. Accioli de Vasconcellos et al.
Fig. 8 Plate showing the generic consistency of the
craniofacial fascial envelope. The ‘A’ layer is the
superficial musculofascial layer and overlies the innominate (L) layer which is loose in the temple and adherent in
the midface. The ‘P’ layer is the periosteal layer and
continuous with the fasciae of the muscles which arise
from it. Regional anatomical functional specialisation
allows for splitting of the temporalis muscle fascia (P)
above the zygomatic arch. Interposition of the parotid
gland, regional blood supply, and facial nerve occurs
between the innominate and aponeurotic layers in the
midface. These layers are important reconstructive flap
options above the zygomatic arch, and important landmarks in aesthetic surgery below the zygomatic arch
(ifp—intermediate fat pad; sfp—superficial fat pad).
space, around the parotid, into which the branches
of the VII cranial nerve emerge from their course
within the parotid. Hence surgical procedures
raising SMAS flaps anteriorly to the parotid will
protect the VII nerve as long as the intact
innominate fascia is deep to the dissection plane.
However, the VII nerve branches eventually traverse the innominate fascia in their course to
innervate the muscles of the SMAS, the majority
of which receive innervation from their deep
surfaces. In the zygomatic region, the safest
surgical dissection plane to avoid temporal branch
damage is subperiosteal. Elevating the subperiosteal midface suspension plane in aesthetic or
reconstructive craniofacial surgery from a buccal
The fascial planes of the temple and face: an en-bloc anatomical study and a plea for consistency
approach safely brings the instrument over the
zygomatic arch subperiosteally. The more superficial, subinnominate fascial plane is gained by
cleaving the superficial lamina of the temporalis
muscle fascia from the zygomatic arch, above the
level crossed by the VII nerve. Gosain et al.17 argued
that the majority of the temporal branches of the
VII nerve cross the middle third of the zygomatic
arch. Taken with our observations, it would seem
that a postero-anterior surgical exposure of the
zygomatic arch in a subperiosteal plane, in combination with the coronal scalp flap would be the
safest approach in craniofacial surgical exposure
requiring access to the midface. Exposure of the
upper third of the craniofacial skeleton without
exposure of the zygomatic arch, would aim to
sweep VII nerve forward in a combined skin—
aponeurotic—innominate fascial flap, leaving the
pericranium-temporalis fascial layer available for
other adjunctive flaps as necessary.
The most superficial layer is the aponeurotic
layer in the subcutaneous plane. It is continuous
with the orbital part of the orbicularis oculi
anteriorly, and the peripheral part of the orbicularis oris antero-inferiorly. Inferiorly it contains
platysma fibres, and superiorly, as the galea, it is in
a continuous sheet with the frontalis and occipitalis. In the midface, the zygomaticus muscles and
extrinsic lip elevators pass though it in reaching
cutaneous insertion. Above the zygomatic arch the
aponeurotic layer finds great use in reconstructive
surgery as the temporoparietal fascial flap, used as
a pedicled or free tissue transfer. This is also the
plane of extended galeal or ‘epicranial’ flaps18 and
these flaps may be pedicled on a variety of available
scalp vessels. Below the zygomatic arch, the
aponeurotic plane finds great use in aesthetic
surgery, as a means of suspending the skin of the
face and neck, and the relative benefits of its use
remain the subject of hot debate amongst aesthetic
surgeons.19
References
1. Tolhurst DE, Carstens MH, Greco RJ, Hurwitz DJ. The surgical
anatomy of the scalp. Plast Reconstr Surg 1991;87:603—12.
629
2. Casanova R, Cavalcante D, Grotting JC, Vasconez LO,
Psillakis JM. Anatomic basis for vascularized outer-table
calvarial bone flaps. Plast Reconstr Surg 1986;78:300—8.
3. Abul-Hassan HS, Von Drasek Asher G, Acland RD. Surgical
anatomy and blood supply of the fascial layer of the
temporal region. Plast Reconstr Surg 1986;77:17—28.
4. Heinrichs HL, Kaidi AA. Subperiosteal face lift: a 200 case, 4year review. Plast Reconstr Surg 1998;102:843—55.
5. Ramirez OM. Three-dimensional endoscopic midface
enhancement: a personal quest for the ideal cheek
rejunevation. Plast Reconstr Surg 2002;109:329—40.
6. Carstens MH, Greco RJ, Hurwitz DJ, Tolhurst DE. Clinical
applications of the subgaleal fascia. Plast Reconstr Surg
1991;87:615—26.
7. Upton J, Baker TM, Shoen SL, Wolfort F. Fascial flap
coverage of Achilles tendon defects. Plast Reconstr Surg
1995;95:1056—61.
8. Biswas G, Lohani I, Chari PS. The sandwich temporoparietal
free fascial flap for tendon gliding. Plast Reconstr Surg 2001;
108:1639—45.
9. Hirase Y, Kojima T, Bang HH. Double-layered free temporal
fascia flap as a two-layered tendon gliding surface. Plast
Reconstr Surg 1991;88:707—12.
10. Tellioglu AT, Tekdemir I, Erdemli EA, Tuccar E, Ulusoy G.
Temperoparietal fascia: an anatomic and histoligic reinvestigation with new potential clinical implications. Plast
Reconstr Surg 2000;105:40—5
11. Gosain AK, Yousif NJ, Madiedo G, Larson DL, Matloub HS,
Sanger JR. Surgical anatomy of the SMAS: a reinvestigation.
Plast Reconstr Surg 1993;92:1254—63.
12. Stuzin JM, Wagstrom L, Kawamoto HK, Wolfe SA. Anatomy of
the frontal branch of the facial nerve: the significance of the
temporal fat pad. Plast Reconstr Surg 1989;83:265—71.
13. Moss CJ, Mendelson BC, Taylor GI. Surgical anatomy of the
ligamentous attachments in the temple and periorbital
regions. Plast Reconstr Surg 2000;105:1475—90.
14. Zhang HM, Yan YP, Qi KM, Wang JQ, Liu ZF. Anatomical
structure of the buccal fat pad and its clinical adaptations.
Plast Reconstr Surg 2002;109:2509—18.
15. Anderson RD, Lo MW. Endoscopic malar/midface suspension
procedure. Plast Reconstr Surg 1998;102:2196—208.
16. Mitz V, Peyronie M. The superficial musculo-aponeurotic
system (SMAS) in the parotid and cheek area. Plast Reconstr
Surg 1976;58:80—8.
17. Gosain AK, Sewall SR, Yousif NJ. The temporal branch of the
facial nerve: how reliably can we predict its path? Plast
Reconstr Surg 1997;99:1224—33.
18. Montandon D, Gumener R, Pittet B. The sandwich epicranial
flaps. Plast Reconstr Surg 1996;97:302—12.
19. Jones BM. Face lifting: an initial eight year experience. Br J
Plast Surg 1995;48:203—11.