The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic
advertisement

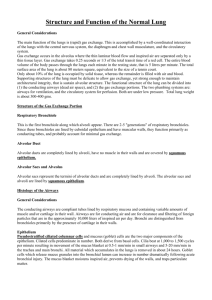
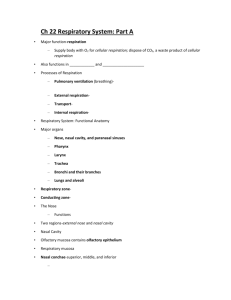
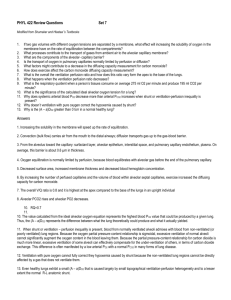
The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic Alveolar Mechanics J. DiRocco, D. Carney, and G. Nieman z Introduction Supportive therapy with mechanical ventilation is critical for survival of all patients with the acute respiratory distress syndrome (ARDS) [1]. We now recognize ventilator-induced lung injury (VILI) as a potential complication of this therapy. VILI occurs when improper methods of mechanical ventilation exacerbate the primary lung injury in ARDS [2]. Indeed, VILI significantly increases mortality from ARDS, yet the mechanism of VILI remains ill-defined [2±4]. No proven remedy for the inflammatory response associated with ARDS has yet been developed. An improved understanding of VILI will limit mortality from ARDS. Known bedside measures to guide the clinician when adjusting mechanical ventilation to minimize VILI are crude and limited [5±8]. In order to investigate the mechanism of VILI, first the dynamic behavior of alveolar inflation and deflation (i.e., alveolar mechanics) during tidal ventilation in the normal and injured lung must be understood. Currently, there are believed to be three mechanisms of VILI: 1) Atelectrauma is an alveolar shear stress-induced injury caused by alveolar recruitment-derecruitment 2) Volutrauma is an alveolar overexpansion injury caused by high lung pressures and volumes, and 3) Biotrauma is an alveolar, inflammatory injury caused by cytokine release from the pulmonary parenchyma secondary to mechanical injury induced by atelectrauma or volutrauma [9]. Since VILI-induced injury occurs mainly at the level of the alveolus or alveolar duct, understanding dynamic alveolar mechanics is critical to clarify the mechanism of VILI. Despite extensive research, the mechanics of alveolar inflation are poorly understood [10±39]. In this chapter, we will move from a review of the dynamic changes in alveoli during ventilation to postulates regarding changes in alveolar mechanics in the acutely injured lung. Finally we will discuss how improper ventilation with preservation of abnormal alveolar mechanics may cause VILI. We will not discuss the role of pulmonary surfactant, the elastin/collagen support tissue, or the three dimensional architecture of the alveolus, all of which may play an important role in normal and abnormal alveolar mechanics as discussed elsewhere [40]. Currently, there is no technique available to measure the three-dimensional changes in the alveolus and alveolar duct during tidal ventilation. However, it is possible to study two-dimensional dynamic alveolar mechanics in subpleural alveo- The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic Alveolar Mechanics li. Our laboratory utilizes in vivo microscopy to study the two-dimensional changes in subpleural alveoli in real-time with lung inflation and deflation. In order to assess dynamic mechanics in both the normal and acutely injured lung, we will integrate data from our in vivo microscopic assessment of alveolar mechanics with those generated from static models (histologic assessment at varying lung volumes) or surrogate measurements (quasi-static pressure/volume [P/V] curve, computed tomography [CT] scan, impedance tomography). z Dynamic Alveolar Ventilation Alveoli are not physically independent structures but rather are interconnected with shared walls containing elastin and collagen fibers [41]. This is disparate to common descriptions in current medical textbooks that depict alveoli as individual balloon-like structures bunched together as a cluster of grapes [42]. Histological studies have contributed substantially to our understanding of alveolar ducts and alveoli, but these studies have focused on two-dimensional static structures with little extrapolation to three-dimensional, dynamically moving structures. This is a critical oversight, for understanding dynamic change is essential to define normal alveolar mechanics and to interpret how alterations in alveolar mechanics in the acutely injured lung may lead to a VILI. Numerous experimental techniques have been used to study dynamic alveolar mechanics. In the normal lung, four models of dynamic alveolar size change have been proposed (Table 1): z isotropic balloon-like expansion and contraction of alveoli; z expansion and contraction of the alveolar ducts with little change in alveolar volume; z successive alveolar recruitment and derecruitment; and z alveolar crumpling and un-crumpling along septa similar to a paper bag [18, 19]. There is no consensus as to which of the above mechanisms predominates [10±25]. Isotropic Balloon-like Alveolar Mechanics Early depictions of alveoli as grape clusters led to a belief that each alveolus was a functionally independent unit. Therefore, it was thought that morphometric measurement of the change in alveolar surface area could be used to determine the mechanism by which alveoli change size during lung expansion [10, 12, 14, 16, 17, 21]. In addition, this thought would allow for mathematical verification since if alveoli truly expand isotropically (i.e., balloon-like stretching), the surface area of the lung should change predictably with change in lung volume. Indeed, early reports indicated that uniform, isotropic alveolar expansion and contraction were responsible for the majority of changes in lung volume [10, 12, 16]. Studies on fresh lung tissue frozen at various levels of inflation and deflation [10, 11, 14±17] indicate that alveolar shape remains relatively unchanged with changes in lung volume, supporting conventional morphometric data that alveoli change by means of isotropic expansion and contraction. Further mathematical interpretation came from Dunnill's comparison of the regression line of alveolar surface area/alveolar volume to the re- 81 82 J. DiRocco et al. Table 1. Measurement of dynamic alveolar ventilation Species Protocol Methods z Rabbit In vivo & Freezing Point count & Lm z Rat In vivo & Freezing z Dog z Dog Formalin vapor Excised lungs z Guinea pig Rapidly Frozen z Cats Freeze + Freeze dry z Cats Freeze + Freeze dry z Cats z Rat Freeze + Freeze dry Vascular perfusion z Rabbit Vascular perfusion z Rat z Dog Airway instillation In vivo z Dog In vivo z Gerbil Freeze + Freeze dry z Rat Vascular perfusion z Human Excised lung z Rat In vivo microscopy z Rabbits Excised lung Conclusions Isotropic alveolar expansion, Interior alveoli also isotropic Dynamic 2 point Geometric hysteresis count Subpleural alveoli same size in vivo and in frozen tissue Lm Isotropic alveolar expansion Alveolar septae and New method for calculating area with map reader surface tension in situ Point count & Lm Alveolar volume : linear Duct volume : at 40% VL No alveolar folding Thickness of A-B barrier ; 33% D/MD ratio No D in alveolar shape FRC ? TLC Alveoli collapse like a accordion Alveolar microholes Isotropic alveolar expansion Alveoli & duct D proportionally Morphometry Alveoli & duct D proportionally Morphometry No D in alveolar diameter and Stereology alveolar walls pleat. R/D is a major mechanism of VLD The entire alveolus does not collapse Morphometry Multiple possible mechanisms of alveolar volume change: 1) Sequential alveolar derecruitment 2) Balloon-like reduction in size 3) Change in size and shape 4) Crumpling of alveolar surface Morphometry Anisotropic alveolar expansion Morphometry Little change in alveolar volume Lung volume change by R/D Monodispersed Little change in alveolar volume Aerosol Lung volume change by R/D Lm Little change in alveolar volume Lung volume change by R/D 3D reconstruction Alveolar shape Ds with deflation Little D in alveolar diameter until very low lung volume P/V curve Alveolar collapse without Pflex Mathematical model Lung volume change by R/D Morphometry 11% D in alveolar diameter during tidal ventilation P/V curve Alveolar diameter ; with : in lung volume, R/D important Reference 10 11 12 13 14 15 16 17 18 19, 20 21 22 23 24 25 26 27 28 The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic Alveolar Mechanics Table 1 (continued) Species Protocol Methods Conclusions Reference z Rats Excised lung z Mice Freeze substitution In situ Airway fixation z Rats Airway fixation Morphometry z Human Frozen section Morphometry z Rat Glutaraldehyde Morphometry Light & EM z N/A Math model Math P/V curve z N/A Math model Math P/V curve z Dog Oleic acid lung injury CT scan z Human ALI/ARDS CT scan z Dog Rabbit Rat Normal Excised Lungs Morphometry Small airway (< 300 lm) D length & diameter with lung volume D Alveoli : in size with lung volume D No maximum lung volume No D in alveolar size with D in lung volume Lung volume D due to :; in alveolar number not size Alveolar wall stretched and thus carry force. Alveolar ducts and alveolar walls in mechanical equailibrium At low lung volume alveoli expand either by unfolding or expansion of alveolar ducts. At high lung volumes the basement membrane and attached cells deform Alveoli recruit throughout lung inflation not only at lower Pflex. The P/V curve did not predict optimal ventilator setting Best compliance during decremental, but not incremental, PEEP is related to open-lung PEEP Recruitment throughout lung inflation not just at Pflex. More alveoli open on expiration than inspiration at the same airway pressure Recruitment throughout lung inflation not just at Pflex. Derecruitment did not parallel deflation Lung folding appeared in all species with some protocols but absent in others. Folding depends on lung volume history 29 z Mice Microfocal X-ray tomography Lm P/V curve Lm 30 31 32 33 34 35 36 37 38 39 Lm: mean linear intercept; A-B: air-blood barrier; R/D: alveolar recruitment/derecruitment; P/V: lung pressure/volume curve; Pflex: inflection point on the P/V curve; N/A: not applicable; VL: Lung volume; FRC: Functional residual capacity; TLC: Total lung capacity; D: Change 83 84 J. DiRocco et al. gression line of alveolar surface area/lung volume [12]. His mathematical comparison supported uniform, isotropic alveolar expansion, however repeat calculations of his data could not distinguish either recruitment/derecruitment or isotropic alveolar volume change as the most important mechanism of lung inflation. Subtle modifications to the postulate of isotropic change followed including ideas that alveoli increase in volume in linear fashion with lung volume [14], alveoli undergo anisotropic expansion (i.e., unequal or asymmetrical alveolar expansion) [21], or a combination of isotropic expansion of the alveolus and alveolar duct [16]. None of these early postulates are easily defended. Alveolar Folding Rather than balloon-like elastic expansion and contraction, the alveolus could change size by folding and unfolding of the alveolar walls similar to an accordion. An early study by Forest suggested that alveoli did not fold [14]. This work was followed by several studies that disagreed and concluded that alveoli do indeed change volume by complex folding [15, 18±20, 34, 39]. In a theoretical model of complex alveolar folding, alveolar surface area would not significantly change with lung inflation and thus alveolar volume and alveolar surface area would not necessarily be related. If the alveolar surface area increased with lung expansion alveoli would change either be stretching or recruiting. The first demonstration of septal folding in the rabbit was by Gil and Weibel who found ªcrumplingº of the alveolar surface and showed that the epithelium folds back onto adjacent epithelium [18]. Gil et al. demonstrated the presence of septal folding in fixed tissue [19]. Their photomicrographs showed heavy thickened septa with capillaries piled upon each other. This demonstrated the potential anatomic mechanism for alveolar septal folding. Klingele and Staub [15] demonstrated that there is no change in alveolar shape from functional residual capacity (FRC) to total lung capacity (TLC) but at low lung volumes alveoli collapse from side to side similar to folding of an accordion. Oldmixon and Hoppin demonstrated that alveolar folding was seen in rat but not dog and rabbit lungs fixed over a range of inflation pressures and inflation histories [39]. They noted that the presence of septal folding was more related to lung volume history that lung pressure at fixation and that there was temporal component to the unfolding process. A transient inflation pressure of 22 cmH2O did not resolve septal folding, but holding the pressure at 22 cmH2O (or cycling the pressure at 30 cmH2O) did eliminate folding. The possibility of septal folding is anatomically feasible since the curvature of the air-liquid interface in the corners of the alveolar space would allow enough ªslacknessº in the alveolus to allow septal folding [16]. Septal folding may be the prime mechanism causing distinctive inflection points (Pflex) on the quasi-static P/V curve that are the hallmarks of lung reopening. Tschumperlin and Margulies [34] found that at low volumes lung inflation is by either septal unfolding or expansion of the alveolar ducts without a change in alveolar volume. At high lung volume, their data suggests that the basement membrane and attached cells deform as the lung nears physiological limits. An electron microscope (EM) photomicrograph clearly demonstrates an alveolar fold at low lung volume (Fig. 1). This biphasic change in alveolar size by one mechanism at low lung volume (septal folding) and a different mechanism at high lung volume (alveolar stretching) was support by the data obtained by Klingele and Staub [15]. The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic Alveolar Mechanics Fig. 1. Electron micrograph demonstrating septal folding (arrow) between an alveolus (alv) and capillary (cap) at low lung volume. Septal folding would allow alveoli to change volume greatly without a change in basement membrane surface area. An alternate interpretation is volume change exclusively in the alveolar duct without a change in alveolar volume or surface area. From [34] with permission Alveolar Recruitment/Derecruitment Another possibility is that the lung changes volume by recruitment and derecruitment of large populations of alveoli. Alveoli are either open or collapsed and do not change size with ventilation, other than by rapid opening or total collapse. To prove the above, it would have to be shown that open alveoli do not change size with ventilation and that there are more alveoli open at inspiration than at expiration. A number of studies have concluded that the lung changes volume primarily by alveolar recruitment/derecruitment [22±24, 26, 28, 32]. Smaldone and coworkers [23] developed a unique technique in which they filled excised lungs with a mono-dispersed aerosol and measured its deposition in alveoli at zero airflow. By evaluating the relationship of particle deposition and morphometric assessment of alveolar size, they concluded that the lung inflates by a progressive recruitment of alveoli and deflates by alveolar derecruitment. In addition they noted that at low lung volume alveoli were large and actually got smaller during inflation concomitant with an increase in alveolar number. Data from Lum and coworkers suggested that the predominant mechanism of lung volume change is alveolar recruitment. They also observed a temporal recruitment of alveoli with application of 30 cmH2O airway pressure [24]. Specifically, alveoli recruit over time as long as elevated airway pressure was maintained. Although not directly observed with EM in this studies, the authors postulate that the anatomical mechanism of alveolar recruitment is septal pleating akin to previously described studies [18, 19]. Using data from postmortem, excised human lungs, Salmon et al. [26] created a mathematical model of a P/V curve and concluded that reopening of collapsed alveoli during lung inflation is responsible for the majority of hysteresis in the P/V curve. Boyle et al. [28] showed that the mean air space diameter declined with increased volume in rabbit lungs. This suggests that a significant amount of alveolar recruitment had occurred. Direct visualization of subpleural alveoli during large changes in lung volume in the living animal also suggests that the lung changes volume by alveolar recruitment/derecruitment [22]. In vivo photomicrographs 85 86 J. DiRocco et al. Fig. 2. In vivo photomicrographs of normal subpleural alveoli at residual volume (RV), inflation to 80% of total lung capacity (TLC) and deflation to a second RV (RV #2). The number of alveoli changed greatly with lung volume change whereas alveolar size changed very little. This suggests that the normal lung changes volume by alveolar recruitment/derecruitment rather than balloon-like expansion and contraction. From [22] with permission showed that the size of alveoli at residual volume, as compared to 80% TLC, was not significantly different suggesting that lung volume change is due to either recruitment/derecruitment or changes in the alveolar duct (Fig. 2). In a recent morphometric study, it was determined that changes in lung volume are due to changes in the number of alveoli (recruitment/derecruitment) without a change in alveolar size [32]. They further postulated that the mechanism of the hysteresis between the inflation and deflation limb of the P/V is due to a difference in the number of open alveoli. Another method to determine if alveolar recruitment/derecruitment occurs is to measure the change in alveolar size with lung inflation. If alveoli do not change size then it can be inferred that recruitment/derecruitment may be taking place. Several studies looked at alveolar size change with lung inflation with variable results. Mercer et al. did a three-dimensional reconstruction of alveoli and found that there was little change in alveolar volume except at low lung volume [25]. In two recent studies by Soutiere et al., [30, 31] it was found that the observation of alveolar size change during lung inflation was dependent on whether fixation was by freezing The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic Alveolar Mechanics (change) [30] or airway fixation (no change) [31]. Thus, these experiments yield variable results in support of the lung changing volume by alveolar recruitment. Summary of Normal Alveolar Mechanics Although there are excellent studies suggesting that alveoli change volume in a balloon-like fashion [10±12, 14±17], we believe the best available data support the theory that the lung changes volume by either alveolar folding [15, 18±20, 34, 39] or alveolar recruitment/derecruitment [22±24, 26, 28, 32]. Alveolar folding and recruitment/derecruitment need not be mutually exclusive. The studies investigating alveolar recruitment/derecruitment did not considered the mechanism by which the alveolus recruits and derecruits. It is very conceivable that lung volume change is by recruitment/derecruitment and the mechanism of alveolar collapse and opening is through septal folding. Hopefully, new techniques such as CT will yield dynamic three-dimensional images of alveoli and alveolar ducts to resolve this long standing controversy [29]. z Abnormal Alveolar Mechanics Although we are still unsure of how the normal lung changes volume, most of the literature favors relatively stable alveoli and that other mechanisms (e.g., duct volume change, normal recruitment/derecruitment, crumpling and pleating) account for normal lung volume change. Thus, unstable alveoli that collapse and expand with each breath will be considered abnormal. Early studies by both Gil et al. [19] and Bachofen et al. [20] demonstrated that derecruitment was the dominant mechanism of lung deflation in a surfactant deactivation model of ARDS. These data are supported by a mathematical model of the P/V curve that suggested that in ARDS the lung changes volume primarily by recruitment/derecruitment [35, 36]. Two studies measuring alveolar recruitment via a CT scan, one in a dog model of ARDS [37], the other in humans with ARDS [38], both support the above hypothesis that in the acutely injured lung volume change is predominately by alveolar recruitment/derecruitment. More recently, alveolar recruitment/derecruitment has been shown to be the predominant mechanism of lung volume change in the acutely injured lung inflated to near TLC [18±22] as well as during tidal ventilation [43, 44]. Indirect techniques have been used to study dynamic alveolar stability during tidal ventilation [43, 44]. Dynamic alveolar collapse and recruitment following lung injury by oleic acid, saline lavage, and endotoxin was assessed utilizing CT [43]. In all three injuries, alveoli collapse and reopen rapidly (as fast as 0.6 seconds following a breath hold) (Fig. 3). Grasso et al. utilized P/V curves during tidal ventilation and hypothesized that increase in slope indicated tidal alveolar recruitment, decrease in slope indicated tidal alveolar over-inflation and a linear curve indicates normal aerated alveoli [44]. These data support those of Neumann [43] and suggest that dynamic alveolar inflation is altered in acute lung injury (ALI) during tidal ventilation. 87 88 J. DiRocco et al. The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic Alveolar Mechanics Ventilator Injury and Dynamic Alveolar Mechanics Regardless of how normal alveoli change volume with tidal ventilation, in ALI dynamic alveolar mechanics are dramatically altered [43±46]. Atelectrauma is caused when unstable alveoli result in a shear stress induced lung injury [41]. Ventilator settings that presumably cause alveolar recruitment/derecruitment are known to cause VILI (i.e., high peak inspiratory pressure and low positive end-expiratory pressure [PEEP]) [47]. Reducing tidal volume, which presumably reduces alveolar recruitment/derecruitment has been shown to reduce mortality in patients with ARDS [1, 5]. Our lab directly measured dynamic alveolar mechanics utilizing in vivo microscopy and demonstrated that inappropriate ventilation of unstable alveoli results in VILI (Fig. 4) [46]. Fig. 4. In vivo photomicrographs of the same normal alveoli at peak inspiration (a) and end expiration (b). Normal alveoli are very stable with little change in size during tidal ventilation (dots). Injurious mechanical ventilation (High peak inspiratory pressure, low PEEP) causes a ventilator induced lung injury resulting in alveolar instability. Abnormal alveoli in an injured lung at peak inspiration (c) and end expiration (d) demonstrating severe instability with alveoli open on inspiration (dots) and collapsed on expiration (arrows) 3 Fig. 3. Computed tomography (CT) scans of lungs injured by 3 different mechanisms (Oleic acid, top; Saline Lavage, middle; Endotoxin, bottom). CT scans were obtained after 4 seconds of inspiratory hold (right) and 4 seconds of expiratory hold (left). Note that there was more collapse during both the expiratory and inspiratory hold in the oleic acid injured lungs (top). This suggests that the etiology of injury has an impact on alveolar instability. From [43] with permission 89 90 J. DiRocco et al. Altered dynamic alveolar mechanics may cause VILI by two mechanisms: 1) large gross tears could be ripped in the alveolar wall, or 2) the cell membrane maybe injured without gross tears [48±50]. In a patient subjected to very high-pressure mechanical ventilation during support for ARDS, Hotchkiss et al. found multiple large tears in the alveolar wall [48]. Gajic et al. demonstrated that injurious mechanical ventilation damaged pulmonary cell membranes and that the injury was reversible if injurious ventilation was discontinued [49]. Injury to the cell membrane was confirmed utilizing electron microscopy that revealed ultra-structural disruption to both pulmonary epithelium and endothelium [50]. VILI caused destruction of epithelial cells and denudation of the basement membrane. These studies suggest that altered alveolar mechanics are a primary mechanism of VILI and that alveolar injury ranges from gross tearing to ultrastructural damage. z Conclusion The exact mechanism of dynamic lung volume change at the alveolar level is unknown. Postulated mechanisms of alveolar mechanics include `normal' alveolar recruitment/derecruitment, change in the size of the alveolar duct with little change in alveolar size, and crumpling/uncrumpling of the alveolus similar to a paper bag and balloon-like alveolar size change. It appears that normal alveoli are stable and that with ALI alveoli become unstable and will often collapse and re-open with every breath. This recruitment/derecruitment causes a shear stress injury that damages lung tissue leading to VILI. More knowledge of normal and abnormal alveolar mechanics is necessary to better understand the mechanism of VILI. This knowledge will ultimately improve ventilator strategies leading to reduced morbidity and mortality associated with VILI. References 1. Acute Respiratory Distress Syndrome Network (2000) Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 342:1301±1308 2. Rubenfeld GD (2003) Epidemiology of acute lung injury. Crit Care Med 31:S276±S284 3. Pinhu L, Whitehead T, Evans T, Griffths M (2003) Ventilator-associated lung injury. Lancet. 361:332±340 4. Dreyfuss D, Saumon G (1998) Ventilator-induced lung injury. Lessons from experimental studies. Am J Respir Crit Care Med. 157:294±323 5. Amato MBP, Barbas CSV, Medeiros DM, et al (1998) Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med 338:347±354 6. Putensen C, Baum M, Hormann C (1993) Selecting ventilator settings according to variables derived from the quasi-static pressure/volume relationship in patients with acute lung injury. Anesth Analg 77:436±447 7. Harris RS, Hess DR, Venegas JG (2000) An objective analysis of the pressure-volume curve in the acute respiratory distress syndrome. Am J Respir Crit Care Med 161:432±439 8. Victorino JA, Borges JB, Okamato, et al (2004) Imbalances in regional lung ventilation. A validation study on electrical impedance tomography. Am J Respir Crit Care Med 169:791± 800 9. Slutsky AS (1999) Lung injury caused by mechanical ventilation. Chest 116 (Suppl): 9S±15S 10. Tangelo E (1972) Local alveolar size and Tran pulmonary pressure in situ and in isolated lungs. Respir Physiology 14:251±266 The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic Alveolar Mechanics 11. Daly BDT, Parks GE, Edmonds CH, Hibbs CW, Norman JC (1975) Dynamic alveolar mechanics as studied by videomicroscopy. Respir Physiol 24:217±232 12. Dunnill MS (1967) Effect of lung inflation on alveolar surface area in the dog. Nature 214:1013±1014 13. Flicker E, Lee JS (1974) Equilibrium of force of subpleural alveoli: implications to lung mechanics. J Appl Physiol 36:366±374 14. Forrest JB (1970) The effect of changes in lung volume on the size and shape of alveoli. J Physiol 210:533±547 15. Klingele TG, Staub NC (1970) Alveolar shape changes with volume in isolated, air-filled lobes of cat lung. J Appl Physiol 28:411±414 16. Kuno K, Staub NC (1968) Acute mechanical effects of lung volume changes on artificial microholes in alveolar walls. J Appl Physiol 24:83±92 17. Storey WF, Staub NC (1962) Ventilation of terminal air units. J Appl Physiol 17:391±397 18. Gil J, Weibel ER (1972) Morphological study of pressure-volume hysteresis in rat lungs fixed by vascular perfusion. Respir Physiol 15:190±213 19. Gil J, Bachofen H, Gehr P, Weibel ER (1979) Alveolar volume±surface area relation in air and saline-filled lungs fixed by vascular perfusion. J Appl Physiol Respir Environ Exercise Physiol 47:990±1001 20. Bachofen H, Gehr P, Weibel ER (1979) Alterations of mechanical properties and morphology in excised rabbit lung rinsed with detergent. J Appl Physiol Respir Environ Exercise Physiol 47:1002±1010 21. Forest JB (1976) Lung tissue plasticity: Morphometric analysis of anisotropic strain in liquid filled lungs. Respir Physiol 27:223±239 22. Carney DE, Bredenberg CE, Schiller HJ, et al (1999) The mechanism of lung volume change during mechanical ventilation. Am J Respir Crit Care Med 160:1697±1702 23. Smaldone GC, Mitzner W, Itoh H (1983) Role of alveolar recruitment in lung inflation: influence on pressure-volume hysteresis. J Appl Physiol Respir Environ Exercise Physiol 55:1321±1332 24. Lum H, Huang I, Mitzner W (1990) Morphological evidence for alveolar recruitment during inflation at high transpulmonary pressure. J Appl Physiol 68:2280±2286 25. Mercer RR, Laco JM, Crapo JD (1987) Three-dimensional reconstruction of alveoli in the rat lung for pressure-volume relationships. J Appl Physiol 62:1480±1487 26. Salmon RB, Primiano FP, Saidel GM, Niewoehner DE (1981) Human lung pressure-volume relationships: alveolar collapse and airway closures. J Appl Physiol Respir Environ Exercise Physiol 51:353±362 27. Moreci AP, Norman JC (1973) Measurements of alveolar sac diameters by incident-light photomicrography. Ann Thorac Surg 15:179±185 28. Boyle J, Englestein ES, Sinoway LI (1977) Mean air space diameter, lung surface area and alveolar surface tension. Respiration 34:241±249 29. Sera T, Fujioka H, Yokota H, et al (2004) Localized compliance of small airways in excised rat lungs using microfocal X-ray tomography. J Appl Physiol 96:1665±1673 30. Soutiere SE, Mitzner W (2004) On defining total lung capacity in the mouse. J Appl Physiol 96:1658±1664 31. Soutiere SE, Tankersley CG, Mitzner W (2004) Differences in alveolar size inbred mouse strains. Respir Physiol Neurobiol 140:283±291 32. Escolar JD, Escolar MA, Guzman J, Roques M (2002) Pressure volume curve and alveolar recruitment/derecruitment. A morphometric model of the respiratory cycle. Histol Histophatol 17:383±392 33. Yager D, Feldman H, Fung YC (1992) Microscopic vs macroscopic deformation of pulmonary alveolar duct. J Appl Physiol 72:1348±1354 34. Tschumperlin DJ, Margulies SS (1999) Alveolar epithelial surface area-volume relationship in isolated rat lungs. J Appl Physiol 86:2026±2033 35. Hickling KG (1998) The pressure-volume curve is greatly modified by recruitment. A mathematical model of ARDS lungs. Am J Respir Crit Care Med 158:194±202 36. Hickling KG (2001) Best compliance during a detrimental, but not incremental, positive end-expiratory pressure trial is related to open-lung positive end-expiratory pressure. A 91 92 J. DiRocco et al.: The Mechanism of Ventilator-induced Lung Injury: Role of Dynamic Alveolar Mechanics 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. mathematical model of acute respiratory distress syndrome lungs. Am J Respir Crit Care Med 163:69±78 Pelosi P, Goldner M, McKibben A, et al (2001) Recruitment and derecruitment during acute respiratory failure. An experimental study. Am J Respir Crit Care Med 164:122±130 Crotti S, Mascheroni D, Caironi P, et al (2001) Recruitment and derecruitment during acute respiratory failure. A clinical study. Am J Respir Crit Care Med 164:131±140 Oldmixon EH, Hoppin FG (1991) Alveolar septal folding and lung inflation history. J Appl Physiol 71:2369±2379 Gatto LA, Fluck RR, Nieman GF (2004) Alveolar mechanics in the acutely injured lung: Role of alveolar instability in the pathogenesis of ventilator-induced lung injury. Respir Care 49:1045±1055 Mead J, Takishima T, Leith D (1970) Stress distribution in lungs: a model of pulmonary elasticity. J Appl Physiol 28:596±608 West JB (2000) Respiratory Physiology ± The Essentials, 6th ed Lippincott Williams & Wilkins, Philadelphia, p 83 Neumann P, Berglund JE, Mondejar EF, Magnusson A, Hedenstierna G (1998) Dynamics of lung collapse and recruitment during prolonged breathing in porcine lung injury. J Appl Physiol 85:1522±1543 Grasso S, Terragni P, Mascia L, et al (2004) Airway pressure-time curve profile (stress index) detects tidal recruitment/hyperinflation in experimental acute lung injury. Crit Care Med 32:1018±1027 Halter JM, Steinberg JM, Schiller HJ, et al (2003) Positive end-expiratory pressure (PEEP) after a recruitment maneuver prevents both alveolar collapse and recruitment/derecruitment. Am J Respir Crit Care Med 167:1620±1626 Steinberg J, Schiller HJ, Halter JM, et al (2004) Alveolar instability causes early ventilator-induced lung injury independent of neutrophils. Am J Respir Crit Care Med 169:57±63 Tremblay L, Valenza F, Riberio SP, Li J, Slutsky AS (1997) Injurious ventilatory strategies increase cytokines and c-fos m-RNA expression in an isolated rat lung model. J Clin Invest 99:944±952 Hotchkiss JR, Simonson DA, Marek DJ, Marini JJ, Dries DJ (2002) Pulmonary microvascular fracture in a patient with acute respiratory distress syndrome. Crit Care Med 30:2368±2370 Gajic O, Lee J, Doerr CH, Berrios JC, Myers JL, Hubmayr RD (2003) Ventilator-induced cell wounding and repair in the intact lung. Am J Respir Crit Care Med 167:1057±1063 Dreyfuss DP, Soler P, Basset G, Saumon G (1988) High inflation pressure pulmonary edema: respective effects of high airway pressure, high tidal volume an positive end-expiratory pressure. Am Rev Respir Dis 137:1159±1164