FINDING SOLUTIONS
Research at the
Workers’ Compensation Board
1150-20 W
(96FS-06)
BACK TO HEALTH: MUSCULOSKELETAL INJURY
PREVENTION FOR HEALTH CARE WORKERS
Wendy Wheeler
© 2000 Workers’ Compensation Board of British Columbia.
All rights reserved. The Workers’ Compensation Board of B.C. encourages the copying,
reproduction, and distribution of this document to promote health and safety in the workplace,
provided that the Workers’ Compensation Board of B.C. is acknowledged. However, no part of
this publication may be copied, reproduced, or distributed for profit or other commercial
enterprise or may be incorporated into any other publication without written permission of the
Workers’ Compensation Board of B.C.
Additional copies of this publication may be obtained by contacting:
Workers’ Compensation Board of British Columbia
Publications & Videos Department
6711 Elmbridge Way
Richmond, BC V7C 4N1
Phone (604) 276-3068 / Fax (604) 279-7406
Toll-free within BC – 1-800-661-2112
1150-20W 1996
(96FS-06)
BACK TO HEALTH: MUSCULOSKELETAL INJURY PREVENTION FOR HEALTH
CARE WORKERS
Issue:
Agency:
Representative:
Funding:
Preventing musculoskeletal injury (MSI) in health care workers.
Work Health Foundation
Wendy Wheeler
$26,179.00
Context: Caregivers are at a high risk of MSI due to a multitude of factors. Prevention
strategies have varied from education, training, promotion of physical fitness, and
application of ergonomics. A health promotion approach builds on knowledge to
encourage a change in beliefs, values, attitudes, intentions and self-efficacy, to ensure
individuals avoid health risk behaviours.
Objective: To determine the effects of a health and safety promotion campaign on
several indicators of MSI prevention among health care workers.
Design: A quasi-experimental field study using non-equivalent comparison groups (a
Solomon 4-Group Design) was used to assess the effect of the health promotion
campaign. Two hospitals were selected as intervention sites and two as control sights.
Pre-intervention surveys were conducted at one of each of the control and intervention
sites. Project teams of six to seven members, representing all occupations within the
hospitals’ caregiver populations, developed the key messages and strategies of the
promotional campaign. The teams also completed situational assessments. Each
campaign was delivered over a six-week period. Post-intervention surveys were
conducted at all sites.
Setting: Four large hospitals in the Lower Mainland of BC.
Subjects: 220 caregivers from each hospital were randomly selected to receive the
survey. Selection was weighted to reflect proportions of occupations. The numbers of
pre-intervention surveys returned were 89 from the pre-test/control hospital and 98 from
the pre-test/intervention hospital. Post-test responses numbers were: 85 from the no
pre-test/control hospital, 56 from pre-test/control hospital, 93 from no pretest/intervention hospital, and 66 from pre-test/intervention hospital.
Main Outcome Measures: The survey included items that measured: self-reported
prevalence of back pain in the past year; individual knowledge; group norms and
individual beliefs; use of safe work practices; exposure to physically demanding tasks
as part of work; and other individual risk factors associate with back pain.
Results: The situational assessment identified expected safe work practices and
barriers to their implementation. MSI was not identified as a primary concern among
caregivers. Attendance at the project team meetings and participation in the
intervention decreased over time, resulting in cancellation of the final project team
meetings and final theme of the campaign. No effect was found for either the pre-test or
the intervention.
Conclusion: The results of the study can be used to guide the development and
implementation of other MSI prevention programs for caregivers. Some significant
recommendations identified are that future programs involve front-line caregivers in their
development and are timed to coincide with expressed concern for the prevention of
MSI from within the caregiver population. Programs should use existing channels to
convey messages, with face-to-face communication as the primary communication
mode. Initiatives should focus on a few specific safe work practices and include
concurrent changes within the organization to support the safe work practices. Also,
interventions should address the multi-factorial nature of the risk factors by including
environmental, psychosocial and individual strategies.
Back to Health:
Musculoskeletal Injury Prevention
for Health Care Workers
Final Report
Prepared by: Wendy Wheeler, MSc.
Back to Health Project Co-ordinator
Employee Health and Safety Services
Healthcare Benefit Trust
On behalf of: WORK HEALTH FOUNDATION
Presented to: Workers’ Compensation Board of British Columbia
Grants and Awards Advisory Committee
Carol Gordon
HEALTHCARE BENEFIT TRUST
TABLE OF CONTENTS
1
INTRODUCTION ............................................................................................................................................. 3
1.1
1.2
1.3
1.4
2
PREVALENCE OF MUSCULOSKELETAL INJURIES AMONG HEALTH CARE WORKERS ................................ 3
RISK FACTORS ASSOCIATED WITH THE PREVALENCE OF MUSCULOSKELETAL INJURY............................ 3
PREVENTION OF MUSCULOSKELETAL INJURIES: HEALTH PROMOTION APPROACH ................................. 4
PURPOSE STATEMENT.................................................................................................................................... 5
METHODS......................................................................................................................................................... 7
2.1
STUDY DESIGN AND STUDY POPULATION ..................................................................................................... 7
TIMELINE .................................................................................................................................................................. 7
2.2 SITUATIONAL ASSESSMENT ........................................................................................................................... 8
2.3 THE INTERVENTION ....................................................................................................................................... 9
2.3.1 Development and Implementation of the BE BACK SAFE Campaign....................................................... 9
2.3.2 Key points for the BE BACK SAFE Campaign .......................................................................................... 9
2.4 BACK TO HEALTH SURVEY .......................................................................................................................... 11
2.4.1 Prevalence of Back Pain...................................................................................................................... 11
2.4.2 Individual Knowledge.......................................................................................................................... 11
2.4.3 Group Norms and Individual Beliefs ................................................................................................... 11
2.4.4 Use of Safe Work Practices.................................................................................................................. 12
2.4.5 Exposure to Physically Demanding Tasks ........................................................................................... 12
2.4.6 Other Risk Factors............................................................................................................................... 12
3
RESULTS......................................................................................................................................................... 13
3.1 SURVEY RESPONSE AND STUDY SAMPLE .................................................................................................... 13
3.2 SITUATIONAL ASSESSMENT ......................................................................................................................... 15
3.2.1 Identification of expected safe work practices ..................................................................................... 15
3.2.2 Identification of barriers that may prevent caregivers from performing safe work practices ............. 15
3.2.3 Issues and Concerns of the Front-line Caregivers .............................................................................. 17
3.2.4 Communication networks of caregivers............................................................................................... 18
3.3 THE INTERVENTION ..................................................................................................................................... 20
3.3.1 Implementation of the Intervention...................................................................................................... 20
3.3.2 Effect of the Intervention ..................................................................................................................... 22
3.4 DESCRIPTIVE SURVEY RESULTS.................................................................................................................. 23
3.4.1 Prevalence of back pain and leave from work ..................................................................................... 23
3.4.2 Individual Knowledge.......................................................................................................................... 25
3.4.3 Group Norms & Individual Beliefs ...................................................................................................... 26
3.4.4 Work practices ..................................................................................................................................... 32
3.4.5 Exposure to physically demanding tasks ............................................................................................. 38
3.4.6 Prevalence of individual risk factors ................................................................................................... 39
4
DISCUSSION................................................................................................................................................... 41
4.1 SIGNIFICANCE OF RESULTS ......................................................................................................................... 41
4.2 SITUATIONAL ASSESSMENT – WHAT DID WE LEARN?................................................................................ 42
4.2.1 Barriers that may prevent caregivers from performing safe work practices. ...................................... 42
4.2.2 Communication Strategies for Reaching Caregivers........................................................................... 43
4.3 THE INTERVENTION -- WHAT DID WE LEARN? .......................................................................................... 43
4.3.1 Development and Implementation of Interventions for Caregivers ..................................................... 43
4.4 SURVEY RESULTS – WHAT DID WE LEARN? ............................................................................................... 44
4.4.1 Prevalence of back pain and associated leave from work ................................................................... 44
4.4.2 Knowledge, Attitudes and Beliefs ........................................................................................................ 44
4.4.3 Work practices ..................................................................................................................................... 45
5
RECOMMENDATIONS ................................................................................................................................ 50
Back to Health: Final Report
Work Health Foundation
page 1
REFERENCES.......................................................................................................................................................... 52
APPENDIX A ............................................................................................................................................................ 53
APPENDIX B ............................................................................................................................................................ 54
Back to Health: Final Report
Work Health Foundation
page 2
1
1.1
INTRODUCTION
Prevalence of Musculoskeletal Injuries Among Health Care Workers
Health care workers have a high rate of musculoskeletal injury (MSI) leading to disability and absence
from work. In the health care industry in British Columbia, MSI injuries account for 71% of all WCB
claims (WCB, 1996), and 46% of all active long-term disability claims covered by the Healthcare Benefit
Trust (HBT, 1996). The WCB WorkSafe Focus Report on the health care industry (WCB, 1996),
revealed that 54% of all serious claims were overexertion type accidents, largely attributed to manual
handling of patients/residents, and 60% of all serious claims were for caregiver occupations (practical
nurse, aide, orderly, registered nurse, psychiatric nurse, and nurse supervisor). Furthermore, back strains
accounted for 52% of all strain type injuries. As a result, there has been a focus on the reduction of back
injuries associated with patient/resident handling activities among caregivers.
Health care workers have also reported a high prevalence of signs and symptoms of MSI. Research
studies have documented a self-reported 12-month pain prevalence rate that represents the percentage of
caregivers that report back pain due to work in the previous year. These studies have reported a lower
body MSI 12-month prevalence rate, which includes low-back pain, ranging between 34 and 64% (Engels
et al 1996; Cust, 1972; Mandel & Lohman, 1987; Smedley et al, 1995; Estryn-Behar et al, 1990; Larese &
Fiotito, 1994; Niedhammer et al, 1994; Josephson et al 1997) and an upper body MSI 12-month
prevalence rate, which includes neck and shoulder pain, ranging between 20 and 60% (Niedhammer et al,
1994; Engels et al 1996; Josephson et al, 1997; Josephson et al, 1998). The self-reports of pain
prevalence and the incidents of disability clearly demonstrate that caregivers are at high risk of MSI.
1.2
Risk Factors Associated with the Prevalence of Musculoskeletal Injury
Researchers have examined a multitude of factors that have been associated with increased risk of workrelated MSI. Generally, these can be divided into 3 main categories: work-related physical factors,
psychosocial factors, and individual factors. Work-related physical factors are related to the physical
demands of work, such as: forceful exertions; repetitive motions; awkward postures; static postures;
vibrations; and work/rest cycles. Psychosocial factors include, among other things: job content (e.g.
workload, repetitiveness, job control, mental demands, job clarity); organizational characteristics (e.g.
organizational structures, communications issues); interpersonal relationships at work (e.g. supervisoremployee relationships, social support); and temporal aspects of work and tasks (e.g. cycle time, shift
Back to Health: Final Report
Work Health Foundation
page 3
work). Individual factors are related to the characteristics of the worker, such as: age; gender; height;
body composition; physical fitness level; smoking status; and previous history of back pain and/or injury.
A critical review of epidemiological evidence for work-related musculoskeletal disorders of the neck,
upper extremity, and low back was conducted by the U.S. National Institute of Occupational Safety &
Health (NIOSH) in 1997. The review identified a number of specific work-related physical factors that
are strongly associated with specific MSI when exposures are intense, prolonged, and particularly when
workers are exposed to several risk factors simultaneously (NIOSH, 1997). Evidence has been presented
linking lifting/forceful movements, awkward postures, heavy physical work and whole body vibration
with back disorders. Evidence has also been presented linking posture, repetition, and force with neck
and shoulder disorders.
The NIOSH review also examined the increasing evidence that psychosocial factors play a role in the
development of work-related MSI. Even though the findings of the studies reviewed were not entirely
consistent, they suggest that perceptions of intensified workload, monotonous work, limited job control,
low job clarity, and low social support are associated with specific work-related MSI. These factors were
found to generally have modest strength after controlling for physical risk factors and seem to be, in part
or entirely, independent of physical factors. At present, the etiological mechanisms are poorly understood
and it is difficult to determine their relative importance in the causation of MSI, with respect to the
physical factors (NIOSH, 1997).
Individual factors may also influence the degree of risk from specific exposures to physical or
psychosocial factors. While the studies reviewed were not entirely consistent, the NIOSH review (1997)
presented evidence that age, gender, smoking, non-work-related physical activity, strength, and
anthropometry (height, weight, body mass index, and obesity) can influence the occurrence of MSI.
The multi-factorial nature of the risk factors associated with MSI has made the study of MSI a
complicated task. The results of studies are often conflicting, and many studies have not controlled for
risk factors that interact with one another. Since the research to date suggests that there are several
interrelated factors that influence the prevalence of MSI, prevention initiatives should consider the effects
of work-related physical risk factors, the psychosocial risk factors and, the individual risk factors.
1.3
Prevention of Musculoskeletal Injuries: Health Promotion Approach
Many approaches have been used to prevent MSI injuries, such as: education of workers in the principles
of MSI prevention; training of workers in standard work procedures; promotion of worker physical
Back to Health: Final Report
Work Health Foundation
page 4
fitness; pre-selection of workers; and the application of ergonomics. Training and education are generally
considered essential components of prevention strategies aimed at reducing injuries. Educational
initiatives in health care have included the presentation of MSI prevention information during workplace
orientation for new employees, specific training in patient/resident mechanical lift and manual transfer
techniques, intermittent back care sessions for workers and, in the event of injury, education as a
component of rehabilitation and return to work programs. Typical education and training efforts focus on
improving an individual’s knowledge and skills. A health promotion approach recognizes that improved
individual knowledge and skills will not, by itself, lead to behavioral or organizational changes. Health
promotion theorists identify a need for knowledge, but assert that a consistent system of beliefs, values,
attitudes, intentions and self-efficacy is also necessary for an individual to avoid health risk behaviours
(Green & Kreuter, 1991).
A health promotion approach also attempts to address issues in context. It recognizes that many
individual, social and environmental factors interact to influence health. For example, if caregivers are
expected to avoid lifting patients/residents, then it is necessary to have sufficient mechanical lifting
devices available for use. Additionally, there must be written policy within the organization, guiding
supervisors and co-workers to support and reinforce the use of mechanical lifting devices as an expected
and accepted behaviour. Health Canada’s experience with social marketing campaigns such as
“ParticipAction” led to the recognition that timely information and resources relevant to an individual’s
health and well-being is necessary to facilitate change on specific health issues, and to help create a social
consensus conducive to health promotion, disease prevention and positive lifestyles (Health Canada,
1992). Their experience stresses the importance of “a sustained effort, effective planning and the use of a
broad array of tactics to produce changes in attitudes and behaviours over the long-term”. While the
development of a comprehensive social marketing campaign was not within the scope of this work, social
marketing theory served as the basis for the development of the communications material for the health
promotion campaign.
1.4
Purpose Statement
Given the magnitude of the problem, the multi-factorial nature of the associated risk factors and the
promise of health promotion campaigns, the purpose of this project is to investigate the effects of a health
and safety promotion campaign on several indicators of MSI prevention among health care workers. The
primary focus of the campaign was the prevention of back injury and/or chronic back pain among
caregivers who were in direct contact with patients/residents, including registered nurses, licensed
practical nurses and long-term care aides. The health and safety promotion campaign was developed
Back to Health: Final Report
Work Health Foundation
page 5
throughout the study period and included a thorough situational assessment, the design of a
comprehensive communications plan, and the ongoing evaluation and revision of materials.
Back to Health: Final Report
Work Health Foundation
page 6
2
2.1
METHODS
Study Design and Study Population
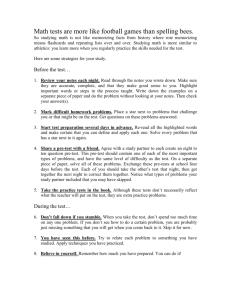
This quasi-experimental field study was designed with non-equivalent comparison groups. A Solomon 4Group Design (Solomon, 1949), was used to assess the effect of the promotion campaign and to assess the
effect of pre-testing. Four large hospitals in the Lower Mainland of British Columbia served as test sites.
Each site was randomly assigned to one of the four test conditions: No pre-test/Control Hospital; Pre-test/
Control Hospital; No pre-test/Intervention Hospital; Pre-test/Intervention Hospital (see Figure 1). No
restrictions were placed on current hospital MSI prevention programs, which continued as usual through
out the study period. Pre-test and post-test measures were collected via the Back to Health Survey (see
section 2.4).
No Pre-test/
Control
Hospital
Pre-test/
Control
Hospital
No pre-test/
Intervention
Hospital
Pre-test/
Intervention
Hospital
Post-test
n=85
Pre-test
n=89
Post-test
n=56
Post-test
n=93
Intervention
Theme #1
Intervention
Theme #2
Intervention
Theme #3
Intervention
Theme #4
Pre-test
n=98
Post-test
n=66
Intervention
Theme #1
Intervention
Theme #2
Intervention
Theme #3
Intervention
Theme #4
TIMELINE
Jan.
‘98
Feb.
‘98
Mar.
‘98
Apr.
‘98
May
‘98
June
‘98
July
‘98
Aug.
‘98
Sept.
‘98
Figure 1: Study Design, Survey Respondents and Timelines
The health and safety promotion campaign was designed to affect the entire caregiver population at each
hospital site. The caregiver population included registered nurses, licensed practical nurses and long-term
care aides that were in direct contact with patients/residents. Sample sizes for survey data collection were
determined using power tables with a desired power measure of 0.80 and a medium to small effect size
Back to Health: Final Report
Work Health Foundation
page 7
(Cohen, 1988). For statistical analysis, alpha was set at 0.05. To meet this desired power level it was
determined that a total sample size of 396 would be necessary. Assuming an attrition rate of 10%
between the pre- and post-test, it was established that 440 Back to Health Surveys were to be collected,
110 surveys from each hospital. Assuming a response rate of 50%, 220 randomly selected caregivers
from each hospital were contacted by mail to complete the Back to Health Survey. The random sample of
caregivers was weighted to reflect the proportion of registered nurses (RN), practical nurses (LPN) and
long-term care aides (LTCA) at each facility (see Table 1).
Table 1
Proportion of Primary Caregivers by Occupation for each Test Hospital
2.2
No Pre-test/
Control
Hospital
Pre-test/
Control
Hospital
(n)
%
(n)
%
(n)
%
(n)
%
(n)
%
RN
LPN
LTCA
(690)
(87)
(0)
89
11
0
(220)
(47)
(99)
60
13
27
(521)
(64)
(111)
75
9
16
(254)
(32)
(147)
59
7
34
(1685)
(230)
(357)
74
10
16
All Caregivers
(777)
(366)
No Pre-test/
Intervention
Hospital
(696)
Pre-test/
Intervention
Hospital
(433)
All
Hospitals
(2272)
Situational Assessment
Two of the four study hospitals were randomly selected to participate in an intervention that included a
situational assessment. Representatives from each of the two intervention hospitals were asked to
establish a research project team, via normal hospital protocol, to assist with the development and
implementation of the intervention. Each 6- and 7-member project team was comprised of at least one
registered nurse, one licensed practical nurse, one care aide, one nurse supervisor, one occupational health
and safety representative (a physiotherapist specializing in musculoskeletal injury prevention and
education of workers), and the research project coordinator. The goal of the team was to develop key
messages and strategies to effectively reach the target population with the promotional campaign.
Each team met four times during the initial planning period of September to December, 1997. Two hour
meetings were then scheduled every six weeks between January and May, 1998 to review and evaluate
the progress of the campaign and to discuss the development of further material. Two of the first four
planning meetings were used to conduct the situational assessment. The purpose of this assessment was
four-fold: (i) to identify the expected safe work practices; (ii) to identify barriers that may prevent
caregivers from performing these safe work practices; (iii) to understand the issues and concerns of the
Back to Health: Final Report
Work Health Foundation
page 8
front-line caregivers; and (iv) to understand the communication networks of the caregivers in order to
design effective messages and communication methods. For the purposes of this project, the term safe
work practices refers to those practices that reduce and/or eliminate exposure to risk factors associated
with musculoskeletal injury.
2.3
2.3.1
The Intervention
Development and Implementation of the BE BACK SAFE Campaign
Results from the planning meetings were used to design a strategic communications plan (see Appendix
A). From the situational assessment, it was determined that primary caregivers preferred verbal face-toface interaction. As a result, it was important to attempt to generate discussion about safe work practices
among caregivers and others with whom they work. The research team proposed a fun, light-hearted
information campaign that would highlight certain key messages. The BE BACK SAFE campaign was
developed to deliver these key messages via several different communication methods, for each of 5
different themes (see section 2.3.2). The promotional material that was developed for the campaign
included I’M BACK SAFE stickers, thematic posters, thematic caregiver newsletters with activity cards for
submission to a BE BACK SAFE collection box, and articles in the respective hospital newsletters. It was
anticipated that the individuals who were interested in the prevention of musculoskeletal injuries would
become aware of the initiative via posters, read the material and promote the initiative within their work
areas.
Each theme in the campaign was delivered over a six-week period. The health promotion material was
taken to each unit by the project coordinator, and given to representatives from the unit who put up the
posters. Newsletters were placed along side a BE BACK SAFE collection box to be picked up by the
caregivers. Activity cards could be detached from the newsletter and placed in the BE BACK SAFE
collection box for submission. A draw prize was provided for each theme to encourage activity card
submissions.
2.3.2
Key points for the BE BACK SAFE Campaign
The timelines of the campaign allowed for five themes to be developed. The themes and key messages
for the campaign were developed based on the expected safe work behaviours and barriers identified by
the project teams (see section 3.1.1.). The five themes along with their key messages are outlined in
Table 2.
Back to Health: Final Report
Work Health Foundation
page 9
Table 2
Key Points for the BE BACK SAFE Promotion Campaign
THEME
KEY MESSAGES
1
•
Introduction
Understand risks associated with patient/resident lift &
transfer activities.
•
Understand the cumulative nature of MSI (Aches to
Injuries).
2
Care for the
•
Caregiver
3
Planning Patient/
Promote “Care for the Caregiver”…do not forget about
yourself.
•
Resident Transfers
Promote idea that you should abort a procedure if it is not
going as planned.
•
Promote benefits of a team approach to transferring
patients/residents.
•
Promote concept of expecting the unexpected.
•
Promote planning and assessment each time transfer is
done.
4
Teamwork
•
Promote understanding of the components of good teamwork.
•
Promote use of good communication between the
caregiver, her/his transfer partner and the patient/resident.
5
Ergonomics
•
Promote the idea of working within a safe work zone. The
idea of a safe work zone would limit the use of awkward
postures, such as extreme forward flexion of the spine and
shoulders.
•
Promote the importance of changing the work
environment so that you can stay within this safe work
zone.
Back to Health: Final Report
Work Health Foundation
page 10
2.4
Back to Health Survey
A comprehensive employee questionnaire was designed to collect measures for analysis. Each section
included items from previously designed survey instruments that were modified, where necessary, to be
appropriate for caregivers. The survey was field tested with 20 third-year nursing students from a college
program in British Columbia. The Back to Health Survey included items that measured: self-reported
prevalence of back pain in the past year (low-back and neck/shoulder); individual knowledge; group
norms and individual beliefs; use of safe work practices; exposure to physically demanding tasks as part
of work; and other individual risk factors associated with back pain.
2.4.1 Prevalence of Back Pain
To assess the prevalence of back injury and/or pain, questions were selected from previous questionnaires
that have been used to assess the prevalence of work-related musculoskeletal injury. A series of questions
were designed to assess prevalence of MSI in the low-back region and were repeated for the
neck/shoulder region. These questions included: self-reported prevalence of back pain in the past year;
frequency of back pain; severity of back pain; medically diagnosed back injury; and, associated leave
from work.
2.4.2
Individual Knowledge
To assess individual knowledge 10 multiple-choice questions were selected from example questionnaires
that were used by the test hospitals to assess the effectiveness of their MSI prevention education
programs. Test items addressed knowledge of a caregiver’s risk of back injury, the most common causes
of back injury, principles of posture and good body mechanics. A knowledge score, representing the
number of correct answers to 10-multiple-choice questions, was determined. Mean scores were
calculated for each hospital group and compared via statistical analysis.
2.4.3 Group Norms and Individual Beliefs
To assess group norms and individual beliefs surrounding health and safety in the workplace, 10 items
were selected from questionnaires previously used with health care workers. Caregivers were asked to
rate their level of agreement with each statement using a 5-point Likert scale, with 1 indicating strongly
agree, 3 indicating neutral and 5 indicating strongly agree. These statements reflected employees’
perceptions of risk, perception of input and control over aspects of work that affect their health and safety,
Back to Health: Final Report
Work Health Foundation
page 11
feelings of recognition and support for their efforts to work safely, and perceived time pressures. Mean
scores were calculated for each of the 10 items and hospital groups were compared via statistical analysis.
2.4.4 Use of Safe Work Practices
Nineteen items were designed to determine the use of safe work practices by the employee and her/his coworkers. Caregivers were asked to rate how often each of the nineteen statements about work practice
occurred as they carried out their daily work. These items were rated on a 5-point scale, with 1 indicating
almost never, 3 indicating sometimes, and 5 indicating almost always. Responses to the nineteen items
were collapsed to represent 8 elements of safe work practice. These elements included: the frequency of
pre-task personal risk assessment; rearrangement of the workspace; assistance from co-workers with
physically demanding tasks; performance of warm-up exercises; avoidance of awkward postures;
informing others of safety issues; receipt of adequate training about the safe use of equipment; and,
following hospital safe work policies and procedures. Mean scores were calculated for each of the 8
elements and hospital groups were compared via statistical analysis. Respondents were also asked to
provide reasons for not reporting a safety issue or problem ‘almost always’, and/or not following hospital
safe work policies and procedures ‘almost always’.
2.4.5 Exposure to Physically Demanding Tasks
To assess exposure to physically demanding tasks as part of work, a series of questions were developed to
assess the daily tasks of the caregiver. Caregivers were asked to indicate which of the following items
were part of their daily work: sitting; standing; crouching; stooping; bathing patients/residents; manual
lifting or transferring patients/residents; lifting/carrying heavy materials or equipment; pulling equipment
or carts; working with elbows above shoulders; forceful or repetitive arm work; and, working with elbows
well out the side. Caregivers were also asked to estimate the frequency and duration of exposure to these
tasks.
2.4.6 Other Risk Factors
Additionally, the survey included questions to determine other individual risk factors, such as: gender;
age; experience as a caregiver; body mass index; smoking status; and, participation in regular physical
activity. The survey also requested information about caregiver occupation and current work area.
Back to Health: Final Report
Work Health Foundation
page 12
3
3.1
RESULTS
Survey Response and Study Sample
The post-test survey response rate for each hospital group was between 25% and 42% (see Table 3). The
attrition rate between the pre-test and the post-test surveys was 35%. A total of 300 post-test
questionnaires were returned from caregivers at all four hospitals in September 1998, and were used for
analysis. None of these results met the study design assumptions (Section 2.1).
Table 3.
Survey Response Rate for each test hospital
No Pre-test/
Control
Hospital
(n)
%
pre-test survey
post-test survey
(83)
37.7
Pre-test/
Control
Hospital
(n)
%
(89)
(56)
40.5
25.4
No Pre-test/
Intervention
Hospital
(n)
%
Pre-test/
Intervention
Hospital
(n)
%
(93)
98)
(66)
42.3
44.5
30.0
All
Hospitals
(n)
%
(187)
(300)
42.5
34.1
Table 4 shows the demographic characteristics of the caregivers in the post-test sample group. The group
was predominantly female, with a median age between 41-49. Almost half of the group had over 20 years
of experience as a caregiver. Additionally, there was representation from all hospital work areas with
some caregivers reporting multiple work areas. χ2-square analysis (p <0.05) was used to determine if
there were differences between hospitals for demographic characteristics. There were no significant
differences found between hospital groups, for gender, age, or experience. However, the two pre-test
hospitals had a significantly greater proportion of long-term care aides (LTCA).
Back to Health: Final Report
Work Health Foundation
page 13
Table 4.
Demographic Characteristics of Caregivers in Post-test Survey Sample
Demographic
Characteristic
No Pre-test/
Control
(n = 85)
Pre-test/
Control
(n= 56)
No Pre-test/
Intervention
(n = 93)
Pre-test/
Intervention
(n = 66)
TOTAL
81
9
0
68
14
18
80
10
10
68
8
24
78
10
12
96
4
96
4
94
6
98
2
96
4
0
27
33
29
11
8
15
39
35
3
7
27
32
31
3
5
23
44
25
3
5
23
37
30
5
7
18
34
41
8
11
38
43
2
20
33
45
6
18
24
52
5
17
32
46
(n = 300)
Occupation*
RN (%)
LPN (%)
LTCA (%)
Gender
Female (%)
Male (%)
Age
< 30 yrs (%)
33-39 yrs (%)
41-49 yrs (%)
51-59 yrs (%)
> 60 yrs (%)
Experience
2-5 yrs (%)
6-10 yrs (%)
11-20 yrs (%)
20+ yrs (%)
Work Area**
Med/Surg/Ortho
LTC/Extended
ER
Critical/ICU
OR/PAR
OB/Maternity
Renal/Dialysis
Ambulatory DC
Psych
Rehab/DPU
Pediatrics
Other
27
12
12
10
8
7
6
5
4
3
6
* Significantly different χ2 analysis, p < 0.05
**Multiple work areas reported by several caregivers therefore percentages add up to more
than 100
Back to Health: Final Report
Work Health Foundation
page 14
3.2
3.2.1
Situational Assessment
Identification of expected safe work practices
The promotion campaign was based upon previously established comprehensive musculoskeletal injury
prevention education programs at the two intervention hospitals. The learning objectives of these
education programs were re-stated in terms of safe work practices and were validated by the research
project teams. These expected safe work practices included:
A. Caregivers use standardized techniques for safe patient/resident transfers whenever possible,
and modify those techniques using basic principles of good body mechanics in non-ideal
situations. These standardized techniques include the use of a mechanical lift when a
patient/resident is unable to weight bear, is not reliable in weight bearing, is agitated or
aggressive, or is unpredictable.
B. Caregivers communicate effectively before, during and after patient/resident transferring
activities to ensure that they are supporting their share of the load in unison with their partner,
for effective execution of team transfers.
C. Caregivers use a problem-solving approach to assess and plan each patient/resident transfer
activity.
D. Caregivers use ergonomic principles to modify their work environments to reduce the
physical demands of their job tasks. (e.g. lower bed rails, move obstacles).
E. Caregivers actively engage in fitness, relaxation and warm-up exercises to prepare their
bodies for the demands of their work.
3.2.2
Identification of barriers that may prevent caregivers from performing safe work
practices
Caregivers on the project team were asked to discuss barriers to utilizing the identified safe work
practices. Listed below are the barriers that correspond to the identified safe work practices. Data from
meeting notes were combined into one comprehensive list that represents the results of four hours of
discussion with the two project teams (6 and 7 team members present).
Back to Health: Final Report
Work Health Foundation
page 15
A. Barriers for the use of standardized techniques and principles of good body mechanics.
•
Some caregivers may not be careful during patient/resident lift & transfer activities. They may have
used non-standard techniques previously and did not get hurt, so it may not be perceived as risky.
•
Some caregivers do not use mechanical lifts. There may be some lack of understanding of their
appropriate use. Some caregivers may not be comfortable using lifts. Some may not have time to get
a lift.
•
There may be a lack of good modeling of safe work practices from co-workers.
•
Some caregivers may not be supported and recognized for safe work practices and there may be a
lack of consistent consequences for unsafe work practices.
•
It is not always possible to use standardized techniques (e.g. lack of space, emergency situations).
Caregivers must react to non-ideal situations.
B. Barriers to effective execution of team transfers.
•
Some caregivers may have a lack of faith and confidence in co-workers, especially if they do not
work with them regularly.
•
Some caregivers may not have a clear understanding of how teams work: support, respect, trust, and
valuing every member for their contribution.
•
There may be a lack of good team leadership/authority.
•
There may be a lack of good communication between everyone involved (caregiver, co-workers, and
patients/residents).
•
Some caregivers may have the feeling that once you start a lift you should finish it no matter what;
caregivers may not remember that it is all right to abort a procedure if it is not working.
•
Some caregivers may prefer to get things done on their own, and may not appreciate the benefits of a
team approach (relates to notion of primary versus team nursing practice).
•
Some caregivers may not be willing/able to help others; it may be difficult to do so when they are
very busy.
Back to Health: Final Report
Work Health Foundation
page 16
C. Barriers to good assessment and planning for all patient/resident transfers.
•
Many incidents happen because of “unexpected” events.
•
Many caregivers rely on instructions from the Care Plan (ADL Card) to identify appropriate transfer
procedures. Patient/residents conditions can change often, and the patient/resident must be reassessed by others.
•
Some caregivers may feel that they must follow the Care Plan instructions, and thus it may be unclear
that they can always choose a safer option.
D. Barriers to the use of ergonomic principles to reduce physical demands of job.
•
Some caregivers may not make changes to the work environment so that it is safer for them. It is
particularly difficult in extended care where the environment is considered the resident’s room, and
the caregiver is the “visitor”.
E. Barriers that inhibit caregivers from preparing their bodies for the physical demands of their
work.
•
Many caregivers may put the needs of the patient/resident first; they may forget about themselves.
•
Caregivers may prefer group activities to stay motivated, but it is very difficult with shift changes to
get everyone together.
•
Warm-up activities may be hard to fit into a hectic schedule.
3.2.3
Issues and Concerns of the Front-line Caregivers
The profile of MSI prevention issues among caregivers was explored via group discussion. MSI
prevention has not been a current “hot topic” among caregivers. Instead, caregivers perceive it to be
primarily a concern for managers, supervisors and occupational health and safety representatives.
Caregivers agreed unanimously that back pain and injury has been accepted as part of their job. Among
caregivers, current support for MSI prevention initiatives seems to come from individuals who have
previously experienced back injury. Some of these individuals, however, may perceive that it is too late
for them to prevent back pain. It was also suggested that the younger caregivers might assume that it
would never happen to them.
Back to Health: Final Report
Work Health Foundation
page 17
Current high profile issues for caregivers were explored via group discussion. The issues raised were
primarily related to the effects of organizational change and pending labour negotiation. Throughout the
study period, the health care system in British Columbia was going through a process of regionalization
and the groups anticipated collective agreement negotiations. Caregivers were concerned about how the
shift to regionalization was going to affect them. This was expressed in terms of concern over job
security, workload and changing work demands. Additionally, caregivers expressed that, as employees in
the midst of the change process, they have not felt valued as part of the organization. This has resulted in
low morale. As such, caregivers will not currently be motivated by long-term benefit or benefits to the
organization as a whole. It was suggested that incentives associated with the campaign should focus on
short-term, personal benefits for primary caregivers.
3.2.4
Communication networks of caregivers
Communication charts were developed to understand how information is transmitted between caregivers
and others with whom they work. Each member of the project team was asked to create a
communications chart, which included: (i) how they communicate with co-workers; (ii) who they
communicate with; (iii) who is influential to the way they carry out their work, and why; and (iv) what are
the barriers to good communication. Summarized data from caregiver communication charts and the
meeting notes are presented below. The summary data represents five caregiver communication network
charts and meeting notes from four hours of discussion with the two project teams (5 + 6 representatives
present).
Caregivers were asked to identify and discuss how they communicate with others in the workplace. The
most frequent method of communication for caregivers was verbal face-to-face interaction, either in pairs
or small groups. This mode was also the most preferred and was perceived to be the most effective
method of interacting with fellow caregivers and other co-workers. To encourage behaviour change
through this face-to-face interaction, one hospital site has had success with peer caregivers being
designated, trained and returned to the units to act as mentors for other caregivers. Written
communication was perceived as a less effective method of reaching caregivers. Both intervention
hospitals commonly use communications books for nurses to receive memos and announcements. It was
stated that caregivers have little time available to read print material such as communication books and
pamphlets, and that caregivers may only read print material that is related to a current issue of particular
interest. Both groups perceived the regular hospital newsletter was worth reading and included articles
that were of interest to caregivers. Reaching front-line caregivers via other technologies would not
Back to Health: Final Report
Work Health Foundation
page 18
currently be effective. While both hospitals have closed circuit television sets for announcements, they
receive little attention from caregivers. These messages are slow to cycle and do not change on a regular
basis. Also, e-mail communication was perceived as effective for people at the
clinician/supervisor/manager level, but front-line caregivers do not use computers as part of their daily
work.
Caregivers were asked to identify whom they communicate with at their work, and to separate them into
two groups; those that have a primary influence on their work and those that have secondary influence on
their work. Table 5 summarizes these primary and secondary influencers for each type of caregiver from
the caregiver communication charts.
Table 5.
Primary and Secondary Infuencers from the Caregiver Communications Charts
Primary Influencers
Secondary Influencers
LTCA
Registered Nurses (RN), Clinical Resource
Nurse (CRN), Supervisor, Families,
Occupational Therapists (OT), Physical
Therapists (PT), Dietary, Occupational
Health &Safety (OH&S), Long-Term Care
Aides (LTCA), Patients, Union,
Communications/Education
Housekeeping, Social Work
LPN
other LPN, RN, CRN, LTCA, OT, PT,
Clients, Families, Manager, Chief Executive
Officer, Human Resources, Educators
Unions, Dietary
RN
*There was no Registered Nurse in
attendance at either meeting.
CRN
Physicians, other CRN,
Patients/Residents/Families, Directors,
Managers
LPN, RN, CRN, PPC, Secretary, Human
Resources, Bed Management/ Admitting/
Unit Clerks, LTCA, Pharmacy, PT, OT,
Social Work, Dietary, RT, Professional
Association.
Caregivers were also asked to discuss why they considered those individuals influential. Managers,
supervisors and other health care professionals were deemed influential because they are in a position of
authority. Families and residents/patients were seen as influential because of the caregiver’s duty of care
and the client-centered care philosophy of the organization. Fellow caregivers and other health care
professionals were influential because of mutual respect for their knowledge and expertise.
Finally, caregivers were asked to identify barriers to good communication within their organization.
Communication with caregivers was often one-way from the top down. It was perceived that this topBack to Health: Final Report
Work Health Foundation
page 19
down communication resulted in lack of understanding about what it was really like as a front-line
caregiver, which served as a barrier to good communication. Caregivers from both organizations also
agreed that information from management and other departments did not effectively get passed on to the
front-line worker.
3.3
3.3.1
The Intervention
Implementation of the Intervention
As the campaign progressed there was a downward trend in the participation rate as measured by the
percentage of caregivers that picked up a newsletter (Figure 3) and the percentage of caregivers that
completed the activity cards (Figure 4). Despite a general lack of interest by the majority of caregivers
for such an initiative, comments recorded on the activity cards returned by participating caregivers
provided positive feedback about the initiative (see Appendix B).
Back to Health: Final Report
Work Health Foundation
page 20
Percentage of primary caregiver population that picked up a
newsletter
100
No pre-test/Intervention
90
Pre-test/Intervention
80
70
60
50
40
30
20
10
0
1
2
3
4
Theme Number
Percentage of primary caregiver population that submitted an
activity card
Figure 3: Participation rate: Percentage of primary caregiver population that picked up a
caregiver newsletter
20
No pre-test/Intervention
Pre-test/Intervention
10
0
1
2
3
4
Theme Number
Figure 4: Participation Rate: Percentage of primary caregiver population that submitted an
activity card
Back to Health: Final Report
Work Health Foundation
page 21
Subsequently, at the project team meetings, there was little enthusiasm for continuing with the initiative.
Caregivers on both project teams reported that it was very difficult to attend the project meetings, as
replacements were not provided to take care of their work responsibilities. As a result, attendance at
project team meetings decreased (Figure 5) and the meeting to discuss the last theme on ergonomics was
cancelled, along with the final theme of the campaign.
10
No pre-test/Intervention
9
Number of Participants at Meeting
Pre-test/Intervention
8
7
6
5
4
3
2
1
0
09/03/1997
10/22/1997
01/09/1998
03/25/1998
Date of Meeting
Figure 5: Attendance at hospital project team meetings
3.3.2
Effect of the Intervention
The results from the previous section reveal that there was no effect of the pre-test on any of the measures
for analysis. The following section presents the results of a comparison between the pre-test intervention
hospital to the pre-test control hospital, to determine the effect of the intervention on the measures for
analysis. Comparisons were made between Control and Intervention Groups on “Post-Pre” Differences
(2-sample t-test to compare Control and Intervention on Pre- and post-intervention differences). There
were no significant differences found for any of the following items: knowledge score; 10 items on group
norms and individual beliefs surrounding health and safety in the workplace; 8 items of safe work
practice.
Back to Health: Final Report
Work Health Foundation
page 22
The only statistically significant differences that were found include one item from the group norms and
individual beliefs surrounding health and safety in the workplace. Comparison between pre-test
responses and post-test responses to the statement “timelines to complete their work were realistic”,
revealed that post-test responses were significantly more disagreeable than pre-test responses to this
question for both pre-test hospitals (2-tailed, paired t-test, p < 0.05).
3.4
Descriptive Survey Results
Since it was determined that there was no effect of the pre-test or the intervention, the following sections
report the overall survey results. Post-test survey responses for the following measures are reported: 12month self-reported prevalence of back pain; knowledge score; Likert-scale responses to items addressing
individual beliefs and group norms; frequency of the use of certain work practices; exposure to physically
demanding tasks: smoking; exercise; and body mass index.
3.4.1
Prevalence of back pain and leave from work
Self-reported prevalence of low-back pain in the past year and self-reported prevalence of neck/shoulder
pain in the past year for the post-test survey were compared for all 4 hospitals (see Figure 6). No
Percentage of respondents that reported
pain in the past year
significant differences were found between hospital groups for either measure (χ2-test, p < 0.05).
No pre-test/Control (n = 85)
Pre-test/Control (n = 55)
No pre-test/Intervention (n = 95)
Pre-test/Intervention (n = 65)
100
80
60
40
20
0
Low-Back Pain
Neck / Shoulder Pain
Figure 6: Comparison of annual self-reported pain prevalence between hospital groups.
Results are presented for the low back and neck/shoulder areas.
Back to Health: Final Report
Work Health Foundation
page 23
No significant differences were found between hospital groups for any of the other measures of MSI
prevalence on the post-test survey, which included: frequency of back pain; severity of back pain; and,
ever having a medically diagnosed back injury (χ2-test, p < 0.05). Figure 7 depicts the prevalence of MSI
among caregiver respondents.
Caregiver post-test survey sample
Caregivers that have ever experienced pain
Caregivers that experienced pain in the past year
Caregivers that have ever had a medically diagnosed
injury
Low-Back
Caregivers that stated their injury was work related
Neck/Shoulder
0
50
100
150
200
250
300
Number of Respondents
Figure 7: Prevalence of musculoskeletal outcomes among respondents
Overall, the sample group reported a high prevalence of MSI signs and symptoms. The self-reported 12month pain prevalence rate was 73% for both the low-back and neck/shoulder areas. Low back pain was
experienced once a month by 33% of respondents, once a week by 25% of respondents, once a year by
22% of respondents, and every day by 20% of respondents. The mean score for severity of low back pain
(rated on a scale of 1-10, 10 being the most severe) was 4.7 ± 2.0. Neck/shoulder pain was experienced
once a month by 33% of respondents, once a week by 23% of respondents, once a year by 20% of
respondents, and every day by 24% of respondents. The mean score for severity of neck/shoulder pain
(rated on a scale of 1-10, 10 being the most severe) was 5.2 ± 2.2.
Caregivers were asked to indicate if they ever had a medically diagnosed back injury and the associated
leave from work. Respondents reported 148 and 141 previous injuries to the low-back area and
neck/shoulder area respectively. The number of reported injuries was greater than the number of
caregivers with medically diagnosed injuries (Figure 7) as some respondents reported multiple injuries.
Back to Health: Final Report
Work Health Foundation
page 24
Ninety-seven percent of reported low-back injuries resulted in leave from work, and 70% of reported
neck/shoulder injuries resulted in leave from work. Table 6 depicts the corresponding type of leave from
work due to pain and/or injury, reported by caregivers. Some caregivers reported multiple leave
categories. The most frequently used leave involved workers’ compensation and sick leave. Almost half
of respondents indicated that they also recovered on scheduled days off.
Table 6.
Type of leave from work associated with back injury
Low-back
injury
Neck/Shoulder
Injury
Type of leave used as a percentage of injuries resulting in leave from work (multiple responses possible):
64%
46%
Workers’ compensation
54%
48%
Sick leave
48%
46%
Recovered on days off
12%
14%
Vacation leave
12%
15%
Leave without pay
7%
9%
Employment insurance
3.4.2
Individual Knowledge
There were no significant differences between hospital groups (1-way ANOVA, p < 0.05) for the
knowledge score for the post-test survey. The mean knowledge score for all caregivers was 7.4 ± 1.3.
Data was collapsed across hospital groups and is reported for the 300 respondents. Percent responses to
specific question are reported below, in order from the most correct responses to the least correct
responses.
•
98% of respondents knew that the leader verbally directs the start of the procedure, when 2 or more
persons perform a lift or transfer procedure together. While 61% of respondents indicated the cue to
move is 1-2-3-lift and 36% of respondents indicated the cue to move is on 3.
•
96% of respondents knew that it is not recommended to hold the load away from you for stability
when lifting.
•
94% of respondents knew that muscle injuries are more likely to occur if the muscle: lacks strength
due to inactivity; has not been warmed up and stretched before activity; and, is tired due to repetitive
movement or stationary positioning which is held too long
Back to Health: Final Report
Work Health Foundation
page 25
•
90% of respondents knew that standing with your feet shoulder width apart, knees slightly bent is the
position of greatest stability (good balance)
•
85% of respondents knew that pushing lets you brace your upper body and apply the force through
your leg muscles
•
81% of respondents knew that the odds of a hospital worker being injured are similar to someone
working in construction
•
80% of respondents knew that back pain is rarely caused by injuries to the discs or joints (versus
muscles & ligaments)
•
68% knew the role of the back muscles is to contract to provide postural stability (28% of respondents
thought that the primary role of the back muscles in lifting is to do nothing – your legs do all the
work).
•
39% knew that injury is least likely to result from a freak accident – some completely unforeseeable
event. (40% of respondents thought that injury is least likely to result from repeated performance of a
simple task. 15% of respondents thought that injury is least likely to result from remaining in a fixed
position for a long period of time.)
•
15% knew that good standing posture can be found if you pull up on a few strands of hair from crown
of your head straight up towards the sky. (77% of respondents thought that good standing posture can
be found if you stand with your back against a wall and do a pelvic tilt).
3.4.3
Group Norms & Individual Beliefs
Significant differences were found between hospitals groups for three of the ten items on the post-test
survey that evaluated group norms and individual beliefs surrounding health and safety in the workplace
(1-way ANOVA, p < 0.05). The three items include: the feeling that the demands of their work place
caregivers at a high risk of low-back injury, the opportunity to provide input on the design and
organization of their work, and the ability to take scheduled breaks during their workday. Comparison of
pre-test to post-test values revealed that there was no significant change over time (2-tailed, paired t-test,
p < 0.05), indicating that these differences were associated with differences between hospitals and not an
effect of pre-testing. Figures 8 to 17 depict responses by each hospital group for each of the 10 items.
These figures are presented in order from the most agreeable mean response to the most disagreeable
mean response for the group of 300 respondents.
Back to Health: Final Report
Work Health Foundation
page 26
Percentage of Respondents
100
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
80
60
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
Disagree
(5)
Strongly
Agree
Figure 8: Percent Responses to the statement, “I feel the people I work with function as
a team”.
Percentage of Respondents
100
80
60
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
Disagree
(5)
Strongly
Agree
Figure 9: Percent responses to the statement, “Generally, I feel in control of my own
health”.
Back to Health: Final Report
Work Health Foundation
page 27
Percentage of Respondents
100
80
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
60
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
(5)
Disagree
Strongly
Agree
Figure 10: Percent responses to the statement, “ I feel that the demands of my work
place me at high risk of low-back injury”.
Percentage of Respondents
100
80
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
60
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
(5)
Disagree
Strongly
Agree
Figure 11: Percent response to the statement, “I have some control over the aspects of
my work that affect my own health & safety”.
Back to Health: Final Report
Work Health Foundation
page 28
Percentage of Respondents
100
80
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
60
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
(5)
Disagree
Strongly
Agree
Figure 12: Percent responses to the statement, “I am able to take scheduled breaks
during my work day”.
Percentage of Repondents
100
80
60
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
Disagree
(5)
Strongly
Agree
Figure 13: Percent responses to the statement, “I have an opportunity to provide input
on design and organization of my work”.
Back to Health: Final Report
Work Health Foundation
page 29
Percentage of Respondents
100
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
80
60
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
Disagree
(5)
Strongly
Agree
Figure 14: Percent responses to the statement, “My employer has taken steps to chamge
unsafe or unhealthy conditions in my workplace”.
Percentage of Respondents
100
80
60
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
Disagree
(5)
Strongly
Agree
Figure 15: Percent responses to the statement, “Timelines to complete work are
realistic”.
Back to Health: Final Report
Work Health Foundation
page 30
Percentage of Respondents
100
80
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
60
40
20
0
(1)
Strongly
Disgree
(2)
Disagree
(3)
Neutral
(4) Agree
(5)
Strongly
Agree
Figure 16: Percent responses to the statement, “I receive recognition and support for the
efforts I make to work safely and follow procedures”.
Percentage of Respondents
100
80
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
60
40
20
0
(1)
Strongly
Disgree
(2)
(3) Neutral (4) Agree
Disagree
(5)
Strongly
Agree
Figure 17: Percent responses to the statement, “There are situations at work where I
choose to compromise own health & safety to benefit others”.
Back to Health: Final Report
Work Health Foundation
page 31
3.4.4
Work practices
Significant differences were found between hospitals groups for two of the eight elements of safe work
practice for the post-test survey (1-way ANOVA, p<0.05). These two items included: frequency of
performing warm-up exercises before lifting at work; and, frequency of receiving adequate
training/orientation about the safe use of equipment. Comparison of pre-test to post-test values revealed
that there was no significant change over time (2-tailed, paired t-test, p < 0.05), indicating that these
differences were associated with differences between hospitals and not an effect of pre-testing. Figures
18 to 25 depict responses by each hospital group for each of the 8 items. These figures are presented in
order from the most frequently occurring work practice, to least frequently occurring work practice for the
300 respondents.
Percentage of Respondents
100
No pre/Control (n = 85)
80
60
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
40
20
0
(1) Almost (2) Seldom
(3)
(4) Often
Never
Sometimes
(5) Almost
Always
Figure 18: Assistance for physically demanding tasks
Back to Health: Final Report
Work Health Foundation
page 32
100
Percentage of Respondents
No pre/Control (n = 85)
80
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
60
Pre-test/Intervention (n = 65)
40
20
0
(1) Almost (2) Seldom
(3)
Never
Sometimes
(4) Often
(5) Almost
Always
Figure 19: Inform others of safety problem
100
Percentage of Respondents
No pre/Control (n = 85)
80
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
60
Pre-test/Intervention (n = 65)
40
20
0
(1) Almost (2) Seldom
(3)
Never
Sometimes
(4) Often
(5) Almost
Always
Figure 20: Assess Situation
Back to Health: Final Report
Work Health Foundation
page 33
100
Percentage of Respondents
No pre/Control (n = 85)
80
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
60
Pre-test/Intervention (n = 65)
40
20
0
(1) Almost
Never
(2) Seldom
(3)
Sometimes
(4) Often
(5) Almost
Always
Figure 21: Rearrange Workspace
Percentage of Respondents
100
Pre-test/Control (n = 55)
80
Pre-test/Intervention (n = 65)
No pre/Control (n = 85)
60
No pre/Intervention (n = 95)
40
20
0
(1) Almost (2) Seldom
(3)
(4) Often
Never
Sometimes
(5) Almost
Always
Figure 22: Follow hospital policies & procedures
Back to Health: Final Report
Work Health Foundation
page 34
Percentage of Respondents
100
80
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
60
40
20
0
(1) Almost (2) Seldom
(3)
Never
Sometimes
(4) Often
(5) Almost
Always
Figure 23: Avoid Awkward Postures
Percentage of Respondents
100
No pre/Control (n = 85)
80
60
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
40
20
0
(1) Almost (2) Seldom
(3)
Never
Sometimes
(4) Often
(5) Almost
Always
Figure 24: Receive adequate training/orientation about safe use of equipment
Back to Health: Final Report
Work Health Foundation
page 35
Percentage of Respondents
100
No pre/Control (n = 85)
Pre-test/Control (n = 55)
No pre/Intervention (n = 95)
Pre-test/Intervention (n = 65)
80
60
40
20
0
(1) Almost (2) Seldom
(3)
Never
Sometimes
(4) Often
(5) Almost
Always
Figure 25: Warm-up before lifting at work
Respondents were asked to provide reasons for not reporting a safety issue or problem ‘almost always’.
Reasons from 126 respondents are depicted in Figure 26. Since multiple responses were possible,
percentages do not add up to 100.
Respondents were asked to provide reasons for not following hospital safe work policies and procedures
‘almost always’. Reasons from 145 respondents are listed in Figure 27. Since multiple responses were
possible, percentages do not add up to 100.
Back to Health: Final Report
Work Health Foundation
page 36
I forget when I'm are too busy
I don’t think any action will be taken
I take care of it myself
I don’t have time to fill in the forms
I don’t think my supervisor will respond
I don’t think the organization has sufficient resources to correct the
problem
I don’t know how to report a safety issue or problem
I don’t want to take a personal risk
I don’t think it is my responsibility
0
10
20
30
40
50
60
70
Percentage of Respondents
Figure 26: Reasons why caregivers don't report a safety issue or problem ‘almost always’
Back to Health: Final Report
Work Health Foundation
page 37
80
It w as an emergency situation
I don’t have enough time
I don’t have enough help from others
I don’t have access to proper equipment
I don’t have enough ready access to quick and simple
information
I don’t have support from others
I don’t have the appropriate know ledge
I don’t agree w ith the particular safety policy or procedure
I don’t think it’s really important enough
I don’t have the appropriate skills
0
10
20
30
40
50
60
70
Percentage of Respondents
Figure 27: Reason why caregivers don’t follow hospital safe work policies and procedures
3.4.5
Exposure to physically demanding tasks
Respondents were asked to report if their work included any of the activities and/or postures presented in
Figure 28. From the results of the post-test survey, it was reported that caregivers are involved in several
physically demanding tasks as part of their work. Significant differences between hospital groups were
found for standing for a long time, lifting/carrying heavy material or equipment, pulling equipment or
carts, and working with elbows above your shoulders (χ2-test, p <0.05). Self-reported measures of
frequency and duration of exposure were incomplete and could not be used for analysis.
Back to Health: Final Report
Work Health Foundation
page 38
80
No pre/Intervention
No pre/Control
Pre-test/Intervention
Pre-test/Control
Working with elbows well out to the side
Forceful or repetitive arm work
Working with elbows above shoulders
Pulling equipment or carts
Lifting/carrying heavy materials or equipment
Manual lifting or transferring patients/residents
Bathing patients/residents
Stooping (for a long time)
Crouching (for a long time)
Standing (for a long time)
Sitting (for a long time)
0
10
20
30
40
50
60
70
80
90
100
Percentage of Respondents
Figure 28: Percent of respondents that indicated that they were exposed to any of the noted physically
demanding tasks as part of their work.
3.4.6
Prevalence of individual risk factors
No differences were found between hospitals for gender, age, experience, number of current smokers, and
number of caregivers that engaged in aerobic exercise more the 3-4 times per week for the post-test
survey (χ2-test, p < 0.05) (see Table 7). Additionally, there was no difference between hospitals for
height, weight, and body mass index (ANOVA, p < 0.05) (see Table 8). Overall, 16% of the caregiver
sample currently smoke and 41% of caregivers do not engage in regular aerobic activity.
Back to Health: Final Report
Work Health Foundation
page 39
Table 7.
Individual Risk Factors (Gender, Age, Experience, Smoking, Exercise)
No Pre-test/
Control
(n = 85)
Pretest
Intervention
Pre-test/
Control
(n= 56)
No Pre-test/
Intervention
(n = 93)
Pre-test/
Intervention
(n = 66)
X
X
X
X
All Hospitals
(n = 300)
Gender
Female (%)
Male (%)
96
4
96
4
94
6
98
2
96
4
0
27
33
29
11
8
15
39
35
3
7
27
32
31
4
5
23
44
25
3
5
23
37
30
5
7
18
34
41
8
11
38
43
2
20
32
45
6
18
24
52
5
17
32
46
15
18
13
21
16
62
62
48
65
59
55
49
53
55
53
21
24
26
38
27
Pre-test/
Control
(n= 56)
No Pre-test/
Intervention
(n = 93)
Pre-test/
Intervention
(n = 66)
All Hospitals
(n = 300)
X
X
X
165 ± 8
70 ± 14
26 ± 4
165 ± 8
69 ± 17
25 ± 6
Age
Under 30 (%)
30-39 (%)
40-49 (%)
50-59 (%)
60 or over (%)
Experience
2-5 years (%)
6-10 years (%)
11-20 years (%)
Over 20 years (%)
Smoking
Current smokers (%)
Exercise
Engage in aerobic activity
> 3-4 times/wk (%)
Engage in flexibility activity
> 1-2 times/wk (%)
Engage in strength exercises
> 3-4 times/wk (%)
Table 8.
Individual Risk Factors (Anthropometry)
No Pre-test/
Control
(n = 85)
Pretest
Intervention
X
Anthropometry
Height (cm)
Weight (kg)
Body Mass Index (kg/m2)
Back to Health: Final Report
Work Health Foundation
165 ± 8
68 ± 15
25 ± 5
168 ± 8
73 ± 15
26 ± 5
165 ± 8
70 ± 15
25 ± 5
page 40
4
4.1
DISCUSSION
Significance of Results
The initial situational assessment provided some insight into potential barriers to safe work practices for
caregivers, issues and concerns of the front-line caregiver at the time of the study and communication
networks of the caregivers. The caregivers on the project teams felt that their contribution to the
situational assessment only represented their own personal experience and did not represent the
experiences of caregivers as a whole. The size of the research project team was determined based on the
needs of a working group to design the intervention, and as a result ended up being a very small
representative focus group for the discussion of the above items. As a result, the findings from the
situational assessment should be interpreted with caution and should be substantiated with further
investigation to determine if the results are typical of caregivers in general.
Even though the intervention had little effect on the measured outcomes, the results of this report can help
to guide ongoing development and implementation of education and MSI prevention programs among
caregivers. The following sections highlight some of the lessons learned about the development and
implementation of an educational intervention in the health care sector.
As with any study that relies on data collected via a mail-out questionnaire, there are limitations on the
ability to generalize results to the whole caregiver population based on the potential for self-selection of
questionnaire respondents. Post-test survey response rates were good at 25 to 42% for each hospital
group, with a typical response rate for mail-out questionnaires expected to be at approximately 10 to 15%.
While measures of age, gender and occupation for the study sample were typical of the caregiver
population, there is an indication that there may have been respondent self-selection based on previous
MSI experience. The self-reported pain prevalence in the past year of 73% for both low-back and
neck/shoulder pain for our study sample revealed a higher prevalence of MSI than other research studies
among caregivers. These other studies reported self-reported 12-month period pain prevalence ranging
between 34 and 64% for the lower body (Engels et al 1996; Cust, 1972; Mandel & Lohman, 1987;
Smedley et al, 1995; Estryn-Behar et al, 1990; Larese & Fiotito, 1994; Niedhammer et al, 1994;
Josephson et al, 1997), and between 20 and 60% for the upper body (Niedhammer et al, 1994; Engels et al
1996; Josephson et al, 1997; Josephson et al, 1998). Alternatively, it could indicate that prevalence rates
among BC caregivers are higher than other groups that have been previously studied.
Back to Health: Final Report
Work Health Foundation
page 41
Potential confounding variables were also identified through the situational assessment. The research
project team identified that concurrent organizational change and pending labour negotiations were
leading to feelings of concern over job security, workload and changing work demands, and low morale
among caregivers. These could have led to lack of interest in MSI prevention initiatives, as it was not
considered a priority by caregivers. The study design assumed that these confounding variables would
have had the same affect on measured outcomes at each site. While a field study of this nature cannot
control for all potential confounding variables, it has merit in assessing the process of implementation and
the effects of such an initiative in a real-world situation.
4.2
4.2.1
Situational Assessment – What did we learn?
Barriers that may prevent caregivers from performing safe work practices.
The situational assessment identified several barriers that prevent caregivers from performing safe work
practices. Many of these barriers warrant further investigation to understand their underlying causes. For
example, why is it perceived that caregivers do not use mechanical lifting devices? Are they not readily
available? Do they not have time to get one? Are they uncomfortable using them? Or, do they perceive
that mechanical interventions interfere with quality patient/resident care? Also, why is it perceived that
there is a lack of recognition and support for safe work practices? Are safe work practices in conflict with
other caregiver work (e.g. the fastest methods are recognized and supported because all the work gets
completed on time)? Are the current methods of recognition and support meaningful for the caregiver?
Or, is there lack of time to provide workers with the recognition and support they would appreciate? A
more thorough understanding of these and other barriers would allow for future planned intervention to be
more effective.
Additionally because of the varied nature of the identified barriers, further planned intervention to reduce
incidents of back pain and/or injury should not be limited to an educational intervention. Further planned
interventions should investigate such things as: availability of mechanical lifting devices; availability of
co-workers to provide assistance when necessary; effective leadership for caregivers; effective support
and recognition for the use of safe work practices; effective peer modeling of safe work practice; and, the
development of safe work procedures for situations where standardized techniques are not possible (e.g.
lack of space, emergency situations, “unexpected” events).
Back to Health: Final Report
Work Health Foundation
page 42
4.2.2
Communication Strategies for Reaching Caregivers
Finding a channel that could provide caregivers with useful health and safety information proved to be a
challenge. The results of this study revealed that a health and safety promotion campaign, based on
information conveyed from an external source via written pamphlets and posters, is ineffective at
reaching caregivers. It is possible that caregivers are most heavily influenced by already established
communication channels and that the information presented to the caregivers as part of this campaign was
not perceived to be from an influential source. Additionally, the campaign failed to tap into the preferred
face-to-face mode of communication among caregivers.
The possibility of using existing formal communication channels, particularly those that are already
perceived as influential, should be investigated further. These existing channels are depicted in Table 5
and vary depending on the caregiver’s occupation. The most likely groups include: peer caregivers,
clinical resource nurses, patient services coordinators, rehabilitation professionals (OT/PT), or health and
safety professionals. Additionally, if these existing formal communication channels are going to be
effective in relaying health and safety information, it is important to ensure that they are working
effectively. Caregivers in the situational assessment revealed that they felt that front-line caregivers were
not receiving information from organizational leaders. The merits of tapping into these existing channels
also include the integration of health and safety information with the overall strategic direction of the
organization to ensure message consistency and appropriate timing of key messages.
4.3
4.3.1
The Intervention -- What did we learn?
Development and Implementation of Interventions for Caregivers
As discussed previously (section 1.1.1), future planned interventions should not be limited to educational
initiatives. Education, however, is one of the typical approaches of most health and safety initiatives and
is a necessary complement to most organizational and environmental changes. The following lessons
were learned as a part of this research study. Front-line caregivers from the research project team
provided a wealth of information based on their knowledge and expertise. Any future educational
initiatives should involve focus group discussions with front-line caregivers to target not only expected
safe work behaviour but also identified barriers to safe work practice. The size of the focus groups should
be increased to provide adequate representation from the whole population. Additionally, small group
meetings scheduled for 2 hours were ineffective, as relief time was not provided to cover work
responsibilities for the caregivers. It was discovered that relief time is provided in 4-hour blocks and it is
Back to Health: Final Report
Work Health Foundation
page 43
therefore recommended that caregiver focus group meeting be planned for ½ day or full day sessions.
With this in mind, the continuous format of meetings every 6 weeks to develop and evaluate the material
for the campaign was not ideal. The expertise of the caregivers would be used much more effectively if
they were involved in initial focus group discussions, and field testing of the initial product. Subsequent
evaluation of material should be done via evaluation methods involving the target audience of the
material.
The intervention as a whole failed to capture the attention of a majority of caregivers. This is typical of
any health promotion campaign as those that tend to be interested in the messages in the early stages of
the campaign tend to be those that already exhibit the expected safe work behaviours. Typical
participation in this type of health promotion intervention is approximately 10-15%. This study may be an
example of program failure (i.e. effective intervention that fails in delivery) or theory failure (i.e. poorly
conceived intervention). The feedback that was received from caregivers that participated in the
campaign was generally positive and, therefore, there is evidence to suggest that the messages that were
developed were perceived as useful and appropriate for the caregiver audience.
4.4
Survey Results – What did we learn?
4.4.1
Prevalence of back pain and associated leave from work
Since prevalence is high for both low back and neck and shoulder areas of pain, MSI initiatives should
focus on prevention in general and not just on the prevention of back injuries. A variety of leave
categories contribute to the total impact of MSI on the healthcare worker. Future studies interested in
capturing the true impact should assess WCB leave, Sick leave and recovery on time off. Hospitals
should consider tracking self-reported symptoms of back pain as an indicator of the risk associated with
particular job categories. Some caregivers may have reported leave due to non-work-related back
injuries.
4.4.2
Knowledge, Attitudes and Beliefs
Knowledge scores revealed that it is generally incorrectly believed by caregivers that pelvic tilting is a
component of good posture. It was also revealed that there is a lack of understanding of the risk factors
associated with back injury and back pain. There is also a lack of understanding that repeated
performance of a simple task (REPETITION), and remaining in a fixed position for a long period of time
(STATIC) can contribute to the occurrence of cumulative MSI. Additionally, several caregivers thought
that the role of the back muscles in lifting is to do nothing – your legs do all the work. This lack of
Back to Health: Final Report
Work Health Foundation
page 44
understanding that the back muscles provide postural stability leads caregivers to be exposed to risk of
MSI when unexpected events occur as part of their daily work.
The survey revealed that caregivers had a strong feeling of control over health and aspects of work that
affect health and safety. Self-efficacy, the feeling that one is in control of one’s own health, is one of the
basic concepts of social cognitive theory (Bandura, 1986), and is important in self-directed health care.
Respondents reported that they felt that generally they were in control of their own health and that they
were in control of aspects of their work that affected their health and safety. Groups that feel in control of
their own health and safety provide a valuable resource for the development of future health promotion
initiatives. The responses to the survey questions are related to general health, and may be subject to
individual interpretation based on an individual’s definition of health. Further research should investigate
these feelings of control with respect to the safe work practices designed to prevent MSI, such as
rearranging the workspace to best suit the caregiver. It was proposed in the situational assessment that
caregivers in long-term care may not rearrange the workspace because it is considered to be the resident’s
space.
Survey responses revealed two groups of respondents; one third of respondents felt that they did receive
recognition and support for the effort they make to work safely and follow procedures, while one third of
respondents felt that they did not (see Figure 6). This recognition and support serves as positive
reinforcement for desirable safe work behaviour, and it increases the credibility of the caregiver as a good
role model for others. Both of these aspects increase the likelihood of repeated safe work practice on the
part of the caregiver and others with whom they work.
4.4.3
Work practices
The situational assessment focused on five expected safe work practices (see A to E below). Survey
findings will be discussed with respect to each of these practices.
The survey results indicated that approximately half of the respondents agreed with the statement, “there
are situations at work where I choose to compromise my own health and safety to benefit others”, while
slightly more than one third disagreed with this statement. Health and safety professionals expect
caregivers to avoid risky behaviour and engage in safe work practices. These expected safe work practices
must be considered within the context of the caregiver’s normative work practice and her/his role as a
caregiver. The decision to engage in a specific work behaviour is dependent on a multitude of factors
including individual values and beliefs, as well as the group norms of the environment. It is expected that
Back to Health: Final Report
Work Health Foundation
page 45
caregivers will make an individual decision to perform a procedure with minimal risk of injury to
themselves, but they also have a need to provide the best quality of care for the patient or resident. An
altruistic person that is willing to sacrifice personal safety for the benefit of others may risk injury in order
to provide the best quality of care for patients/residents.
Consider the example of a nurse who is providing a minimal assist to a resident as he is walking. The
resident is wearing a transfer belt and the caregiver is walking along side. If the resident collapses, he’ll
fall to the floor without support from the caregiver. The caregiver has to make a decision: do I allow the
resident to fall to the floor on his own (he might hurt himself); do I support his entire weight myself (I
might hurt myself); or do I guide the resident to the floor protecting him from injury, and leave him on the
floor to go get a mechanical lift, so that I don’t have to lift him up off the floor myself? The expected safe
work behaviour is a compromise that minimizes risk of injury for the caregiver, and minimizes risk of
injury to the resident. However, if leaving the patient on the floor while going to get a mechanical lift is
perceived to be sacrificing patient care, then this behaviour will not be exhibited. If one is going to
influence the behaviour of the caregiver, who is willing to sacrifice her/his own health and safety for the
benefit of others, further study needs to examine the safe work activities that are perceived to be in
conflict with delivering quality patient care.
It is assumed that those activities that are perceived to be associated with potential for injury would
generally be avoided. Survey results revealed that, in general, caregivers knew that the odds of a hospital
worker being injured are high and that the majority of caregivers agreed that the demands of their work
placed them at high risk of low-back injury. The survey also revealed, however, that a substantial group
of caregivers did not know that an MSI could result from repeated performance of a simple task, or that
an MSI could result from remaining in a fixed position for a long period of time. This indicates that
further investigation should be done to understand the specific perceptions of risk associated with specific
work activities, and the associated ability to avoid the risks associated with those work activities. Some
risks may be unavoidable given the current working environment, e.g. lifting a collapsed resident in a
washroom with insufficient space for a mechanical lifting device.
The survey revealed that half of the respondents indicated that if they do not follow hospital policy and
procedure it is because they do not have enough help from others. Yet, the majority of respondents
indicated that they almost always ask for assistance, receive assistance and provide assistance for
physically demanding tasks.
Back to Health: Final Report
Work Health Foundation
page 46
A. Caregivers use standardized techniques for safe patient/resident transfers whenever possible, and
modify those techniques using basic principles of good body mechanics in non-ideal situations.
These standardized techniques include the use of a mechanical lift when a patient/resident is unable to
weight bear, is not reliable in weight bearing, is agitated or aggressive, or is unpredictable.
The project team identified the concern that it was not always possible for caregivers to use standardized
techniques in non-ideal situations (e.g. lack of space, emergency situations). It was also suspected by the
project team that many work related MSIs occur because of “unexpected” events. 53% of respondents
indicated that they almost always follow hospital safe work policies and procedures. The mean response
was 4.5 ± 0.6. 75% of 145 respondents reported that if hospital safe work policies and procedures were
not followed almost always, this was because it was an emergency situation. Additionally, 28% of survey
respondents thought that the primary role of the back muscles in lifting is to do nothing – your legs do all
the work. This concept may place these caregivers at increased risk during an “unexpected” event since
their back muscles will not be prepared to provide postural stability, thus leaving the spine unguarded and
the back muscles unprepared to respond to unexpected physical demands. Further training in emergency
situations would seem to be indicated.
Mechanical lifting devices have been identified as one method to reduce the physical demands of
patient/resident handling activities. The situational assessment identified that for a variety reasons, some
caregivers do not use mechanical lifts. There may be some lack of understanding of their appropriate use.
Some caregivers may not be comfortable using lifts and some may not have time to get a lift. While 53%
of respondents indicated that they almost always follow hospital safe work policies and procedures, it was
reported by 41% of respondents that if hospital safe work policies and procedures are not followed, it is
almost always because they do not have access to proper equipment. Additionally, only 28% of
respondents revealed that they almost always receive adequate training/education about the safe use of
equipment. The mean response was 3.8 ± 1.0.
The survey questions were not designed specifically to focus on the use of mechanical lifting devices and,
therefore, further investigation should be conducted to more fully understand the patterns of use of
mechanical lifting devices by caregivers. If they are not being used, is it because there are not enough
devices readily accessible, because they are not comfortable using the technology, or because they believe
it interferes with the quality of care for the resident/patient? Additionally, this research should assess the
quality and effectiveness of any training that caregivers receive in the use of this equipment.
Back to Health: Final Report
Work Health Foundation
page 47
Caregivers also expressed concern that mechanical lifting devices were not used because there was not
enough time to get one. In fact, 71 % respondents indicated that if hospital policy and procedures were
not followed it was almost always because they do not have enough time (See Figure 27). Interestingly,
there was a bimodal response when asked if there was sufficient time to complete their work; 37% of
respondents felt that timelines were unrealistic, whereas 40% felt that timelines were realistic. The mean
response was 3.0 ± 1.0. Further analysis is required to clarify the differences between these groups.
B. Caregivers communicate effectively before, during and after patient/resident transferring activities to
ensure that they are supporting their share of the load in unison with their partner, when performing
team transfers.
There may be a lack of good communication between everyone involved (caregiver, co-workers, and
patients/residents). 98% of respondents knew that the leader verbally directs the start of the procedure,
when 2 or more persons perform a lift or transfer procedure together. 61% of respondents indicated the
cue to move is 1-2-3-lift. 36% of respondents indicated the cue to move is on 3. Basic discrepancy in
understanding safe work practices increases the risk of MSI.
C. Caregivers use a problem-solving approach to assess and plan each patient/resident transfer activity.
Many caregivers rely on instructions from the Care Plan (ADL Card) to identify the appropriate transfer
procedure. Patient/resident conditions can change often, and the patient/resident must be re-assessed by
others. Some caregivers may feel that they must follow the Care Plan instructions; it may be unclear that
they can always choose a safer option. 64% of respondents indicated that before performing a work
related task, they almost always assess the nature of the object or person, the predictability of the object or
person and the workspace for potential obstacles. The mean response was 4.6 ± 0.5. Some caregivers
may have the feeling that once they start a lift they should finish it no matter what rather than
remembering that it is acceptable to abort a procedure if it is not working.
D. Caregivers use ergonomic principles to modify their work environments to reduce the physical
demands of their job tasks. (e.g. lower bed rails, move obstacles).
Some caregivers may not make changes to the work environment so that it is safer for them. It is
particularly difficult in extended care where it is considered the resident’s room, and the caregiver is a
visitor. 64% of respondents indicated that before performing a work related task, they almost always
rearrange the workspace (i.e. adjust beds/chairs, move obstacles). The mean response was 4.6 ± 0.7.
Back to Health: Final Report
Work Health Foundation
page 48
29% of respondents indicated that they almost always try to avoid awkward or static postures while
working. The mean response was 4.0 ± 0.6.
E. Caregivers actively engage in fitness, relaxation and warm-up exercises to prepare their bodies for the
demands of their work.
Warm-up activities may be hard to fit into a hectic schedule. 94% of respondents knew that muscle
injuries are more likely to occur if the muscle has not been warmed up and stretched before activity. Yet,
only 5% of respondents indicated that they almost always perform warm-up exercises before lifting at
work. The mean response was 1.9 ± 1.2.
Back to Health: Final Report
Work Health Foundation
page 49
5
RECOMMENDATIONS
1. The process to develop strategies for musculoskeletal injury prevention among caregivers should be
re-evaluated to ensure that front-line caregivers are involved and are able to provide their expertise
and input. Consideration should be paid to developing MSI prevention expertise within the nursing
population, and developing strategies that strike a balance between providing the best possible care
for the resident/client, the demands of modern nursing practice, and the health and safety of the
caregivers themselves. Timing of future initiatives should coincide with expressed concern for the
prevention of musculoskeletal injuries from within the caregiver population. Until such time, efforts
should focus on understanding why such a prevalent cause of pain and disability may not be a high
priority among some caregivers, and may be accepted by some caregivers as part of the job.
2. Future health promotion initiatives designed to influence caregivers should focus on using existing
channels to convey messages using face-to-face communication as the primary mode of
communication. Consideration should be paid to the development of expertise within the nursing
population, which might include peer champions and/or mentors, clinical resource nurses and/or
nurse managers.
3. A revised questionnaire should be developed to investigate, in more detail, many of the issues that
were raised through discussion with the project team throughout the progress of this study. This
questionnaire may include items that examine such things as: the perceptions of risk of nursing
activities; competing priorities (i.e. welfare of patient/resident); insufficient equipment; and
insufficient time.
4. With the lack of difference between hospital groups, it may be appropriate to develop an industry
wide initiative to address some of the barriers to safe work practice among caregivers. Before this is
considered, further investigation is necessary to better understand sub-groups within the caregiver
population. Important factors may include: caregiver occupations (CRN, RN, LPN, LTCA); type of
nursing practice (long-term care, orthopaedic, intensive care); those that will sacrifice their own
health and safety for the benefit of others versus those that do not; and those that are feeling increased
time demands versus those who do not.
5. Future health and safety promotion initiatives should focus on a few specific safe work practices and
the associated barriers to their use by caregivers. Consideration should given to the inclusion of other
concurrent changes within the organization. For example, health promotion material designed to
Back to Health: Final Report
Work Health Foundation
page 50
influence the use of mechanical lifting devices should be accompanied by an organizational “no lift
policy”, the availability of sufficient equipment, training for appropriate use of that equipment, and
support from co-workers and staff for the use of that equipment.
6. The role of primary influencers should be evaluated in future initiatives and attention should be paid
to the consistency of messaging throughout the organization. It is clear that competing and
inconsistent messages from others within the organization will influence the attitudes, beliefs and
behaviour of the caregiver. Actions and messages from primary influencers within the organization
should be consistent with the health promotion campaign materials.
7. Consideration should be given to incidents that are associated with emergent or unexpected events.
Standard safe work practices do not consistently address these situations and the current
misconception that your “legs do all the work” may, in fact, be an inhibitor of the ability of the back
muscles to react in an unexpected situation.
8. Because of the multi-factorial nature of the risk factors associated with MSI, initiatives should
continue to examine methods to reduce the physical demands of nursing tasks through environmental,
psychosocial and individual intervention strategies.
Back to Health: Final Report
Work Health Foundation
page 51
REFERENCES
Cust G, Pearson JCG, Mair A (1972). The prevalence of low back pain in nurses. International Nurses
Review, 19, 169
Engels JA, van der Gulden JW, Senden TF, van’t Hof B (1996). Work related risk factors for
musculoskeletal complaints in the nursing profession: results of a questionnaire survey. Occupational &
Environmental Medicine, 53(9), 636-41.
Estryn-Behar M, Kaminski M, Peigne E et al (1990). Strenuous working conditions and musculo-skeletal
disorders among female hospital workers. International Archives of Environmental Health, 62, 47 – 57.
Glazner, L.K., Yaloff, F., Forsyth, M., Morris, G., & Roggenburg, M.P. (1993) Back Health:
Development of a Risk Assessment Tool. AAOHN Journal, 41(6), 289 – 292.
Green, L.W. & Kreuter, M.W. (1991). Health Promotion Planning: An Educational and Environmental
Approach (2nd ed.). Mountain View: Mayfield.
Health Canada (1992). Making a Difference II: The impact of the Health Promotion Directorate’s social
marketing campaigns 1991-1992.
Healthcare Benefit Trust (1996) Trends: Plan Administration Data Report. Annual Report
Josephson M, Lagerstrom M, Hagberg M & Wigaeus Hjelm E (1997). Musculoskeletal symptoms and
job strain among nursing personnel: a study over a three year period. Occupational and Environmental
Medicine, 54, 681-685.
Josephson M, Vingård E, MUSIC-Norrtälje Study Group (1998). Workplace factors and care seeking for
low-back pain among female nursing personnel. Scandinavian Journal of Work Environment and Health,
24(6), 465-472.
Larese F, Fiorito A (1994). Musculoskeletal disorders in hospital nurses: a comparison between two
hospitals. Ergonomics, 37(7), 1205 - 1211.
Mandel JH, Lohman W (1987). Low-back pain in nurses: the relative importance of medical history,
work factors, exercise and demographics. Research in Nursing Health, 10, 165-170.
Niedhammer, I, Lert, F., Marne MJ (1994). Back Pain and associated factors in French Nurses.
International Archives of Occupational and Environmental Health, 66, 349-357.
Smedley J, Egger P, Cooper C, Coggon D (1995). Manual handling activities and risk of low back pain
in nurses. Occupational and Environmental Medicine, 52, 160-163.
Snook, S.H. (September 1987). Approaches to the Control of Back Pain in Industry: Job Design, Job
Placement and Education/Training. Spine: State of the Art Reviews, vol. 2(1), 45-59.
Workers’ Compensation Board of British Columbia. (December 1996) WorkSafe Focus Report on the
Health Care Industry
Back to Health: Final Report
Work Health Foundation
page 52
APPENDIX A
Strategic Communications Plan
Back to Health: Final Report
Work Health Foundation
page 53
STRATEGIC COMMUNICATIONS PLAN
1. Problem
•
•
High incidence of MSI among caregivers
Majority of MSI incidents are back injuries that occur while lifting/transferring
patients
2. Goals & Objectives of Campaign
1.
Increase awareness of health and safety issues in the workplace
2.
Promote the use of safe work practices
3.
Decrease # of injuries, and increase health & productivity of employee
3. Research/Interview
•
Hospital Action Committee Meetings
(focus group of caregivers and OHS representative)
4. Target Audience(s)
Primary Audience
A. Front-line patient caregivers (RNs, LPNs, LTCAs)
Secondary Audience B. Nursing Supervisors/Managers
5. Communications Objectives for Each Audience
A. Front Line Patient Care Providers
1. Value of teamwork in health and safety of nurses
•
includes elements of respect, support, communication
•
specifically important when there is a need for 2-person procedure
2. Importance of following safe lift and transfer procedures (standard & principles)
•
“expert” refresher, peer support, champions, mini-teams
•
what to do in non-ideal situations
•
proactive thinking saves your back
3. Importance of Caring for the Caregiver
•
need to look out for yourself and your co-workers, because no-one else
will
•
importance of fitness, warm-up
•
availability of EAP to deal with stress on the job (?)
4. Promoting Ergonomic Factors in thinking
•
stay within your safe work zone
•
important to change work environment to make it safer for you
B. Nurse Supervisors/Managers
Back to Health: Final Report
Work Health Foundation
Appendix A page 1
1. Update them regularly so that they are aware of campaign and its key messages.
Encourage them to promote the messages.
6. Communications Strategy
-- Fun, simple, straight-forward
1.
2.
3.
4.
5.
6.
Communications to be delivered to hospital units for each direct patient caregiver
Structured in game-like fashion with unit participation and personal rewards as
incentives
Newsletters promoted via activity card (attached at the bottom) submission for
incentives
Posters up around unit
Communication with supervisors and management to encourage
participatory/action to increase involvement
Attempt to identify assistants at unit level (unit clerk)
7. Messages
Theme 1: Be INVOLVED
è Promote general awareness of the campaign and its collection boxes and activity
cards.
Poster
•
Too many patient/resident care providers experience back pain and injury. Safe
work practices will reduce your risk of injury.
•
Watch for upcoming themes of Caring for the Caregiver, Modifying your work
environment, Decision Making, Teamwork.
•
1. Participate with your team, 2. Fill in your activity card, 3. Wear a sticker.
Newsletter
•
Move with Care: BE BACK SAFE. This is a pilot research project; the goal is to
raise awareness and to promote the prevention of musculoskeletal injuries in the
workplace. Campaign designed to promote activities. Will continue to August
1998
•
Why do this? Too many patient/resident care providers experience back, neck
and shoulder pain. Be BACK SAFE Campaign designed to promote safe work
practices which will reduce the risk of injury.
•
What you can expect? 8 months, 4 more newsletters, themes, activity cards,
collection box
•
Basic Back-saving Tips (8)
Activity Card
•
Initiate thinking and sharing of information about own back pain experience.
•
1. Wear a sticker with your work group. 2. Your experience with back pain. 3.
Your back safety tips. 4. Share experience with others.
Back to Health: Final Report
Work Health Foundation
Appendix A page 2
Incentive
•
‘We are back safe’ banner and recognition in hospital newsletters.
Theme 2: Care for the Caregiver
è Promote mentality that you need to care for yourself while caring for your patients.
Poster
•
On shifts like this…don’t forget about yourself …Care for the Caregiver.
(humour)
•
Ready – yourself for your shift
•
Recognize – your limits
•
Request – help when needed
•
Recharge – on your breaks
•
Retain – sense of humour
Newsletter
•
Change is taking place at an increasingly rapid rate. Being overwhelmed with
multiple responsibilities means we put our own needs last on the list, resulting in
poor health, fatigue and low energy.
•
Remember the 5 R’s
•
1. Participate with your team, 2. Fill in your activity card. 3. Wear a sticker
•
Are you being good to yourself? A QUIZ
•
Care for the Caregiver Tips
Activity Card
•
Awareness of project
•
Read the newsletter
•
Answer the quiz
•
Posters
•
Comic Caption
Incentive
•
Free Massage (draw)
Theme 3: Murphy’s Law of Planning Patient Transfer
è Promote the thinking process that is involved in assessing patients before every
transfer
Poster
•
Expect the Unexpected
•
Reassess the patient/resident: Is the patient/resident a reliable partner in the
transfer?
•
Consider safer transfer methods: Are you comfortable with the recommended
transfer method?
Back to Health: Final Report
Work Health Foundation
Appendix A page 3
•
Organize your area and team: Is the working area clear? Is your team
synchronized?
Newsletter
•
Unexpected or sudden move while transferring patient/resident can cause injury.
75% of all injuries occur during transfer. Good preparation and planning helps
reduce the risk.
•
Step 1: Assess & Reassess the patient/resident
•
Step 2: Check the Care Plan & Plan your transfer
•
Step 3: Organize your work area and Transfer Team
•
Basic principles for Transferring a Patient/resident (Starting Position, Good Bond,
Smooth & Steady, Communication)
•
1. Participate with your team, 2. Fill in your activity card. 3. Wear a sticker
Activity Card
•
Read the newsletter
•
Posters
•
Awareness
•
Do you use checklist for assessment?
•
Puzzler
Incentive
•
Transfer Belt (draw)
Theme 4: Teamwork
è Promote the concept of effective teamwork in the prevention of MSI.
Poster
•
Teams “individuals working together to achieve a common goal”
•
Keys for Success
•
plan ahead
•
establish a leader
•
form a clear strategy
•
communicate throughout
•
move in unison
Newsletter
•
It is often the case that you need to get the help of a co-worker to complete your
work safely. It is important to remember that you need effective leadership and
communication or one person may end up bearing more of the load than she/he
expected.
•
Keys for success
•
1. Participate with your team, 2. Fill in your activity card. 3. Wear a sticker
•
Are you a team player? A QUIZ.
•
Teamwork Tips
Back to Health: Final Report
Work Health Foundation
Appendix A page 4
Activity Card
•
Read the newsletter
•
Answer the quiz
•
Posters
•
What does your team look like?
Incentive
•
Tim Horton’s coffee (team with highest participation)
Theme 5: Ergonomics
è Cancelled due to lack of participation by hospitals and to ensure enough time for data
collection.
8. Communication Tools
•
•
•
•
•
•
11x17 Posters
Legal size Newsletter/Activity Cards
Collection Boxes
Logo Stickers
Hospital newsletters (bi-weekly submission)
presentation and e-mails to management
9. Focus Test Tools & Messages
•
Hospital Action Committee Meetings
10. Evaluation of Results
•
Research Questionnaire
Back to Health: Final Report
Work Health Foundation
Appendix A page 5
APPENDIX B
Activity Card Comments
Back to Health: Final Report
Work Health Foundation
page 54
Theme #1 BE INVOLVED
Pre-test/Intervention Hospital
•
•
71 activity cards were collected and 55 stickers were counted on the collection boxes out of
403 F/T and P/T employees (casuals were not included in calculation of percentages). This
results in a hospital wide participation rate of 18% for the activity cards and 13% for the
stickers.
660 newsletters and stickers were distributed to the hospital units, 366 newsletters were
returned unread.
PARTICIPATION RATES BY UNIT
(out of 403 F/T, P/T employees)
Activity Cards
Stickers
•
•
0%
1-9%
4
6
4
6
1019%
6
1
2029%
1
2
>30%
5
5
From collecting the boxes it seems that nurses are not picking up the newsletters from the
boxes. The low participation rates may be due to the lack of information getting to the nurses
at all. For the first theme, there was no designated individual that was responsible for
distributing the newsletters; they were simply left on the unit with the charge nurse. Most
boxes were displayed prominently on the unit or in the break room.
Many tips were submitted on the activity cards, a summary of which is included.
No Pre-test/Intervention Hospital
•
•
84 activity cards were collected and 83 stickers were counted on the collection boxes out of
686 F/T and P/T employees (casuals were not included in calculation of percentages). This
resulted in a hospital wide participation rate of 12% for the activity cards and 12% for the
stickers.
820 newsletters and stickers were distributed to the hospital units, 413 newsletters were
returned unread. Additionally, 13 posters were returned that were not posted.
PARTICIPATION RATES BY UNIT
(out of 686 F/T, P/T employees)
Activity Cards
Stickers
•
•
0%
1-9%
2
11
8
1
1019%
5
2
2029%
4
2
>30%
2
5
From collecting the boxes it seems that nurses are not picking up the newsletters from the
boxes. The low participation rates may be due to the lack of information getting to the nurses
at all. For the first theme, there was no designated individual that was responsible for
distributing the newsletters, they were simply left on the unit with the charge nurse. Most
boxes were in the break room. There is a considerable lack of space on most units at SMH,
as a result it was difficult for most units to place it in a prominent area.
Many tips were submitted on the activity cards, a summary of which is included.
Back to Health: Final Report
Work Health Foundation
Appendix B page 1
Theme #1 BE INVOLVED
Pre-test/Intervention Hospital
Your Tips to make your work easier on your back. (61 Responses Cards Collected)
POSTURE/BODY/LIFTING MECHANICS
• use good body mechanics *********
• use legs to protect back, bend with my knees, “lift with your legs” **************
• avoid over reaching ****
• I put my lt. or rt. foot up on bottom of bed rail when feeding resident. Stand with foot on
stool. ***
• I keep good posture at all times ***
• push instead of pull, never pull **
• sit with back straight and raise one foot when sitting **
• Follow Smart Moves Program at PAH (annual review of Smart Moves for employees, I
suggest!) *
• have wide base of support when lifting patients *
• hold objects close to you *
• place one knee on the bed. This prevents me from bending and stretching incorrectly. *
• use momentum to help with transfers
• keep your back straight
• knees bend and attempting to keep back straight when helping moms to breast feed
• raise patients legs in bed to prevent drag
• don’t hold on/lift up someone who is falling – let them slide
• Second floor stall are required to attend codes. When doing CPR it is often impossible to get
up on the bed to do chest compressions & a footstool is required for standing on. This is very
hard on the back & compressions are not as effective. Lowering the beds would be helpful
i.e. ER’s beds.
• Lift heads of stretchers with both arms rather than one.
• roll head of bed up before sitting patient up
• elevate bed to slide off when standing patient (we need wheelchairs that can be elevated so
we don’t have to pull patients to standing)
• when on the phone don’t cradle the receiver on shoulder
CARE FOR CAREGIVER
• going to the gym twice weekly workout specific to old injury area for strengthening. I work
out at a gym 3-4 times a week. If I didn’t, I don’t think I would be able to perform my job
properly. Keep back and stomach muscles in shape. Regular exercise, especially sit-ups.
***********
• stretching before start work (5-10 minutes should be provided officially to the workers for
stretching before start of shift). I do my exercises on the way to work making sure I am
warmed up before work . Stretch frequently throughout the day *****
• bed rest, medication, stretching exercises. Anti-inflammatory, ice *
• wear proper shoes *
• working 5 or 6 nights in a row is inhumane to one’s back (with two people). No wonder
there are so many WCB.
Back to Health: Final Report
Work Health Foundation
Appendix B page 2
Theme #1 BE INVOLVED
•
•
•
visit a chiropractor once a month
keep my weight in order
stop and do pelvic tilting or rocking several times an hour
ERGONOMICS/WORK PRACTICES
• put bed to workable level to avoid bending while doing care. Raise bed up. **************
• use mechanical lift.************
• use transfer belts ******* (hospitals should provide support belts for all staff members)
• put down side rail *****
• make sure the space is uncluttered to avoid falling or tripping over things. Be aware of
hazards on the floor *
• wear a lifting belt when back is really sore. *
• use proper equipment for lifts
• use a lifting sheet
• have asked for transfer board
• alternate heavy and light work
• rest back whenever able ie in breaks
• I find it difficult at times when we have many bed and other furniture moves to accommodate
patients even though 2 persons involved – any solution to this dilemma?
• use stool to sit on while starting I.V.s **
• use a back supportive chair to sit and do charting
• try to sit while interviewing clients
TEAMWORK
• get help when unable to manage by myself , when in doubt as to resident transfer à use lift
or 2 person transfer. Get help when I need it. ********************
• work as a team. Work with a buddy *****
• always let your partner know what you are trying to do, communicate **
• work with or turn patients with co-worker with same height. Work with a co-worker who is
approximately the same height and strength *
DECISION MAKING
• always assess residents on a daily basis
• plan lifts
• common sense
Back to Health: Final Report
Work Health Foundation
Appendix B page 3
Theme #1 BE INVOLVED
No Pre-test/Intervention Hospital
Your Tips to make your work easier on your back. (77 Responses Cards Collected)
POSTURE/BODY/LIFTING MECHANICS
• Proper lifting techniques *
• Always bend knees, keep back straight when lifting (Use legs not
back)************************
• Good body mechanics ****
• Push instead of pull ******
• Keep weight close to body
• Shoulders, feet, hips facing forward, do not twist *
• Try to keep own arms close to body
• Not bending back over patient
• Standing on one foot alternating stool or side of bed ****
• Put knee on bed while turning resident***
• If patient able to be up on commode – after they are finished, I release the brakes and move
commode to the head of the bed. Side rail down bed made flat. Brakes on commode,
Transfer to bed, therefore they are in the highest position in bed, no need to lift again.
• Patient in reverse trendelenberg to lift up in bed **
• Pelvic tilt to relieve back pain/rest back *
• Squat at knees when rolling head of bed up or down
• Be aware of posture
• Work with shoulders back, stomach in, head held straight *
• Keep tummy tucked in as much as possible to place less strain on my back
• Bend forward when lift
• Turn patient in ½ turns
CARE FOR CAREGIVER
• Do exercises during work day, do exercise outside work time *************
• Do some stretching before work ********** (getting up and moving around)
• Take your time when giving care, don’t rush ****** (Ensure adequate staff)
• Wear the proper footwear **
• Feet up on break and at home
• Proper diet
• Adequate sleep
• Sleep on side not stomach
• Regular visits to massage therapist
• If you feel aches in your back stop and rest and don’t continue by yourself
• Smile and do your move with caution
• Be good to yourself
• Take time to void when nature calls (full bladder – more pressure on back)
• Nursing team has been participating faithfully and with great spirit in our morning warm-up
stretching exercises.
Back to Health: Final Report
Work Health Foundation
Appendix B page 4
Theme #1 BE INVOLVED
•
Staff were pilot unit for mechanical lifts & continue to enthusiastically support & advocate
these initiatives.
ERGONOMICS/WORK PRACTICES
• Raise bed to start IVs, etc. ******************* (Adjust bed height for nursing comfort)
• Put side rails down when turning a patient *******
• Wipe up spills on floor, watch for tripping & slipping hazards ******
• Sit in supportive chair when possible (i.e. doing patient admissions) *****
• Avoid prolonged sitting and standing, when I am feeding patients I sit on the chair, then
standing, vary body position *
• Alternate light and heavy work * (take breaks/trade tasks)
• Use mechanical lifts ************
• Use transfer belts ****
• Lift sheets for repositioning patients **
• Use blue transfer boards for unconscious patients, bed – bed transfer
• Roll the whole bed up when washing a patients.
• Ensure breaks on bed when moving patient up in bed *
• Use carts to move heavy articles
• Tip: put a larger plastic bag under a heavy or awkward patient for easier slide up in bed.
• With the beds we have the back injury should be less, still have 5 beds that are “killer” as
they are the old crank style and if they don’t get your back , then they get your wrist and
shoulders.
TEAMWORK
• Don’t lift patient that is too heavy by yourself, get help to move patients, wait for assistance
******************************
• Communicate with partner ***
• Know your limits *
• Ask patient to help when able
• Work as a team, work in 2’s *
DECISION MAKING
• Never start a lift unless both of you are completely ready
• Always follow ADL chart for proper lift *
• Get physio. to assess transfer prior to first time
• Think before you lift
Back to Health: Final Report
Work Health Foundation
Appendix B page 5
Theme #2 CARE FOR THE CAREGIVER
Pre-test/Intervention Hospital
•
•
•
54 activity cards were collected and no new stickers were counted on the collection boxes out of 403
F/T and P/T employees (casuals were not included in calculation of percentages). This results in a
hospital wide participation rate of 13.4% for the activity cards and 0% for the stickers.
The overall participation rate for the hospital has decreased compared to Theme #1 by 4%, 7 units
increased their participation, 11 units decreased their participation and 1 unit maintained the same
participation rate. Also, there does not seem to be any interest in wearing the stickers. The first
theme involved a sticker day (I don’t believe this continued)
590 newsletters and 55 stickers were distributed to the hospital units; 383 newsletters were returned
unread. (227 newsletters picked up)
PARTICIPATION RATES BY UNIT
(out of 403 F/T, P/T employees)
Activity Cards
Stickers
•
•
0%
1-9%
2
21
5
0
1019%
7
0
2029%
1
0
>30%
4
0
Again I noticed a problem in that the nurses are not aware of the campaign. They do not seem to
read the Making it Happen and have not had mention of the campaign in staff meetings. Attempts
have been made to designate an individual to inform the nurses when the newsletters arrive, but it
seems like there is not much time or attention paid to the information.
Several Humour Captions and some feedback comments on the material were collected via the
activity cards, a summary of which is attached.
No Pre-test/Intervention Hospital
•
•
•
43 activity cards were collected and no new stickers were counted on the collection boxes out of 686
F/T and P/T employees (casuals were not included in calculation of percentages). This results in a
hospital wide participation rate of 6.2% for the activity cards and 0% for the stickers.
The overall participation rate for the hospital has decreased compared to Theme #1 by 6%, 2 units
increased their participation, 14 units decreased their participation and 6 unit maintained the same
participation rate. Also, there does not seem to be any interest in wearing the stickers. The first
theme involved a sticker day (I don’t believe this continued)
805 newsletters and 435 stickers were distributed to the hospital units, 666 newsletters were returned
unread. (139 newsletters picked up)
PARTICIPATION RATES BY UNIT
(out of 686 F/T, P/T employees)
Activity Cards
Stickers
•
•
0%
1-9%
7
21
8
0
1019%
5
0
2029%
0
0
>30%
1
0
Again I noticed a problem in that the nurses are not aware of the campaign. Attempts have been
made to designate an individual to inform the nurses when the newsletters arrive, but it seems like
there is not much time or attention paid to the information.
Several Humour Captions and some feedback comments on the material were collected via the
activity cards, a summary of which is attached.
Back to Health: Final Report
Work Health Foundation
Appendix B page 6
Theme #2 CARE FOR THE CAREGIVER
Pre-test/Intervention Hospital
Suggested humour captions
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Bend Down, Ben Brown
The woman having a baby wants something
for pain
This ought to make him sleep for a month!!
The most prominent and followed
“commandment” in healthcare nowadays
“…just turn the other cheek!”
I couldn’t find a bigger needle
Well, he has been a pain in the ass….
Bend over I think I know you!
One shot and you’re good for the whole day
You think this is big?? You should see the guy getting it.
You want it where??!*
Right or Left cheek?
I’ve got some vitamins here to help the man in 629B get his strength back.
Don’t be wimpy it’s just a little needle.
It’s like having a bee sting!
I couldn’t find anything smaller will this do?!
It’s a muscle relaxant for the back care program
Oh Boy. It sure works for a 300 pounder
Whoever said there was a blood shortage, wasn’t doin’ it right!
Feedback on material
•
Newsletter
• Informative and Educational
• Informative
• Makes Sense
• Very informative
• I liked
• very nice
•
Quiz
•
•
•
•
Most of the answers were false
Doesn’t getting out of bed daily count as a warm-up (8/11)
Made me realize what I have to do
Posters
• one really helps control my low back pain
• could have more!
Back to Health: Final Report
Work Health Foundation
Appendix B page 7
•
•
•
Theme #2 CARE FOR THE CAREGIVER
Good reminders
Constant reminders
I think, it is helpful – to be back safe
Back to Health: Final Report
Work Health Foundation
Appendix B page 8
Theme #2 CARE FOR THE CAREGIVER
No Pre-test/Intervention Hospital
Suggested humour captions
• Who do want me to scare the crap out of next?
• You said you wanted me to get to the point!
• Doctor, I found out what was causing Mr. Bale’s back
pain!
• Walk softly and carry a big stick.
• Plenty for all!
• Where to next?
• Poor body mechanics
• If this doesn’t put him to sleep I don’t know what will
• This one’s for you
• Hi Herman, do you think this dose is a little heavy?
• I thought you wanted some enthusiasm injected around here
• Are you sure this is a big enough dose? He seems to have gained a few pounds.
• I can’t understand why they never come back for the second shot.
• But Dr. Jones, you said you wanted bloodwork on Mr. Elephant, not Mr. Oliphant.
• It’s a tick
• Ask me how to be back safe!?
• Just a little poke
• I thought that’s what you ordered!?
• That’s gotta hurt?
Feedback
• How can we be back safe with NO “power” Beds and not enough staff
• Newsletter
• good
• very informative
• excellent reminders
• This will help me and my health for future
• Awesome – It is a big help for everybody
• good info
• I think it is excellent
• Keep up the good work. I am doing it too.
• Ready, Recognize, Request, Retain, Recharge
•
Quiz
•
•
•
•
•
•
•
need to focus more on myself – thanks
wonderful ideas not always possible
I had only 7 trues. I know where to improve
exciting… J
I have room for improvement
I got very good scores
Exercise regularly
Back to Health: Final Report
Work Health Foundation
Appendix B page 9
Theme #2 CARE FOR THE CAREGIVER
•
Posters
• good idea
• good reminders
• excellent
• These posters will make staff think twice about themselves
• Good Feeling – It’s good , had wonderful news to all…
• Great campaign
• It’s food to remind everyone to be safe
• very helpful for nurses
Back to Health: Final Report
Work Health Foundation
Appendix B page 10
Theme #3 PLANNING PATIENT TRANSFERS
Pre-test/Intervention Hospital
•
•
•
22 activity cards were collected and no new stickers were counted on the collection boxes out of 403
F/T and P/T employees (casuals were not included in calculation of percentages). This results in a
hospital wide participation rate of 5.5% for the activity cards and 0% for the stickers.
The overall participation rate for the hospital has decreased compared to Theme #2 by 8%, 3 units
increased their participation, 15 units decreased their participation and 1 unit maintained the same
participation rate. Also, there does not seem to be any interest in wearing the stickers.
600 newsletters and 25 stickers were distributed to the hospital units; 480 newsletters were returned
unread. (120 newsletters presumed to be picked up by care providers)
PARTICIPATION RATES BY UNIT
(out of 403 F/T, P/T employees)
Activity Cards
Stickers
•
•
0%
1-9%
10
21
4
0
1019%
3
0
2029%
0
0
>30%
2
0
Again I noticed a problem in that the nurses are not aware of the campaign. They do not seem to
read the Making it Happen and have not had mention of the campaign in staff meetings. Attempts
have been made to designate an individual to inform the nurses when the newsletters arrive, but it
seems like there is not much time or attention paid to the information. Many people now seem to be
anxious for us to get the box out of their way. A couple people even asked “Is this thing not over
yet?”
A few Planning Patient Transfer Strategies and some feedback comments on the material were
collected via the activity cards, a summary of which is attached.
No Pre-test/Intervention Hospital
•
•
•
6 activity cards were collected and no new stickers were counted on the collection boxes out of 686
F/T and P/T employees (casuals were not included in calculation of percentages). This results in a
hospital wide participation rate of 0.87% for the activity cards and 0% for the stickers.
The overall participation rate for the hospital has decreased compared to Theme #2 by 5.5%, 0 units
increased their participation, 12 units decreased their participation and 10 unit maintained the same
participation rate. Also, there does not seem to be any interest in wearing the stickers. The first
theme involved a sticker day (I don’t believe this continued)
720 newsletters and 55 stickers were distributed to the hospital units, 709 newsletters were returned
unread. (61 newsletters presumed picked up by care providers)
PARTICIPATION RATES BY UNIT
(out of 686 F/T, P/T employees)
Activity Cards
Stickers
•
0%
1-9%
16
21
5
0
1019%
0
0
2029%
0
0
>30%
0
0
Again I noticed a problem in that the nurses are not aware of the campaign. Attempts have been
made to designate an individual to inform the nurses when the newsletters arrive, but it seems like
there is not much time or attention paid to the information. Many people now seem to be anxious for
Back to Health: Final Report
Work Health Foundation
Appendix B page 11
Theme #3 PLANNING PATIENT TRANSFERS
•
us to get the box out of their way. A couple people even asked “Is this thing not over yet?” Several
units at Surrey have been relocated, and one unit has even lost their box.
A few Planning Patient Transfer Strategies and some feedback comments on the material were
collected via the activity cards, a summary of which is attached.
Back to Health: Final Report
Work Health Foundation
Appendix B page 12
Theme #3 PLANNING PATIENT TRANSFERS
Pre-test/Intervention Hospital
Mr. A’s Care Plan says “2-person transfer” but his sitting balance is very poor and needs support when
standing. During the transfer one person feels his knees begin to give out.
Puzzler Solutions
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
LIFTING BELT hopefully in use, brace knee if able or abort lift and try again. Always have 2
people
Sit him back down and reassess to use lift
Lower patient to floor. Revise care plan. Use mechanical lift
Lower patient to floor gently, use mechanical lift --> have physio. Reassess to change care plan
Use a mechanical lift after guiding patient to floor
Sit the resident back on the bed, start over using a mechanical lift
Transfer belt. Lower back down safely. Ttalk to O./T. for reassessment / mechanical lift
Block person’s knees with your own
Lower them slowly to the ground using your legs
Reminds me to use proper techniques
Should know this information by now
it’s good help in reminding us to use proper position
Put him back where he started, bed or chair, whatever’s closer. Don’t try to catch or carry him.
Reason for weakness? Go to mechanical if necess.
Sit Mr. A back onto chair and use lift for this and any further transfers. Use chair extra support /
pillows to keep Mr. A upright.
Slowly return him to chair – use a lift
Whose knees give out – the nurse or the patient? Do not rush transfer – get patient to nearest surface
– chair/bed/floor. Should patient be reassessed to mechanical lift?
This person should be a Sara Lift – not just a two person alone
Feedback on material
•
Newsletter
• We should get posters in all rooms to educate visitors & family
• Very Good?
• Very well done
•
Posters
• Good
• I’m not sure if I’ve seen them
• Good message-even children visiting the unit notice it – catchy!
• I think posters are a waste of time and money
•
Awareness 75% of all back injuries occur while transferring patient/resident
• we should always ask someone to help. Not on your own.
• No, but I do now.
• What about confused aggressive patients? Turning them in bed?
Back to Health: Final Report
Work Health Foundation
Appendix B page 13
Theme #3 PLANNING PATIENT TRANSFERS
•
Specific set of questions asked for each assessment?
• Assessment is very important
• I ask that & “where’s the transfer belt” sometimes
• Each patient needs frequent assessment
Back to Health: Final Report
Work Health Foundation
Appendix B page 14
Theme #3 PLANNING PATIENT TRANSFERS
No Pre-test/Intervention Hospital
Mr. A’s Care Plan says “2-person transfer” but his sitting balance is very poor and needs support when
standing. During the transfer one person feels his knees begin to give out.
Puzzler Solutions
• Use a lift?
• Let person slide to floor and then get lift to put back in bed
• Both people bring him to the floor gently by going down with him.
• Reassess transfer status. May need to use a mechanical lift
• Reseat patient / use maxi lift. Referral to PT to reassess
Feedback on material
•
Newsletter
• Good diagrams
• very helpful tips
•
Posters
• none
•
Awareness 75% of all back injuries occur while transferring patient/resident
• none
•
Specific set of questions asked for each assessment?
• N/A in FBU West
Back to Health: Final Report
Work Health Foundation
Appendix B page 15
Theme #4 TEAMWORK
Pre-test/Intervention Hospital
•
•
•
10 activity cards were collected and no new stickers were counted on the collection boxes out
of 403 F/T and P/T employees (casuals were not included in calculation of percentages).
This results in a hospital wide participation rate of 2.5% for the activity cards and 0% for the
stickers.
The overall participation rate for the hospital has decreased compared to Theme #3 by 2.5%,
1 unit increased their participation, 7 units decreased their participation and 11unit
maintained the same participation rate.
600 newsletters and 0 stickers were distributed to the hospital units, 556 newsletters were
returned unread. (44 newsletters presumed to be picked up by care providers)
PARTICIPATION RATES BY UNIT
(out of 403 F/T, P/T employees)
Activity Cards
Stickers
•
0%
1-9%
13
21
5
0
1019%
0
0
2029%
0
0
>30%
1
0
A few Teamwork Drawings and some feedback comments on the material were collected via
the activity cards, a summary of which is attached.
No Pre-test/Intervention Hospital
•
•
•
27 activity cards were collected and no new stickers were counted on the collection boxes out
of 686 F/T and P/T employees (casuals were not included in calculation of percentages).
This results in a hospital wide participation rate of 3.9% for the activity cards and 0% for the
stickers.
The overall participation rate for the hospital has increased compared to Theme #3 by 1.0%.
The primary reason for the increase in that one unit decided to all get together and fill in 19
cards. 5 units increased their participation, 2 units decreased their participation and 14 unit
maintained the same participation rate. Also, there still does not seem to be any interest in
wearing the stickers.
720 newsletters and 0 stickers were distributed to the hospital units, 668 newsletters were
returned unread. (52 newsletters presumed picked up by care providers)
PARTICIPATION RATES BY UNIT
(out of 686 F/T, P/T employees)
Activity Cards
Stickers
•
0%
1-9%
15
21
3
0
1019%
1
0
2029%
1
0
>30%
1
0
A few Teamwork Drawings and some feedback comments on the material were collected via
the activity cards, a summary of which is attached.
Back to Health: Final Report
Work Health Foundation
Appendix B page 16
Theme #4 TEAMWORK
Pre-test/Intervention Hospital
What does you work team look like?
• 6 drawings submitted, most quite funny
Feedback on material
•
Newsletter
• They’re great
• Drawing pictures of staff members is definitely NOT something R.N.’s have time for.
Most injuries occur because of workload problems.
No Pre-test/Intervention Hospital
What does you work team look like?
• 22 drawings submitted, most quite funny
Feedback on material
•
Newsletter
• excellent reminders
• what a waste of time! x 2
Back to Health: Final Report
Work Health Foundation
Appendix B page 17