Lateral Sleeping Position Reduces Severity of Central Sleep Apnea
advertisement

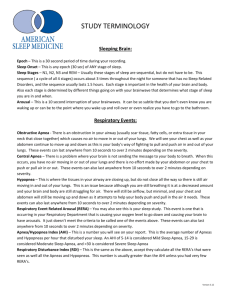
Lateral Sleeping Position Reduces Severity of Central Sleep Apnea / CheyneStokes Respiration Irene Szollosi BSc1,2; Teanau Roebuck BAppl Sc1; Bruce Thompson PhD1; Matthew T Naughton MD1,2 Department of Allergy Immunology and Respiratory Medicine, Alfred Hospital, Melbourne, Australia; 2Department of Medicine, Monash University, Melbourne, Australia 1 wave sleep, 15.9 ± 6.4 events per hour vs 5.4 ± 2.9 events per hour [p < .01]; rapid eye movement sleep, 38.0 ± 7.3 events per hour vs 11.0 ± 3.0 events per hour [p < .001]). Lateral position attenuated apnea and hypopnea associated desaturation (supine 4.7% ± 0.3%, lateral 3.0% ± 0.4%; p < .001) with no difference in event duration (supine 25.7 ± 2.8 seconds, lateral 26.9 ± 3.4 seconds; p = .921). Mixed apneas were longer than central (29.1 ± 2.1 seconds and 19.3 ± 1.1 seconds; p < .001) and produced greater desaturation (6.1% ± 0.5% and 4.5% ± 0.5%, p = .003). Lateral position decreased desaturation independent of apnea type (supine 5.4% ± 0.5%, lateral 3.9% ± 0.4%; p = .003). Conclusions: Lateral position attenuates severity of CSA-CSR. This effect is independent of postural effects on the upper airway and is likely to be due to changes in pulmonary oxygen stores. Further studies are required to investigate mechanisms involved. Keywords: Central sleep apnea, body position, ventilatory control Citation: Szollosi I; Roebuck T; Thompson B et al. Lateral Sleeping Position Reduces Severity of Central Sleep Apnea / Cheyne-Stokes Respiration. SLEEP 2006;29(8):1045-1051. Introduction: The influence of sleeping position on obstructive sleep apnea severity is well established. However, in central sleep apnea with Cheyne Stokes respiration (CSA-CSR) in which respiratory-control instability plays a major pathophysiologic role, the effect of position is less clear. Study Objectives: To examine the influence of position on CSA-CSR severity as well as central and mixed apnea frequency. Methods: Polysomnograms with digitized video surveillance of 20 consecutive patients with heart failure and CSA-CSR were analyzed for total apnea-hypopnea index, mean event duration, and mean oxygen desaturation according to sleep stage and position. Position effects on mixed and central apnea index, mean apnea duration, and mean desaturation were also examined in non-rapid eye movement sleep. Results: Data are presented as mean ± SEM unless otherwise indicated. Group age was 59.9 ± 2.3 years, and total apnea-hypopnea index was 26.4 ± 3.0 events per hour. Compared with supine position, lateral position reduced the apnea-hypopnea index in all sleep stages (Stage 1, 54.7 ± 4.2 events per hour vs 27.2 ± 4.1 events per hour [p < .001]; Stage 2, 43.3 ± 6.1 events per hour vs 14.4 ± 3.6 events per hour [p < .001]; slow- ment of cardiovascular disease,7 occurring in 2% to 4% of the general adult population.8 Upper-airway instability during sleep and an inadequate capacity of upper-airway musculature to maintain airway patency is thought to be the main pathophysiologic event, with respiratory-control instability (loop gain) playing a potential role in some patients.9,10 It has been established that OSAHS severity as measured by the apnea-hypopnea index (AHI) is increased in the supine position.11 Even in nonpositional OSAHS, the duration of respiratory events and the consequent hypoxemia is more marked in the supine position.12 This effect is attributed to gravitational effects on the upper airway13 leading to increased upper-airway collapsibility while supine. In support of this, Penzel et al confirmed that body position has a significant impact on the pharyngeal critical closing pressure, an objective measure of upper-airway collapsibility.14 In addition, the optimal continuous positive airway pressure required to treat OSAHS has been demonstrated to be approximately 2 cmH2O higher in the supine position compared with the lateral.15 The impact of position in CSA-CSR is less clear. Recently, it has been reported that patients with heart failure have a preference for the lateral sleeping position16 and, furthermore, that the right lateral decubitus position is preferred over the left lateral decubitus position.17 In addition, Sahlin et al have shown that central AHI is increased during supine sleep compared with nonsupine sleep.18 However, previous investigators have also observed that upper-airway instability is common during CSA-CSR, with many patients exhibiting mixed apneas in which pharyngeal occlusion prevents the immediate resumption of airflow when ventilatory effort returns.19,20 It remains unclear whether upper-airway col- INTRODUCTION SLEEP-RELATED BREATHING DISTURBANCES OCCUR IN UP TO 50% OF PATIENTS WITH HEART FAILURE, WITH 40% EXHIBITING CENTRAL SLEEP APNEA and CheyneStokes respiration (CSA-CSR) and a further 10% of patients exhibiting obstructive sleep apnea hypopnea syndrome (OSAHS).1 CSA-CSR is attributed to respiratory-control instability in which periodic hyperventilation drives PaCO2 below the apneic threshold, such that central drive and efferent output to the respiratory pump muscles are transiently reduced or absent. Proposed mechanisms for hyperventilation include stimulation of pulmonary vagal afferents secondary to pulmonary congestion2 and heightened sympathetic activation.3,4 Increased chemosensitivity of the central and peripheral chemoreceptors and the underlying increase in circulation time associated with heart failure5,6 predisposes to ventilatory instability that manifests as CSA-CSR. OSAHS is a known independent risk factor for the develop- Disclosure Statement This was not an industry supported study. Dr. Naughton is on the medical advisory board of ResMed Inc. Ms. Szollosi, Roebuck, and Dr. Thompson have indicated no financial conflicts of interest. Submitted for publication November 16, 2005 Accepted for publication March 21, 2006 Address correspondence to: Matthew T. Naughton, Alfred Hospital, PO Box 315, Prahran, Victoria, 3181, Australia; Tel: +61 3 9276 3770; Fax: +61 3 9276 3601; E-mail: m.naughton@alfred.org.au SLEEP, Vol. 29, No. 8, 2006 1045 Influence of Position on CSA-CSR Severity—Szollosi et al Figure 1—Representative polygraph from 1 subject, showing classification of central, mixed, and obstructive apneas while supine. CSA-CSR. Measurements included electroencephalogram (C4A1, C3-A2, O2-A1, O1-A2), EOG, submental electromyogram, electrocardiogram, oronasal flow measured with thermistor and nasal pressure cannula (Pro-Tech Services, Mukilteo,WA), ribcage and abdominal effort measured by piezoelectric sensors, calibrated body position sensor, SpO2 with 2-second averaging time (Oxypleth, Novametrix, Wallingford, CT), esophageal pressure manometry (Millar Instruments, Houston,TX), and snoring sound. All signals were stored onto a computerized polysomnographic data acquisition and analysis system (Compumedics Eseries, Abbottsford, Australia). In order for lateral position to be confirmed, patients had to have 1 shoulder elevated visually on the digitized video and the position sensor reading either left or right position; supine sleep required both shoulders to be in contact with the bed on video and confirmed with position sensor. Sleep stages were manually scored as previously described.21 Apneas were scored in the absence of oronasal flow in both the thermistor and nasal cannula signals—obstructive if continued effort persisted in the ribcage and abdominal bands or esophageal pressure, central in the absence of ventilatory effort, and mixed if there was an absence of oronasal flow when ventilatory effort resumed. Hypopneas were scored on the basis of a 50% or greater reduction in oronasal flow associated with a 2% desaturation and/or arousal—obstructive in the event of paradoxical motion in the effort bands or increasing esophageal pressure amplitude and central if ribcage and abdominal effort remained in phase22 or esophageal pressure swings decreased. Examples of central, mixed, and obstructive apneas are shown in Figure 1. CSA-CSR was defined as an AHI greater than 5 events per hour, with fewer than 25% of events being obstruc- lapse favored by the supine position is important in the initiation or propagation of CSA-CSR. Our primary aims were to assess the effect of position on the severity of CSA-CSR, as measured by AHI, respiratory-event duration, and hypoxemia associated with events, while controlling for sleep-stage effects. Secondary aims were to examine whether mixed apneas during CSA-CSR were more severe than central apneas in terms of duration and desaturation. Finally, we wished to examine whether the increase in respiratory-control instability observed in the supine position is associated with an increase in mixed-apnea frequency, reflecting an increased contribution of upper-airway collapse to the development of ventilatory instability. METHODS Consecutive patients aged 18 to 80 years with stable congestive heart failure, as defined by a past episode of acute cardiogenic pulmonary edema, no hospital admission for more than 3 months, left ventricular ejection fraction less than 45%, and New York Heart Association class 2 or worse despite optimal medical management, who were referred to our institution’s heart failure program were assessed. Exclusion criteria included pregnancy and significant pulmonary, renal, or neurologic disease. All patients provided written informed consent, and data were collected prospectively. Twenty consecutive patients with continuous digital video surveillance during polysomnography with predominantly CSACSR and who spent at least 30 minutes sleeping in the supine and lateral positions were analyzed for the effects of position on CSACSR severity. Patients were not selected on the basis of positional SLEEP, Vol. 29, No. 8, 2006 1046 Influence of Position on CSA-CSR Severity—Szollosi et al AHI (events/h) Table 1—Subject Characteristics Age, y Sex Men Women CHF etiology IHD DCM HOCM ECG Rhythm SR AF Paced NYHA II III IV Echo FS, % LVEF, % BMI, kg/m2 ESS AHI, events/h Total Central Mixed Obstructive TST, h SpO2, % Mean Min PtcCO2, mm Hg Max Mean Min Sleep Stage (%TST) 1 2 SWS REM Position (%TST) Supine Left Right 70 59.9 (2.3) 60 18 2 * 50 * 40 13 6 1 30 10 5 5 0 # 20 10 1 2 SWS REM * p < .001, # p < .01 10 5 5 18.2 (2.1) 26.5 (2.2) 26.5 (0.8) 7.4 (0.8) Figure 2—Apnea-hypopnea index (AHI) by sleep stage and sleeping position inclusive of all central and mixed events. Right and left positions combined into a single lateral position. SWS refers to slow wave sleep; REM, rapid eye movement sleep. Note significant reduction in AHI with lateral compared to supine positon in all sleep stages. gen desaturation, mean minimum saturation, and mean baseline SpO2 were calculated (excluding obstructive events) for each subject in each combination of sleep stage and position. The baseline SpO2 was calculated as the sum of the minimum saturation and the desaturation associated with each respiratory event and, thus, reflects the oxygen saturation in each sleep stage and position, excluding the dips in saturation occurring with respiratory events. Mixed and central apnea contribution to the apnea index was examined in the supine and lateral positions with the left and right positions combined during non-rapid eye movement (NREM) sleep. Apnea index, mean duration, and mean desaturation associated with central and mixed apneas was calculated for each subject in the supine and lateral positions. Preliminary analysis revealed no differences between right and left positions for any of the outcome variables of interest, consistent with previous observations.17 As such, data from the right and left positions were combined into a single lateral position for analysis. AHI and ArI were not normally distributed; therefore, we used a negative binomial regression model to analyze the number of events per time in each sleep stage and body position. All other outcome variables for the group (i.e., mean event duration, desaturation, and minimum and baseline saturation) were normally distributed with equal variances across groups; therefore, we used linear regression to assess the influence of sleep stage and position. Similarly, the apnea index was analyzed using negative binomial regression to assess the influence of apnea type and position on the number of events per time; linear regression was used to assess influence of apnea type and position on mean duration and mean desaturation associated with events. All analyses were performed with robust standard errors adjusted for clustering by subject using Stata9 (StataCorp LP, College Station, TX). Data presented as mean ± SEM. 26.4 (3.0) 21.1 (2.7) 3.2 (1.6) 2.1 (0.4) 5.0 (0.3) 96.5 (0.3) 86.6 (1.3) 48.3 (1.4) 43.6 (1.5) 38.9 (1.6) 16.2 (1.9) 51.3 (1.8) 14.2 (1.7) 18.2 (1.9) 39.1 (5.0) 23.5 (5.2) 37.5 (6.7) Data presented as mean (SEM). CHF refers to congestive heart failure; ECG electrocardiogram; IHD ischemic heart disease; DCM, dilated cardiomyopathy; HOCM, hypertrophic obstructive cardiomyopathy; SR, sinus rhythm; AF, atrial fibrillation and flutter; NHYA, New York Heart Association classification; FS, fractional shortening measured by echocardiography; LVEF, left ventricular ejection fraction measured gated blood pool scan; BMI, body mass index; ESS, Epworth Sleepiness Scale score; AHI, apnea-hypopnea index; TST, total sleep time; SWS, slow-wave sleep; REM, rapid eye movement sleep). tive in nature. Arousals were scored according to American Sleep Disorders Association criteria.23 Sleep-stage, respiratory-event, and arousal information was exported for manual analysis. RESULTS The group of patients studied were typical of a heart failure population with a mean age of 59.9 ± 2.3 years, male predominance, sinus rhythm in approximately 50% and atrial fibrillation or pacemaker in approximately 50%, mean left ventricular ejection fraction (via 99Tc equilibrium radionuclide angiography) 26.5% ± Statistical Analyses To determine the influence of position on CSA-CSR severity, all obstructive events were removed from further analysis. AHI, Arousal Index (ArI), mean respiratory event duration, mean oxySLEEP, Vol. 29, No. 8, 2006 supine lateral * 1047 Influence of Position on CSA-CSR Severity—Szollosi et al �� DESATURATION % 1* 2* SWS .09]). The mean duration of events for all subjects was 26.2 ± 2.0 seconds (supine 25.7 ± 2.8 seconds and lateral 26.9 ± 3.4 seconds) and was not significantly influenced by either sleep stage or sleeping position. The desaturation and minimum saturation were significantly influenced by position in Stage 1 and Stage 2 sleep, during which 29% and 51% of events occurred, respectively (Figure 3). The lateral position was associated with decreased apnea-hypopnea– related hypoxemia during Stage 1 and Stage 2 sleep. The differences were not statistically significant in SWS and REM sleep, probably due to the relatively small numbers of events occurring in these sleep stages (20% of all events). There was no significant influence of sleep stage or position on baseline SpO2 (supine 96.8% ± 0.3% and lateral 97.4% ± 0.1 %). The supine position was associated with a significantly greater total apnea index compared with the lateral position (19.0 ± 4.9/ hour and 7.0 ± 2.9/hour; p < .001). This increase in the supine apnea index was driven by significant increases in both central and mixed events; however, the proportion of central versus mixed events remained similar in both positions (supine 71:29 and lateral 69:31, p = NS). During NREM sleep, mixed apneas were of longer duration than central apneas (29.1 ± 2.1 and 19.3 ± 1.1 seconds; p < .001) and resulted in greater desaturation (6.1% ± 0.5% and 4.5% ± 0.5%; p = .003) and lower minimum SpO2 (91.5% ± 0.6% and 92.9% ± 0.6%; p = .039). Similar to the apnea-hypopnea results, there was no influence of position on apnea duration; however, the supine position was associated with significantly greater desaturations independent of apnea type (supine 5.4% ± 0.5% and lateral 3.9% ± 0.4%, p = .003). REM 0 supine lateral 1 2 3 4 5 6 7 �� MINIMUM SpO2 % 98 96 94 92 90 88 86 84 1* 2* SWS REM * p < .001 Figure 3—Influence of body position on (a) oxygen desaturation and (b) minimum oxygen saturation associated with respiratory events. SWS refers to slow wave sleep; REM, rapid eye movement sleep. Note significantly greater desaturation and lower minimum SpO2 in the supine compared with lateral position in Stage 1 and Stage 2 sleep, where the majority of events occurred. 2.2%, and fractional shortening (via transthoracic echocardiography) 18.2% ± 2.1%. The overall AHI was 26.4 ± 3.0 events per hour; central, mixed and obstructive AHI were 21.1±2.7, 3.2±1.6, and 2.1±0.4 events per hour, respectively (Table 1). Six of 20 patients tolerated the esophageal pressure manometer. A total of 2326 central and mixed events during 5996 minutes of sleep were analyzed from polygraphs of 20 patients. Mean time spent sleeping supine was 118.7 ± 17.4 minutes, left lateral was 65.4 ± 17.3 minutes, and right lateral was 115.7 ± 21.6 minutes. The AHI was significantly influenced by both sleep stage and position (Figure 2). AHI showed a progressive decrease from Stage 1 to Stage 2 to slow-wave sleep (SWS) (all p < .005); respiratory events persisted during rapid eye movement (REM) sleep, with greater frequency than during SWS (p < .05) but with lower frequency than during Stage 1 sleep (p < .001). Position had a significant influence on AHI, independent of sleep-stage effects. The lateral position was associated with significant reduction in AHI compared with supine in all sleep stages (Stage 1, 54.7 ± 4.2 events per hour vs 27.2 ± 4.1 events per hour [p < .001]; Stage 2, 43.3 ± 6.1 events per hour vs 14.4 ± 3.6 events per hour [p < .001]; SWS, 15.9 ± 6.4 events per hour vs 5.4 ± 2.9 events per hour [p < .01]; REM, 38.0 ± 7.3 events per hour vs 11.0 ± 3.0 events per hour [p < .001]). Similarly, the ArI decreased from Stage 1 to Stage 2 and SWS with a small rise in REM; however, the decrease in ArI observed in the lateral position reached statistical significance only during Stage 2 sleep (Stage 1, 46.3 ± 4.9 events per hour vs 41.3 ± 5.7 events per hour [p = .55]; Stage 2, 28.2 ± 5.8 events per hour vs 12.6 ± 2.1 events per hour [p < .01]; SWS, 5.7 ± 2.5 events per hour vs 2.8 ± 0.7 events per hour [p = .24]; REM, 12.1 ± 3.4 events per hour vs 9.7 ± 2.5 events per hour [p = SLEEP, Vol. 29, No. 8, 2006 DISCUSSION There are 2 important novel observations that have emerged from this detailed study of CSA-CSR in patients with heart failure. First, compared with the supine position, the lateral position is associated with reduced apnea-hypopnea–related hypoxemia despite respiratory events of similar duration in addition to a more than 50% reduction in AHI. Second, mixed apneas were of longer duration and produced greater desaturation than central apneas; however, the ratio of mixed to central apneas was unchanged by the move from supine to lateral position (~30:70 ratio). These novel findings would suggest that the effect of posture on respiratory-control instability during sleep is more likely to be due to supine reductions in pulmonary oxygen stores rather than increases in upper-airway instability in this patient group. Our findings support 2 recently published articles in which the importance of sleeping posture in patients with heart failure was highlighted. We have confirmed the findings of Sahlin et al, who reported a higher central AHI in the supine compared with nonsupine position (41 and 26 events per hour) in a group of 20 patients.18 Similarly, Leung and coworkers reported a voluntary predisposition to sleep in the right lateral decubitus position compared to the left lateral decubitus position in 75 patients with heart failure. Of note, Leung reported the AHI and mean and minimum SpO2 values to be similar in the left and right lateral positions.17 As well as confirming these previous findings, the present study extends upon these previous observations. Importantly, we have shown that the severity of CSA-CSR, as assessed by the magni1048 Influence of Position on CSA-CSR Severity—Szollosi et al tude of hypoxemia but not of event duration, is also reduced in the lateral position. This observation offers valuable insights into the pathogenesis of CSA-CSR, namely that the supine increase in CSA-CSR occurs in the presence of reduced oxygen stores. The pathogenesis of CSA-CSR has been explained by instability in the metabolic control of ventilation. Recently, this hypothesis has also been applied to explain the pathogenesis of OSAHS, with some studies reporting that patients with OSAHS also have an underlying instability in ventilatory control.9,10 In terms of control theory, a negative feedback loop, such as the metabolic control of ventilation, will exhibit unstable behavior if the loop gain of the system exceeds 1. If the loop gain is less than 1, any disturbance causing changes in blood gases will be dampened out, and ventilation will return to a stable pattern. Simplistically, there are 3 factors that can contribute to increasing loop gain and the development of oscillatory behavior in ventilatory control, namely, increased circulation time, increased sensitivity of chemoreceptors (controller gain), and decreases in lung volume (plant gain).24,25 The limited evidence for each of these 3 factors is discussed in the context of transverse postural changes. Although this study was not designed to identify which of these mechanisms may be influenced by postural changes during sleep, our results provide indirect evidence that the increase in supine AHI in this patient group occurred in the presence of decreased oxygen stores/lung volumes, as reflected by the greater degree of hypoxemia occurring with events of similar duration in the supine position. The influence of transverse gravitational effects on hemodynamics in humans are few and, to date, have only been conducted during wakefulness. Pump et al reported that, in healthy subjects, the left lateral posture increases left atrial diameter, facilitates venous return, and decreases mean systemic arterial pressure; however, the right lateral posture was not examined.26 The importance of posture on sleep-disordered breathing is also highlighted by observations that both central and obstructive apneas are decreased during microgravity conditions.13 Postural hemodynamic changes during sleep may therefore be important in the setting of heart failure. Increased venous return in the lateral position may contribute to maintaining increased cardiac output, decreasing circulation time, and thus favoring ventilatory stability. Postural changes in lung volume in the transverse plane are also not well documented. In a study by Hurewitz et al, which assessed regional ventilation in obese and nonobese controls, the lateral decubitus position was associated with an increase in functional residual capacity of approximately 560 mL, compared with the supine position in the control subjects.27 However, the numbers were small (n = 3) and generalizations thus difficult to make. Patients with heart failure are known to have decreased lung volumes due to pulmonary congestion with or without enlargement of the heart within the thorax.28 Recently, it has also been observed that, during CSA-CSR, fluctuations in end-expiratory lung volume occur with changes in tidal volume.29 Decreases in lung volume, and therefore oxygen stores, favors the development of CSA-CSR as the ability of the lungs to buffer changes in blood gases is reduced, leading to an increase in plant gain. A small reduction of lung volume that may occur from the lateral to supine position may therefore be an important mechanism that would explain the supine increase in AHI that we and others have observed. Given that we found a greater degree of hypoxemia resulting from respiratory events in the supine position, without any differences in the duration of events, lung-volume changes are SLEEP, Vol. 29, No. 8, 2006 likely to be involved in explaining positional changes in ventilatory stability. Further indirect evidence to support the importance of lung-volume changes come from studies investigating the efficacy of continuous positive airway pressure (CPAP) and supplemental oxygen in the treatment of CSA-CSR secondary to heart failure. Application of CPAP has been equally effective in reducing AHI and ArI, as compared with the administration of supplemental oxygen.30,31 CPAP is known to increase lung volumes,32 and both forms of treatment acutely reduce hypoxemia through increasing total body oxygen stores,33 thus favoring the development of ventilatory stability. Furthermore, CPAP as well as supplemental oxygen have been shown to improve left ventricular ejection fraction after a 3-month treatment period.4,34 Thus, the importance of reductions in lung volume and its effect on reducing oxygen stores may be underestimated in the pathogenesis of CSA-CSR. At present, there have been no studies that have investigated the influence of transverse postural changes in chemoreceptor sensitivity; thus we cannot rule out this mechanism as playing a role in explaining the increase in AHI observed in the supine position. However, this is unlikely given that supine to upright changes in chemoreceptor sensitivity to CO2 have not been observed in normal subjects.35,36 Previous investigators have reported that upper-airway collapse is common during CSA-CSR19,20 and that the tendency for upper-airway collapse is enhanced in the supine position in patients with OSAHS.14 This observation, together with evidence that upper-airway collapse is common during CSA-CSR, may make it plausible that an obstructive component during CSACSR may be important in explaining the increased frequency of respiratory events in the supine position. It has also been reported that fluctuations in state changes, such as those that occur as a consequence of the arousal response, illicit changes in chemoreceptor sensitivity and that involvement of the peripheral chemoreceptors amplifies the state-related changes in ventilation.37 During sleep, chemoreceptor sensitivity is blunted to both hypoxic and hypercapnic stimuli.38,39 The arousal response or the wakefulness drive is thus associated with an increase in chemoreceptor sensitivity. It is possible that as the supine position favors upper-airway collapse, it would lead to longer apneas and a greater degree of oxygen desaturation. The resultant increase in hypoxic drive, together with an increased sensitivity of chemoreceptors associated with the arousal response, may be associated with an exaggerated ventilatory response and be an important mechanism that promotes respiratory instability. To address this question, we have examined the prevalence of upper-airway collapse that resulted in mixed apneas during CSACSR in both supine and lateral positions during NREM sleep. We have limited this part of the analysis to include only apneas because the subclassification of hypopneas into central and mixed is difficult, even with the presence of esophageal pressure measurement in a subgroup of our patients. Mixed apneas were found to be longer in duration and resulted in a greater degree of hypoxemia than did central apneas. For both duration and desaturation, this effect was independent of position; however, desaturation associated with mixed and central apneas was further increased in the supine position. Importantly, the proportion of central and mixed apneas was similar in both positions; therefore, we believe that mechanisms other than upper-airway collapse are responsible for the increased ventilatory instability that we have found in the 1049 Influence of Position on CSA-CSR Severity—Szollosi et al supine position. Our findings give indirect support that lung-volume reductions may be more important than previously thought in the pathophysiology of CSA-CSR. It is likely that changes in lung volume occur in association with postural changes in the transverse plane; however, we cannot rule out that changes in cardiac chamber dimensions, cardiac filling, cardiac output, or other hemodynamic variables affecting circulation time, as well as changes in chemoreceptor sensitivity, may also contribute to ventilatory instability in the supine position. It is also possible that active or passive collapse of the upper airway may be occurring during central apneas. In summary, this study has shown that the lateral position is associated with a greater than 50% reduction in the AHI and the apnea index independent of sleep-stage effects. These reductions are of similar magnitude to those observed with application of CPAP.4 Although event duration is not influenced by position, hypoxemia is attenuated in the lateral position, suggesting that postural changes in lung volume may be responsible for postural changes in ventilatory instability. Thus, changes in loop gain rather than upper-airway collapse are likely to cause the increase in AHI observed in the supine position in patients with heart failure and CSA-CSR. Because the prevalence of CSA-CSR is common in patients with heart failure, avoiding the supine position during sleep may be important in altering the expression of ventilatory instability in this patient group. This may have profound effects on sleep quality by promoting consolidation of sleep architecture and by reducing hypoxic damage, sympathetic nervous system activation, and consequent cardiovascular morbidity. However, further studies are required to identify precise mechanisms involved and whether a simple therapeutic intervention such as avoidance of the supine position during sleep can contribute to improvements in quality of life and survival. Finally, this study highlights that AHI during CSA-CSR, as in obstructive sleep apnea, is highly dependent on body position and sleep stage. The weak correlation between AHI and morbidity in many studies40 may in part be explained by the shifting expression of ventilatory instability caused by positional influences. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. REFERENCES 1. 2. 3. 4. 5. 6. 7. Javaheri S, Parker T, Liming J, et al. Sleep apnea in 81 ambulatory male patients with stable heart failure. Types and their prevalences, consequences, and presentations. Circulation 1998;97:2154-9. Churchill ED, Cope O. The rapid shallow breathing resulting from pulmonary congestion and edema. J Exp Med 1929;49:531-7. Mansfield D, Kaye DM, Brunner La Rocca H, Solin P, Esler MD, Naughton MT. Raised sympathetic nerve activity in heart failure and central sleep apnea is due to heart failure severity. Circulation 2003;107:1396-400. Naughton M, Benard D, Liu P, Rutherford R, Rankin F, Bradley T. Effects of nasal CPAP on sympathetic activity in patients with heart failure and central sleep apnea. Am J Respir Crit Care Med 1995;152:473-9. Naughton M, Benard D, Tam A, Rutherford R, Bradley TD. Role of hyperventilation in the pathogenesis of central sleep apneas in patients with congestive heart failure. Am Rev Respir Dis 1993;148:330-8. Solin P, Roebuck T, Johns DP, Haydn WE, Naughton MT. Peripheral and central ventilatory responses in central sleep apnea with and without congestive heart failure. Am J Respir Crit Care Med 2000;162:2194-200. Shahar E, Whitney CW, Redline S, et al. Sleep-disordered breathing SLEEP, Vol. 29, No. 8, 2006 22. 23. 24. 25. 26. 27. 28. 1050 and cardiovascular disease . cross-sectional results of the sleep heart health study. Am J Respir Crit Care Med 2001;163:19-25. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 1993;328:1230-5. Wellman A, Jordan AS, Malhotra A, et al. Ventilatory control and airway anatomy in obstructive sleep apnea. Am J Respir Crit Care Med 2004;170:1225-32. Hudgel DW, Gordon EA, Thanakitcharu S, Bruce EN. Instability of ventilatory control in patients with obstructive sleep apnea. Am J Respir Crit Care Med 1998;158:1142-9. Cartwright R. Effect of sleep position on sleep apnea severity. Sleep 1984;7:110-4. Oksenberg A, Khamaysi I, Silverberg DS, Tarasiuk A. Association of body position with severity of apneic events in patients with severe nonpositional obstructive sleep apnea. Chest 2000;118:101824. Elliott AR, Shea SA, Dijk D-J, et al. Microgravity reduces sleepdisordered breathing in humans. Am J Respir Crit Care Med. 2001;164:478-85. Penzel T, Moller M, Becker HF, Knaack L, Peter JH. Effect of sleep position and sleep stage on the collapsibility of the upper airways in patients with sleep apnea. Sleep 2001;24:90-5. Oksenberg A, Silverberg DS, Arons E, Radwan H. The sleep supine position has a major effect on optimal nasal continuous positive airway pressure: relationship with rapid eye movements and non-rapid eye movements sleep, body mass index, respiratory disturbance index, and age. Chest 1999;116:1000-6. Fujita M, Miyamoto S, Sekiguchi H, Eiho S, Sasayama S. Effects of posture on sympathetic nervous modulation in patients with chronic heart failure. Lancet 2000;356:1822-3. Leung RST, Bowman ME, Parker JD, Newton GE, Bradley TD. Avoidance of the left lateral decubitus position during sleep in patients with heart failure: relationship to cardiac size and function. J Am Coll Cardiol 2003;41:227-30. Sahlin C, Svanborg E, Stenlund H, Franklin KA. Cheyne-Stokes respiration and supine dependency. Eur Respir J 2005;25:829-33. Alex C, Onal E, Lopata M. Upper airway occlusion during sleep in patients with Cheyne-Stokes respiration. Am Rev Respir Dis 1986;133:42-5. Badr MS, Toiber F, Skatrud JB, Dempsey J. Pharyngeal narrowing/ occlusion during central sleep apnea. J Appl Physiol 1995;78:180615. Rechtschaffen A, Kales A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects. Washington: US Government Printing Office; 1968. Hirshkowitz M, Kryger M. Monitoring techniques for evaluating suspected sleep-disordered breathing. In: Kryger MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine, 4th ed. Philadelphia: Elsevier Saunders; 2005:1378-93. EEG arousals: scoring and examples. A preliminary report from the Sleep Disorders Atlas Task Force of the American Sleep Disorders Association. Sleep 1992;15:174-84. Khoo MC. Determinants of ventilatory instability and variability. Respir Physiol 2000;122:167-82. Khoo MC, Gottschalk A, Pack AI. Sleep-induced periodic breathing and apnea: a theoretical study. J Appl Physiol 1991;70:2014-24. Pump B, Talleruphuus U, Chouristensen NJ, Warberg J, Norsk P. Effects of supine, prone, and lateral positions on cardiovascular and renal variables in humans. Am J Physiol Regul Integr Comp Physiol 2002;283:R174-80. Hurewitz AN, Susskind H, Harold WH. Obesity alters regional ventilation in lateral decubitus position. J Appl Physiol 1985;59:77483. Yap JCH, Moore DM, Cleland JGF, Pride NB. Effect of supine posture on respiratory mechanics in chouronic left ventricular failure. Am J Respir Crit Care Med 2000;162:1285-91. Influence of Position on CSA-CSR Severity—Szollosi et al 29. Brack T, Jubran A, Laghi F, Tobin MJ. Fluctuations in end-expiratory lung volume during cheyne-stokes respiration. Am J Respir Crit Care Med 2005;171:1408-13. 30. Krachman SL, D’Alonzo GE, Berger TJ, Eisen HJ. Comparison of oxygen therapy with nasal continuous positive airway pressure on cheyne-stokes respiration during sleep in congestive heart failure. Chest 1999;116:1550-7. 31. Teschler H, Dohouring J, Wang Y, Berthon-Jones M. Adaptive pressure support servo-ventilation: a novel treatment for CheyneStokes respiration in heart failure. Am J Respir Crit Care Med 2001;164:614-9. 32. Alex CG, Aronson RM, Onal E, Lopata M. Effects of continuous positive airway pressure on upper airway and respiratory muscle activity. J Appl Physiol 1987;62:2026-30. 33. Krachman SL, Crocetti J, Berger TJ, Chatila W, Eisen HJ, D’Alonzo GE. Effects of nasal continuous positive airway pressure on oxygen body stores in patients with Cheyne-Stokes respiration and congestive heart failure. Chest 2003;123:59-66. 34. Sasayama S, Izumi T, Seino Y, Ueshima K, Asanoi H. Effects of nocturnal oxygen therapy on outcome measures in patients with chronic heart failure and Cheyne-Stokes respiration. Circ J 2006;70:1-7. 35. Xie A, Takasaki Y, Poppin J, Orr D, Bradley T. Influence of body position on pressure and airflow generation during hypoxia and hypercapnia in man. J Physiol 1993;465:477-87. 36. Weissman C, Abraham B, Askanazi J, Milic-Emili J, Hyman AI, Kinney JM. Effect of posture on the ventilatory response to co2. J Appl Physiol 1982;53:761-5. 37. Dunai J, Wilkinson M, Trinder J. Interaction of chemical and state effects on ventilation during sleep onset. J Appl Physiol 1996;81:2235-43. 38. Douglas N, White D, Weil J, et al. Hypoxic ventilatory response decreases during sleep in normal men. Am Rev Respir Dis 1982;125:286-9. 39. Douglas N, White D, Weil J, Pickett C, Zwillich C. Hypercapnic ventilatory response in sleeping adults. Am Rev Respir Dis 1982;126:758-62. 40. Solin P, Bergin P, Richardson M, Kaye DM, Walters EH, Naughton MT. Influence of pulmonary capillary wedge pressure on central apnea in heart failure. Circulation 1999;99:1574-79. SLEEP, Vol. 29, No. 8, 2006 1051 Influence of Position on CSA-CSR Severity—Szollosi et al