MKT in Pharmaceutical Cold Chain Management
advertisement

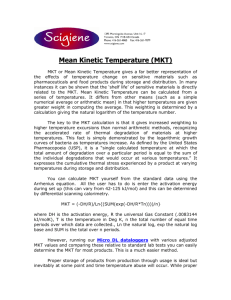
Cold Chain The Use of Mean Kinetic Temperature (MKT) in the Handling, Storage, and Distribution of Temperature Sensitive Pharmaceuticals Robert H. Seevers, Ph.D., Jeffrey Hofer, & Paul Harber Eli Lilly and Company David A. Ulrich Abbott Laboratories Rafik Bishara, Ph.D. Chair PDA Pharmaceutical Cold Chain Interest Group Introduction S tability data from both accelerated and long-term studies are used to establish recommended storage conditions and expiration dating for drug products [1]. As long as the product remains in its approved container within the specified temperature range, the quality of the product is assured until the date of expiration. However, it is likely that a product will be exposed to temperatures outside of its specified storage range as it passes through the distribution chain from the manufacturer to the final customer. For this reason, it is important to have a means to analyze the temperature exposures which may occur and to understand their potential impact on the quality of the drug product. Mean Kinetic Temperature (MKT) has been proposed as a means of evaluating thermal excursions that occur during storage and shipment [2]. For example, the United States Pharmacopeia (USP) has defined Controlled Room Temperature (CRT) as: A temperature maintained thermostatically that encompasses the usual and customary working environment of 20° to 25°C (68° to 77° F); that results in a mean kinetic temperature calculated to be not more than 25°C ; and that allows for excursions between 15° and 30°C (59° and 86°F) that are experienced in pharmacies, hospitals, and warehouses. Provided the mean kinetic temperature remains in the allowed range, transient spikes up to 40 are permitted as long as they do not exceed 24 hours. Spikes above 40°C may be permitted if the manufacturer so instructs. Articles may be labeled for storage at “controlled room temperature” or at “up to 25°C ”, or other wording based on the same mean kinetic temperature. The mean kinetic temperature is a calculated value that may be used as an isothermal storage temperature that simulates the non-isothermal effects of storage temperature variations. [3] and Controlled Cold Temperature (CCT) as: This temperature is defined as the temperature maintained thermostatically between 2° and 8°C (36° and 46°F), that allows for excursions in temperature between 0° and 15°C (32° and 59°F) that may be experienced during storage, shipping, and distribution such that the allowable calculated MKT is not more than 8°C (46°F). Transient spikes up to 25°C (77° F) may be permitted if the manufacturer so instructs and provided that such spikes do not exceed 24 hours unless supported by stability data or the manufacturer instructs otherwise [3]. These definitions each use the principles underlying MKT to provide a single temperature reflective of the exposure of a product to heat over the course of time. Thus, understanding MKT and its use is key to understanding the risks to quality experienced by a drug product exposed to temperatures outside its recommended storage conditions as it passes through the distribution system. This paper will examine the use of MKT as a tool to evaluate typical thermal excursions that occur during storage and shipment and attempt to clarify the proper role for MKT in the distribution process. Definition of MKT Mean Kinetic Temperature (MKT) is defined in the International Conference on Harmonization (ICH) Q1A document as [1]: “A single derived temperature that, if maintained over a defined period of time, affords the same thermal challenge to a drug substance or drug product as would be experienced over a range of both higher and lower temperatures for an equivalent defined period. The mean kinetic temperature is higher than the arithmetic mean temperature and takes into account the Arrhenius equation. When establishing the mean kinetic temperature for a defined period, the formula of J. D. Haynes (J. Pharm. Sci., 60:927-929, 1971) can be used.” The use of MKT to represent the expected impact of temperature variations on the quality of a drug product was described by Wolfgang Grimm [2]. 12 Pharmaceutical Outsourcing May | June 2009 Cold Chain The MKT may be calculated as follows [4]: where: ∆H = the heat of activation for the degradation reaction; assumed to be 83.144 kJ per mol (see discussion below) unless more accurate information is available from experimental studies. R = 8.3144 × 10-3 kJ per degree per mol (the universal gas constant) T1 = the average temperature, in degrees Kelvin, during the first time period T2 = the average temperature, in degrees Kelvin, during the second time period Tn = the average temperature, in degrees Kelvin during the nth time period n = the total number of temperatures recorded. Note that the interval between temperature measurements is assumed to be identical. Of particular note is the fact that Grimm [2] selected the rate constant in the equation example for two reasons. First, the value of 83.144 kJ per mol lies within the range of rate constants conceivable for the reactions that lead to loss of drug quality [5]. Secondly, the value simplifies the MKT equation because the rate constant of 83.133 kJ per mol divided by the gas constant becomes simply 10,000. The assumptions relied on to permit MKT to substitute for and simplify the temperature history of a product are: 1. 2. The activation energy for the degradation reaction is approximated by 83.144 kJ per mol The temperature/rate equation (Arrhenius) is linear through the temperature range of interest. The range of interest can be stated as “typical” supply chain temperatures, which are 0-40C. If the compound/product of interest does not follow the Arrhenius equation through this whole range, putting upper and lower temperature control limits would still allow the use of MKT. The first assumption is justified by noting that this is an average value of activation energy for breaking most covalent bonds. The use of activation energies either somewhat higher or lower will not result in significant changes to the calculated value of MKT. However, it is not always covalent bond breaking that leads to degradation; changes to the tertiary or quaternary structure of proteins, for example may result from hydrogen bond breaking [6,7]. The effect of much lower activation energies, such as might be seen for hydrogen bond breaking, on the resulting MKT is addressed below. Regarding proteins/biologics, stability profiles must be understood since there can be heat-activated or metalactivated enzymes that can dramatically change the degradation rate at specific temperatures. The second assumption of a linear model for the reaction rate versus temperature, in the absence of product-specific kinetic data, may be justified as follows. The temperature range of concern in the distribution system is generally from 0°C to 40°C. For temperatures below 0°C, the risk for solution proteins is agglomeration, and thus prolonged exposure to these temperatures should be avoided during shipping or storage of such products, unless data supports otherwise. Since most proteins are active at a body temperature of 37°C, having the upper control at 30°C (or if data supports higher) is acceptable. For freeze-dried products, exposures to temperatures as low as -20°C have been shown not to have a deleterious effect on the product in the development of the lyophilization cycle, so extended exposures to temperatures below 0°C would not be expected to have a quality impact. For solid oral drug products, in the absence of appropriate specific data, exposure to temperatures below 0°C is to be avoided. For sterile products, it is possible that exposure to temperatures below 0°C may impact contain/closure integrity, so testing, such as dye ingress, at these temperatures is recommended. However, the issue with low temperatures is not degradation, but potential physical damage. If moisture (Loss on Drying) or Solvent (Residue on Ignition) are low, potential physical degradation is probably not an issue. Similarly, exposures to temperatures above 40°C, unless supported by specific stability data, are to be avoided. There are certainly drug products that are not stable even at 30°C, but this will be known from standard stability studies performed during development, filed in the marketing authorization (e.g., NDA/BLA) [1]. The assumption of linearity may be viewed another way. Most degradation reactions are either zero or first order, that is either independent of the concentration of reactant or dependent on the concentration of only one reactant (e.g., water) [5]. Thus, the logarithmic plot of the reaction rate versus 1/T, the Arrhenius plot, will be linear until most of the reactants have been used up, a condition which seldom applies to drug products in the distribution environment based off of typical distribution/supply chain temperatures. Thus, for most drugs, in the temperature range of interest (0° to 40°C), the assumption that underlies the use of MKT in this range is that the relationship between reaction rate and temperature is either linear or pseudolinear. The shorter the timeframe under consideration the greater the likelihood that the relationship is linear or nearly so in this range. Methods In order to explore the use of MKT in evaluating temperature exposures outside storage conditions during the distribution process, it was decided to create two model pharmaceuticals, one intended for storage under refrigerated conditions and the other for Controlled Room Temperature (CRT). For each pharmaceutical a model temperature exposure history was developed which tracked the temperature experienced by the drug product every 20 minutes as it passed through the distribution process over the course of approximately one year. The shelf life of most drugs is in the range of 24-36 months, however distribution to prescription/dispensing is usually within 12 months. Of that time, a typical drug is likely to spend a month, at most, in various states of transport [8]. The remainder of the shelf life is spent in storage, first at the manufacturer, then at storage facilities in the distribution system, followed by time in storage at locations which may include pharmacies, doctor’s offices, hospitals, or the patient’s home. This is illustrated in Figures 1 and 2 which shows the temperature life history of the model drug products in 20-minute increments over the course of a year from the time of manufacture to the time the patient takes the drug. The size of the time increment can be an important consideration in evaluating the temperature history of a drug as it goes through the distribution process. In general, the increment selected should take into consideration both the duration of the segment of the distribution path being tracked (i.e., a shipping segment will take hours to days, while a storage segment is likely to be weeks or months) and the probability of a temperature excursion being experienced (more likely during shipping than storage in general). For the model presented here, 20-minute increments were selected so as to use the same increments for both shipping and storage portions of the temperature history. In practice, longer increments may be more appropriate for monitoring storage temperatures, given both the greater duration expected for storage and the decreased likelihood of temperature excursion. Tables 1 and 2 show the details of the temperature life history of our model drugs. Random numbers were used to generate the temperatures in each segment using the MKT and a standard deviation of 0.1 degrees. It can be seen from Figures 1 and 2 that a typical drug spends most of its lifetime in some type of temperature-controlled storage, whether at the original manufacturer, wholesaler, or pharmacy. This is true for both refrigerated and CRT drugs. Due to the relatively effective temperature control typical for such locations, excursions in this environment are also likely to be of fairly short duration, i.e., hours to days. Once again, in this time frame the reaction kinetics of product degradation are likely to be linear or nearly so. 13 Pharmaceutical Outsourcing May | June 2009 Cold Chain Table 1. Model Refrigerated Drug Lifetime Table 2. Model CRT Drug Lifetime Excursions Nevertheless, excursions do occur and so the models were modified to include excursions such as might be expected. Temperature excursions were inserted into each model to determine their impact on the MKT. The first excursion was inserted during the time that the drug product is stored in its commercial container at the manufacturer and the second was placed during transit from wholesaler to pharmacy. The two excursions added to each model were the same: each ramped up for 6 hours, reached a high of 20ºC above baseline, stayed at the peak for 36 hours, and ramped down for 6 hours, for a total excursion time of 48 hours. For the refrigerated product, the peak temperature was 25ºC and for the CRT product 45ºC. The models with excursions are shown in Figures 3 and 4. Figure 3. Refrigerated Product Temperature History with Excursions Figure 1. Refrigerated Drug Product Temperature History Figure 4. Controlled Room Temperature Product Temperature History with Excursions Figure 2. Controlled Room Temperature Product Temperature History Results With the models in place we can test the assumption that the choice of the activation energy has little impact on the resulting calculated MKT value. Table 3 shows the result in terms of the calculated MKT for the entire temperature history shown in Figure 2 for different values of the activation energy. 14 Pharmaceutical Outsourcing May | June 2009 Cold Chain As can been seen in Table 3, the calculated value of MKT is not very sensitive to the choice of activation energy. Changing from 83.144 kJ/ mol to 4 kJ/mol, from a value that approximates breaking weaker covalent bonds to one that represents hydrogen bond breaking only decreases the resulting value by 0.2ºC for both the refrigerated and CRT products. Similarly, using a value of 125 kJ/mol, an activation energy more in line with covalent bond breaking, leaves the values unchanged from those calculated using 83.144 kJ/mol. Finally, using a value of 250 kJ/mol, raises the MKT by 0.3 ºC for the refrigerated product and 0.2 ºC for the CRT product. Clearly, knowledge of the actual value of the activation energy of degradation reactions will permit a more accurate determination of MKT, but this is challenging in practice. It may not be possible to determine a single activation energy when more than one degradation reaction is occurring simultaneously. Furthermore, the kinetic experiments required to do so are not always performed during the development of a drug product; however, standard “accelerated stability” studies are performed (as part of ICH 1A). The value of 83.144 kJ/mol is a reasonable one to use in the absence of more specific kinetic information. Table 3. MKT Values for Model Temperature History for Different Activation Energies The impact of excursions on the calculated MKT values was determined and the results are shown in Table 4. MKT was calculated for Scenario 1 (without excursions) and Scenario 2 (with excursions) for the storage segment at the Manufacturer, for transit to the Pharmacy, and for the full year of the product’s life. The results shed light on the impact of excursions on MKT and, thus, on the value of MKT in evaluating the impact of such excursions. Table 4. Calculated MKT Values for the Segments of the Model Drug Lifetime It can be seen that the impact of adding two excursions, each with a temperature rise of 20ºC, each lasting 48 hours, on the calculated mean kinetic temperature for the entire lifetime of both the refrigerated and CRT drug, is to raise the MKT 1.6ºC and 0.6ºC, respectively. In neither case would the resulting small increase in MKT be likely to cause any concern in regard to quality. The impact of the excursions on their individual segments was also examined and is shown in Table 4. Although the excursions are identical, the change in MKT that results is not. The addition of the excursion raised the MKT of the Manufacturer Storage segment by 1.9ºC for the refrigerated drug and 1.6ºC for the CRT drug. The impact of the excursion on the Transit to Pharmacy segment was more significant: a rise of 9.8ºC for the refrigerated product and 19.2ºC for the CRT one. The resulting MKT values are 14.8ºC and 34.2ºC, respectively, making it likely that concern would be raised about the impact of the excursion on product quality. But no such alarm would be raised about the identical excursion in the manufacturer storage segment, if MKT is the only result relied upon. The difference is clearly due to the difference in the length of the segments. The transit segment is only 7 days while the storage segment is 2 months. It is also possible to calculate the MKT for the time period of the excursion alone. For the refrigerated drug product the two excursions each have a calculated MKT value of 23.5ºC. For the CRT drug product, both excursions have calculated a MKT value of 43.5ºC. Clearly, these are values that would result in an investigation and careful determination of the likely impact of the excursion on product quality, if these values were considered, rather than ones dominated by the long baseline of a storage segment. Conclusions It is clear from the models presented above that the calculated mean kinetic temperature is not sensitive to the impact of excursions that may occur if the baseline is a long period of time such as a storage segment or the entire lifetime of the drug product. For shorter baseline periods of time, such as transport segments, an excursion can have a significant impact on the resulting MKT for that segment; however, this would not necessarily have a significant impact on product quality. For most refrigerated drugs, spending 48 hours at 23.5ºC would probably raise minimal concern, since accelerated stability data at 25ºC would routinely be available to the manufacturer to help interpret the likely impact of such an excursion. In the case of room temperature drugs spending 48 hours at 43.5 ºC, this would cause concern, since it would exceed readily available accelerated stability data for the product at 40ºC for six months. The key here is that it is better to compare the length of the actual excursion approximating its magnitude with a calculated MKT against product stability data than it is to calculate an MKT for an entire segment because the length of each segment compared to the length of the typical excursion masks the impact when the MKT covers the entire segment. The value of MKT for evaluating long-term storage segments of a drug’s lifetime is then limited because, first, the length of temperature excursions will naturally tend to be limited to a small fraction of the storage time (hours or days vs. months), and second, because storage facilities are not subject to the external causes of temperature excursions that affect transport vehicles (e.g., traffic and customs). This calls into question the USP recommendation for making the standard calculation of a warehouse MKT over 12 months [4]. Over the period of a year, only a temperature excursion that covered several weeks would have a significant impact on the resulting MKT. Further, this illustrates the importance of setting upper and lower bounds on the use of MKT based on available stability data. In the CRT case above, unless the manufacturer had obtained stability data above 40ºC, something that may not routinely be done, it would be hard to estimate the impact of the excursions that went up to 45ºC and had calculated MKTs of 43.5ºC [9]. Therefore, it is appropriate to use the calculated Mean Kinetic Temperature for a drug product to approximate the effects of temperature variation that may occur during product transport in the absence of productspecific kinetic data. This is because, in the range of temperatures of interest for most drug products, the MKT equation is a valid approximation, given the magnitude of the activation energy expected and the anticipated linear or nearly linear nature of any degradation reaction that may occur. The use of long temperature histories is likely to mask the impact of a temperature excursion that lasts only hours or days unless the MKT is calculated just for the period of the excursion. Further, it is incumbent on manufacturers to perform the necessary stability studies so that the MKT of a temperature excursion can be compared against available stability data to enable an informed conclusion regarding the impact on product quality [9]. It must always be kept in mind, however, that a calculated MKT represents an approximation of the impact of temperature variation on the drug. For this reason, the use of MKT in the distribution environment should be limited to temperatures for which there are stability data to support it. At higher temperatures than evaluated in accelerated or other stability studies, the kinetics of product degradation may change or other routes of degradation may become possible. At temperatures at or below 0ºC, phase 15 Pharmaceutical Outsourcing May | June 2009 Cold Chain change may occur (tablets with moistures below 1% would be likely to have no observable effect). This may or may not be detrimental to the product, but this will not be known unless freeze-thaw studies have been done [9]. There are drugs which show significantly different rates of degradation at higher temperatures [10]. This is why it is so important that the use of MKT for a drug is supported by kinetic and stability data which verify the temperature range for which a linear temperature-degradation relationship can be expected to hold. Thus, implementing upper and lower temperature control limits that are either justified or based off of data allows MKT to be used consistently and effectively throughout the supply chain. Such studies are typically performed by the manufacturer of a drug, who will, therefore, have the necessary data to analyze the impact of temperature excursions on the drug. Others in the distribution chain will only have access to what is provided in the drug’s labeling, typically storage statements (e.g., Store at Controlled Room Temperature; excursions permitted 15-30ºC, or Do Not Freeze). Therefore, proper temperature maintenance during the storage of a drug product has the potential to have a greater positive impact on drug quality than a short-term excursion such as might happen during transportation has to damage it. Furthermore, if any excursion, whether during storage or transportation, reaches a temperature for which no stability data are available to permit understanding of the effect, then calculating MKT does not help; the product may be at significant risk. At the present time, the distribution of drugs is set up in a manner where temperature data may not be collected over the entire supply chain or may not be shared from one leg to another [8]. MKT calculations for each portion of the distribution process may be used to estimate the impact of temperature excursions on the quality of the drug product. The effectiveness of this process is limited, however, because 1) temperature data may not be collected, 2) if temperature data is collected, it is critically dependent on monitor placement; the temperature exposure observed by the monitor may not be representative of drug product that is at some distance, 3) temperature data may not be shared from one distribution leg to another, 4) only the manufacturer has all the stability and kinetic data to fully interpret the calculated MKT, and 5) the calculated MKT for a longer segment such as storage may minimize the impact of a temperature excursion due to the long baseline as demonstrated above. For these reasons MKT cannot be used as the “whole” answer to the impact of temperature excursion to drug quality. It is essential for manufacturers to set upper and lower temperature limits outside of which MKT is and is not appropriate. Manufacturers, wholesalers and mailorder pharmacies need to know (by monitoring if necessary) the temperatures to which they expose products in the distribution process. Based on the data presented here, the authors have the following recommendations: • • • • For brief segments such as transport, the MKT for the segment is best used together with proper adherence to upper and lower temperature control limits based on available stability data. For longer segments like storage, calculating the MKT of only the excursion may be preferable. Within these limitations, MKT and the Controlled Room Temperature and Cold Temperature as defined by USP are useful in understanding the impact of temperature excursions on product quality over the lifetime of a drug. Each successive owner of the material (manufacturer, wholesaler, pharmacy, and patient) can, at best, be responsible for only his or her particular segment, including the storage and transport temperatures and the interpretation of the resulting partial MKT values. ɶɶ Manufacturers should establish upper and lower control temperatures based on available stability data outside of which MKT should not be used. ɶɶ It may be useful for manufacturers to publish MKT data in the package insert. Finally, the manufacturer of a drug product has a unique responsibility since it is the manufacturer who performs the stability studies to determine the expiration dating of the drug. It is those stability studies, plus any additional ones that the manufacturer may choose to do such as freezethaw and temperature cycle studies beyond the standard ICH data package, that enable informed decisions to be made about the use of MKT to evaluate the impact of typical temperature excursions on the product. For this reason, when questions arise during the distribution process about such temperature excursions, they are best raised with the manufacturer who can use the stability data to interpret the MKT that results. Acknowledgements The authors are grateful to the members of the Pharmaceutical Cold Chain Interest Group of the PDA for their help and comments in the development of this paper. References 1. International Conference on Harmonization (ICH) Q1A(R2): Stability Testing of New Drug Substances and Products (Second Revision). 2. Grimm, W., Storage conditions for stability testing in the EC, Japan and USA; the most important market for drug products. Drug Dev Ind Pharm 1993;19:2795– 830. 3. United States Pharmacopeia (USP) General Notices. 4. USP General Chapter <1160> Pharmaceutical Calculations In Prescription Compounding. 5. Carstensen J.T. Solution Kinetics in Carstensen J.T. and Rhodes C.T. eds., Drug Stability Principles and Practices, 3rd Edition, Marcel Dekker, Inc, New York, 2000, pp 19-55. 6. Dibiase, M.D., and Kottke, M., Stability of Polypeptides and Proteins in Carstensen J.T. and Rhodes C.T. eds., Drug Stability Principles and Practices, 3rd Edition, Marcel Dekker, Inc, New York, 2000, pp 553-578. 7. Kommanaboyina, B. and Rhodes, C. T., Effects of Temperature Excursions on Mean Kinetic Temperature and Shelf Life’, Drug Development and Industrial Pharmacy,25:12,1301 — 1306, 1999. 8. USP General Chapter <1079> Good Storage and Shipping Practices. 9. Seevers, R.H., Bishara, R.H., Harber, P.J. and Lucas, T.I.,“Designing Stability Studies for Time/Temperature Exposure”, American Pharmaceutical Outsourcing, September 2005, pp. 18-23 and 55. 10. Kishore, A K. Nagwekar, J B., Influence of temperature and hydrophobic group-associated icebergs on the activation energy of drug decomposition and its implication in drug shelf-life prediction, Pharm Res. 7(7):730-5, 1990 Jul. 16 Pharmaceutical Outsourcing May | June 2009 Robert H. Seevers, Ph.D. is a Principal Regulatory Scientist, Global Regulatory Affairs (CMC) with Eli Lilly and Company in Indianapolis, Indiana (Lilly Research Laboratories, Lilly Corporate Center, Indianapolis, IN 46285). Cold Chain Rafik H. Bishara, Ph.D. is retired from his position as Director, Quality Knowledge Management and Technical Support with Eli Lilly and Company in Indianapolis, Indiana. He is Chair of the Pharmaceutical Cold Chain Interest Group, of the Parenteral Drug Association. Paul Harber — (AgEn, BS, MS, Purdue Univ., 1981) is an Associate Engineering Consultant at Eli Lilly and Company. Paul has 28 years experience with Lilly, the past 14 years in Packaging Development. He has been active in the Pharmaceutical Cold Chain Discussion Group for the past 10 years. He has co-authored numerous articles relating to various aspects of cold chain subjects. Currently, his work is primarily devoted to supporting the shipment of early phase compounds, Active Pharmaceutical Ingredients, Clinical Trial Materials, as well as launch support for new products. Dave Ulrich is the QA Director for Distribution and Logistics for Abbott’s Global Pharmaceutical Operations (GPO) division. He has been in his current role for 4 years and his responsibilities include standardization & optimization of quality systems (cGDPs), cold chain management, supply chain system optimization, ePedigree/Track-n-Trace and import export compliance activities (FDA, USDA and EPA). He has been at Abbott 21 years, with the majority of time spent in bulk (API) manufacturing operations, manufacturing QA and plant maintenance, validation & engineering. Jeffrey Hofer — (MS, Iowa State University, 1990) is a Research Advisor at Eli Lilly and Company. Jeff has 19 years experience with Lilly, the past 16 years in Product Development. Currently, his work is primarily devoted to supporting the analytical and pharmaceutical scientists during the development of the process understanding and design space exploration for new products. Jeff is also very active externally and has been an active member of the PhRMA CMC Statistics Expert Team for the past 14 years and chaired the committee for several years during that time. 17 Pharmaceutical Outsourcing May | June 2009