Biphasic Alcohol Response Differs in Heavy Versus Light Drinkers
advertisement

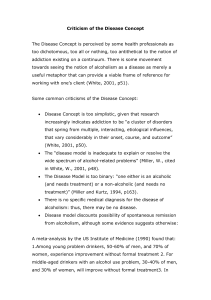
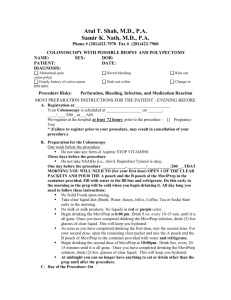
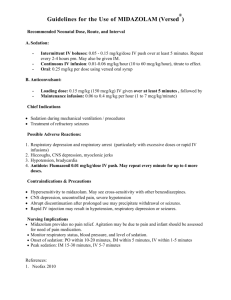
0145-6008/02/2606-0827$03.00/0 ALCOHOLISM: CLINICAL AND EXPERIMENTAL RESEARCH Vol. 26, No. 6 June 2002 Biphasic Alcohol Response Differs in Heavy Versus Light Drinkers Andrea C. King, Tim Houle, Harriet de Wit, Louis Holdstock, and Alyson Schuster Background: Most studies of risk factors for alcohol-related problems have focused on biological family history as a primary risk factor. However, other factors, such as early-age heavy drinking, are also risk factors for sustained or progressive heavy consumption. Little is currently known about the mechanisms underlying binge or heavy drinking. Methods: This study examined the acute subjective and objective effects of ethanol in heavy drinkers versus light drinkers. Thirty-four subjects participated in this within-subjects study consisting of three early-evening testing sessions in which subjects consumed a beverage containing either 0.8 or 0.4 g/kg ethanol or placebo. Results: Compared with lighter drinkers, heavy drinkers were more sensitive to the positive stimulantlike effects of ethanol (p ⬍ 0.05), especially during the increasing limb of the blood alcohol curve. Heavy drinkers also showed less sedation and cortisol response after alcohol than the light drinkers (p ⬍ 0.05). Conclusions: The results indicate that young adult binge drinkers show a biphasic alcohol response, with heightened sensitivity to stimulant-like alcohol effects and greater tolerance to sedative alcohol effects compared with their light-drinking counterparts. Key Words: Alcohol Response, Heavy Drinker, Risk for Alcoholism, Biphasic Alcohol Effects Scale, Cortisol. H EAVY ETHANOL DRINKING among young adults is a serious problem in this country (Chou and Pickering, 1992), and the consequences of this excessive use, both financial and personal, are widespread. The cost of ethanol-related health care, loss of productivity, crime, and accidents totals more than $148 million annually in the United States alone (Harwood et al., 1999). Approximately 30% of all accidents are connected to ethanol use, and excessive ethanol use contributes to many chronic and life-threatening illnesses, including gastrointestinal, liver, and cardiovascular disease (“Tenth Special Report to Congress on Alcohol and Health,” 2000). Data indicate that those who start drinking before the age of 14 years are 12 times more likely to be injured in accidents while under the influence of ethanol than those who start drinking after age 21 (Hingson et al., 2000). Early-onset alcohol drinking is also strongly associated with lifetime alcohol problems (Chou and Pickering, 1992). Understanding the factors that contribute to the escalation and maintenance of excessive ethanol drinking is crucial to improve prevention, public From The University of Chicago, Pritzker School of Medicine, Department of Psychiatry, Chicago, Illinois. Received for publication September 13, 2001; accepted March 27, 2002. Supported by the Alcoholic Beverage Medical Research Foundation (AK) and NIH/NIAAA Grants AA-11133 (AK) and M01-RR00055. Reprint requests: Andrea King, PhD, University of Chicago, Department of Psychiatry, 5841 S. Maryland Ave., Chicago, IL 60637; Fax: 773-702-6454; E-mail: aking@yoda.bsd.uchicago.edu Copyright © 2002 by the Research Society on Alcoholism. Alcohol Clin Exp Res, Vol 26, No 6, 2002: pp 827–835 education, and early intervention strategies. At this time, it is still unclear why some individuals abuse ethanol and others do not. One potential source of vulnerability to developing alcohol use problems is the quality and magnitude of acute subjective responses to alcohol (Fischman and Foltin, 1991). For instance, individuals who experience greater stimulant-like effects from an acute dose of ethanol also report greater drug liking and euphoria and have greater behavioral preference for ethanol (over placebo) compared with those individuals who experience mostly sedative-like effects (Chutuape and de Wit, 1994; de Wit et al., 1987, 1989; Duka et al., 1998). Whether these differences in the quality of the acute effects of alcohol also occur in individuals who are at risk for developing alcohol-related problems (e.g., because of their relatively high habitual consumption of alcohol is unclear). It is not known whether these patterns of subjective responses to alcohol predispose certain individuals to consume larger quantities of alcohol or, viewed another way, whether individuals who consume larger amounts of alcohol (i.e., heavy drinkers; HD) also exhibit this pattern of enhanced stimulant-like responses to alcohol. Heavy consumption of alcohol is in itself a potentially hazardous behavior, and it is also a risk factor for developing more serious alcohol-related problems, such as alcohol dependence. Aside from the differences in stimulant effects of alcohol, vulnerability to alcoholism has also been linked to other variations in acute responses to alcohol. Most of 827 828 these studies have been conducted by Schuckit and colleagues (Schuckit, 1984, 1985; Schuckit and Gold, 1988; Schuckit et al., 1987, 1996) and have examined persons at risk by virtue of a family history (FH) of alcoholism. Their results have indicated that sons of alcoholics have diminished subjective ratings of sedation, less body sway, and decreased cortisol responses to ethanol compared with sons of nonalcoholics. Thus, they proposed that diminished responses to acute alcohol administration are associated with risk for abuse. However, several other studies have failed to support this idea. In fact, other researchers (Conrod et al., 1997, 2001; Finn and Pihl, 1987; Finn et al., 1990; Gianoulakis et al., 1989, 1996; Peterson et al., 1996; Stewart et al., 1992) have reported that sons of alcoholics exhibit enhanced responses to ethanol, including greater stress response dampening, greater heart rate increases, and enhanced -endorphin–like responses after ethanol compared with sons of nonalcoholics. A differentiator model has been proposed to resolve these apparently discrepant data (Newlin and Thomson, 1990, 1999). This model posits that high-risk subjects (i.e., FH positive; FH⫹) experience greater stimulant-like effects from ethanol on the ascending limb of the blood alcohol curve [when blood alcohol concentrations (BACs) are increasing] and lower sedative-like effects on the descending limb (when BACs are decreasing). Thus, high-risk FH⫹ subjects would experience greater stimulant-like effects (which are typically reported to be positive) during increasing BACs and would experience fewer sedative and impairing effects (which are typically reported to be negative) during decreasing BACs. It remains to be seen whether this model can be extended to other at-risk populations, such as young HDs. Recently, we (Holdstock et al., 2000) reported findings that provided a potential extension of the differentiator model. We found that heavier social drinkers (range, 12–24 drinks weekly) reported greater stimulant-like subjective effects to ethanol than lighter drinkers (fewer than five drinks weekly). In addition, moderate/HDs tended to report fewer sedative-like and aversive effects from ethanol than light drinkers (LD). Thus, there may be both qualitative and quantitative differences between light and moderate/HDs in the nature of their subjective responses to ethanol, similar to other at-risk populations. These differences in subjective responses in our previous study occurred in the absence of differences in BACs, and they were specific; i.e., they were not associated with alterations in other subjective effects, adrenocortical hormone levels, or general psychomotor performance. However, the results were based on post hoc analyses of existing datasets with a relatively small number of subjects. The goal of this investigation was to extend the results of our previous study by using a more robust methodology, a larger sample size, and more carefully delineated groups of drinkers. We examined the subjective and objective (cortisol and heart rate response) effects of ethanol on the rising KING ET AL. and falling portions of the BAC curve in young adults with established HD patterns [a minimum of 10 drinks per week, with at least one weekly binge occasion of 5 or more drinks (4 drinks for women)] compared with LDs (1–5 drinks per week with no binge occasions). In line with the differentiator model, we hypothesized that HDs would exhibit greater stimulant-like effects on the ascending limb of the blood alcohol curve and reduced sedative-like effects on the descending limb of the curve. METHODS Subjects The subjects were 34 healthy male and female volunteers from the ages of 24 to 38 years recruited through newspaper advertisements, word-ofmouth referrals, and local flyers. They were initially screened by telephone to determine whether they met criteria for an LD or HD group. The criteria for the LD group (n ⫽ 14; 10 men and 4 women) was consumption of 5 or fewer drinks weekly (1–3 drinks per occasion, 1–2 times weekly) and never exceeding 5 drinks per occasion (4 for women). To qualify for the HD group (n ⫽ 20; 16 men and 4 women), respondents had to report habitual, regular consumption (i.e., predominant pattern since age 21 or at least the past 2 years) of a minimum of 10 drinks per week and consuming at least 5 drinks on 1 occasion, 1 to 4 times each week (4 drinks for women). Candidates who consumed an intermediate amount of alcohol or whose consumption varied considerably over time were not accepted. The drinking inclusion criteria for the HD group were based on laboratory, epidemiological, and clinical studies defining a binge as five or more drinks (four for women) consumed on one occasion. This level of drinking departs from normative social drinking, may indicate aspects of loss of control (Dawson, 2000; Dufour, 1999), and is frequently associated with adverse consequences (Dawson, 1999; Single, 1996). Eligible participants from the phone interview were invited to an in-person screening session that consisted of questionnaires, an interview by a trained master’s- or doctoral-level clinician, and a routine physical examination by a resident physician. The screening questionnaires consisted of the Symptom Checklist (Derogatis, 1983), a quantity-frequency index scale (Cahalan et al., 1969), the Brief Michigan Alcohol Screening Test (Pokorny et al., 1972), and a family tree for both primary and secondary biological relatives to assess two-generational FH for alcohol dependence (American Psychiatric Association, 1994). Exclusion criteria included a history of alcohol or substance dependence or regular heavy use of drugs other than alcohol, moderate or variable drinking patterns, psychiatric or medical disorders, clinically significant abnormalities on screening laboratory tests (aspartate aminotransferase, alanine aminotransferase, bilirubin, and so on), or a positive urine drug screen (amphetamines, barbiturates, opiates, or cocaine). Female candidates were tested for pregnancy before participating in the study and before each experimental session. The protocol was approved by the University of Chicago Institutional Review Board. Before participating in the study, subjects read and signed the consent form. The consent form stated that the purpose of the study was to assess mood responses to commonly used substances and that the category of substances may include a stimulant, sedative, alcohol, or a placebo. Each subject was instructed to abstain from any medication or substance use for 12 hr before and after sessions and to abstain from alcohol for 48 hr before participating. Also, the subject was instructed to refrain from eating for at least 2 hr before the session. At the end of each session, transportation was provided, and the subject was instructed not to drive or operate heavy machinery for at least 12 hr after the session. After completing the entire study, all subjects were debriefed and paid for their participation. 829 BIPHASIC ALCOHOL RESPONSE DIFFERS IN HEAVY/LIGHT DRINKERS Procedure The study used a within-subject design. Each subject participated individually in three experimental sessions in which he or she received either of two doses of ethanol (0.4 or 0.8 g/kg) or placebo administered in random order and counterbalanced within the group. The ethanol drinks consisted of 8% volume 180-proof alcohol (0.4 g/kg) and 16% volume alcohol (0.8 g/kg) mixed with water, Nutrasweet, and sugar-free grape Kool-Aid® (Kraft, Northfield, IL). The placebo beverage contained the mix with 1% ethanol as a taste mask to reduce expectancy effects. The study was conducted double-blind so that neither the subject nor the experimenter knew the contents of each beverage. Sessions were conducted in a comfortable living room–like laboratory environment, with at least 48 hr separating each session. During each session, the subject arrived at 4:30 PM, was given a light snack (noncaffeine, low-fat meal with 15% of calories from fat on the basis of body weight), and completed several demographic and personality questionnaires. At 5:15 PM, the subject submitted to a breathalyzer test, saliva sample, and cardiovascular recordings and also completed baseline questionnaires. Other noninvasive cognitive and performance testing was obtained at various intervals as part of another investigation. At 5:30 PM, the subject consumed the beverages in the presence of the experimenter. The beverage was divided equally into two portions, each consumed within a 5-min interval, with a 5-min rest in between (15 min total consumption interval). The experimenter was present during the entire beverage consumption and engaged in high conversation with the subject. After finishing the beverages, the subject was allowed to read or watch videotapes and completed subjective (questionnaires) and objective (cardiovascular, saliva cortisol, BAC) measures 15, 45, 105, and 165 min after the completion of drinking. In addition to the forms that subjects completed, the experimenter returned to the testing room frequently, to observe the activities of the subject and note any signs of intoxication. At the end of the session, around 9:00 PM, subjects were transported home. Dependent Measures—Subjective Biphasic Alcohol Effects Scale (BAES). The BAES (Martin et al., 1993) is a 14-item adjective-rating scale that is sensitive to ethanol-induced stimulant- and sedative-like effects. The BAES has been validated to yield higher stimulation scores during ascending BACs and higher sedation during descending BACs (Martin et al., 1993). The subject indicates the extent to which they are feeling each adjective on an 11-point scale from “not at all” (0) to “extremely” (10). The Stimulation scale is measured by summing the scores for the adjectives elated, energized, excited, stimulated, talkative, up, and vigorous. The Sedation scale score is measured by summing the descriptors down, heavy head, difficulty concentrating, inactive, sedated, slow thoughts, and sluggish. Addiction Research Center Inventory (ARCI). The ARCI (Martin et al., 1971) is a standardized questionnaire that consists of 49 true/false statements that are summed to five empirically derived scale scores. The ARCI is a sensitive, reliable measure of the effects of specific drugs or classes of drugs, including alcohol (e.g., Fischman and Foltin, 1991). The stimulantlike effects used from this scale were the Morphine-Benzedrine group (MBG), which reflects drug-induced euphoria, and the Amphetamine (A) scale, which provides a measure of stimulation. Sedative-like effects were derived from the Pentobarbital-Chlorpromazine-Alcohol Group (PCAG) scale. Drug Effects Questionnaire (DEQ). The DEQ consists of four visual analog scales for which subjects make a vertical mark on a 100-mm line for each item. The scale measures positive drug effects in items such as: (a) Like: “Do you like the effects you are feeling now?” [labeled dislike (0), neutral (50), and like extremely (100)]; and (b) Want More: “Would you like more of what you consumed, right now?” [labeled not at all (0), some (50), and a lot (100)]. The DEQ Scale also measures general drug effects in items such as (c) Feel: “Do you feel any drug effects?” and (d) High: “Do you feel high?” [both items labeled not at all (0) and a lot (100)]. In past studies, “high” has been shown to relate to some drug effects, although not associated with stimulant like or alcohol effects (Martin et al., 1993). Dependent Measures—Objective BAC. Instrumentation for estimating BACs from breath samples included the Alco-Sensor IV™ (Intoximeters Inc., St. Louis, MO). This breathalyzer read 0.000 for all measures during testing, with actual levels downloaded to a computer after the subject completed the study, thereby ensuring that the experimenter was blinded to alcohol dose condition. Heart Rate. An automated monitor (Laptron®, Kappa Medical Incorporated, Hauppauge, NY) measured heart rate (in beats per minute) at each time point and was recorded by the research assistant. Cortisol. Saliva samples were collected with plain cotton Salivettes™ (Sarstedt, Newton, NC) and stored in a ⫺20°C freezer until assayed by enzyme immunoassay (catalog No. 0101™, Salimetrics, State College, PA). Samples were thawed, centrifuged, and assayed in duplicate. The assay method was standardized and validated in the University of Chicago Clinical Research Center core laboratory. Data Analysis Because this study was primarily concerned with the differential stimulant and sedative effects of alcohol, the main dependent variables were the Stimulation and Sedation scales on the BAES. These data were analyzed by 2 ⫻ 3 ⫻ 5 repeated-measures analyses of variance (ANOVAs), with group (HD and LD) as a between-subjects factor and dose (placebo, 0.4 g/kg, and 0.8 g/kg) and time (baseline and 15, 45, 105, and 165 min) as within-subjects factors. To further examine the subjective stimulant- and sedative-like effects of alcohol, subscales from the ARCI and DEQ, as well as the objective measures of salivary cortisol and heart rate, were also analyzed in repeated-measures ANOVAs. Because of the rising and falling nature of BAC in an acute administration paradigm, it was expected that subjective effects might also vary in accordance with these levels. Therefore, a priori analyses examined the groups on curvilinear functions of different degrees (linear, quadratic, cubic, etc.) that represent an increase, peak, and decrease for the main dependent variables (BAES Stimulation and Sedation). These preliminary examinations with polynomial functions represent unique information compared with that of the traditional ANOVA and should not be interpreted as indicating a significant interaction unless otherwise stated. For all analyses, F values were considered significant at p ⬍ 0.05. To protect against violations of sphericity, Greenhouse-Geisser corrections were used to adjust the degrees of freedom of the F tests. Finally, in accordance with the suggestions made by Schmidt (1996), estimates of effect size will also be reported (2) as warranted. RESULTS Background Characteristics Table 1 displays the general demographic and alcoholdrinking characteristics for the HD and LD groups. The groups were similar on most background characteristics, except that LDs had more years of education than HDs (17.2 vs. 15.2 years). By definition, the HDs consumed more alcoholic drinks per typical drinking occasion, had more drinking occasions per week, had a greater frequency of binge drinking [i.e., five or more drinks per occasion (four for females)] over the last 6 months, and had a greater lifetime prevalence of Alcohol Abuse (58 vs. 0% in LDs). Ten subjects in the HD group reported smoking cigarettes daily, although 60% of these reported smoking 10 or fewer cigarettes per day. In contrast, only one of the LDs reported current smoking. There were no significant 830 KING ET AL. Table 1. Sample/Drinking Characteristics by Group Variable Demographics Age (years) Education (years) Race (black/white) Sex (M/F) Liver function Bilirubin (total) Alkaline phosphate SGOT SGPT Drinking behaviora Drinks/occasion Occasions/week 5⫹ drink occasions (last 6 months) Family historyb ⫹ Alcohol Abuse (lifetime, DSM-IV) Smoking behavior % Current smokerc Cigarettes/day Light drinkers Heavy drinkers 28.7 (0.72) 17.2 (0.56)* 5/8 10/4 28.5 (0.82) 15.2 (0.34) 5/15 16/4 .72 (0.10) 61.2 (4.08) 28.2 (2.59) 24.9 (2.9) .72 (0.06) 70.0 (4.15) 24.1 (0.92) 24.8 (2.19) 1.9 (0.21)* 1.2 (0.14)* .54 (0.22)* 31% 0%* 7%* .07 (0.27)* 4.8 (0.43) 3.4 (0.18) 45 (6.1) 50% 58% 50% 4.6 (6.72) Data presented are mean (SEM) or % where indicated. SGOT, serum glutamic oxaloacetic transaminase; SGPT, alanine transaminase. a Drinking behavior derived from 6-month quality-frequency index. b FH⫹, one or both parents or three or more secondary relatives with alcohol abuse or dependence. c Current smoker, reporting smoking one or more cigarettes weekly. * p ⬍ 0.05. differences in subjective responses to alcohol between the HD smokers and nonsmokers during the sessions (smoking was not permitted during the sessions). Demographic and alcohol consumption data were nearly identical for the HD smokers and nonsmokers, except for a greater frequency of binge occasions in the last six months in the former versus the latter group (mean, 63 vs. 35 occasions, respectively; p ⬍ 0.01). BACs As expected, BAC levels significantly increased over time and as a function of increasing alcohol dose [dose, F(2,58); and time, F(4,116) ⬎ 296.66, p ⬍ 0.0001; dose ⫻ time, F(8,232) ⫽ 158.45, p ⬍ 0.0001; see Fig. 1]. The LD and HD groups exhibited nearly identical BAC curves (F ⬍ 1.02; ps ⫽ ns). Alcohol Effects Alcohol increased BAES Stimulation scores during the initial rising BACs and increased Sedation scores over declining BACs [dose ⫻ time, Fs (8,248) ⱖ 2.29; ps ⬍0.05]. During the rising BAC, alcohol also increased other stimulant-like and general drug effects derived from the ARCI and DEQ scales (ARCI: A, MBG; DEQ: Like, Feel, and High scales; dose ⫻ time, ps ⬍0.05) and increased the DEQ rating of Want More [dose, F(1,30) ⫽ 4.67; p ⬍ 0.05]. Additionally, alcohol produced increases in other sedativelike effects during declining BACs, such as the ARCIPCAG scale (dose ⫻ time, p ⬍ 0.0001). For the objective measures, alcohol increased heart rate on both the rising and declining limbs of the BAC curve [dose, F(2,58) ⫽ 5.14, p ⬍ 0.01]. After covarying for baseline differences in cortisol between sessions, alcohol tended to increase cortisol levels, although this was nonsignificant [dose ⫻ time, F(6,174) ⫽ 1.92; p ⫽ 0.08]. Post hoc comparisons for most of these dependent variables indicated that the effects of ethanol were mainly apparent at the high dose compared with placebo (ps ⬍ 0.05, simple effects), whereas the low dose produced minimal or subtle mood changes. Therefore, the ensuing results on alcohol response refer primarily to the effects of the high alcohol dose, with the low dose producing a minimal or intermediate response, unless otherwise indicated. Group Comparisons on Alcohol-Related Effects Alcohol increased BAES Stimulation scores in the HD group but not in the LD group [group ⫻ dose, F(2,62) ⫽ 3.13; p ⫽ 0.05]. A priori analyses examining effects over the course of the BAC curve showed that alcohol produced a rapid, short-lived increase in Stimulation, with a slowing rate of decline [dose (linear) ⫻ time (cubic): F(1,18) ⫽ Fig. 1. Comparison of blood alcohol curve estimates from breathalyzer tests in the HD and LD groups for placebo, 0.4 g/kg (low dose), and 0.8 g/kg (high dose). One HD subject was removed from analyses as an outlier. The x axis time points indicate the following: base, measurement taken immediately before beverage consumption; and time points, time after the beverages were consumed. Dose ⫻ time interaction, p ⬍ 0.0001. 䡲, High dose; Œ, Low dose, 䡩, Placebo. BIPHASIC ALCOHOL RESPONSE DIFFERS IN HEAVY/LIGHT DRINKERS 831 Fig. 2. Mean stimulation subscale scores from the BAES for the HD and LD groups. Data correspond to the time points before beverage consumption (base) and after the beverages were consumed. For the HD group, data fit a curvilinear function (dose ⫻ cubic time, p ⫽ 0.001). 䡲, High dose; Œ, Low dose, 䡩, Placebo. 16.52, p ⫽ 0.001; 2 ⫽ 0.48; see Fig. 2]. Inspection of the means indicated that alcohol increased Stimulation in HDs at the 15 min postconsumption time point. In comparison, after drinking the placebo beverage, the HD group exhibited decreased Stimulation during this acute, rising BAC time point (p ⬍ 0.05). In the LD group, neither alcohol nor placebo beverage produced significant changes in selfreported Stimulation [F(1,13) ⫽ 0.41; p ⫽ not significant]. Alcohol also produced similar sharp and rapid increases in the HDs, but not LDs, on the other measures of stimulant-like effects during rising BACs, including the ARCI A and MBG scales [dose (linear) ⫻ time (cubic): F(1,19) ⱖ 13.94, p ⱕ0.001; 2 ⱖ 0.42]. Enhanced alcohol sensitivity on the DEQ Like scale [group ⫻ dose, F(1,30) ⫽ 6.14; p ⬍ 0.05] was also apparent in the HDs, as was a trend for increased ratings during rising BACs of DEQ Want More (group ⫻ dose, p ⫽ 0.07). Alcohol increased ratings (above neutral) for Like and Want more at rising BACs in 90 and 56% of HDs, respectively, compared with only 38 and 31% of LDs, and the relationship between these two Fig. 3. Mean sedation subscale scores from the BAES for the HD and LD groups. Data correspond to the time points before beverage consumption (base) and after the beverages were consumed. For both groups, data fit a curvilinear function (dose ⫻ cubic time, p ⬍ 0.05). 䡲, High dose; Œ, Low dose, 䡩, Placebo. psychological constructs was significant [r(31) ⫽ ⫹0.64; p ⬍ 0.001]. In contrast, on the more general scales of drug effects, including the DEQ Feel Drug and High, alcohol produced greater rising-BAC increases in LDs compared with HDs, and this augmented response was apparent even at the lower alcohol dose (group ⫻ dose ⫻ time, ps ⱕ0.01). Alcohol increased BAES Sedation scores to a greater extent in the LD group than the HD group [group ⫻ dose, F(2,62) ⫽ 5.33, p ⬍ 0.01; 2 ⫽ 0.15]. This was supported in our a priori examination of dynamic effects over time for the groups [group ⫻ dose (linear) ⫻ time (cubic), F(1,31) ⫽ 5.67, p ⫽ 0.024; 2 ⫽ 0.16]. For the LDs, increases in Sedation emerged during the early portion of the BAC curve and were sustained throughout testing [dose (linear) ⫻ time (cubic), F(1,13) ⫽ 4.79, p ⬍ 0.05; see Fig. 3]. However, in the HD group, alcohol increased Sedation ratings, but this was primarily during declining BACs [dose (linear) ⫻ time (cubic), F(1,18) ⫽ 5.13; p ⬍ 0.05]. Similarly, alcohol increased ratings on the other measure of sedativelike effects, the ARCI-PCAG scale, to a greater extent in 832 KING ET AL. Fig. 4. Mean saliva cortisol response for the HD and LD groups. Data correspond to the time points before beverage consumption (base) and after the beverages were consumed. 䡲, High dose; Œ, Low dose, 䡩, Placebo. the LD group and did so earlier in the BAC curve than in the HD group [group, p ⬍ 0.05; dose, p ⬍ 0.001; dose (linear) ⫻ time (quadratic), F(8,248) ⫽ 7.34, p ⬍ 0.001]. Alcohol increased cortisol levels in the LD group, but not in the HD group [group ⫻ dose, F(2,58) ⫽ 3.78; p ⬍ 0.05]. This cortisol increase in LDs occurred during the later portions of the BAC curve [i.e., 165 min; p ⬍ 0.05, simple effects; see Fig. 4], following the time course for LD/HD differences in Sedative-like responses. Finally, the HD group exhibited a significantly higher heart rate than the LDs at baseline and throughout the study, regardless of whether they received alcohol or placebo [group, F(1,29) ⫽ 4.41; p ⬍ 0.05], but the groups did not differ in their heart rate increases to alcohol (ANCOVA: group ⫻ time, group ⫻ dose, ps ⫽ not significant). Relationships Between Main Measures Although the BAES and ARCI scales were developed by using different methodologies and subject populations (normal drinkers and experienced addicts, respectively), there were significant correlations between these measures: BAES Stimulation was positively associated with the ARCI A and MBG scales during rising BACs [r(33) ⬎ 0.42; ps ⬍0.05], with ARCI A and MBG scales highly associated with each other [r(33) ⬎ 0.71; ps ⬍0.001]. Results for the BAES Sedation scale were positively associated with the ARCI PCAG scale during declining BACs [r(33) ⬎ 0.55; ps ⬍0.001]. Sedation, but not Stimulation, was also correlated with the cortisol response to alcohol [r(31) ⫽ 0.37; p ⬍ 0.05]. Examination of FH Effects Although this study was not designed to specifically address the effects of subjects’ differential FH of alcoholism, information about FH was obtained during screening as part of an attempt to equate groups on this variable. Chisquare analysis revealed that the HD and LD groups did not differ in incidence of FH⫹, defined as having at least one parent or three or more secondary relatives with alcoholism (50 vs. 31%; Table 1). Furthermore, for the main variables of interest—the BAES Stimulation and Sedation scales, as well as the objective measures of cortisol and heart rate—FH as a covariate did not alter the significant effects of drinking group. The only exception noted was a trend for the subgroup of HDs with FH⫹ to show the most blunted cortisol response to alcohol (FH ⫻ group ⫻ dose ⫻ time, p ⫽ 0.08). DISCUSSION In this study, we observed that HDs, compared with LDs, were more sensitive to the positive or euphorigenic subjective effects of alcohol during the early portion of the BAC and less sensitive to the sedative-like effects of alcohol during both rising and declining BACs. These results were obtained on a range of measures, including both alcoholspecific scales (BAES Stimulation and Sedation) and stimulant- and sedative-like drug effect scales (ARCI and DEQ). The HD subjects, compared with LD subjects, also had lower salivary cortisol levels during declining BACs. Although some studies have reported greater alcoholinduced heart rate changes in subjects at risk for alcoholism (Conrod et al., 1997, 2001; Peterson et al., 1996) and a positive relationship between heart rate increase and selfreported stimulation during rising BACs (Conrod et al., 2001), we did not observe differential effects of alcohol on heart rate changes between the HD and LD groups. This discrepancy between our study and other studies may be due to differences in the risk groups examined (FH⫹ versus HD) and in frequency of measurement and other instrumentation factors. BIPHASIC ALCOHOL RESPONSE DIFFERS IN HEAVY/LIGHT DRINKERS The collective pattern of response to alcohol observed on a variety of dimensions in this study provides partial support for the differentiator model (Newlin and Thomson, 1990, 1999). Newlin and Thomson proposed in their model that individuals with an FH of alcoholism would experience more stimulant effects on the ascending limb and less sedation on the descending limb of the BAC. Our study extends these findings to another at-risk group, i.e., young people who habitually engage in heavy social drinking beyond the college years. The most striking subjective differences between our groups occurred during the rising portion of the BAC (Figs. 2 and 3). During the ascending limb of the BAC, the HDs showed greater subjective stimulation and less sedation than LDs, but the differentiator model proposes that the sedation effect would occur only during declining BACs. Thus, this initial pattern after consumption of a moderate-to-high dose of alcohol, if supported in future studies or in other risk groups, may support an alternative “rising limb theory” that may be more applicable than the differentiator model to account for enhanced risk for the development and maintenance of alcohol use disorders. One important question that arises is whether the heightened alcohol stimulation and reduced sedation in HDs represent an acquired response to alcohol, evident only after multiple repeated exposures, or an inherent predisposition, or premorbid individual difference. In terms of the latter, because the data are cross-sectional in nature, we can only speculate that HDs might have been more likely to have early initial alcohol sensitivity to stimulation, tolerance to sedation, or both, even during their first exposure. This initial pattern of positive reinforcement without concomitant negative effects could be an important factor rendering them at risk for the acquisition of binge-drinking patterns. Unfortunately, due to ethical constraints in testing this model in human subjects, such as performing alcohol challenge studies on children or adolescents, and methodological difficulties, such as examining retrospective reports of initial exposures in adults (Schuckit et al., 2001), the premorbid sensitivity hypothesis will remain speculative. With respect to the former hypothesis (acquired alcohol response), it is possible that after repeated exposures, HDs become sensitized to the euphoric effects (or liking) of alcohol and then are more likely to continue to engage in HD. Alternatively, a recent incentive-sensitization theory postulates that the repeated use of addictive substances, including alcohol, sensitizes brain systems that mediate incentive motivation or reward (or wanting), resulting in further use (Robinson and Berridge, 1993, 2001). Because our results showed that HDs exhibited heightened alcohol liking and wanting, especially during the rising limb, and that these two factors were positively correlated with each other, these effects do not seem to be dissociated in this sample. Finally, it is possible that acquired tolerance to the sedative-like effects of alcohol, especially during rising BACs, may be the key component that contributes to in- 833 creased heavy drinking levels (Kalant, 1998; Schuckit, 1994). Schuckit and colleagues have shown that low level of alcohol response, as measured by subjective (mainly sedative-like) and physiologic measures, was evident in people with an FH of alcoholism and also predicted future drinking (Schuckit, 1994). However, as Conrod et al. (2001) point out, this theory is somewhat inconsistent with most current theories of the mechanisms of motivational states and drug-seeking behavior (i.e., addictive or rewarding properties). Several neurobiological systems may be involved in the stimulant effects of alcohol, including dopaminergic, opioidergic, and serotonergic neurotransmitter systems. The mesolimbic dopamine system, through pathways connected to the nucleus accumbens, has been postulated as the final common pathway for all drugs of abuse, including alcohol (Leshner, 1997; Wise and Bozarth, 1987). Two recent findings provide some support for dopamine involvement. First, acute administration of the dopamine antagonist haloperidol blocks alcohol craving in alcoholic subjects (Modell et al., 1993), and second, in healthy volunteers, haloperidol treatment reduced alcohol-related increases in BAES Stimulation (Enggasser and de Wit, 2001). Evidence for the involvement of the endogenous opioid system in alcohol euphoria comes from the finding that naltrexone, an opioid antagonist, reduces ethanol intoxication in social drinkers (Davidson et al., 1996; Swift et al., 1994), especially those with an FH of alcoholism (King et al., 1997). Finally, there is also limited evidence that serotonin is involved in alcohol reward (Meert et al., 1991; Myers et al., 1992), but these findings are mixed in human clinical trials (Johnson et al., 1996, 2000). Future investigations examining acute alcohol response paradigms with pharmacological manipulations or brain imaging techniques may help elucidate the mechanisms and role of several potential neurobiological systems in alcohol sensitivity and tolerance. There are two other important findings in this study that are worth discussion. First, the HD subjects demonstrated a rapid decrease in subjective stimulation in the HDs during the placebo beverage session, in contrast to their rapid increases in stimulation after consuming alcohol (Fig. 2). This differential effect may represent an opponent process (Siegel, 1983) or an antagonistic placebo response (Newlin, 1985), such that the high-risk HD, when exposed to alcohol-related cues (i.e., the placebo contained 1% alcohol as a taste mask), exhibits conditioned responses in the direction opposite to the drug effect. Paradigms involving more extensive, repetitive doses of alcohol or alcoholrelated cues may help elucidate the role of this differential placebo response to the etiology of alcohol-related disorders—a link that has yet to be established (Newlin, 1985). Second, the LDs’ absence of alcohol stimulation, in combination with increased sedation and stress hormone levels after alcohol consumption, may be an important factor rendering them at very low risk for the development of future alcohol disorders. Understanding the mechanisms 834 KING ET AL. underlying LDs’ alcohol response, a group putatively at low risk for harmful drinking, may provide clues as to the protective factors associated with LD, beyond racial or ethnic characteristics. The majority of research on people at low risk for future alcoholism has largely been confined to studies of individuals with unusual genetic variants (Agarwal et al., 1981; Wall et al., 1992; Yoshida et al., 1991). This study had several limitations. First, our sample size was modest; therefore, analyses on the basis of sex or individual difference factors could not be fully assessed. For example, we were unable to compare men and women. Although the prevalence of heavy alcohol use is higher in men, there has been a steady increase in binge drinking in young women (Dawson, 1996; Johnston et al., 2000), and the factors controlling drinking in women may be different than in men (King et al., 2002). Second, although the groups were similar on most demographic variables measured, the HDs had fewer years of education and higher smoking rates than LDs. Although these factors were not significant covariates in our analyses, it remains to be determined whether they are a factor in terms of etiology and/or maintenance of binge drinking. Third, the data do not provide longitudinal information, and therefore any conclusions remain speculative until prospective or largescale studies are conducted. In summary, although early onset of drinking (Chou and Pickering, 1992) and engagement in HD both strongly predict progression to future alcohol misuse, the factors or mechanisms underlying earlier-stage HD are not well understood. This study demonstrates biphasic alcohol responses, including rising BAC–associated increases in stimulation and declining BAC increases in sedation, in young HD/binge drinkers compared with light social drinkers. In contrast, LDs did not show biphasic alcohol response, with no increases in stimulation, and heightened sedation throughout both limbs and cortisol increases during the declining limb. The collective pattern of results may highlight the potential relative importance of changes during the ascending limb of the BAC in risk for alcohol use disorders. Finally, continued examination of factors involved in various risk groups beyond FH of alcoholism is warranted given the multiple etiologies for the complex disorders of alcohol abuse and dependence. Acute subjective and objective responses to alcohol remain an important potential determinant along with the myriad of environmental, psychological, and genetic influences on the degree of risk for alcohol-related problems. ACKNOWLEDGMENTS We appreciate the support of The University of Chicago Clinical Research Center (CRC). In particular, we thank Sujata Patel, Core Lab Director, for the cortisol assays; Veronica Wald, CRC administrative director, for oversight and organizational support; and the entire CRC nursing and dietary staff for their assistance. Paul Meyer was also helpful in the early data-collection phase of this study. Finally, we thank Emil Coccaro, MD, for helpful suggestions on this manuscript. REFERENCES Agarwal DP, Harada S, Goedde HW (1981) Racial differences in biological sensitivity to ethanol: the role of alcohol dehydrogenase and aldehyde dehydrogenase isozymes. Alcohol Clin Exp Res 5:12–16. American Psychiatric Association (1994) Diagnostic and Statistical Manual of Mental Disorders. 4th ed. American Psychiatric Press, Washington, DC. Cahalan V, Cisin I, Crossley HM (1969) American Drinking Practices. Rutgers Center for Alcohol Studies, New Brunswick, NJ. Chou SP, Pickering RP (1992) Early onset of drinking as a risk factor for lifetime alcohol-related problems. Br J Addict 87:1199 –1204. Chutuape MA, de Wit H (1994) Relationship between subjective effects and drug preferences: ethanol and diazepam. Drug Alcohol Depend 34:243–251. Conrod PJ, Peterson JB, Pihl RO (2001) Reliability and validity of alcohol-induced heart rate increase as a measure of sensitivity to the stimulant properties of alcohol. Psychopharmacology 157:20 –30. Conrod PJ, Peterson JB, Pihl RO, Mankowski S (1997) Biphasic effects of alcohol on heart rate are influenced by alcoholic family history and rate of alcohol ingestion. Alcohol Clin Exp Res 21:140 –149. Davidson D, Swift R, Fitz E (1996) Naltrexone increases the latency to drink alcohol in social drinkers. Alcohol Clin Exp Res 20:732–739. Dawson D (1996) Gender differences in the risk of alcohol dependence: United States, 1992. Addiction 91:1831–1842. Dawson D (1999) Alternative definitions of high risk for impaired driving: the overlap of high volume, frequent heavy drinking and alcohol dependence. Drug Alcohol Depend 54:219 –228. Dawson D (2000) Drinking patterns among individuals with and without DSM-IV alcohol use disorders. J Stud Alcohol 61:111–120. Derogatis L (1983) SCL-90-R Manual—II. Clinical Psychometric Research, Towson, MD. de Wit H, Pierri J, Johanson CE (1989) Assessing pentobarbital preference in normal volunteers using a cumulative dosing procedure. Psychopharmacology 99:416 – 421. de Wit H, Uhlenhuth EH, Pierri J, Johanson CE (1987) Individual differences in behavioral and subjective responses to alcohol. Alcohol Clin Exp Res 11:52–59. Dufour MC (1999) What is moderate drinking? Defining “drinks” and drinking levels. Alcohol Res Health 23:1–14. Duka T, Stephens DN, Russell C, Tasker R (1998) Discriminative stimulus properties of low doses of ethanol in humans. Psychopharmacology 136:379 –389. Enggasser J, de Wit H (2001) Haloperidol reduces stimulant and reinforcing effects of ethanol in social drinkers. Alcohol Clin Exp Res 25:1448 –1456. Finn PR, Pihl RO (1987) Men at risk for alcoholism: the effect of alcohol on cardiovascular response to unavoidable shock. J Abnorm Psychol 96:230 –236. Finn PR, Zeitouni NC, Pihl RO (1990) Effects of alcohol on psychophysiological hyperreactivity to nonaversive and aversive stimuli in men at high risk for alcoholism. J Abnorm Psychol 99:79 – 85. Fischman MW, Foltin RW (1991) Utility of subjective-effects measurements in assessing abuse liability of drugs in humans. Br J Addict 86:1563–1570. Gianoulakis C, Beliveau D, Angelogianni P, Meaney M, Thavundayil J, Tawar V, Dumas M (1989) Different pituitary -endorphin and adrenal cortisol response to ethanol in individuals with high and low risk for future development of alcoholism. Life Sci 45:1097–1109. Gianoulakis C, Krishnan B, Thavundayil J (1996) Enhanced sensitivity of pituitary -endorphin to ethanol in subjects at high risk of alcoholism. Arch Gen Psychiatry 53:250 –257. BIPHASIC ALCOHOL RESPONSE DIFFERS IN HEAVY/LIGHT DRINKERS Harwood HJ, Fountain D, Fountain G (1999) Economic cost of alcohol and drug abuse in the United States, 1992: a report. Addiction 94:631– 635. Hingson RW, Heeren T, Jamanka A, Howland J (2000) Age of drinking onset and unintentional injury involvement after drinking. JAMA 284: 1527–1533. Holdstock L, King AC, de Wit H (2000) Subjective and objective responses to ethanol in moderate/heavy and light social drinkers. Alcohol Clin Exp Res 24:789 –794. Johnson BA, Jasinski DR, Galloway GP, Kranzler H, Weinreib R, Anton RF, Mason BJ, Bohn MJ, Pettinati HM, Rawson R, Clyde C (1996) Ritanserin in the treatment of alcohol dependence—a multi-center clinical trial. Psychopharmacology 128:206 –215. Johnson BA, Roache JD, Javors MA, DiClemente CC, Cloninger CR, Prihoda TJ, Bordnick PS, Ait-Daoud N, Hensler J (2000) Ondansetron for reduction of drinking among biologically predisposed alcoholic patients. A randomized controlled trial. JAMA 284:963–971. Johnston LD, O’Malley PM, Bachman JG (2000) Monitoring the Future National Survey Results on Drug Use, 1975–1999. Volume 2: College Students and Young Adults (NIH Publication No. 00-4803). National Institute on Drug Abuse, Bethesda, MD. Kalant H (1998) Research on tolerance: what can we learn from history? Alcohol Clin Exp Res 22:67–76. King AC, Bernardy NC, Hauner K (2002) Stressful events, personality, and mood disturbance: gender differences in alcoholics and problem drinkers. Addict Behav, in press. King AC, Volpicelli JR, Frazer A, O’Brien CP (1997) Effect of naltrexone on subjective alcohol response in subjects at high and low risk for future alcohol dependence. Psychopharmacology 129:15–22. Leshner AI (1997) Addiction is a brain disease, and it matters. Science 278:45– 47. Martin CS, Earleywine M, Musty RE, Perrine MW, Swift RM (1993) Development and validation of the Biphasic Alcohol Effects Scale. Alcohol Clin Exp Res 17:140 –146. Martin WR, Sloan JW, Sapira JD, Jasinski DR (1971) Physiologic, subjective and behavioral effects of amphetamine, methamphetamine, ephedrine, phenmetrazine and methylphenidate in man. Clin Pharmacol Ther 12:245–258. Meert TF, Awouters F, Niemegeers CJ, Schellekens KH, Janssen PA (1991) Ritanserin reduces abuse of alcohol, cocaine, and fentanyl in rats. Pharmacopsychiatry 24:159 –163. Modell JG, Mountz JM, Glaser FB, Lee JY (1993) Effect of haloperidol on measures of craving and impaired control in alcoholic subjects. Alcohol Clin Exp Res 17:234 –240. Myers RD, Lankford M, Björk A (1992) Selective reduction by the 5-HT antagonist amperozide of alcohol preference induced in rats by systemic cyanamide. Pharmacol Biochem Behav 43:661– 667. Newlin DB (1985) Offspring of alcoholics have enhanced antagonistic placebo response. J Stud Alcohol 46:490 – 494. Newlin DB, Thomson JB (1990) Alcohol challenge with sons of alcoholics: a critical review and analysis. Psychol Bull 108:383– 402. Newlin DB, Thomson JB (1999) Chronic tolerance and sensitization to alcohol in sons of alcoholics: II. Replication and reanalysis. Exp Clin Psychopharmacol 7:234 –243. 835 Peterson JB, Pihl RO, Gianoulakis C, Conrod P, Finn PR, Stewart SH, LeMarquand DG, Bruce KR (1996) Ethanol-induced change in cardiac and endogenous opiate function and risk for alcoholism. Alcohol Clin Exp Res 20:1542–1552. Pokorny AD, Miller BA, Kaplan HB (1972) The brief MAST: a shortened version of the Michigan Alcoholism Screening Test. Am J Psychiatry 129:342–345. Robinson TE, Berridge KC (1993) The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Res Brain Res Rev 18:247–291. Robinson TE, Berridge KC (2001) Incentive-sensitization and addiction. Addiction 96:103–114. Schmidt FL (1996) Statistical significance testing and cumulative knowledge in psychology implications for training of researchers. Psychol Meth 1:115–129. Schuckit MA (1984) Subjective responses to alcohol in sons of alcoholics and control subjects. Arch Gen Psychiatry 41:879 – 884. Schuckit MA (1985) Ethanol-induced changes in body sway in men at high alcoholism risk. Arch Gen Psychiatry 42:375–379. Schuckit MA (1994) Low level of response to alcohol as a predictor of future alcoholism. Am J Psychiatry 151:184 –189. Schuckit MA, Edenberg HJ, Kalmijn J, Flury L, Smith TL, Reich T, Bierut L, Goate A, Foroud T (2001) A genome-wide search for genes that relate to a low level of response to alcohol. Alcohol Clin Exp Res 25:323–329. Schuckit MA, Gold E, Risch C (1987) Plasma cortisol levels following ethanol in sons of alcoholics and controls. Arch Gen Psychiatry 44:942– 945. Schuckit MA, Gold EO (1988) A simultaneous evaluation of multiple markers of ethanol/placebo challenges in sons of alcoholics and controls. Arch Gen Psychiatry 45:211–216. Schuckit MA, Tsuang JW, Anthenelli RM, Tipp JE, Nurnberger JI (1996) Alcohol challenges in young men from alcoholic pedigrees and control families: a report from the COGA project. J Stud Alcohol 57:368 –377. Siegel S (1983) Classical conditioning, drug tolerance, and drug dependence, in Research Advances in Alcohol and Drug Problems (Smart RG, Glaser FB, Isreal Y, Kalant H, Popham RE, Schmidt W eds), vol 7, pp 207–246. Plenum Press, New York. Single E (1996) Harm reduction as an alcohol-prevention strategy. Alcohol Health Res World 20:239 –243. Stewart SH, Finn PR, Pihl RO (1992) The effects of alcohol on the cardiovascular stress response in men at high risk for alcoholism: a dose response study. J Stud Alcohol 53:499 –506. Swift RM, Whelihan W, Kuznetsov O, Buongiorno G, Hsuing H (1994) Naltrexone-induced alterations in human ethanol intoxication. Am J Psychiatry 151:1463–1467. Tenth Special Report to Congress on Alcohol and Health (2000) National Institute on Alcohol Abuse and Alcoholism, Bethesda, MD. Wall TL, Thomasson HR, Schuckit MA, Ehlers CL (1992) Subjective feelings of alcohol intoxication in Asians with genetic variations of ALDH2 alleles. Alcohol Clin Exp Res 16:991–995. Wise RA, Bozarth MA (1987) A psychomotor stimulant theory of addiction. Psychol Rev 94:469 – 492. Yoshida A, Hsu LC, Yasunami M (1991) Genetics of human alcoholmetabolizing enzymes. Prog Nucleic Acid Res Mol Biol 40:225–287.