to view one of our SAMPLE MULTI
advertisement

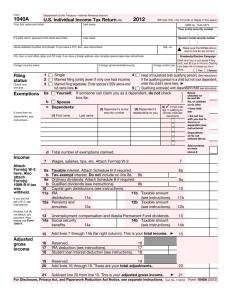
EXAMPLE OF MULTI-STATE INCOME TAX RETURN
JUSTIN and JUSTINE CASE
ONE MILITARY W-2 IN –JUSTIN $40,000 income
ONE CIVILIAN W-2 CA –JUSTINE $20,000 income
MARRIED FILING JOINTLY
STATIONED IN CA
NO DEPENDENTS
This is a military tax return with income from two different states. Active military
Husband Justin has $40,000 of income and paid $2,000 in state taxes to his home state
of Indiana. Spouse, Justine has $20,000 of income and paid $1,000 in state taxes to her
home state of California.
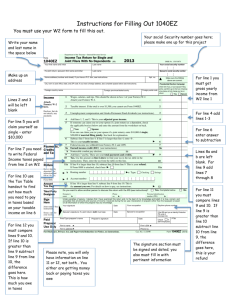
This is a line by line example of what an incorrect and correctly prepared military tax
return looks like. The incorrectly prepared tax return shows a state refund of $28.00 in
Indiana and they owe $28.00 in California. The correctly prepared state tax return
shows a state refund of $855.00 in Indiana and $1,000.00 in California. There is a total
difference of $1,855.00 between the correct and incorrect state tax returns.
The reason this happens is that tax software atomically imports the combined income
into both states. It is then up to the tax preparer to know how to do this on a state by
state basis. Also based on years of experience the best way to do this depends on the
individual state. Some states are relatively straight forward about how to do this and
other states are rather complex.
The main strategy to properly preparing a multi-state military tax return is it must be
prepared in a step by step fashion. Step one is to determine if there is any special tax
treatment for active military income in this particular state. Step two is to isolate active
duty military income from spouse’s income or any other non-military civilian income.
Step three would be to isolate spouse’s civilian or military income to the appropriate
state. In addition to the steps some states may require the return to be filed as “married
and separate” or to prepare two separate returns in order to maximize tax advantages
and amount of tax return.
DIRECTIONS: Please refer to the page number of the PDF document in the table below
and then look at the corresponding form number. Then look at the line or box number to
see how much income is being used to calculate the state tax. You can then refer to the
refund column to see the difference.
NOTE: Any incorrectly prepared military state tax return over the past three years can
be amended in order to receive the proper amount.
Page#
3
5
5
5
5
6
6
6
6
7
7
8
10
10
10
11
12
12
13
14
14
14
14
16
Form#
Line# Box# State Income Taxes Refund
Federal 1040
7
60,000
W-2
1
IN
40,000
W-2
15
IN
W-2
16
IN
40,000
W-2
17
IN
2,000
W-2
1
CA
20,000
W-2
15
CA
W-2
16
CA
20,000
W-2
17
CA
1,000
IT-40
1
IN
60,000
IT-40
7
IN
58,000
IT-40
22
IN
28
CA RES. INC. 540
12
CA
60,000
CA RES. INC. 540
13
CA
60,000
CA RES. INC. 540
19
CA
52,318
CA RES. INC. 540
111
CA
-28
* IT-40 PNR
1
IN
40,000
* IT-40 PNR
7
IN
33,666
* IT-40 PNR
22
IN
855
* CA NON-RES 540NR
12
CA
20,000
* CA NON-RES 540NR
13
CA
60,000
* CA NON-RES 540NR
14
CA
40,000
* CA NON-RES 540NR
17
CA
20,000
* CA NON-RES 540NR 125
CA
1,000
* CORRECTLY PREPARED STATE TAX RETURN
Form
Department of the Treasury - Internal Revenue Service
1040
(99)
U.S. Individual Income Tax Return
2012
For the year Jan. 1-Dec. 31, 2012, or other tax year beginning
OMB No. 1545-0074 IRS Use Only - Do not write or staple in this space.
, 2012, ending
Your first name and initial
See separate instructions.
, 20
Last name
JUSTIN
Your social security number
CASE
If a joint return, spouse's first name and initial
131-65-2217
Last name
JUSTINE
Spouse's social security number
CASE
212-54-1187
Home address (number and street). If you have a P.O. box, see instructions.
Apt. no.
Make sure the SSN(s) above
and on line 6c are correct.
123 MAIN ST
City, town or post office, state, and ZIP code. If you have a foreign address, also complete spaces below (see instructions).
Presidential Election Campaign
SAN DIEGO, CA 92101
Foreign country name
Foreign province/county
Foreign postal code
Check here if you, or your spouse if filing
jointly, want $3 to go to this fund. Checking
a box below will not change your tax or
refund.
You
Filing Status
1
2
Check only one
box.
3
Exemptions
6a
4
Single
X
the qualifying person is a child but not your dependent, enter this
Married filing jointly (even if only one had income)
Married filing separately. Enter spouse's SSN above
and full name here.
b
X
X
c
Dependents:
child's name here.
5
Qualifying widow(er) with dependent child
Yourself. If someone can claim you as a dependent, do not check box 6a . . . . . . . .
Spouse . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
(1) First name
(2) Dependent's
social security number
(3) Dependent's
relationship to you
Last name
}
(4) X if child
under age 17
qualifying for
child tax credit
(see instr.)
If more than four
dependents, see
instructions and
check here
Attach Form(s)
W-2 here. Also
attach Forms
W-2G and
1099-R if tax
was withheld.
If you did not
get a W-2,
see instructions.
Enclose, but do
not attach, any
payment. Also,
please use
Form 1040-V.
Adjusted
Gross
Income
7
8a
b
9a
b
Total number of exemptions claimed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Wages, salaries, tips, etc. Attach Form(s) W-2 . . . . . . . . . . . . . . . . . . . . . . .
7
Taxable interest. Attach Schedule B if required . . . . . . . . . . . . . . . . . . . . . .
8a
Tax-exempt interest. Do not include on line 8a . . . . . . .
Qualified dividends . . . . . . . . . . . . . . . . . . . . .
2
0
0
0
Add numbers on
lines above
2
60,000.
8b
Ordinary dividends. Attach Schedule B if required . . . . . . . . . . . . . . . . . . . . . .
9a
9b
10
Taxable refunds, credits, or offsets of state and local income taxes . . . . . . . . . . . . . .
10
11
Alimony received . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11
12
Business income or (loss). Attach Schedule C or C-EZ . . . . . . . . . . . . . . . . . . .
12
13
Capital gain or (loss). Attach Schedule D if required. If not required, check here . . . .
13
14
Other gains or (losses). Attach Form 4797 . . . . . . . . . . . . . . . . . . . . . . . . .
15a
IRA distributions . . . . .
15a
b Taxable amount . . . . . . .
15b
16a
Pensions and annuities . .
16a
b Taxable amount . . . . . . .
16b
17
Rental real estate, royalties, partnerships, S corporations, trusts, etc. Attach Schedule E . . .
17
18
Farm income or (loss). Attach Schedule F . . . . . . . . . . . . . . . . . . . . . . . . .
18
19
Unemployment compensation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
20a
Social security benefits . .
21
Other income. List type and amount
21
22
Combine the amounts in the far right column for lines 7 through 21. This is your total income
22
60,000.
23
Educator expenses . . . . . . . . . . . . . . . . . . . . .
24
Certain business expenses of reservists, performing artists, and
0.
60,000.
b Taxable amount . . . . . . .
20a
14
19
20b
23
fee-basis government officials. Attach Form 2106 or 2106-EZ .
24
25
Health savings account deduction. Attach Form 8889 . . . . .
25
26
Moving expenses. Attach Form 3903
. . . . . . . . . . . .
26
27
Deductible part of self-employment tax. Attach Schedule SE . .
27
28
Self-employed SEP, SIMPLE, and qualified plans . . . . . . .
28
29
Self-employed health insurance deduction . . . . . . . . . .
29
30
Penalty on early withdrawal of savings . . . . . . . . . . . .
30
31a
Alimony paid
31a
32
IRA deduction . . . . . . . . . . . . . . . . . . . . . . .
33
Student loan interest deduction . . . . . . . . . . . . . . .
33
34
Tuition and fees. Attach Form 8917 . . . . . . . . . . . . .
34
35
Domestic production activities deduction. Attach Form 8903 . .
35
36
Add lines 23 through 35 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
36
37
Subtract line 36 from line 22. This is your adjusted gross income . . . . . . . . . . .
37
b Recipient's SSN
For Disclosure, Privacy Act, and Paperwork Reduction Act Notice, see separate instructions.
UYA
Boxes checked
on 6a and 6b
No. of children
on 6c who:
lived with you
did not live with
you due to divorce
or separation
(see instructions)
Dependents on 6c
not entered above
d
Income
Spouse
Head of household (with qualifying person). (See instructions.) If
32
Form
1040 (2012)
Form 1040 (2012)
Tax and
Credits
JUSTIN
38
39a
b
Standard
Deduction
forPeople who
check any
box on line
39a or 39b or
who can be
claimed as a
dependent,
see
instructions.
All others:
Single or
Married filing
separately,
$5,950
Married filing
jointly or
Qualifying
widow(er),
$11,900
Head of
household,
$8,700
40
41
42
43
44
45
46
47
48
42
Alternative minimum tax (see instructions). Attach Form 6251 . . . . . . . . . . . . . . . . .
Add lines 44 and 45 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Foreign tax credit. Attach Form 1116 if required . . . . . . . . . . 47
Credit for child and dependent care expenses. Attach Form 2441 . . 48
45
51
56
46
5,209.
54
0.
5,209.
49
55
56
8919 . . . . . . 57
Additional tax on IRAs, other qualified retirement plans, etc. Attach Form 5329 if required . . . . . 58
Household employment taxes from Schedule H . . . . . . . . . . . . . . . . . . . . . . . . . 59a
First-time homebuyer credit repayment. Attach Form 5405 if required . . . . . . . . . . . . . . . 59b
Unreported social security and Medicare tax from Form:
57
58
44
50
53
Add lines 47 through 53. These are your total credits . . . . . . . . . . . . . . . . . . . . .
Subtract line 54 from line 46. If line 54 is more than line 46, enter -0- . . . . . . . . . . . . .
Self-employment tax. Attach Schedule SE . . . . . . . . . . . . . . . . . . . . . . . . . . . .
54
a
4137
b
60
Other taxes. Enter code(s) from instructions
61
61
Add lines 55 through 60. This is your total tax . . . . . . . . . . . . . . . . . . . . . . .
Federal income tax withheld from Forms W-2 and 1099 . . . . . . 62
6,000.
63
2012 estimated tax payments and amount applied from 2011 return
Earned income credit (EIC) . . . . . . . . . . . . . NO
. . . . . . 64a
62
64a
b Nontaxable combat pay election. .
65
60
65
68
70
Amount paid with request for extension to file . . . . . . . . . . .
Excess social security and tier 1 RRTA tax withheld . . . . . . . .
Credit for federal tax on fuels. Attach Form 4136 . . . . . . . . . .
71
Credits from Form: a
71
72
Add lines 62, 63, 64a, and 65 through 71. These are your total payments . . . . . . . . . .
If line 72 is more than line 61, subtract line 61 from line 72. This is the amount you overpaid . . . .
Amount of line 73 you want refunded to you. If Form 8888 is attached, check here . . . .
68
69
73
74a
2439 b
Reserved c
8801 d
8885
b
Routing number
d
Account number
Amount of line 73 you want applied to your 2013 estimated tax
75
76
77
5,209.
64b
Additional child tax credit. Attach Schedule 8812 . . . . . . . . . .
American opportunity credit from Form 8863, line 8 . . . . . . . .
Reserved . . . . . . . . . . . . . . . . . . . . . . . . . . . .
67
Amount
You Owe
41
43
52
11,900.
48,100.
7,600.
40,500.
5,209.
40
Taxable income. Subtract line 42 from line 41. If line 42 is more than line 41, enter -0- . . . . . .
Tax (see instructions). Check if any from: a
Form(s) 8814 b
Form 4972 c
962 election
Residential energy credits. Attach Form 5695 . . . . . . . . . . .
c
Other credits from Form: a
3800
b
8801
66
Direct deposit?
See
instructions.
39b
Itemized deductions (from Schedule A) or your standard deduction (see left margin) . . . . . .
Subtract line 40 from line 38 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Exemptions. Multiply $3,800 by the number on line 6d . . . . . . . . . . . . . . . . . . . . .
Child tax credit. Attach Schedule 8812, if required . . . . . . . . .
63
Refund
If your spouse itemizes on a separate return or you were a dual-status alien, check here
51
53
131-65-2217 Page 2
. . 38
60,000.
}
52
b
If you have a
qualifying
child, attach
Schedule EIC.
{
Education credits from Form 8863, line 19 . . . . . . . . . . . . .
Retirement savings contributions credit. Attach Form 8880 . . . . .
49
59a
Payments
Amount from line 37 (adjusted gross income) . . . . . . . . . . . . . . . . . . . . . . . .
Check
You were born before January 2, 1948,
Blind.
Total boxes
if:
Spouse was born before January 2, 1948,
Blind.
checked
39a 0
50
55
Other
Taxes
and JUSTINE CASE
c Type:
66
67
69
70
Checking
73
74a
6,000.
791.
791.
76
0.
72
Savings
75
Amount you owe. Subtract line 72 from line 61. For details on how to pay, see instructions
Estimated tax penalty (see instructions) . . . . . . . . . . . . .
77
Third Party
Designee
Do you want to allow another person to discuss this return with the IRS (see instructions)?
Sign
Here
Under penalties of perjury, I declare that I have examined this return and accompanying schedules and statements, and to the best of my knowledge and belief,
they are true, correct, and complete. Declaration of preparer (other than taxpayer) is based on all information of which preparer has any knowledge.
Joint return?
See instr.
Keep a copy
for your
records.
Your signature
Paid
Preparer
Use Only
Designee's
name
Date
Yes. Complete below.
Spouse's signature. If a joint return, both must sign.
Date
Daytime phone number
Your occupation
(619)555-1212
Spouse's occupation
OFFICE MGR.
Print/Type preparer's name
Firm's name
Preparer's signature
No
Personal identification
number (PIN)
USMC
Firm's address
UYA
Phone
no.
Date
Check
if
self-employed
If the IRS sent you an Identity Protection
PIN, enter it
here (see inst.)
PTIN
Firm's EIN
Phone no.
Form
1040
(2012)
This W-2 belongs to:
X JUSTIN
a Employ ee's social security
JUSTINE
OMB No.
1545-0008
X Standard W-2 (Ty ped or computer generated)
Non-Standard W-2 (Altered or hand written)
131-65-2217
Form W-2c, Corrected Wage and Tax Statement
b Employ er identif ication
1 Wages, tips, other comp 2 Federal inc tax withheld
53-9990000
40,000.00
3 Social security wages
c Employ er's name
4,000.00
4 Social Sec tax withheld
0.00
DFAS
5 Medicare wages and tips
Employ er's address
0.00
1240 East Ninth Street
State
Employ er's
Cleveland
OH
0.00
6 Medicare tax withheld
Zip Code
44199
Employ er's f oreign country
7 Social security tips
0.00
8 Allocated tips
0.00
0.00
9
10 Dependent care benef its
11 Nonqualif ied plans
12 Code
0.00
Foreign prov ince/county
0.00
Foreign postal code
13 Statutory employ ee
e Employ ee's f irst
JUSTIN
Employ ee's last
Suf f .
D
700.00
Q
5,000.00
Retirement plan
0.00
Third-party sick pay
0.00
CASE
f
0.00
Employ ee's address
123 MAIN ST
State
Employ ee's
SAN DIEGO
CA
Zip Code
92101
Employ ee's f oreign country
Foreign prov ince/county
15 State State ID
IN
80501907
Amount
0.00
14 See
se
ction d
e xpande
below.
0.00
0.00
Foreign postal code
16 State wages
17 State inc tax
18 Local wages
19 Local W/H
40,000.00
2,000.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
W-2 Wage and Tax
2012
20 Local name
Department of the Treasury Internal Rev enue
State me nt
Othe r Ite ms reported on this copy of Form
W-2
This W-2 belongs to:
X JUSTINE
JUSTIN
a Employ ee's social security
OMB No.
1545-0008
X Standard W-2 (Ty ped or computer generated)
Non-Standard W-2 (Altered or hand written)
212-54-1187
Form W-2c, Corrected Wage and Tax Statement
b Employ er identif ication
1 Wages, tips, other comp 2 Federal inc tax withheld
33-9875214
20,000.00
3 Social security wages
c Employ er's name
2,000.00
4 Social Sec tax withheld
0.00
TARGET
5 Medicare wages and tips
Employ er's address
0.00
6 Medicare tax withheld
0.00
123 ELM DR
State
Employ er's
SAN JOSE
CA
Zip Code
92871
Employ er's f oreign country
7 Social security tips
0.00
8 Allocated tips
0.00
0.00
9
10 Dependent care benef its
11 Nonqualif ied plans
12 Code
0.00
Foreign prov ince/county
0.00
Foreign postal code
0.00
Retirement plan
0.00
Third-party sick pay
0.00
JUSTINE
Suf f .
CASE
f
0.00
Employ ee's address
123 MAIN ST
State
Employ ee's
SAN DIEGO
CA
Zip Code
92101
Employ ee's f oreign country
Foreign prov ince/county
15 State State ID
CA
5628874
500.00
13 Statutory employ ee
e Employ ee's f irst
Employ ee's last
D
Amount
0.00
14 See
se
ction d
e xpande
below.
0.00
0.00
Foreign postal code
16 State wages
17 State inc tax
18 Local wages
19 Local W/H
20,000.00
1,000.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
0.00
W-2 Wage and Tax
2012
20 Local name
Department of the Treasury Internal Rev enue
State me nt
Othe r Ite ms reported on this copy of Form
W-2
Form
2012
IT-40
State Form 154
(R11 / 9-12)
Indiana Full-Year Resident
Individual Income Tax Return
Due April 15, 2013
If filing for a fiscal year, enter the dates (see instructions) (MM/DD/YYYY):
to:
from
Your Social
Security Number
131
65
2217
Spouse's Social
Security Number
Place “X” in box if applying for ITIN
Initial
Last name
Your first name
JUSTIN
212
54
1187
Place “X” in box if applying for ITIN
Suffix
CASE
If filing a joint return, spouse's first name
Initial
JUSTINE
Last name
Suffix
CASE
Present address (number and street or rural route)
Place "X" in box if you are
married filing separately.
Zip/Postal code
123 MAIN ST
State
City
SAN DIEGO
CA
92101
School corporation number (see pages 59 and 60 )
Foreign country 2-character code (see pg. 6)
Enter below the 2-digit county code numbers (found on the back of Schedule CT-40) for the county where you lived and
worked on January 1, 2012.
County where
County where
County where
County where
you lived
you worked
spouse lived
spouse worked
Round all entries
1. Enter your federal adjusted gross income (AGI) from your federal tax return (from Form 1040,
line 37; Form 1040A, line 21; or from Form 1040EZ, line 4)
Federal AGI
1
60000.00
2. Enter amount from Schedule 1, line 8, and enclose Schedule 1
2
.00
3
60000.00
Indiana Deductions
4
.00
Indiana Adjusted Income
5
60000.00
Indiana Exemptions
6
2000.00
State Taxable Income
7
58000.00
11
1972.00
Indiana Add-Backs
3. Add line 1 and line 2
4. Enter amount from Schedule 2, line 12, and enclose Schedule 2
5. Subtract line 4 from line 3
6. You must complete Schedule 3. Enter amount from Schedule 3, line 5,
and enclose Schedule 3
7. Subtract line 6 from line 5
8. State adjusted gross income tax: multiply line 7 by 3.4% (.034)
(if answer is less than zero, leave blank)
9. County tax. Enter county tax due from Schedule CT-40
(if answer is less than zero, leave blank)
10. Other taxes. Enter amount from Schedule 4, line 4 (enclose sch.)
8
1972.00
9
.00
10
.00
11. Add lines 8, 9, and 10. Enter total here and on line 16 on the back
15112111064
Indiana Taxes
12. Enter credits from Schedule 5, line 8 (enclose schedule)
2000.00
12
13. Enter offset credits from Schedule 6, line 7 (enclose schedule) 13
14. Automatic Taxpayer Refund credit. Leave blank if not eligible. See instructions on page 9.
Enter $111 if you are eligible
Enter $222 if joing filing and both eligible
14
Enter $111 if joing filing but only one is eligible
.00
.00
Indiana Credits
15
2000.00
Indiana Taxes
16
1972.00
17. If line 15 is equal to or more than line 16, subtract line 16 from line 15 (if smaller, skip to line 24)
17
28.00
18. Amount from line 17 to be donated to the Indiana Nongame Wildlife Fund
18
.00
19
28.00
Total to be applied to your estimated tax account (a + b + c; cannot be more than line 19)
20d
.00
21. Penalty for underpayment of estimated tax from Schedule IT-2210 or IT-2210A (enclose sch.)
21
.00
22. Refund: Line 19 minus lines 20d and 21. Note: If less than zero, see line 24
22
28.00
24. If line 16 is more than line 15, subtract line 15 from line 16. Add to this any amount on line 21
(see instructions on page 13 )
24
.00
25. Penalty if filed after due date (see instructions)
25
.00
26. Interest if filed after due date (see instructions)
26
.00
15. Add lines 12, 13 and 14
16. Enter amount from line 11
19. Subtract line 18 from line 17
Overpayment
20. Amount from line 19 to be applied to your 2013 estimated tax account (see instructions on page 11 ).
Enter your county code
county tax to be applied $
a
.00
Spouse's county code
county tax to be applied $
b
.00
c
.00
Indiana adjusted gross income tax to be applied
23. Direct Deposit (see page 12)
c. Type:
$
Checking
Savings
Your Refund
Hoosier Works MC
a. Routing Number
b. Account Number
c. Place an "X" in the box if refund will go to an account outside the United States
.00
Amount You Owe 27
27. Amount Due: Add lines 24, 25 and 26
Do not send cash. Please make your check or money order payable to: Indiana Department of Revenue.
Sign and date this return after reading the Authorization statement on Schedule 7. You must enclose Schedule 7.
Your Signature
Date
Spouse's Signature
If enclosing payment mail to: Indiana Department of Revenue, P.O. Box 7224, Indianapolis, IN 46207-7224.
Mail all other returns to: Indiana Department of Revenue, P.O. Box 40, Indianapolis, IN 46206-0040.
15112121064
Date
For Privacy Notice, get form FTB 1131.
California Resident
Income Tax Return
APE
131-65-2217
JUSTIN
JUSTINE
2012
2
0
00
0
00
0
208
60000
60000
0
0
60000
7682
52318
1236
208
1028
0
1028
0
0
0
0
0
540
CA
212-54-1187
AC
12
A
R
RP
92101
45
46
47
48
61
62
63
64
71
72
73
74
75
91
92
93
94
95
400
401
402
403
01-01-1981
0
0
0
1028
0
0
0
1028
1000
0
0
0
1000
0
0
0
28
0
0
0
0
0
404
405
406
407
408
410
412
413
414
419
420
421
422
423
110
111
112
113
115
116
117
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
28
0
0
0
0
0
01-01-1983
APE
FS
3800
3803
SCHG1
5870A
5805 5805F
DESIGNEE
TPID
FN
CCF
3805P
NQDC
3540
3805Z
3807
3808
3809
3549A
IRC 1341
Under penalties of perjury, I declare that I have examined this tax return, including accompanying schedules and statements, and to the best of my knowledge and belief, it is true, correct, and complete.
Sign
Here
It is unlawful
to forge a
spouse's/
RDP's
signature.
Joint tax
return?
(see instr.)
Your signature
Daytime phone number (optional)
C1 Side 1
DO NOT ATTACH FEDERAL RETURN
P
CASE
CASE
CASE
123 MAIN ST
SAN DIEGO
01
06
09
10
11
12
13
14
16
17
18
19
31
32
33
34
35
40
41
42
43
44
FORM
Spouse's/RDP's signature (if a joint tax return, both must sign)
619-555-1212
Date
Your email address (optional). Enter only one.
Paid preparer's signature (declaration of preparer is based on all information of which preparer has any knowledge)
PTIN
Firm's name (or yours, if self-employed)
Firm's address
FEIN
Do you want to allow another person to discuss this return with us? (see instructions)
Print Third Party Designee's Name
. . . . . . . . . . .
Telephone Number
031
3101126
Yes
No
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Your name:
CASE
Filing Status
Your SSN or ITIN: 131-65-2217
1
2
Single
X
Married/RDP filing jointly. (see instructions)
3
Married/RDP filing separately. Enter spouse’s/RDP’s SSN or ITIN above and full name here
4
Head of household (with qualifying person). (see instructions)
5
Qualifying widow(er) with dependent child. Enter year spouse/RDP died.
If your California filing status is different from your federal filing status, check the box here . . . . . . . . . .
6 If someone can claim you (or your spouse/RDP) as a dependent, check the box here (see instructions) . . . .
Exemptions
6
Whole dollars only
7 Personal: If you checked box 1, 3, or 4 above, enter 1 in the box. If you checked 2 or 5, enter 2 in the box.
If you checked the box on line 6, see instructions . . . . . . . . . . . . . . . . . . . . . 7
2 X $104 = $
. . 8
X $104 = $
X $104 = $
8 Blind: If you (or your spouse/RDP) are visually impaired, enter 1; if both are visually impaired, enter 2
9 Senior: If you (or your spouse/RDP) are 65 or older, enter 1; if both are 65 or older, enter 2
9
208.
10 Dependents: Do not include yourself or your spouse/RDP.
First Name
Dependent's
relationship to you
Last Name
Total dependent exemptions . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Taxable
Income
10
X $321 = $
$
11 Exemption amount: Add line 7 through line 10. Transfer this amount to line 32 . . . . . . .
11
12 State wages from your Form(s) W-2, box 16 . . . . . . . . . . . . . . . . . .
60,000.
12
13 Enter federal adjusted gross income from Form 1040, line 37; Form 1040A, line 21; Form 1040EZ, line 4
13
14 California adjustments - subtractions. Enter the amount from Schedule CA (540), line 37, column B . . .
14
15 Subtract line 14 from line 13. If less than zero, enter the result in parentheses (see instructions) . . . . . 15
16 California adjustments - additions. Enter the amount from Schedule CA (540), line 37, column C . . . .
16
17 California adjusted gross income. Combine line 15 and line 16 . . . . . . . . . . . . . . . . . . . .
17
18 Enter the larger of your CA standard deduction OR your CA itemized deductions. . . . . . . . . .
18
19 Subtract line 18 from line 17. This is your taxable income . If less than zero, enter -0- . . . . . . . . .
19
31 Tax. Check box if from:
Tax
X
Tax Table
Tax Rate Schedule
32
33 Subtract line 32 from line 31. If less than zero, enter -0- . . . . . . . . . . . . . . . . . . . . . . .
33
Payments
Schedule G-1
Form FTB 5870A . . . . .
35
40 Nonrefundable Child and Dependent Care Expenses Credit, (See inst.). Attach Form FTB 3506. . . . .
40
41 New jobs credit, amount generated (see instructions) . . . . . . . . . . . . . .
42
amount . . . . . . . . . . . . . . . .
43
44 Credit
Code
amount . . . . . . . . . . . . . . . .
45 To claim more than two credits (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . .
44
46 Nonrefundable renter's credit (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . .
46
47 Add line 40 and line 42 through line 46. These are your total credits . . . . . . . . . . . . . . . . . .
47
48 Subtract line 47 from line 35. If less than zero, enter -0- . . . . . . . . . . . . . . . . . . . . . . .
48
61 Alternative minimum tax. Attach Schedule P (540) . . . . . . . . . . . . . . . . . . . . . . . . . .
61
62 Mental Health Services Tax (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . . .
62
63 Other taxes and credit recapture (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . .
63
64 Add line 48, line 61, line 62, and line 63. This is your total tax . . . . . . . . . . . . . . . . . . . . .
64
71 California income tax withheld (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . .
71
72 2012 CA estimated tax and other payments (see instructions) . . . . . . . . . . . . . . . . . . . .
72
73 Real estate and other withholding (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . .
73
74 Excess SDI (or VPDI) withheld (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . .
74
75 Add line 71, line 72, line 73, and line 74. These are your total payments (see instructions) . . . . . . .
75
Side 2 Form 540 C1 2012
031
3102126
60,000.
60,000.
7,682.
52,318.
1,236.
208.
1,028.
1,028.
41
42 New jobs credit, amount claimed (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . .
Code
60,000.
34
35 Add line 33 and line 34 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
43 Credit
Other
Taxes
31
32 Exemption credits. Enter the amount from line 11. If your federal AGI is more than $169,730 (see instr.)
34 Tax. (see instructions) Check box if from:
Special
Credits
FTB 3803 .
FTB 3800 or
208.
45
0.
1,028.
1,028.
1,000.
1,000.
Your name:
CASE
Overpaid Tax/
Tax Due
Use Tax
Your SSN or ITIN: 131-65-2217
91 Overpaid tax. If line 75 is more than line 64, subtract line 64 from line 75. . . . . . . . . . . . . . .
91
92 Amount of line 91 you want applied to your 2013 estimated tax . . . . . . . . . . . . . . . . . . . .
92
93 Overpaid tax available this year. Subtract line 92 from line 91 . . . . . . . . . . . . . . . . . . . . .
93
94 Tax due. If line 75 is less than line 64, subtract line 75 from line 64 . . . . . . . . . . . . . . . . . .
94
95 Use Tax. This is not a total line (see instructions) . . . . . . . . . . . . . . .
Code
C
O
N
T
R
I
B
U
T
I
O
N
S
California Seniors Special Fund (see instructions) . . . . . .
Alzheimer’s Disease/Related Disorders Fund . . . . . . . .
California Fund for Senior Citizens . . . . . . . . . . . . .
Rare and Endangered Species Preservation Program . . . .
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
400
Add code 400 through code 423. This is your total contribution . . . . . . . . . . . . . . . . . . . . . . . . .
110
State Children’s Trust Fund for the Prevention of Child Abuse
California Breast Cancer Research Fund . . . . . .
California Firefighters’ Memorial Fund . . . . . . . .
Emergency Food For Families Fund . . . . . . . .
California Peace Officer Memorial Foundation Fund .
California Sea Otter Fund . . . . . . . . . .
Municipal Shelter Spay-Neuter Fund . . . . .
California Cancer Research Fund . . . . . . .
ALS/Lou Gehrig's Disease Research Fund . .
.
.
.
.
Child Victims of Human Trafficking Fund . . .
.
California YMCA Youth and Government Fund.
.
.
California Youth Leadership Fund . . . . . . .
School Supplies for Homeless Children Fund .
.
State Parks Protection Fund/Parks Pass Purchase.
110
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
402
403
404
405
406
407
408
410
412
413
414
419
420
421
422
423
111 AMOUNT YOU OWE. Add line 94, line 95, and line 110 (see instructions). Do Not Send Cash.
Interest and
Penalties
112 Interest, late return penalties, and late payment penalties . . . . . . . . . . . . . . . . . . . . . . . . 112
Mail to: FRANCHISE TAX BOARD, PO BOX 942867, SACRAMENTO CA 94267-0009 . .
Pay online – Go to ftb.ca.gov for more information.
FTB 5805 attached
Amount
401
Amount
You Owe
113 Underpayment of estimated tax. Check box:
28.
95
28.
111
FTB 5805F attached . .
113
28.
114 Total amount due (see instructions). Enclose, but do not staple, any payment . . . . . . . . . . . . . 114
Refund and
Direct Deposit
115 REFUND OR NO AMOUNT DUE. Subtract line 95 and line 110 from line 93 (see instructions).
Mail to: FRANCHISE TAX BOARD, PO BOX 942840, SACRAMENTO CA 94240-0009
115
Fill in the information to authorize direct deposit of your refund into one or two accounts. Do not attach a voided check or a deposit slip (see instructions).
0.
Have you verified the routing and account numbers? Use whole dollars only.
All or the following amount of my refund (line 115) is authorized for direct deposit into the account shown below:
Routing number
Checking
Savings
Type
Account number
116 Direct deposit amount
The remaining amount of my refund (line 115) is authorized for direct deposit into the account shown below:
Routing number
Checking
Savings
Type
031
Account number
3103126
117 Direct deposit amount
Form 540 C1 2012
Side 3
Form
Indiana Part-Year or Full-Year Nonresident
Individual Income Tax Return
IT-40PNR
State Form 472
(R 11 / 9-12)
2012
If filing for a fiscal year, enter the dates (see instructions) (MM/DD/YYY):
from:
Your Social
Security Number
131
65
2217
Spouse's Social
Security Number
JUSTIN
212
54
1187
Place “X” in box if applying for ITIN
Suffix
Place “X” in box if applying for ITIN
Initial
Last name
Your first name
Due April 15, 2013
to:
CASE
If filing a joint return, spouse's first name
Initial
JUSTINE
Suffix
Last name
CASE
Present address (number and street or rural route)
Place “X” in box if you are
married filing separately.
Zip/Postal code
123 MAIN ST
State
City
SAN DIEGO
CA
92101
School corporation number (see pages 61 and 62)
Foreign country 2-character code (see pg. 5)
9999
Enter below the 2-digit county code numbers (found on the back of Schedule CT-40PNR) for the county where you lived and
worked on January 1, 2012.
County where
you lived
00
County where
you worked
County where
spouse lived
00
County where
spouse worked
00
00
Round all entries
1. Complete Schedule A first. Enter here the amount from Section 3, line 37B, and enclose
Schedule A
Indiana Income
1
40000.00
2. Enter amount from Schedule B, line 6, and enclose Schedule B
2
.00
3
40000.00
Indiana Deductions
4
5000.00
Indiana Adjusted Income
5
35000.00
Indiana Exemptions
6
1334.00
State Taxable Income
7
33666.00
Indiana Taxes 11
1145.00
Indiana Add-Backs
3. Add line 1 and line 2
4. Enter amount from Schedule C, line 12, and enclose Schedule C
5. Subtract line 4 from line 3
6. You must complete Schedule D. Enter amount from Schedule D, line 7,
and enclose Schedule D
7. Subtract line 6 from line 5
8. State adjusted gross income tax: multiply line 7 by 3.4% (.034)
(if answer is less than zero, leave blank)
9. County tax. Enter county tax due from Schedule CT-40PNR
(if answer is less than zero, leave blank)
8
1145.00
9
.00
10. Other taxes. Enter amount from Schedule E, line 4 (enclose sch.)
10
.00
11. Add lines 8, 9 and 10. Enter total here and on line 16 on the back
15712111064
12. Enter credits from Schedule F, line 8 (enclose schedule)
12
2000.00
13. Enter offset credits from Schedule G, line 7 (enclose schedule)
14. Automatic Taxpayer Refund credit
Enter $111 if joint filing but only one is eligible (leave blank
if not eligible; see instructions on page 9 )
13
.00
14
.00
Indiana Credits
15
2000.00
Indiana Taxes
16
1145.00
17. If line 15 is equal to or more than line 16, subtract line 16 from line 15 (if smaller, skip to line 24)
17
855.00
18. Amount from line 17 to be donated to the Indiana Nongame Wildlife Fund
18
.00
19
855.00
Total to be applied to your estimated tax account (a + b + c; cannot be more than line 19)
20d
.00
21. Penalty for underpayment of estimated tax from Schedule IT-2210 or IT-2210A (enclose sch.)
21
.00
22. Refund: Line 19 minus lines 20d and 21. Note: If less than zero, see line 24 instructions
22
855.00
24. If line 16 is more than line 15, subtract line 15 from line 16. Add to this any amount on line 21
(see instructions on page 13 )
24
.00
25. Penalty if filed after due date (see instructions)
25
.00
26. Interest if filed after due date (see instructions)
26
.00
15. Add lines 12, 13 and 14
16. Enter amount from line 11
Overpayment
19. Subtract line 18 from line 17
20. Amount from line 19 to be applied to your 2013 estimated tax account (see instructions on page 11 ).
Enter your county code
county tax to be applied $
a
.00
Spouse's county code
county tax to be applied $
b
.00
c
.00
Indiana adjusted gross income tax to be applied
23. Direct Deposit (see page 12)
c. Type
$
Checking
Savings
Your Refund
Hoosier Works MC
a.
Routing Number
b.
Account Number
d.
Place an "X" in the box if refund will go to an account outside the United States
.00
27. Amount Due: Add lines 24, 25 and 26
Amount You Owe 27
Do not send cash. Please make your check or money order payable to: Indiana Department of Revenue.
Sign and date this return after reading the Authorization statement on Schedule H. You must enclose Schedule H.
Your Signature
Date
Spouse's Signature
If enclosing payment mail to: Indiana Department of Revenue, P.O. Box 7224, Indianapolis, IN 46207-7224.
Mail all other returns to: Indiana Department of Revenue, P.O. Box 40, Indianapolis, IN 46206-0040.
15712121064
Date
For Privacy Notice, get form FTB 1131.
FORM
California Nonresident or Part-Year
Resident Income Tax Return 2012
Long Form
540NR
C1
Side 1
APE
131-65-2217
JUSTIN
JUSTINE
CASE
CASE
CASE
123 MAIN ST
SAN DIEGO
Filing Status
1
2
3
4
5
CA
212-54-1187
92101
P
AC
A
R
RP
12
01-01-1981
01-01-1983
Single
X
Married/RDP filing jointly. (see instructions)
Married/RDP filing separately. Enter spouse's/RDP's SSN or ITIN above and full name here
Head of household (with qualifying person). (see instructions)
Qualifying widow(er) with dependent child. Enter year spouse/RDP died
.
If your California filing status is different from your federal filing status, fill in the box here . . . . .
6 If someone can claim you (or your spouse/RDP) as a dependent, fill in the box (see instr.) . . . .
Exemptions
U
6
For line 7, line 8, line 9, and line 10: Multiply the amount you enter in the box by the pre-printed dollar amount for that line.
7 Personal: If you filled in 1, 3, or 4 above, enter 1 in the box. If you filled in 2 or 5, enter 2 in the box.
If you checked the box on line 6, see instructions. . . . . . . . . . . . . . . . . . . .
8 Blind: If you (or your spouse/RDP) are visually impaired, enter 1; if both are visually impaired, enter 2
7
8
9 Senior: If you (or your spouse/RDP) are 65 or older, enter 1; if both are 65 or older, enter 2 . . . .
9
2
0
0
Whole dollars only
X $104 = $
X $104 = $
X $104 = $
208.
10 Dependents:
First name
Total
Taxable
Income
Last name
Dependent's
relationship to you
Total dependent exemptions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 0
X $321 = $
11 Exemption amount: Add line 7 through line 10 . . . . . . . . . . . . . . . . . . . 11
$
12 Total California wages from your Form(s) W-2, box 16 . . . . . . . . . . . . . . .
12
20,000.
13 Enter federal AGI from Form 1040, line 37; 1040A, line 21; 1040EZ, line 4; 1040NR, line 36; or 1040NR-EZ, line 10 . . .
13
14 California adjustments - subtractions. Enter the amount from Schedule CA (540NR), line 37, column B .
14
15 Subtract line 14 from line 13. If less than zero, enter the result in parentheses (see instructions) . . . . . 15
208.
60,000.
40,000.
20,000.
16 California adjustments - additions. Enter the amount from Schedule CA (540NR), line 37, column C . .
16
17 Adjusted gross income from all sources. Combine line 15 and line 16 . . . . . . . . . . . . . . . . .
17
20,000.
Your California standard deduction (see instructions) . . . . . . . . . . . . . . . . . . . . . . .
18
19 Subtract line 18 from line 17. This is your total taxable income. If less than zero, enter -0- . . . . . .
19
7,682.
12,318.
18 Enter the larger of: Your California itemized deductions from Schedule CA (540NR), line 43; OR
031
3131124
Your name:
CASE
CA
Taxable
Income
Your SSN or ITIN: 131-65-2217
31
123.
35 CA Taxable Income from Schedule CA (540NR), Part IV, line 49 . . . . . . . . . . . . . . . . . . .
35
36
36 CA Tax Rate. Divide line 31 by line 19 . . . . . . . . . . . . . . . . . .
0.0100
37 CA Tax Before Exemption Credits. Multiply line 35 by line 36 . . . . . . . . . . . . . . . . . . . . . 37
38
38 CA Exemption Credit Percentage. Divide line 35 by line 19. If more than 1, enter 1.0000
1.0000
12,318.
31 Tax. Fill in the box if from:
X
Tax Table
Tax Rate Schedule
FTB 3800
32 CA adjusted gross income from Schedule CA (540NR), Part IV, line 45 . . .
FTB 3803
20,000.
32
123.
39 CA Prorated Exemption Credits. Multiply line 11 by line 38. If the amount on line 13 is more than
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
39
40 CA Regular Tax Before Credits. Subtract line 39 from line 37. If less than zero, enter -0- . . . . . . . .
Schedule G-1
FTB 5870A . . . . . . . .
41 Tax (see instructions). Check the box if from:
42 Add line 40 and line 41.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
40
$169,730 (see instr.)
Special
Credits
0.
50
52
53
1.000000
55 Credit amount (see instructions)
55
56
56 New jobs credit, amount generated (see instructions) . . . . . . . . . . . .
57 New jobs credit, amount claimed (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . .
57
58 Enter credit name
code number
and amount . .
58
59 Enter credit name
code number
and amount . .
59
60 To claim more than two credits (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . .
60
61 Nonrefundable renter's credit (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . . .
61
. . . . . . . . . . . . .
62
63 Subtract line 62 from line 42. If less than zero, enter -0- . . . . . . . . . . . . . . . . . . . . . . .
63
71 Alternative minimum tax. Attach Schedule P (540NR) . . . . . . . . . . . . . . . . . . . . . . . .
71
. . . . . . . . . . . . . . . . . . . . . . . . . . .
73 Other taxes and credit recapture (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . .
72
. . . . . . . . . . . . . . . . . . . .
74
0.
1,000.
62 Add line 50, line 55 and line 57 through line 61. These are your total credits
72 Mental Health Services Tax (see instructions)
74 Add line 63, line 71, line 72, and line 73. This is your total tax
Payments
42
51
If more than 1, enter 1.000 (see instructions) . . . . . . . . . . . . . . . . 54
Other Taxes
41
50 Nonrefundable Child and Dependent Care Expenses Credit (see page 20). Attach form FTB 3506 . . .
51 Credit for joint custody head of household (see instructions) . . . . . . . . .
52 Credit for dependent parent (see instructions) . . . . . . . . . . . . . . .
53 Credit for senior head of household (see instructions) . . . . . . . . . . . .
54 Credit percentage. Divide line 35 by line 19.
208.
0.
73
. . . . . . . . . . . . . . . . . . . . . . . . . .
81
82 2012 CA estimated tax and other payments (see instructions) . . . . . . . . . . . . . . . . . . . .
82
83 Real estate or other withholding (see instructions) . . . . . . . . . . . . . . . . . . . . . . . . . .
83
. . . . . . . . . . . . . . . . . . . . . . . . .
85 Add line 81, line 82, line 83, and line 84. These are your total payments . . . . . . . . . . . . . . .
84
81 California income tax withheld (see instructions)
84 Excess SDI (or VPDI) withheld. (see instructions)
Overpaid Tax/ 101 Overpaid tax. If line 85 is more than line 74, subtract line 74 from line 85 .
102 Amount of line 101 you want applied to your 2013 estimated tax . . . . .
Tax Due
103 Overpaid tax available this year. Subtract line 102 from line 101 . . . . .
104 Tax due. If line 85 is less than line 74, subtract line 85 from line 74 . . .
Side 2 Long Form 540NR 2012
031
3132124
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
0.
85
1,000.
101
1,000.
102
103
104
1,000.
Your name:
CASE
Your SSN or ITIN: 131-65-2217
Code
400
C
O
N
T
R
I
B
U
T
I
O
N
S
Amount
. . . . . . . .
410
Alzheimer's Disease/Related Disorders Fund . . .
401
Municipal Shelter Spay-Neuter Fund . . . . .
412
California Fund for Senior Citizens . . . . . . .
402
California Cancer Research Fund . . . . . .
413
ALS/Lou Gehrig’s Disease Research Fund . .
414
Child Victims of Human Trafficking Fund . . .
419
California YMCA Youth and Government Fund
420
California Seniors Special Fund (see instructions)
California Sea Otter Fund
Rare and Endangered Species
Preservation Program . . . . . . . . . . . .
403
State Children's Trust Fund for the Prevention
of Child Abuse . . . . . . . . . . . . . .
404
California Youth Leadership Fund . . . . . .
421
California Breast Cancer Research Fund . . . . .
405
School Supplies for Homeless Children Fund .
422
California Firefighters’ Memorial Fund . . . . . .
406
State Parks Protection Fund/Parks Pass Purchase
423
Emergency Food For Families Fund . . . . . . .
407
California Peace Officer Memorial
Foundation Fund . . . . . . . . . . . . . .
408
120 Add code 400 through code 423. This is your total contribution . . . . . . . . . . . . . . . . . . . .
Amount
You Owe
121 AMOUNT YOU OWE. Add line 104 and line 120 (see instructions). Do not send cash.
Mail to: FRANCHISE TAX BOARD, PO BOX 942867, SACRAMENTO CA 94267-0001 . . . . .
120
0.
121
Pay Online – Go to ftb.ca.gov form more information.
Interest and
Penalties
122 Interest, late return penalties, and late payment penalties . . . . . . . . . . . . . . . . . . . . . . .
122
FTB 5805F attached .
123
124 Total amount due (see instructions). Enclose, but do not staple, any payment . . . . . . . . . . . .
124
Refund and
Direct Deposit
125 REFUND OR NO AMOUNT DUE. Subtract line 120 from line 103.
123 Underpayment of estimated tax. Check the box:
FTB 5805 attached
Mail to: FRANCHISE TAX BOARD, PO BOX 942840, SACRAMENTO CA 94240-0001 . . . . .
1,000.
125
Fill in the information to authorize direct deposit of your refund into one or two accounts. Do not attach a voided check or a deposit slip
(see instructions) Have you verified the routing and account numbers? Use whole dollars only.
All or the following amount of my refund (line 125) is authorized for direct deposit into the account shown below:
Checking
Savings
Routing number
Account number
Type
126 Direct deposit amount
The remaining amount of my refund (line 125) is authorized for direct deposit into the account shown below:
Checking
Savings
Routing number
Type
127 Direct deposit amount
Account number
IMPORTANT: Attach a copy of your complete federal return.
Under penalties of perjury, I declare that I have examined this tax return, including accompanying schedules and statements, and to the best of my
knowledge and belief, it is true, correct, and complete.
Sign
Here
It is unlawful
to forge a
spouse’s/RDP’s
signature.
Joint tax return?
(see instr.)
Your signature
Spouse's/RDP's signature
(if a joint return, both must sign)
Daytime phone number (optional)
X
X
Date
(619)555-1212
Your email address (optional). Enter only one email address.
Paid preparer's signature (declaration of preparer is based on all information of which preparer has any knowledge)
PTIN
Firm's name (or yours if self-employed)
FEIN
Firm's address
Do you want to allow another person to discuss this tax return with us (see instructions)? .
. . . . . . . . .
Yes
No
Telephone Number
Print Third Party Designee's Name
031
3133124
Long Form 540NR C1 2012 Side 3