Manual Therapy 16 (2011) 399e402
Contents lists available at ScienceDirect
Manual Therapy
journal homepage: www.elsevier.com/math
Technical and measurement report
Anatomical validity of the HawkinseKennedy test e A pilot study
Stacey Tucker a, b, Nicholas F. Taylor a, b, Rodney A. Green a, c, *
a
Musculoskeletal Research Centre, La Trobe University, Victoria 3086, Australia
School of Physiotherapy, La Trobe University, Victoria 3086, Australia
c
School of Human Biosciences, La Trobe University, Victoria 3086, Australia
b
a r t i c l e i n f o
a b s t r a c t
Article history:
Received 3 September 2010
Received in revised form
27 January 2011
Accepted 2 February 2011
Purpose: Despite routine use, clinical tests used to diagnose subacromial impingement often display poor
diagnostic accuracy. A lack of anatomical validity may contribute to the poor diagnostic accuracy. The
current study aimed to examine the anatomical validity of measuring subacromial pressure in the
HawkinseKennedy impingement test in a cadaveric shoulder.
Methods: Subacromial pressures were measured using pressure transducers in non-provocative and
provocative HawkinseKennedy test positions using an ABA research design with 25 repeated measures
in one cadaver. Data collected included pressure at four subacromial locations (coracoid process, coracoacromial ligament, anterior acromion and posterior acromion), and observation of anatomical structures
impinging on transducers. The split-middle method of visual analysis and the Reliable Change Index
(RCI) were applied to examine any differences between provocative and non-provocative positions.
Results: There was increased pressure in the provocative position at the coraco-acromial ligament, which
impinged biceps brachii, and at the anterior acromion, which impinged the rotator interval.
Conclusion: Findings of the current study provide evidence that suggest that structures other than the
rotator cuff tendons may be impinged during the HawkinseKennedy test.
Ó 2011 Elsevier Ltd. All rights reserved.
Keywords:
Shoulder impingement syndrome
Anatomy
Cadaver
Measurement
1. Introduction
Shoulder pain is common with a point prevalence in the general
community of 14e21% (Bongers, 2001; Picavet and Schouten,
2003). Approximately 40% of all patients who visit a doctor for
shoulder pain are diagnosed with impingement syndrome (Van der
Windt et al., 1995). Impingement syndrome is used to describe the
patho-mechanics of increased subacromial compression of the
rotator cuff, subacromial bursa and biceps tendon during arm
elevation (Neer, 1983; Wuelker et al., 1994).
The HawkinseKennedy clinical test is routinely used to detect
subacromial impingement by placing the shoulder joint in a position that increases contact between the head of humerus and
acromion, therefore compressing structures that course through
the subacromial space (Roberts et al., 2002). The test developers
proposed that during their test the supraspinatus tendon is
compressed against the under surface of the coraco-acromial ligament (Hawkins and Kennedy, 1980). A positive test is reproduction
of pain. Although this clinical test to determine impingement is
* Corresponding author. School of Human Biosciences, La Trobe University,
Victoria 3086, Australia. Tel.: þ613 9479 5751; fax: þ613 9479 5784.
E-mail address: rod.green@latrobe.edu.au (R.A. Green).
1356-689X/$ e see front matter Ó 2011 Elsevier Ltd. All rights reserved.
doi:10.1016/j.math.2011.02.002
commonly used, the diagnostic accuracy is often poor (Hegedus
et al., 2007; Hughes et al., 2008).
A lack of anatomical validity to support the use of this clinical
test may explain the poor diagnostic accuracy (Green et al., 2008).
Evidence of anatomical validity of shoulder impingement can be
established by measuring subacromial pressure during clinical tests
to determine if the test increases compression on the structure that
it purports to place stress on.
Therefore the main aim of the current study was to compare the
subacromial pressure between provocative HawkinseKennedy
shoulder impingement test position and a non-provocative position using pressure transducers in a cadaveric upper limb. It was
hypothesised that the pressure would be significantly higher in the
provocative position therefore providing evidence about the
anatomical validity of the HawkinseKennedy test.
2. Methods
2.1. Design
We used a single-case ABA research design to determine
whether there was a significant difference in subacromial pressure
between a non-provocative position and the HawkinseKennedy
impingement test position in one cadaver specimen.
400
S. Tucker et al. / Manual Therapy 16 (2011) 399e402
2.2. Apparatus
2.3. Procedure
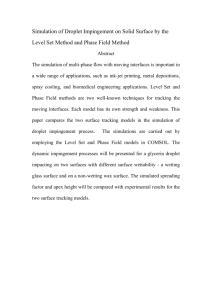
Single use force sensitive resistors (model No. 400 Interlink
Electronics, California, Fig. 1) were used as the transducers to
measure subacromial pressures. The pressure transducers were
sufficiently small (5 mm diameter) to be placed in the subacromial
arch and were affordable (less than AUD$5 for each transducer).
The electrical output from the pressure transducers was connected to an existing 4-channel PowerLab unit via a custom
designed 4-channel variable offset amplifier (Computing and
Technical Services Unit, Faculty of Health Sciences) with a maximal
error due to noise of 1.2%. The data were then fed directly to
a computer and collected using ‘LabChart 6 for Windows’ software
(ADI Instruments, Sydney). Data were collected at a frequency of
1000 Hz. For each trial the mean pressure data was obtained for
a 200 ms period commencing from the time the limb was placed in
the required position.
The inter-device reliability of the pressure transducers was
determined in a bench top experiment. Four pressure transducers
were tested by applying a series of 10 weights (31e91 g) to each
transducer in 6 g intervals across 5 trials. There was high interdevice reliability in each of the 5 trials (Intraclass Correlation
Coefficient ICC [3,1] ¼ 0.96, 0.92, 0.88, 0.97 and 0.98).
Subacromial pressure measurements with the transducers in
HawkinseKennedy impingement test position displayed high
re-test reliability (ICC [2,1] ¼ 0.88, 95% confidence interval [CI]
0.61e0.99) across five trials using pressure transducers in four
subacromial locations.
Dissection of one cadaveric upper limb complete with pectoral
girdle involved removal of the deltoid muscle and subacromial
bursa to expose the glenohumeral joint capsule and the rotator cuff
tendons. The embalmed cadaver specimen was an 82 year old male
with no observed pathology of rotator cuff tendons nor previous
surgery. The body of the scapula was fixed in a vice using two bolts
so that the limb was suspended in the anatomical position with the
glenohumeral joint free to move. The borders of the exposed
muscle fibres of subscapularis, supraspinatus, infraspinatus and
teres minor tendons were traced laterally, representing the
blending of the tendon of each muscle onto the exposed joint
capsule using a permanent marker. The rotator interval was marked
between subscapularis and supraspinatus tendons (Fig. 1).
The four pressure transducers were adhered to the specimen in
the following positions within the subacromial space (Fig. 1):
posterior surface of coracoid process
mid-point of the coraco-acromial ligament
1 cm posterior to the anterior border of the lateral edge of the
acromion process
1 cm anterior to the posterior border of the lateral edge of the
acromion process.
Shoulder flexion angle in each test position was measured using
a universal goniometer (model G300; Whitehall Manufacturing,
City of Industry, CA). Universal goniometers have demonstrated
excellent re-test reliability in measuring shoulder flexion (ICC:
091e0.97) with high levels of agreement with digital inclinometers
(ICC: 0.81e0.95) (Mullaney et al., 2010). The HawkinseKennedy
test position was performed by passively flexing the glenohumeral
joint to 60 and adding maximal internal rotation to a point where
the tissues were providing significant passive resistance. The nonprovocative position was 60 passive shoulder flexion without any
shoulder rotation. According to the two-to-one ratio of scapulohumeral rhythm described by Levangie and Norkin (2005), when
the shoulder is at 90 flexion the glenohumeral joint contributes
60 and the scapula-thoracic joint contributes 30 . Recent threedimensional studies confirm that the scapula-thoracic joint
contributes between 20 and 40 of the first 90 of elevation
(McClure et al., 2001; Yano et al., 2010). As the scapula of the
cadaver was fixed in the vice this normal two-to-one ratio was
disrupted. Therefore for this study, 60 of glenohumeral flexion in
the cadaver was approximately equivalent to 90 shoulder flexion
in a living person.
As part of the ABA research design in phase A, the nonprovocative position was repeated for 10 consecutive trials. The
provocative test position was then completed for 10 consecutive
trials in phase B. Testing was then repeated in phase A, the nonprovocative position for another five consecutive trials. The limb
was returned to the neutral (anatomical) position between each
trial. Tests were performed in series with approximately 1 min
intervals between each trial. The person carrying out the movement of the cadaver specimen was blinded to the pressure being
recorded.
2.4. Data analysis
Fig. 1. Supero-lateral view of left cadaveric upper limb with borders of rotator cuff tendons
traced onto the glenohumeral joint capsule and pressure transducers attached (CP ¼ coracoid process, CA ¼ coraco-acromial ligament, AA ¼ anterior acromion, PA ¼ posterior acromion, RI ¼ rotator interval, SS ¼ supraspinatus tendon, IS ¼ infraspinatus tendon,
TM ¼ teres minor tendon, *pressure transducer fixed under AA). Note that subscapularis
tendon is anterior to RI (not fully visible on this figure).
Two methods of analysis for single subject data were used to
increase the strength and confidence of findings: Reliable Change
Index (RCI) and visual analysis using the split-middle method of
trend estimation. A difference between the provocative and nonprovocative positions was only considered significant if indicated
by both analyses.
S. Tucker et al. / Manual Therapy 16 (2011) 399e402
The RCI tests whether two or more scores obtained from the
same subject on two or more occasions are significantly different
and is based on the rationale that difference in the scores on the
two different occasions (non-provocative position versus provocative position) should be much greater than the variability due to
measurement error (Gorman and Allison, 1997). The RCI is suitable
for use on small data series and can assess changes beyond those
resulting from measurement error (Harbst et al., 1991).
The RCI results in a z score. For this experiment a Bonferroni
correction, that divides the significance level by the number of
comparisons, was performed to decrease the risk of a type one
error. Allowing for eight comparisons in the current study a z score
of 2.75 was accepted as significant at the 0.006 (0.05/8) level
(Portney and Watkins, 2000, p461). The RCI was calculated for both
phase AeB and BeA for each subacromial transducer location.
Data obtained in the non-provocative and provocative test
positions were graphed. The split-middle method of trend estimation was applied to the graphed data (Nourbakhsh and
Ottenbacher, 1994). This method is designed to demonstrate
whether data are displaying a change in level or trend between the
non-provocative (A) and provocative (B) positions. To do this, a line
of best fit or ‘celeration line’ was applied to the non-provocative
position; the line was extended to data in the provocative position.
The difference between the non-provocative and provocative test
positions was assessed by comparing the proportion of points
above and below the celeration line across the two test positions.
Statistical significance was determined using a binomial test with
an alpha level of 0.006 accepted as the level of significance allowing
for the eight comparisons. If there is no difference between the two
positions the proportion of data points above and below the line
should remain the same between the test positions (Nourbakhsh
and Ottenbacher, 1994).
Subacromial pressure values were expressed as grams. Data
obtained via observation of the cadaver were recorded and tabulated to analyse if pressure transducers were in contact with the
specimen and, if so, which tendon was in contact with the
transducer.
3. Results
There was a statistically significant difference in subacromial
pressure between the non-provocative and provocative positions
for both phase AeB and BeA for transducers at the coracoid
process, coraco-acromial ligament, and at the anterior acromion,
but not at the posterior acromion. The average range of shoulder
internal rotation measured during the five trials was 50 (range:
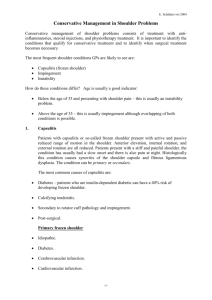
45e52 ). There was a large increase in pressure in the provocative
position for transducers placed at the coraco-acromial ligament,
and the anterior acromion (mean increase of 43 g (95% CI 36e50 g)
and 23 g (95% CI 15e32 g) respectively, Table 1, Fig. 2). The
401
Fig. 2. Graphical representation and celeration line for pressure transducer 2 (coracoacromial ligament) subacromial pressures (g) during non-provocative (A) and
provocative (B) positions.
transducer placed at the coracoid process demonstrated a small
decrease in pressure of 6 g (95% CI 3e9 g) in the provocative
position and there was no change in the pressure at the transducer
at the posterior acromion (mean increase <0.1 g, 95% CI
0.01e0.20 g).
On observation, long head of biceps brachii tendon was
impinged in the intertubercular groove by the coraco-acromial
ligament and the coracoid process, and the rotator interval was
impinged by the anterior acromion during the provocative test
positions (Table 1).
4. Discussion
Subacromial impingement is a common cause of shoulder pain.
Hawkins and Kennedy (1980) proposed that during their test the
supraspinatus tendon is impaled against the under surface of the
coraco-acromial ligament. Supraspinatus is most commonly
implicated in impingement syndrome closely followed by infraspinatus. Pathology of subscapularis usually occurs in conjunction
with other rotator cuff findings and teres minor pathology is
uncommon (Chung et al., 2008).
However, in our study HawkinseKennedy impingement test did
not compress supraspinatus within the subacromial space and this
is consistent with another recent study replicating this test using
cadaver specimens (Yamamoto et al., 2009). The only structures
observed to be compressed in the provocative test position were
the long head of biceps brachii tendon and the rotator interval,
structures which are rarely implicated in impingement syndrome.
Yamamoto et al. (2009) indicated contact between the subscapularis tendon and both the coraco-acromial ligament and the
acromion process in the HawkinseKennedy position (Yamamoto
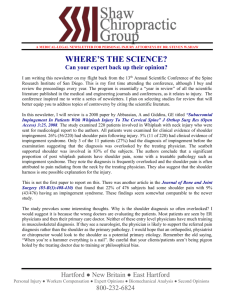
Table 1
Reliable Change Index (RCI), binomial test for phase AeB and BeA and observational data for HawkinseKennedy impingement test.
Pressure transducer
Trial
RCI (z)
Binomial test (p)
Contact between pressure
transducer and
specimen yes/no
Muscle/tendon in contact with
pressure transducer
1. Coracoid process
AeB
BeA
AeB
BeA
AeB
BeA
AeB
BeA
4.1*
12.2*
219.4*
31.4*
10.7*
117.9*
2.9*
2.5
0.002*
0.002*
0.002*
0.002*
0.002*
0.002*
0.34
> 0.99
Yes
Biceps brachii long head
Yes
Biceps brachii long head
Yes
Rotator interval
2. Coraco-acromial
ligament
3. Anterior acromion
4. Posterior acromion
* Statistically significant change p 0.006.
No
402
S. Tucker et al. / Manual Therapy 16 (2011) 399e402
et al., 2009). Although subscapularis was not impinged in the
current study, the adjacent nature of subscapularis tendon on the
lesser tuberosity and the long head of biceps tendon in the intertubercular groove indicate that Yamamoto’s findings are similar
findings to the current study. These results raise the possibility that
production of pain during the HawkinseKennedy test may be due
to compression of structures other than the supraspinatus tendon.
The presence of neuropeptides consistent with pain sensation has
been recently confirmed in the long head of biceps tendon thus
confirming this structure as a possible source of shoulder pain
(Alpantaki et al., 2005). The result of the current study may also
help to explain the relatively poor accuracy of HawkinseKennedy
test in diagnosing rotator cuff pathology (Hughes et al., 2008).
Our results are also consistent with other observations that have
not been able to demonstrate supraspinatus contact with the
acromion or coraco-acromial ligament during the HawkinseKennedy test (Roberts et al., 2002; Struhl, 2002). However, Pappas et al.
(2006) observed subacromial contact of the supraspinatus or
infraspinatus in their magnetic resonance imaging (MRI) investigation, while Valadie et al. (2000) observed that the coracoacromial ligament was in contact with rotator cuff tendons or
biceps tendon in four cadaveric specimens during the test although
it was not stated if supraspinatus tendon was implicated. Our
results add to the previous literature by basing our conclusions on
direct measurement of pressure and not just observation.
One potential limitation of our study is that the measurement
error in the pressure transducer may have obscured any real differences between the provocative and non-provocative positions of the
HawkinseKennedy test. However, we established that the device
demonstrated high levels of inter-device and re-test reliability.
This suggests that the pressure transducer had sufficient reliability
to overcome measurement error and detect large increases in
subacromial pressure in the provocative positions during
HawkinseKennedy test position.
A further limitation is that the results of this study are based on
a single cadaver. To partly account for this we used a rigorous
single-case design analysis. Finally, a limitation is that the subacromial bursa, a common source of pain in impingement
syndrome (Lewis, 2009), was removed from the cadaver during
dissection. However, our procedure allowed us to test whether the
supraspinatus tendon is compressed against the under surface of
the coraco-acromial ligament as proposed by the test developers
(Hawkins and Kennedy, 1980).
5. Conclusion
Findings of the current study provide evidence of the anatomical validity of HawkinseKennedy test, and provide new evidence
that suggest that structures other than the rotator cuff tendons may
be impinged during this test.
Acknowledgements
This work was supported by La Trobe University Faculty of
Health Sciences Research Grant No. 2006/A1.
The authors gratefully acknowledge Cameron Grant and Frank
Neibling (Faculty of Health Sciences Technical Services Unit) for
development and production of the 4-channel force sensitive
resistor variable offset amplifier.
References
Alpantaki K, McLaughlin D, Karagogeos D, Hadjipavlou A. Sympathetic and sensory
neural elements in the tendon of the long head of the biceps. Journal of Bone
and Joint Surgery 2005;87(7):1580e3.
Bongers PM. The cost of shoulder pain at work. BMJ 2001;322:64e5.
Chung C, Pedowitz R, Resnick D. Magnetic resonance imaging in orthopaedic sports
medicine. London: Springer; 2008.
Gorman B, Allison D. Statistical alternatives for single-case designs. In: Franklin R,
Allison D, Gorman B, editors. Design and analysis of single-case research.
Mahwah, NJ: Lawrence Erlbaum Associates; 1997. p. 159e214.
Green R, Shanley K, Taylor N, Perrott M. The anatomical basis for clinical tests
assessing musculoskeletal function of the shoulder. Physical Therapy Reviews
2008;13(1):17e24.
Harbst K, Ottenbacher K, Harris S. Inter-rater reliability of therapists’ judgments of
graphed data. Physical Therapy Reviews 1991;71:107e15.
Hawkins R, Kennedy J. Impingement syndrome in athletes. American Journal of
Sports Medicine 1980;8:151e8.
Hegedus E, Goode A, Campbell S, Morin A, Tamaddoni M, Moorman C, et al. Physical
examination tests of the shoulder: a systematic review with meta-analysis of
individual tests. British Journal of Sports Medicine 2007;42:80e92.
Hughes PC, Taylor NF, Green RA. Most clinical tests cannot accurately diagnose
rotator cuff pathology: a systematic review. Australian Journal of Physiotherapy
2008;54(3):159e70.
Levangie P, Norkin C. Joint structure and function. Philadelphia: FA Davis; 2005.
Lewis J. Rotator cuff tendionopathy. British Journal of Sports Medicine 2009;
43:236e41.
Mullaney MJ, McHugh M, Johnson C, Tylor T. Reliability of shoulder range of motion
comparing a goniometer to a digital level. Physiotherapy Theory and Practice
2010;26(5):327e33.
McClure P, Michener L, Sennett B, Karduna A. Direct 3-dimensional measurement of
scapular kinematics during dynamic movements in vivo. Journal of Shoulder
and Elbow Surgery 2001;10:269e77.
Neer C. Impingement lesions. Clinical Orthopaedics and Related Research 1983;
173:70e7.
Nourbakhsh M, Ottenbacher K. The statistical analysis of single-subject data:
a comparative examination. Physical Therapy Reviews 1994;74(8):768e76.
Pappas C, Blemker S, Beaulieu C, McAdams T, Whalen S, Gold G. In vivo anatomy of
the Neer and Hawkins sign positions for shoulder impingement. Journal of
Shoulder and Elbow Surgery 2006;15:40e9.
Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands: prevalences,
consequences and risk groups, the DMC(3)-study. Pain 2003;102:167e78.
Portney L, Watkins M. Foundations of clinical research. Applications to practice. 2nd
ed. Upper Saddle River, NJ: Prentice Hall Health; 2000.
Roberts C, Davila J, Hushek S, Tillet E, Corrigan T. Magnetic resonance imaging
analysis of the subacromial space in the impingement sign positions. Journal of
Shoulder and Elbow Surgery 2002;11(6):595e9.
Struhl S. Anterior internal impingement: an arthroscopic observation. Arthroscopy
2002;18(1):2e7.
Valadie 3rd A, Jobe C, Pink M, Ekman E, Jobe F. Anatomy of provocative tests for
impingement syndrome of the shoulder. Journal of Shoulder and Elbow Surgery
2000;9(1):36e46.
Van der Windt D, Koes B, de Jong B, Bouter L. Shoulder disorder in general practice:
incidence, patient characteristics, and management. Annals of the Rheumatic
Diseases 1995;54:959e64.
Wuelker N, Plitz W, Roetman B. Biomechanical data concerning the shoulder
impingement syndrome. Clinical Orthopaedics and Related Research 1994;
303:242e9.
Yamamoto N, Muraki T, Sperling J, Steinmann S, Itoi E, Cofield R, et al. Impingement
mechanisms of the Neer and Hawkins signs. Journal of Shoulder and Elbow
Surgery 2009;18:942e7.
Yano Y, Hamada J, Tamai K, Yoshizaki K, Sahara R, Fujiwara T, et al. Different
scapular kinematics in healthy subjects during arm elevation and lowering:
glenohumeral and scapularothoracic patterns. Journal of Shoulder and Elbow
Surgery 2010;19:209e15.