annotation - The Bone & Joint Journal
advertisement

ANNOTATION
SPINAL
A constant
and worrying
surgery
is growth.
This
at
factor
in children’s
occurs
different
in three
same
time,
body,
utero
for two decades
or more
and during
adolescence.
rates
in
orthopaedic
dimensions
different
at the
parts
of
with increased
Growth
may
malunited
fractures
by allowing
remodelling
limits
of acceptability,
but on the other
militate
against
improvement,
particularly
of early
onset.
The
notorious
tendency
Both
conservative
are
treatment
used
to
from wide
hand
it may
in deformity
of club
foot
and
counter
the
spinal
effects
attention
has
been
Nonetheless,
been
clarified
paid
over the years,
; knowledge
understanding
facts
behaviour
ofspinal maturity.
deformities
cease
to
in scoliosis
surgery,
In the
after
is no
to the
little
have
to an
that
from
the
ossification
while
Adams
essay
attainment
of the
apophysis
stated
detailed
study
children
Robert
(1962)
Jones
was
Gold
femoral
growth,
and
stopped
growing
in girls
years
of
limb
respectively
respectively,
and
He
showed
that
growth
in quarters.
referring
to their
Risser
and
scoliosis
and
had formerly
when
the ossific
spine.
This
surgeons,
readily
patient’s
Ferguson
with
which
iliac
Scoliosis
of maturity,
status
reported
Risser
More
evidence
of
of the
has
girls
at an average
age
iliac
Other
4. In 1936
and
authors
the vertebrae
supported
assess
maturity
(Clarisse
the method
was quickly
(Zaoussis
and
the use of these
1974;
adopted
Heine
and Reher
and is now widely
1958).
to
1975);
used.
Follow-up,
however,
did not extend
far into the postmature
phase
and failed to provide
direct
evidence
of the
690
the
and
normal
and
femur
of 13.7 and
trunk
beyond
14.2
I 5.4
was
not
years
finished
the end point
in
of his
favour
maturity.
Leatherman
scoliosis
attainment
which
of
the
Ponseti
and
of 600 or more were
(Collis
and Ponseti
(1976)
had
ofgeneral
In these
found
10 cases
radiographs
skeletal
cases
taken
maturity
the
to 60#{176}
after
initial
and
mean
a mean
also
curve
interval
of
after
some
of 44#{176}
of six years.
from 40#{176}
at the age of 20 years to
at the age of 33 years.
These
observations
were
confirmed
by others
and it was noted
that adults
could
lose as much
as 24 cm in height
as a result of progression
950
spinal
deformity
(Stagnara,
Gonan
and
Fauchet
by some that this progression
was
or some
mysterious
soft-tissue
factor,
evidence
was
provided
(Hassan
and
It was suggested
due to pregnancy
although
little
when
he
and noted
in the
James
Dickson
1984).
of 14 years
apophyses
1969).
idiopathic
of
superior
and
crest
tibia
accumulated
curves
One curve had increased
system,
300 children
1 5.5 for boys.
James
(1954)
confirmed
this end
point
studied
his patients
with idiopathic
scoliosis
that
apophyseal
fusion
occurred
synchronously
for
for some
the posterior
that
had
and
Friedman
(1950)
reported
that curves
progressed
about
10 per year
in adulthood,
while another
report
from Iowa
demonstrated
that the average
increase
in curve
after
that
curve
progression,
lO per month,
stopped
reached
occurred
as, say,
the
sex by the age of 16 years,
progression
the
this
on almost
observed
averaged
nucleus
eager
adopted
in his
and
in
1 5.5 and
progressed
crest
growth
at
had
iliac
measurement
too
by the award
of the
measured
tibial
and
in boys
later.
by considering
informative
ages
years
be quantified
quite
of the
slowly”,
to estimate
at the mean
and
while
spine
recognised
Medal.
ilium.
can
to
art”. He observed
that the curves
progressed
after
their
maturity
maturity
was 15#{176},
and that curves
particularly
likely
to deteriorate
process
come
“distortion
advances
“it is impossible
ofthe iliac crest (Risser and Ferguson
1936; Risser 1958).
Ossification
of the apophysis
first appears
in the region
of the anterior
superior
iliac spine and then spreads
posteriorly
and medially
until the whole apophysis
is
ossified.
During
the next year the apophysis
fuses to the
This
growth
highly the importance
of studying
the natural
progress
of
any disease
as it pursues
its course when not interfered
of
maturity
previously
the
in his wonderfully
(1865),
on scoliosis,
and
study.
spinal
skeletal
had
different
conclusions,
observing
that
spine is never stationary
but always
in either
work has been directed
towards
of this time. Risser, a pioneer
demonstrated
be assessed
the
that
(1864)
fusion
could increase
at any age. Calvo
(1957) observed
spinal growth does not stop when the iliac apophyses
completed
their ossification.
Tupman’s
important
deformities.
belief
Broadhurst
apophyseal
is
growth.
points
crucial
of spinal
progress
skeletal
maturity,
much
the accurate
identification
of spinal
many important
of these
is
of the
The assessment
could
to the
itself.
with by medical
scoliosis
patients
growth;
when this has ceased progression
of the deformity
longer important.
Yet despite
much effort directed
amelioration
of the unfavourable
effect of growth,
between
of
fusion
of
relationship
of the spine
the
rates in
benefit
deformity
to relapse, despite treatment,
is one example
the unfortunate
effect of growth ; but for unpredictability
during
development
the most
difficult
deformity
scoliosis.
operations
GROWTH
Bjerkreim
1983;
Vertebral
growth.
Weinstein
and
Vertebral
Ponseti
growth
1983).
occurs
in a similar
fashion
as growth
in the long bones (Haas
1939). Increase
in length
and change
in shape
takes
place
as a result
of
activity
in the
physeal
growth.
In the
vertebrae,
growth
cartilage
lies
body and
between
the tissues
the
roles
plates,
of the
being
being
between
ofthe
THE
there
there
the
bone
of
intervertebral
vertebral
JOURNAL
no interstitial
no bony
ring
OF BONE
epiphyses,
the
disc.
apophysis
AND
JOINT
vertebral
Confusion
and
the
SURGERY
691
ANNOTATION
physeal
plate
and Copel
persist
careful
growth
studies
(Bick
1950, 1951).
The
peripherally
vertebral
ossified
plate,
the
at
despite
ring
part
apophyses
are
of the cartilaginous
attachment
of
beyond
the perichondrial
with
the vertebral
body
ring
long
ligament
(Figs
before
merely
the
vertebral
or
periosteum
1 and 2). They fuse
the end of spinal
about
the
attainment
skeletal
maturity,
they
bear no relationship
to spinal
growth
or its cessation.
course,
because
the vertebral
growth
plates
are
present
until
an average
age of 25 years,
this does
imply
that significant
longitudinal
growth
continues
occur
until
this
demonstrated
that
.
Fig.
of general
time.
Indeed,
vertebral
it
bodies
has
been
are half
Of
still
not
to
clearly
the adult
size
.
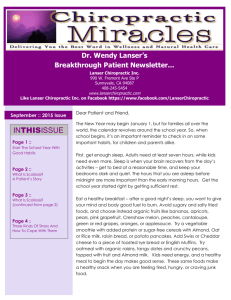
Fig.
1
2
1 - Lateral
radiograph
of thoracic
vertebrae
showing
the step-like
recesses in the upper and
margins of the ossific vertebral
body which are due to the cartilage
of the vertebral
epiphyseal
plates.
Figure
2 - Lateral
radiograph
showing
the vertebral
apophyses
: regions of ossification
at the
sites of ligamentous
insertion.
Note that these are outside
the vertebral
epiphyses.
Figure
lower
growth.
Bick
takes
no
clearly
part
ossification
in
have
showed
that
longitudinal
any
relationship
the
ring
by the
apophysis
growth,
nor
does
to this growth.
its
He
observed
that calcification,
and later ossification,
in the
ring
apophysis
lies outside
the plane
of the physeal
growth
plate
and that
apophyseal
fusion
occurs
over
several
years with different
timing
in different
regions
of
the spine.
If the term “traction
apophysis”
were used, as
suggested
by
Bick,
then
growth
plate
would
not
been
confirmed
(Larsen
confusion
arise.
and
with
the
These
observations
Nordentoft
1962)
physeal
have
and a
histological
study
of the cartilaginous
end-plates
from
birth
to 73 years
of age has demonstrated
that growth
cartilage
is present
but decreasing
in width
until
the
patient’s
age is well
into
the twenties
(Bernick
and
Cailliet
secondary
1982).
Since
the
vertebral
centres
of ossification
as
bones,
there
is no
and
so demonstrate
epiphysis
the
to fuse
obliteration
cartilage
which
is seen at the
elsewhere
in the skeleton.
Therefore
while the status
crest
VOL.
and
69-B.
vertebral
No.
ring
5. NOVEMBER
time
with
the diaphysis
of the
growth
of skeletal
of ossification
apophyses
1987
bodies
have
no
is the case in long
may
say
maturity
age
occurring
of two
after
the
years,
age
with
little
of 10 years
longitudinal
(Haas
growth
1939,
Bick
and
Copel
1950; Larsen
and Nordentoft
1962; Bernick
and
Cailliet
1982).
Nonetheless,
while
the end-plates
are
open,
time for change
in shape
is available.
This may be
oflittle
importance
in the symmetrical
spine,
but may be
crucial
in the presence
of a structural
scoliosis,
which
is
subject
1984).
to enormous
It would
hormonal
progression
stopped
factors
in early
asymmetrical
therefore
be
forces
unwise
or pregnancy
adult life when
(Dickson
et al.
to postulate
as causes
the spine
of curve
has not yet
growing.
Although
estimated
twenties”,
determination.
Assessment
the
time
of spinal
no more
accurately
there
is little
point
of growth.
maturity
than
in
of the iliac
something
cal
always
recorded,
be
midexact
is to
particularly
during
velocity
heralds
the
danger
of curve
progression.
While
some
can be gleaned
in this respect
from the Risser
are many more accurate
methods
available.
although
thus
the
its
What is much more important
discover
how scoliotic
children
grow,
adolescence
when
increased
growth
age,
can
“during
effort
at
information
scale, there
Chronologi-
is a notoriously
ANNOTATION
692
inaccurate
measure
of true biological
age.
Fifty
years
ago in Cleveland
growth
studies
on
normal
children
were performed
and, in particular,
the
development
of the bones of the left hand and wrist were
estimated
radiographically
(Todd
work
formed
the basis
atlas,
against
whose
ance
of
Measurement
more
the
basis
of
does
biological
therefore
cal
were
and
Pyle
radiographic
formed
not
fulfil
all the criteria
age
is assigned
for a certain
to the
a consistent
tendency
previous
year:
to under-rate
Bick
method,
currently
no objection
hand
and wrist
children.
If the
biological
there
is
so that
going
is
this
longitudinal
through
for
ratings
standing
(Tanner
radiographs
are
the same
of the pelvis
technique
dosage
low-dose
Conclusions.
in the
subject
to
Clarisse
P. Prognostic
in
ossification
apophyses
The
best
and
method
of bone
ratings,
and
years
the progress
and
of
assessing
that
than
longitudinal
crest
the
of the
growth
of scoliosis
lower
the spine
limbs.
is marginal
should
not
The
; but
the
ROBERT
P. Deacon,
Department
Leeds
L59
MA,
BSc,
ChM,
FRCS,
of Orthopaedic
7TF,
England.
FRCS,
Senior
of
Professor
of Orthopaedic
an
puberty
grows
for
effect
on
effect
on
DEACON
Surgery
St James’s
University
Hospital,
J Bone
Surg
JO,
London
: John
spine
mineures
de lO
Lyons : Claude
length
Press,
of
Joint
Surg
Acta
Arch
in
Surg
1939:38:245-9.
idiopathic
Orthop
Scand
scoliosis
der unbehandelten
Skoliose
Z Orthop
EL. Growth
ofthe
after
1983,54:88-90.
diagnosis
the age
epiphyses
nach
1 975 : 1 13:876-9.
and operative
at onset.
J Bone
and vertebra.
Ada
1962:32:210-7.
IV, Friedman
[Am]
pathogenesis
J Bone
1959.
of vertebrae.
scoliosis
: the prognosis,
related
to curve
patterns
and
[Br] l954:36-B:36-49.
Scand
changing
atlas of skeletal
derelopment
a/the
: Stanford
University
Press:
and
I. Progression
EH, Nordentolt
in adults:
:729.
asymmetry.
Idiopathic
B. Prognosis
in idiopathic
scoliosis.
J Bone
Joint
l950,32-A:381-95.
Risser JC. The iliac apophysis
: an invaluable
1958:1 1 :1 1 1-9.
of scoliosis. Clin Orthop
JC,
vertebra.
Surg
[Am]
female
adolescent
1957:10:40-7.
1976:58-A
spinal
University
in
treatment.
indications
Joint Surg
Risser
ed.
IA, Butt WP. The
Archer
J, Reher H. Die Progredienz
Poliomyelitis
bis Wachstumsabschluss.
(Eng.
Abstr.)
Orthop
vertebra
: a
Surg
[Am]
human
Joint
2nd
deformity
[Am]
biplanar
I, Bjerkreim
Larsen
of human
of patients
with idiopathic
Bone
Joint
Surg
lAm]
J
KD. Spinal
Joint
Oxford
JIP.
aging
:425-45.
SL. Growth
Ferguson
AB. Scoliosis
sign
: its prognosis.
in the
management
J Bone
Joint
Surg
1936:18:667-70.
Stagnara
P, Gonan
G-P,
Fauchet
P. Surgical
treatment
rigid
lumbar
scoliosis
in the adult.
In : Dickson
RA,
eds. Management
ofspinal
deformities.
Butterworths
Medical
Reviews:
Orthopaedics
2. London
etc:
l984;303-21.
of idiopathic
Bradford
DS,
International
Butterworths,
JM, Whitehouse
RH. Height
standard
chart.
Castlemead:
Creaseys,
1975.
Tanner
JM, Whitehouse
RH, Cameron N, Marshall WA, Healy MJR,
Goldstein H. Assessment
of skeletal
maturity
and prediction
of
Tanner
adult
1983.
Todd
height
(TW2
method).
TW. Atlas ofskeletal
Kimpton,
1937:137-203.
Tupman
GS.
relationship
1962;44-B
Weinstein
Bone
Registrar
Surgery,
Haas
ring
A. DICKSON
PHILIP
R. A. Dickson,
and is
is no
spinal
be underestimated.
follow-up
surgically.
Leatherman
RA, Lawton
Surg
is
treated
idiopathic
scoliosis:
[Br] 1984:66-B:8-lS.
Ponseti
maturity
on average
the
Dickson
is
status
and
RA,
spine.
of the
Orthop
Clipi
IV. Long-term
not
concepts.
James
x-ray
when
a
vertebral
measurements
Dickson
Heine
occurs in the same
adolescents;
height
age,
it is clear
longer
these
skeleton,
factors,
there
of determining
method
children
of the iliac
is irrelevant.
amalgam
and
in the
governing
satisfactory
maturity
simple
same
scoliosis
1969:51-A
oJthe
with
of the
J Bone
II.
FM.
radiographic
of the human
Bone
Joint
apophysis
other
A, Harding
low-dose
et’oluiifdes
scolioses
idiopathiques
de croissance.
Doctoral
thesis.
periode
1974.
Collis DK, Ponseti
J
osteogeny.
to scoliosis.
conservative
and
measurement
growth
as elsewhere
:
changes
on the growth
relation
29#{176}
en
Hassan
which
no scoliosis
While
hand
and
and height
safe
of
height
1975)
without
complete.
physeal
spine
the
completely
ten
IJ. Observations
its
ring
curvature
1864.
& Sons,
London:
there
cannot
be said for repeated
of growing
children,
even
is used (Adran
et al. 1980).
Although
manner
sitting
Whitehouse
are depicted
on centile
charts,
record
should
be considered
phase
The
human
Gruelich
WW, Pyle SI. Radiographic
hand and wrist. 2nd ed. Stanford
child
Similarly,
height,
and
that
JW.
BE. On lateral
Churchill
of the
all such
at every
growth
assessed.
is
or normal
in relation
to
in which
RA, Dixon-Brown
in children
l980;53:146.-7.
Longitudinal
growth
human
osteogeny.
to
:803-14.
Copel
Broadhuist
a
There
of a radiograph
important
be accurately
standards
harmless,
accurate.
manner
the
can
puberty
more
be elucidated
then
simple
test performed
to
have
the
adolescence
is
JW.
Contribution
to
1951 :33-A:783-7.
and
the biologi-
in either
scoliosis
patients
natural
history
of scoliosis
should
wrist
Copel
EM,
Bick
Calvo
then
are now available.
The
1983), although
a more
to the taking
growth
patients
are
EM,
Bernard,
time-consuming
R, Dickson
of scoliosis
Br J Radio!
contribution
l950;32-A
age.
visit,
Coates
S, Cailliet
R. Vertebral
end-plate
vertebrae.
Spine
1982:7:97-102.
the
age,
GM,
and treatment
of lateral
and
London
: Churchill,
1865.
Bernick
drawbacks.
who
W. Lectures
on the patholog;’
forms
of curvature
ot the spine.
Adran
(1959)
be compared.
became
much
children
Adams
Assessment
technique.
appear-
two principal
Cleveland
More up-to-date
standards
TW2 bone age (Tanner
et al.
is
important
the atlas
still appear
to be among
the most
on record
and,
secondly,
most
of the age
are one year, though
some are six months.
If a
advanced
intervals
child
the
wrist
could
age therefore
but there
upper-class
This
of the Gruelich
standards
hand
and
of biological
accurate
The
1937).
REFERENCES
Zaoussis
curves
A study
to
:42-67.
of bone
SL, Ponseti
JIP.
THE
London:
growth
in normal
J
progression
1983:65-A
:447-55.
The
apophysis
Surg [Br]
J Bone
JOURNAL
iliac
Joint
Academic
Part I : Hand.
maturation.
IV. Curve
in scoliosis.
ed.
maturation,
skeletal
Joint Surg [Am]
AL, James
2nd
OF BONE
Bone
Press,
London
children
Joint
in idiopathic
Henry
and
Surg
its
[Br]
scoliosis.
and
the evolution
l958:40-B:442-53.
AND
JOINT
SURGERY
J
of