The site of focal osteomyelitis lesions in foals
advertisement

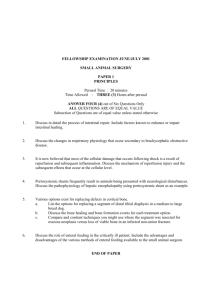
The site of focal osteomyelitis lesions in foals E. C. Firth' and S. A. Goedegebuure2 SUMMARY The long bone ends of foals with infectious disease were sawn into sagittal slabs, washed and inspected. Tissue suspected to be abnormal on the basis of change of colour and consistency was radiographed, and then decalcified and examined histologically. The exact site of 140 focal osteomyelitis lesions from 18 foals was determined. There were more lesions in the epiphysis than the metaphysis. Epiphyseal lesions were in specific sites within a given epiphysis, and in most epiphyses the lesions were at the site of thickest cartilage. Metaphyseal lesions in the metacarpal, metatarsal and distal radial growth plates tended to be on the more inclined parts of the growth plate. INTRODUCTION Infectious arthritis is a serious disease of young foals and most cases are complicated by the concurrent presence of osteomyelitis in the bone adjacent to the affected joint. In one study, about 70% of foals presented for examination of joint ill had osteomyelitis in one or more bones (2). The most commonly affected sites have been described in radiographic and pathological studies (1, 4, 5). No reason for the apparent predisposition of some bone ends to osteomyelitis has so far been given, and the suggestion that infection occurs more often in one particular site than another within a given bone end has not been put forward. One of us noted that epiphyseal osteomyelitis often occurred at or near the site of the thickest 'articular' cartilage in a particular bone end. The sites of thick cartilage in the major joints of the foal has recently been described (3). In this paper we describe the sites of focal osteomyelitis lesions in young foals with naturally occurring haematogenous arthritis/osteomyelitis. MATERIALS AND METHODS The bones of 18 foals aged 4-150 days old were obtained from routine post-mortem material. The cause of death or euthenasia is shown (Table 1). All foals included had a history of predisposition to infection (early birth, late standing or sucking after birth, perinatal disease, etc), had evidence of infectious disease prior to death or at necropsy, and had bone lesions in more than one limb. The limbs were boned out, and the ends of the long bones were sawn off about 5 cm from the metaphyseal growth plate, so that metaphysis, physis, epiphysis and articular cartilage could be examined. The following bones were collected: proximal and distal humerus, proximal and distal radius, distal third metacarpal bone, proximal and distal femur, proximal and distal tibia, talus, and distal third metatarsal bone. The bones were sawn into sagittal slabs 4-7 mm thick with a bandsaw, washed in running water, and examined visually under bright light, in most cases before fixation in 4% buffered formalin. Each slab was numbered. The slabs were radiographed in a Faxitron 43805N X-ray apparatus (HewlettPackard, McMinnville, CA, USA) and the films were hand developed. The visual and radiographic examinations were performed to determine the presence and site of focal lesions. Defects which were so extensive that the whole epiphysis or metaphysis was destroyed, making it impossible to pinpoint the site at which the process had begun, were discarded from the study. Localised lesions (i.e. less than 10 mm diameter) were detected by observing round or irregularly shaped discoloration (whitening) of the cancellous bone or absence of bone and/or cartilage with replacement by exudate or soft necrotic tissue. 1 2 Dept of Large Animal and General Surgery, State University Utrecht, P.O. Box 80.153, 3508 TD Utrecht, The Netherlands. Present address: Massey University, Palmerston North, New Zealand. Dept of Veterinary Pathology, State University Utrecht, P.O. Box 80.158, 3508 TD Utrecht, The Netherlands. THE VETERINARY QUARTERLY, VOL. 10, No. 2, APRIL 1988 99 Table I. Cause of death or reason for euthanasia of 18 foals with focal osteomyelitis. All bacteriological determinations were conducted on material collected at necropsy, except those mentioned under 'joints', synovia from which was collected by sterile arthrocentesis at the time of clinical examination. Bone culture at necropsy implies sampling of macroscopically visible lesions. *Synovia was repeatedly negative at the time of distal radial osteomyelitis, 5 months before euthanasia. TT=tibio-tarsal, BHS=beta haemolytic streptococcus, DJD=degenerative joint disease, MtPJ=metatarsophalangeal joint, Mt3=third metatarsal bone, WPN=Dutch Warmblood. Foal Breed 8401 WPN 10 8410 WPN 4 8411 WPN 8412 Age days Other Necropsy Lesions Culture metaphysitis, path. fracture Mt3 Proteus fracture site polyserositis, meningitis polyarthritis, omphalitis E.coli bones/organs 11 polyarthritis E.coli T-T joint 12 omphalitis, polyarthritis culture negative 28 osteomyelitis tibia E.coli distal tibia 8419 mini Shet 8507 WPN 10 polyserositis E.coli organs 8512 WPN 14. polyarthritis E.coli 2 joints 8521 WPN 30 bronchopneumonia osteomyelitis L&R dist, femurs and R ulna BHS lung, C.equi lung abscess 8602 WPN 24 bronchopneumonia polyosteomyelitis E.coli 4 joints 8603 WPN 21 polyosteomyelitis E.coli 2 joints; several bones 8309 WPN omphalophlebitis, persistent urachus, polyarthritis, rib osteomyelitis BHS navel, E.coli femur, ulna, rib 793 WPN 11 omphalitis, bronchopneumonia, polyosteomyelitis E.coli bones/organs 8004 WPN 28 osteomyelitis proximal , humerus not done 8037 WPN 150 DJD radiocarpal joint synovia negative* 8119 pony polyarthritis not done 8123 WPN 120 physitis Mt3, arthritis MtPJ synovia culture negative 8127 WPN 13 polyarthritis/osteomyelitis omphalophlebitis, endocarditis Klebsiella bones 8510 WPN polyosteomyelitis not done 100 19 THE VETERINARY QUARTERLY, VOL. 10, No. 2, APRIL 1988 Suspected changes were recorded by photography, usually of the whole series of slabs of the bone end concerned, in order to show the exact site of the lesion. In some cases, photography of (part of) an individual slab was used to record the nature and form of the lesion. On the radiographs, the presence of localised lesions was suggested by focal osteolysis. When visual and/or radiographic evaluation indicated that lesions were present, or might be present, the part concerned was decalcified in 35% formic acid and 6.8% sodium formate, rinsed in running water, and embedded in paraffin. Sections were cut at 6u and stained with haematoxylin and eosin (HE) and Azan. In this group of young foals, the diagnosis of osteomyelitis was based on the presence of history typical of bone infection (2), the multifocal nature of the disease, evidence of other infectious disease in other organs at necropsy, and histological findings in bone and carti- lage. In some cases clinical and laboratory findings were also contributory. Culture of synovial fluid taken at clinical examination was positive in 3 foals. In 6 foals, bacteriological culture of suspected abnormal bone was performed after sawing of the bone end, flaming the lesion, and inserting the swab deep into the bone lesion. Laboratory culture techniques have been previously described (2). For inclusion in this study, the histological criteria consistent with osteomyelitis included one or more of: exudate in marrow spaces and vessels with polymorphonuclear or mononuclear cellular infiltration, thrombosis of vessels, necrosis of marrow tissue or bone or cartilage, and absence of bone or cartilage and replacement by exudate, necrotic debri, or fibrosis. RESULTS Of a total of 35 sets of limbs sawn and examined, those of 18 foals were included in the study. The others were rejected because no lesions were found on macroscopic or radiological examination, or because the nature of the lesions did not support the diagnosis of active or chronic bone infection. E.coli was by far the most commonly isolated micro-organism (Table 1). In almost all cases, the focal lesions were detected by visual examination, because discoloration or bone loss was visible on one or both surfaces of one or more slabs. The discoloration was white or yellow, and it surrounded areas of focal bone loss, which was evidenced by a small or large cavity filled with glistening exudate or dull necrotic material. The lesions were all at the junction of bone and cartilage, and occurred at, or very close to, the junction of epiphyseal bone and the cartilage covering the articular aspect of the epiphysis, or at the junction of bone and physeal cartilage, usually on the metaphyseal side of the growth plate. These lesions have previously been referred to as E or P lesions respectively (2). Extension of the lesion into epiphyseal bone was evident in some cases, and in others there was extension into the deeper layers of cartilage. In some instances there was penetration of the articular surface by the infectious process. Almost all lesions near the metaphyseal growth plate showed cartilage destruction and either radiological and/or histological evidence of involvement of bone on the opposite side of the growth plate. The presence of the lesions was confirmed by histological study, and the extent of the lesions was often better demonstrated by radiology. Usually, the extent of bone loss evident on radiological and/or histological exam- inations indicated the probable site of origin of lesions near the metaphyseal growth plate. The incidence of lesions in the various foals, and a breakdown of the number of lesions in each bone end, are shown in Table 2 and Fig. 1 respectively. The sites of the focal osteomyelitis lesions in each bone end were as follows. Proximal humerus. There were 6 lesions in the caudo-central aspect of the epiphysis. In some cases the lesion extended through up to 4 slabs. The apparent site of origin of the process was not constant, being the epiphysis in 4 cases and the metaphysis in 2 cases, and the lesion extended through the growth plate. There was one metaphyseal lesion found at the proximal humeral growth plate ventral to the major tubercle. THE VETERINARY QUARTERLY, VOL. 10, No. 2, APRIL 1988 101 Table 2. Site of lesions found in long bone ends of 18 foals. The first number identifies the foal, R=right, L=left; the last digit(s) indicate the slab(s) involved. E=epiphyseal osteomyelitis, P=osteomyelitis at the physis. a=radiographically or histologically detected bone lysis. MtHI=third metatarsal bone, McIII=third metacarpal bone, T=trochanter, U=ulna. 8412L 3 L 6 R5-7 R 4 P P Proximal Tibia Distal Tibia Distal Femur Proximal Femur 8401R E* 8410R10 L 3 E 8411R 9 LIO E* Talus MtIII E 8411R 6 E 8411R 9 P* E 84121,81-2 E* 8412L 4 E/P* R 3 P 8412L 7 P* 8412L 3 P* 8412R 6 P* 8412L 10 E* R 11 E* P* P 8419L 2 E* R5-6 E* 8512R2-3 P 8419L2-3 P* R 3 P* 8512R2-4 E* 8521R2-4 E* L2-4 E* 8309R6-8 E* R 2 L2-3 L2-3 L 6 E* E* E* E* P* P* E L1-2 P 8507L 4 E L 5 E* 8507R 6 8602L2-3 E* 8602L 2 P* L8-9 E* L2-4 P/E* 8602L 4 P* 8602L 2 8603R2-3 E* 8603L 5 E* R6-7 E* L2-4 P/E* L 6 P* R3-4 E/P* L6-7 E* E* R 5 L2-3 E* 8603L 4 E* L 7 E* R 4 E* 8507R 2 R 7 P/E* P* R 3 R 4 L3-4 P/E 8507LB 2 P* 8510L 2 R 2 15 Distal humerus. 25 E* E* 8510 L 5 8603L L L , R R E* E* E* E* E* 8603L L L L L 2 4 4 6 P* E* E* P* 7 P* 8510R 3 E* 4 E/P* 11 3 5 5 7 4 P* P* 3 6 15 There were 9 epiphyseal lesions in the distal humeral epiphysis; 3 of these were in medial slabs (trochlea) and 6 in lateral slabs (capitulum). The capitulum lesions were all in its caudal half. There was one metaphyseal lesion, which had broken through the caudo-lateral aspect of the metaphysis into the surrounding fascia. 102 THE VETERINARY QUARTERLY, VOL. 10, No, 2, APRIL 1988 Proximal Humerus 84111. 4 Distal Humerus Proximal Radius Ulna Distal Radius 8410R 3 E* 8411R1-2 R 10 L1-3 L 13 R 9 P* P* P* P P* 8412L 6 P* 8419R5-7 E* L5-8 E* 8419L 8 E E E R4-6 E 8412L 3 E/P* 8419L2 -3 P* 8412L 7 R 7 8512L 5 8507L 3 8507R 3 E/P* 8507R 3 E/P* 8602L 2 8603R 3 R R L L 9 2 6 6 8411L 8 E 8419R 6 P* P* P R 4 E* 8309R 1 8309L 2 R8-9 R 8 L 8 L 8 E* P* E* P* E* 8507L 6 P* 8507R L R L P* E* 8603L2-6 P/E* R2-5 P/E* McIII 3 3 8 8 E 8507R 4 L 4 P* P E* E* E* 8602R7-8 P* E* E* E* E* E* 8603L R P* P* 8603L L R R R 2 8 2 2 8 R 7 R 8 P* E* P* E* E* P* P* 7903R 2 L 7 E* P* 8004R 2 P* 8037R 6 P* R 7 P* 8127R 2 P* 8 8119L 2 P* L 7 P* R7-8 P* 10 1 4 8123R 5 P* 8127L 7 P* 34 8 . 103 CA Fore limb CR 1 6 Prox. radius Distal humerus Proximal humerus CR Axial Lat. Med. Lat./Med. Distal radius Axial Distal Mc3 Hind limb Lat. Med. Distal femur Prox. femur R Axial Med. CR DA A Lat. Distal tibia Prox. tibia CA CR Lat./Med. Med. ridge Lat. ridge Axial Distal Mt3 Talus Figure I. Schematic drawings of the sagittal slabs in which most lesions were detected in the bone ends. The numbers refer to the numbers of lesions found at each site indicated. 104 THE VETERINARY QUARTERLY, VOL. 10, No. 2, APRIL 1988 Ulna. Four lesions were found in the metaphysis of the olecranon, but in all cases there was either radiographic and/or histological evidence of involvement of both the metaphysis and the apophysis. Proximal radius. One lesion was found in the epiphysis close to the synovial fossa. Distal radius. There were 13 lesions in the epiphysis of either the medial process of the radius (5) or in the lateral styloid process (8). The medial lesions were always at the junction of cartilage and bone and were always focal; several, but not all, of the lateral styloid process lesions were demonstrated to be in its most cranial part, adjacent to the fibrous tissue separating the process from radial epiphysis. In other cases, the lateral styloid process contained more than one lesion and/or copious exudate, and extension of the infiltrate into the radial epiphysis and into the distal radial metaphysis was observed. The 21 P type lesions were in moste cases found in the inclined parts of the distal radial growth plate. The localisations were cranial inclination (1), caudal inclination (1) or both the cranial and caudal inclinations (2) of the growth plate in the medial aspect of the radius; there were a further 3 lesions at the junction of the perichondrium and growth plate on the caudal aspect of the bone. On the lateral aspect of the radius, the sites were the most caudal (5) or more cranial parts of the growth plate (7) dorsal to the lateral styloid process. In several of the caudolaterally sited lesions, association with infiltrate or lysis in the radial epiphysis or lateral styloid process was observed. Between the two processes of the radius i.e. axially, there were 2 lesions on the cranial aspect of the growth plate. Third metacarpal bone. One epiphyseal lesion was observed just caudal to the most distal aspect of the convexity of the epiphysis, on the lateral side. There were 7 metaphyseal lesions in the cranial (4) and caudal (3) inclinations of slabs lateral (5) or medial (1) to the median sagittal ridge, and 1 of these lesions was in the central slab containing the median ridge. Proximal femur. There were 15 lesions detected in 8 bones from 5 foals. There were 7 lesions in the epiphysis, and 2 of these were adjacent to the insertion of the round ligament. The other 5 were at the most medio-ventral aspect of the epiphysis, and all but one of these 5 had involvement on both sides of the growth plate. The lesions appeared to have originated in the metaphysis. The other 7 lesions were found at various sites along the metaphyseal growth plate, and one lesion was in the major trochanter. Distal femur. There were 25 lesions detected in 18 bones from 11 foals. The most common site (14 lesions) was in the medial femoral condyle, caudal and dorsal to the articular contact surface. Five lesions were found in the lateral femoral condyle at the same level as in the medial condyle. There were 5 lesions in the lateral femoral trochlear ridge (in its proximal (4) or middle (1) third), and there was one lesion in the medial femoral trochlear ridge. Proximal tibia. There was one lesion in an identical site in the lateral part of the left and right proximal tibial epiphyses of one foal. On the medial aspect of one of these bones there was a metaphysitis of the proximal tibial growth plate. Distal tibia. There were 5 lesions in the cranio-distal aspect of the distal intermediate ridge, and one lesion in the most caudo-dorsal aspect of the ridge. There was 1 lesion in the fibular styloid process. Metaphyseal lesions were detected in the cranial inclination (3) and caudal inclination (1) of the distal tibial growth plate; one of these lesions was lateral, the other 3 were in the central part of the bone. THE VETERINARY QUARTERLY, VOL. 10, No. 2, APRIL 1988 105 Talus. There were 5 lesions found in the tali of 1 animal. In both tali there was a lesion at the junction of cartilage and bone in the distal part of the medial talar ridge; both lesions were 15 mm from the insertion of the joint capsule. There was a lesion in the most distal aspect of both lateral talar ridges, and in the left talar ridge there was an additional lesion in the mid-region of the convexity of this ridge. In another foal there was one lesion in the mid region of the convexity of the medial ridge. Third metatarsal bone. There were 4 epiphyseal lesions, 1 of which was caudal and 3 of which were cranial to the most distal point in the convexity of the epiphysis. All but one of these lesions were in the median sagittal ridge. The 11 metaphyseal lesions were in the 'through' (1 lesion) or on the cranial (5) or caudal (5) inclinations of the growth plate in slabs lateral (6) or medial (5) to the median sagittal ridge. In the cases of the epiphyseal lesions in the medial styloid process and lateral styloid processes of the radius, the medial and lateral condyles and lateral trochlear ridge of the distal femur, proximal humerus, proximal femur, and intermediate ridge of the tibia, the site of the lesions in these parts of the bones was in the direct vicinity of the thickest cartilage in that part of the bone. In some bones, the plane of sectioning, or bone growth since the time of onset of necrosis, meant that the lesion was not exactly at the site of thickest cartilage, but within 4-5 mm of it. Almost all of the P type lesions (metaphysitis) in the distal radius and metacarpus and metatarsus were on the inclined parts of the growth plate. In the proximal humerus and proximal femur, the lesion appeared in some cases to have begun in the metaphysis at a site where it is covered by articular cartilage i.e. in the centrocaudal part of the bone end. In many subacute lesions, exudate and cells in transphyseal vessels and on both sides of the growth plate were present. In many other cases, communication through the growth plate was a result of direct extension of the lesion through the physeal cartilage. DISCUSSION We chose to examine the site of focal osteomyelitis lesions in foals because defining these sites may contribute to increased knowledge of the pathogenesis of polyosteomyelitis and provide insight into the sites of articular cartilage which should be especially well evaluated radiologically and arthroscopically in the diagnosis and treatment of the disease. Ideally, infection experiments would provide more accurate data, but these were not possible, and we thus resorted to examination of naturally occurring disease. Strictly speaking, the definitive diagnosis of bacterial osteomyelitis can be made only by observing the characteristic histological and radiological changes in tissue from which pathogenic micro-organisms have been cultured. In examining focal lesions which have not extended to the outside through bone or cartilage, it is impossible to culture the lesions before sawing of the bones, because it is impossible to predict the site of possible bone lesions without the benefit of clinical and radiological examinations in vivo. Many of the focal lesions were too small to have been demonstrated on clinical radiographs in any case, and for this reason, and due to expense, we did not radiograph the limbs collected from routine post- mortem cases. Others have expressed the difficulty in diagnosing chronic bone infection on the basis of histological changes (10). We excluded foals with lesions which had features of other disease processes (e.g. retained cartilage). Although we 106 THE VETERINARY QUARTERLY, VOL. 10, No. 2, APRIL 1988 proved infection in the joint or bone of only half the foals in this study, we believe that the combination of clinical and pathological data, the multifocal nature of the disease in the foals included in the study, and the radiological and histological features of the lesions observed were sufficient to justify at least a strongly tentative, if not conclusive, diagnosis of infection as the cause of arthritis and osteomyelitis in these foals. Of the 140 lesions observed, 119 showed obvious bone loss on microradiographs or histological preparations. There are no other disease processes in very young foals which cause multifocal bone and/or cartilage loss. This meant that the difficulty in making the diagnosis on the basis of chronic infiltrative changes in affected bone was alleviated. In cases without lysis or necrosis, the obvious infiltrate of exudate and cells pointed to the presence of (sub)acute inflammatory change. The lesions were found at the junction of bone and the metaphyseal growth plate cartilage, or at the junction of bone and epiphyseal growth cartilage (7,8); (the latter has also been referred to (9) as the spherical physis or secondary physis to more precisely indicate that we mean the growth plate by which the epiphysis expands in all directions i.e. the growth plate surrounding the secondary ossification centre). Siffert (8) has indicated that regardless of their anatomical location, growth cartilages apparently function in a similar biological manner, and this supports the use by Nixon (6) of the therm 'metaphyseal equivalent site' to indicate the significance of the vascular arrangement in the pathogenesis of haematogenous osteomyelitis in flat bones in man. This vascular arrangement, in which sharp loops in marrow capillaries open into wide sinusoids and produce sluggish circulation, has been a constant feature of explanations for the localisation of lesions at the cartilage/bone junction. In the distal humerus, the site of the lesions within the capitulum or trochlea was not constant. In the case of the talus, there were lesions at the site of thickest cartilage, but also at sites with thinner cartilage. In the case of the medial styloid process of the radius, femoral condyles, distal tibia, and proximal humerus, it could be seen that the site of focal lesions was exactly adjacent to the thickest cartilage on the slabs examined in this study, and these sites have previously been shown to be the sites of thickest cartilage in the respective parts of the bone end (3). In the lateral styloid process of the radius and proximal femur, the focal lesions were close to the thickest cartilage, but not at an absolutely constant site. This may be due to the small size and rapid rate of enchondral ossification in the lateral styloid process and to the possible role of the insertion of the round ligament in the proximal femur. The incidence of epiphyseal lesions found in the proximal radius and proximal tibia was extremely low (only 4 lesions). The distribution of the lesions in the various bone ends agrees with a previous study (1), except for the higher incidence of epiphyseal lesions in the distal humerus, and of lesions in the proximal femur. The difference in the latter case may be due to the greater difficulty in examining the hip area in clincial cases. We confirm the known (1) predisposition sites within some epiphyses such as the site in the lateral and medial femoral condyles and distal intermediate ridge of the tibia, and present new apparently predisposed sites (medial styloid process radius, proximal humerus). We presume the relationship of lesion site and thick cartilage to be associated with local vascular morphology. It appeared that more lesions occurred on inclined parts of the growth plate than on those parts of the physis at 90 degrees to the long axis of the bone. It also appeared that the lesions were on the most inclined part of the physis, but this THE VETERINARY QUARTERLY, VOL. 10, No. 2, APRIL 1988 107 could not be substantiated since detailed morphological studies of the developing equine growth plate are lacking. Because of the greater site variation in the metaphysis lesions than in the epiphysis lesions, and because of insufficient numbers, we do not at this time have an explanation for the apparent predisposi- tion site within a given metaphysis. This study of focal lesions provided clear evidence of the role of transphyseal vessels in permitting infection to cross the growth plate, although invasion directly through cartilage may also occur. ACKNOWLEDGEMENTS The authors are extremely grateful to Mr. A. Klarenbeek for his skillful preparation of bone slabs, radiographs and histological slides. They also thank Mr. F. Blok for illustrative material and Ms. J. de Graaf-de Hart for developing the radiographs. REFERENCES I. Dik KJ. Rontgenologische aspecten van polyarthritis bij veulens. Thesis, Utrecht, 1981. 2. Firth EC, Dik KJ, Goedegebuure SA, Hagens FM, Verberne LRM, Merkens HW, and Kersjes AW. Polyarthritis and bone infection in foals. Zentralbl Veterinarmed 1980; 27: 102-24. 3. Firth EC and Greydanus Y. Cartilage thickness measurements in foals. Res Vet Sci 1987 (accepted). 4. Goedegebuure SA, Dik KJ, Firth EC, and Merkens HW. Polyarthritis and polyosteomyclitis in foals. Berl Tierarztl Wschr 1980; 63B: 126-31. 5. Martens R and Auer JA. Hematogenous septic arthritis and osteomyelitis in the foal. Proc Am Assoc Eq Pract 1980; 47-63. 6. Nixon GW. Hematogenous osteomyelitis in metaphyseal equivalent zones. Am J Rontg 1978; 130: 123-9. 7. Siffert RS. The effect of trauma to the epiphysis and growth plate. Skel Radiol 1977; 2: 21-30. 8. Siffert RS. Classification of the osteochondroses. Clin Orth and Rel Res 1981; 158: 10-8. 9. Ogden JA. In: Fundamental and Clinical Bone Physiology, Lippincott, Philadelphia, Editor M. Urist. 10. Waldvogel FA, Medolf G, and Schwartz MN. Osteomyelitis: A review of clinical features, therapeutic aspects and unusual aspects. New Eng J Med 1970; 282: 198-206. 108 THE VETERINARY QUARTERLY, VOL. 10, NO. 2, APRIL 1988