Renal response to graded intravenous pertonic NM3 infusion in
advertisement

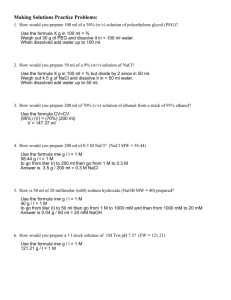
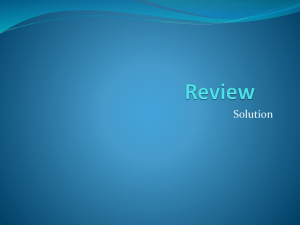
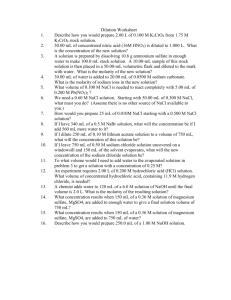
Renal response to graded intravenous pertonic NM3 infusion in pertensive subjects:dose-related impairment in distal FdaCl reabsorption” Janos I’. Radb, M.D. Eva Juhos, M.D. Ever-t J. Dorhout Mees, M.D. Budapest, Hungary, and Utrecht, The Netherlands Enhanced sodlium excretion after a salt load has been described as “‘exaggerated natriuresis” (EN) in patients with various forms of hypertension.‘-4 Its mechanisms and the renal site of impaired sodium reabsorption have been extensively investigated, but are increasingly controversial in the recent literature. A primary tubular defect or an abnormal response to volume expansion were considered as possibly responsible for the phenomenon9, Xl a.nd alpredominant role was claimed for both the proximal tubuleP and the distal nephron.s-l’ The abnormal renal handling of sodium previously was,thought to be characteristic to all patients with essential hypertension, but very recently it was postulated as a feature of renin suppression.12-‘4 Our preliminary studies suggested that depression of free water reabsorption (T&) was a more sensitive indicator of the altered renal response to acute NaCl loading than EN itself, becoming more pronounced with increasing the load. Furthermore, a similar tendency was found also in the healthy persons when very high NaCl loads were used. Therefore, the present work was designed to compare the renal responses of healthy subjects and “normal renin” essential From the Department ry, and the Department The Netherlands. Received for publication Accepted for publication Reprint Hospital, requests: Dr. XII. Diosarok *This study of Medicine, Jams Hospital, of Nephrology, University was supported 0002~8703/80/080183 Budapest, Hospital, HungaUtrecht, Oct. 30, 1978. March 26, 1979. JBnos P. Rad6, Dept. u. 1, H-1125 Budapest, by the Dutch + 08$00.80/00 Kidney 1980 of Medicine, Hungary. Janos V. Materials and Mosby Co. methods Participants. Studies were performed on 12 patients with uncomplicated essential hypertension (average age: 34.3 + 2.9 (SEM) years) and on 15 healthy volunteers (average age: 23.5 r?~1.9 years). In the Protocol I and II studies (seebelow) six male and two female healthy subjects and 10 male and two female hypertensive patients participated; Protocol III was performed on four male and threle female healthy persons. In the bypertensive groups the elevation of blood pressure was from mild to moderate and all patients were free from any demonstrable cardiovascular, renal, or endocrinologiical consequences of longstanding hypertension. Normal renal function was assessedb,y urine analysis, creatinine clearance, and DDAVl?* concentration test.15 Renovascular hypertension was ruled out by normal radiorenogram, intravenous pyelogram and in certain casesby renal arteriogram. secondary hypertension were excluded by appronriate tests including renal biopsy. Hypertensive ‘l-Desamino-8-D-Argtiinine Foundation. The C. hypertensive patients to graded acute intravenous hypertonic NaCl loading with special reference to changes in the normal relationship between solute excretion (“osmolal clearance,” Cosm) and Th+,. From such a comparison we expected to ex.clude an intrinsic tubular abnormality and to demonstrate that EN is an acute renal response ,abnormally reset to a lower level in the hypertensive patients. vasopressin. American Heart Journal 183 4.75 i- 1.6G 0.68 4.56 2.20 +- 4.78 i 0.3 6.29 2.12 k0 0.36 5.64 a.08 to 5.65 + o 0.73 '- 7.61 1.3'6 0.95 15.85 i 19.24 0.001 4.20 i 2.9c; ct.64 14.09iI.73 23.19i" 2.26 6.41 1.87 i 4.95 0.94 + 4.04 f m.79 -1- 34.48 1.64 1_O 2" 3.50 14.10 3.97 ta 2.57 k 20.76 3.03 0.05 0.001 k" 3.53 z" 5.10 0.52 1.91 x-3 6.98 1.13 i" 4.85 0.85 ?a 6.67 i-O 1.33 3.005 -t 0.54 4.14 7.26i 2.04 zk 3.97 3.64 +- 0.70 5.76 10.72 i 1.49 21.7Oi 1.36 4.51 Q.47 2.40 NS to 6.86 6.98t" 3.21 +' 31.03 +O 3.18 23.65 i 8.54 k0 2.18 1.44 1.59 29.07 _c' 4.00 29.08 3.48 0.01 0.01 0.001 6.38 III) in investigations the the Y!.hAarati.ion i~v~§tigati~~ and wtitten behe -e 9.06 1.13 + 14.01 1.13 to 5.57 0.98 to + o ka 2.62 0.01 Q.05 N, = healthy subjects (n = 4); M, = hypertensive patients (n = 9); ’ = not significant; p = p < 0.05 (hypertensive vs normal). “Moderate” NaCi load = intravenous infusion of 2.92% NaCl during 60 minutes. During NaCl loading = mean of periods 2 to 6. After loading = mean of periods 7 to 10. MaxirnaP change = mean of individual maximum (in a single period from 3 to 10) minus Data are presented as mean +- SEM. The 2.30 0.41 8.26-t' 1.39 ute ekarance k 0.80 5.68+ 2.99 -c 2.73 1.48 18.1Qc0 baseline. perio two 3G minute JBnos w of was fu consent the study. elsinki. The explained was obtained three membess nature to each during 60 minutes; an intravenous dose of 4 pg DDAVP was given at 9 A.m. in additiion to the two from them. All sf the hyper- l/T treatment was Ilo but during the whole experiment 500 mU. ilysine~as~~~~ss~~~ per hour were infused ~t~av~nO~$ly~ No baseline periods were run. One Biter 2.5% NaCl dukng the first two C1 was infused during the ether, 854 mEq. Na were our one 60 minute clear- venous catheter &ma1 y=.58x+.27 response to IV hypertonic NaCl ,H NaCl rz.99.. B T ?i20 mI/min A 5 10 15 ‘OS&W 20 25 mllmin under the influence of a “moderate” intravenous NaCl load in Fig. 1. Relationship between Cosm and Q, healthy (circles; N) and in hypertensive (black dots; El) subjects. A, All TH?, values obtained during and after intravenous NaCl loading were plotted against Cosm. B, Regression lines of data of baseline and NaCl studies. Note the significant difference between the slopes in the hypertensive group (solid line, baseline extrapolated) vs. no difference in the healthy group (dashed line). Asterisk = p -C 0.05. Urine and blood samples were analyzed for creatinine, sodium, Ipotassium (in all groups), calcium, magnesium, phlosphate (in all lbut group N,), and for uric acid (only in groups N, and N,) by procedures applied to the Technicon-Autoanalyzer. Chloride was measured by a chloridometer. All ion clearances were expressed as a percentage of GFR (creatinine clearance). When calculating Ca and Mg clearances, it was assumedlGthat 60% of the total plasma Ca concentration and 70% of the total Mg concentration underwent ultrafiltration in the glomerulus. Osmolality was determined by an Advanced Osmometer; Cosm and T~I,~ were calculated acciording to standard formulas. In order to save space in the Tables, contracted data of periods 1 and 2 (“baseline”) 3 to 6 (“during NaCl loading”) and 7 to 10 (“after loading”) are included. For unity, period 6 was included in the “during NaCl loading” contracted data of Protocols I and II/a, Correlation coefficients and regression lines were computed by the method of least squares. Statistical signifficance was deter- American Heart Journal mined by the paired t test except when digerent groups were compared; then the unpaired t test was used. Data are presented as mean t SEM. Results Baseline rehationship between CQSRP and TLp A “normal” relationship between Cosm and T&, was established during high NaCl intake by including all baseline values of the healthy subjects (groups N, and N,) and hypertensive patients (groups II, and II,). The relationship is expressed by the formula y = 0.58 X 40.27 (r = 0.99; p < 0.001) in the bealthy subjects and lby y = 0.63 x -0.03 (r = 0.99; p < 0.001) in the hypertensive patients. No statistical difference was found between the slopes (Fig. 1). Effect of a “‘moderate” i~~~ave~Q~s NaCB load on the baseline relationship between C2osm and -cl*0 Healthy subjects (group IV,). The time-course of changes in Cosm and ThTo can be seen in Fig. 2. 185 2. Time courseof changesin sarate exe te i&ravenous P&a loading iI? womar TfHzo after a high NaCl bad (h) apparently (m) iduced expected changes. n&m and free water reabsorption and in hypertensive patients. Note the ed to cianges in CQSsn an both gonps. ‘ hiuting and after decrease in )’ NaGI load Fig. 3. Relationship (group IV,; circles) between and “high” Cosm and ‘I& NaCl loading in healthy a significantly higher level in this group than an oup N,, but there was no significant difference Na, Ca, Mg, and P excretion between the groups (Table 1). ealthy subjects (group N,, Protocol II/a). The relationship during high NaCl loading is expressed by the formula y = 0.26 X + 1.09 (r = 0.56; p < O.OOl). The slope of this Iiine was ficantly different from that of moderate g (p < 0.05). The correlation between Cosm and Tg2, became much less close after a high NaCl load than after a moderate hoad (Figs. 2 and 3). There was a significant difference (p < 0.001) between the mean maximum and minimum TfHzovalues (6.74 t 0.48 ml./minute vs 1.42 + 0.61 ml./minute) obtained during high Na@l loading, but without a significant diBerence between the corresponding mean Cosm values (15.17 + 1.24 :ml./minute vs 11.92 ?I 1.57 ml./ mmute), suggesting that the rise of Cosm per se was not responsible for the dramatic decreas T& (Fig. 2). The risesin fractional Na, M, Ca, and Cl excretions were significantly higber after high NaCI loading than after moderate NaCl loading (Table II; Fig. 4), but there was no significant difference in P excretions. It is intering that fractional uric acid excretion slightly creased after moderate NaC!l loading, but significantly increased in response to a high NaC1 load. It should be noted that during administration of a relatively high dose of NaCI by slow intrave- American Heart Jownd subjects under the influence of “moderate” NaCl loading (group IV,; bhck stars). rims infusion (group N3, Protocol III), the correlation between changes of Cosm and TfIzO remained excellent, r G=0.99; Hypertensive patients (gro b). ‘The reliationship between Cosm and TfIzo (expressed by the formula y = 0.27 x +0.59) was less close after high loading (r = 0.49; p < 0.85) than after a moderate load in group p < 0.001). Thlere was a significant difference (p < O.OSl) between tke mean maximum and minimum TR+ values (5.87 -t 0.43 ml./minute vs 0.86 _t 0.59 ml.imi e), but no significant difference was found in corresponding mean Cosm values (Il.09 +: 1.42 d./minute QS 7.92 + 1.81 ml./minute). This study cleady shows that acute Na@l loading may depress Tg2, not only in hypertensive patientqg. lo but also in heakhy subj to 3). In earlier studies carried out in kealthy subjects, this has not be because during intravenous administration of hypertonic I?JaC% solutions there no evidence e increasing for an upper limit of T&l0Y as delivery from the proximal nephron enhanced out of the ascending hmb of owever, in the previous studies only moderate Na@l doses were use&l8 and the present results show that degression of TCHzO seeurred apparently as a dose-related consequence of acute NaCl ina kg. The a~~~~tat~o~ Qf ‘k,o at any rate of distal delivery of NaCI was significantly less during high NaCl loading than after moderate NaCl loadmg, suggestmg impaired 4. e course h TFi,a during and **p < 0.01; ***p < of changes in fraetionai excretion after “moderate” NaCl loading 0.005; ****p g, uric acid (TJ and phosphate (P) as well as and “higPa” Na@l load& (square). *p < Q.W5; of Na, K, Ca, (circles) < o.@m. NaCPreabsQr~tiQ~in striking finding wastlhe in the distal IllQUSNaCSloads. ur results are in agreement with those 0 u&es of t&de tive role in tlae6 tions7) an acceptable ““proximab marker 9719then of difference in phos crate and high NaCl jT rt the distal interpretation aiternative explanation f n of TfHzo wsuld be ins ~~ui~~~rat~o~ in the collecting tubules as a resu%t e osmotic diuresis or/an t. This, however, probab case because osmotic diuresis (Cosm) was not Renal higher when the lowest Tc,+, values were measured than in the presence of the maximal Tc,?, values, and special care was taken to provide the subjects with supramaximal amounts of DDAVP’” before and during the experiment. The persistence of the close correlation between Cosm and T&TOin group N, (given not lmuch less NaCl but in slow intravenous infusion) underlined the significance of the speed of a.cute loading in disruption of the normal relationship. Our study confirmed that impaired NaCl transport in Henle’s loop is a normal renal response to a certain degree of volume expansion.zo In hypertensive persons this response is found even after relatively small NaCl loadings which do not cause any distortion in the normal relationship between Cosm and Tc,?,, in the healthy subject. Therefore EN in the hypertensives seemsnot to be due to an intrinsic renal tubular defect but is probably the consequence o:f a basically normal renal response reset to a lower level. It was concluded that: (1) impaired distal NaCl reabsorption may also occur in response to acute NaCl loadings in the dehydrated healthy subject, and (2) EN is a.normal renal response abnormally reset to a l’ower level in the hypertensive patient. Heart Journal NaCl REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. American to IV hypertonic NaCl loadings in healthy subjects, and (2) “exaggerated natriuresis” is the consequence of a normal renal response (imparied NaCl transport in Henle’s loop) to a certain degree of volume expansion reset abnormally to a lower level in hypertensive paltients. Summary The effects of graded acute intravenous hypertonic NaCl loads on the baseline relationship between osmolal clearance and free water reabsorption established during high NaCl dietary intake and on the fractional excretion of various ions were investigated in 15 healthy subjects and in 12 “normal renin” essential hypertensive patients. No significant influence on the baseline relationship could be demonstrated after a moderate NaCl load in the healthy subjects, while free water reabsorption was depressed by the same intervention in the hypertensive patients. High NaCl loads induced depression of free water reabsorption in a dose-related fashion in both groups. No difference was foulnd in phosphaturia between the groups after the same NaCl load as well as in the healtlhy persons after different NaCl loads, supporting the contention that the observed differences in free water reabsorption were not due to changes in the proximal nephron. It was concluded that: (1) impaired NaCIL reabsorption in Henle’s loop (depression of free water reabsorption) may also occur in response to acute response 9. 10. 11. 12. 13. 14. Farnsworth, E. B.: Renal reabsorption of chloride and phosphate in normal subjects and in patients with essential hype:rtension, J. Clin. Invest. 25:897, 1946. Cottier, P. T., ‘Weller, J. M., and Hoobler, S. W.: Effect of an intravenous sodium chloride load on renal hemodynamics and elmectrolyte excretion in essential hypertension, Circulation 17:750, 1958. Rovner, D. R., Conn, J. W., Knopf, R. F., Cohen, E. L., and Hsucb, M.‘T.-Y.: Nature of renal escape from the sodium retaining effect of aldosterone in primary aldosteronism and normal subjects, J. Clin. Endocrinol. 25:53, 1965. Rado, J. P., Tako, J., and Szabo, T.: Salt loading in renal aldosteronism before and after nepbrectomy, Arch Surg. 98:357, 1969. Baldwin, D. S., Biggs, A. W., Goldring, W., Hulet, W. H., and Chasis, 1-I.: Exaggerated natriuresis in essential hypertension, Am. J. Med. 24:893, 1958. Dorhout Mees, E. J., and de Graaf, H.: Free water clearance in patients with essential hypertension, Clin. Sci. Mol. Med. 45:469, 1973. Chaimovitz, C., Spierer, A., Leibowitz, H., Tuma, S., and Better, 0. S.: Exaggerated phosphaturic response to volume expansion in patients -with essential hypertension, Clin. Sci. Mol. Med. 49207, 1975. Raeder, M., Qmvik, P., and Kiil, F.: Effect of acute hypertension on the natriuretic response to saline loading, Am. J. Pbysiol. 226:989, 1974. Buckalew, V. M., Puschett, J. B., Kintzel, J. E., and Goldberg, M.: Mechanism of exaggerated natriuresis in hypertensive :man: Impaired sodium transport in the loop of Henle, J. Clin. Invest. 48~1007, 1969. Rado, J. P., Szende, L., Borbely, L., Banos, Cs., Tako, J., and Fischer, Jr.: Different effects of frusemide administered during hypertonic saline infusion in healthy subjects and hypertensive patients, Clin. Sci. 39:833, 1970. Viskoper, R. J., Ben-Ishay, D., and Aviram, A.: Lack of exaggerated phosphaturia in essential hypertension, Nephron 13:390, 1974. Krakoff, L. R., Goodwin, F. J., Baer, L., Torres, M., and Laragh, J. H.: The role of renin in the exaggerated natriuresis in hypertension, Circulation 42:335, 1970. Schalekamp, IM. A. D. H., Krauss, X. H., SchalekampKuvken. M. P. A., Kolsters. .G.. and BirkenhPger. W. H.: S&dies bn the mkchanism’of hypernatriures; h essential hypertension in relation to measurements of plasma renin concentration, body fluid compartments ana renal function. Clin. Sci. 41:219, 1971. Luft, F. C., Grim, 6. E., V&Us, L. R., Higgins, J. T., and Weinberger, M. H.: Natriuretic response to saline infusion in normotensive and hypertensive man. The role of renin suppression in exaggerated natriuresis, Circulation 55:779, 15. 16. 1977. Rado, J. P.: l-Desamino-8-D-Arginine Vasopressin (DDAVP) cocentration test, Am. J. Med. Sci. 275:43. i978. Cannon, P. J., Svahn, D. S., and Demartini, F. E.: The influence of hypertonic saline infusions upon the frac- 189 17. 18. 19. tional reabsorption of usate and other ions in normal and hypertensive man, Circulation 419, 1970. Haber, E., Koemer, T., Page, L. Purnode, A.: Application of a ra angiotensiin itothephysiologic measurements ofplasma omal human subjects, 9. Clin, Endocrinol. Metab. Goldberg, M., McCnrdy, D. K., and Ramirez, M. A.: Differences behveem saline and mannittoi dime& in hydropenic man, 6. Clin. Invest. 44~182, 1965. Massey, S. G., Friedler, W. M7 and Coburn, 3. W.: Excretion of phosphate and caicium, Arch. Intern, Med. “?3 1:828, 1973. E A to: 20. Alexander, E. A., Doner, D. W., Add, R. B., and Levirisky, N. G.: Tubular reabsorption of sodimm during aacute and cbmnic v&me expansion ira man, J. Ch. 21. Danovitch, 6. M., and Bricker, N. S: Influence of volunze expansion on N&i reabsorption in the diluting segments of the nephron: A study us-kg clearance methods, Kidney ht. l&229, P976. hh-Shalom, N., Rapopert, J., Chaimovitz, c., ana Better, 0. S.: The effect of acute extraceU&r vchme expamion on sodium chloride seabsorption in the diluting segment in wan, Ch. Sci. Mol. Med. 54~333, 9978. 22.