Pap Test Training Guideline for Registered Nurses
advertisement

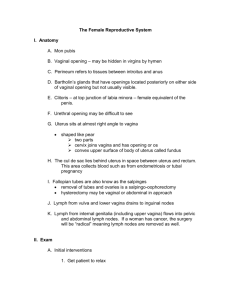
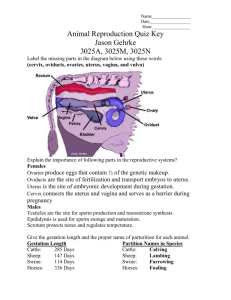
PAP TRAINING GUIDELINE FOR REGISTERED NURSES Updated January 2015 Cancer Care Nova Scotia, Cervical Cancer Prevention Program Rm 543 Bethune Building 1276 South Park Street Halifax, NS B3H 2Y9 Phone: 902-473-7438 or 1-888-480-8588 Fax: 902-473-4982 Email: screening@ccns.nshealth.ca Website: www.cancercare.ns.ca This is a generic training guide developed by the Cervical Cancer Prevention Program, Cancer Care Nova Scotia, designed for Registered Nurses (RN) to guide the development of their competency in Pap test collection. It is not a mandatory requirement. The RN is responsible for ensuring that he/she is practicing in accordance with their scope of practice as outlined by their licensing body and are encouraged to use other available resources to meet their individual learning needs. * This guideline consists of a summary of the following: SECTION 1: Self Study Review of Anatomy & Physiology Health History Physical Examination SECTION 2: Preceptorship SECTION 3: Critical Reflection on Quality SECTION 4 - Practical Tips from Pap Test Providers to support conversations with women about Pap testing. *For specific competency policies and procedures, refer to your practicing insitution/health region Pap Training Guideline for Registered Nurses v.2015 -2- SECTION 1 – Self Study Learning Objectives: On completion of self study the learner should be able to: 1. Describe the three sampling areas and identify the importance of obtaining samples from these three areas. 2. Describe the steps in the procedure for obtaining a Pap test. 3. Identify possible complications, contraindications, and precautions associated with obtaining a Pap test. 4. Identify the preferred sampling methods for nulliparous, parous, post-treatment, postmenopausal, pregnant and post-hysterectomy women. 5. Describe the difference between a Pap test and a pelvic exam. For a glossary of terminology related to Pap test screening and references that support the material provided within this manual see Appendix A. REVIEW OF ANATOMY & PHYSIOLOGY A. Female Genitalia External and internal structures comprise the female genitalia. External Genitalia The vulva contains the external female genitalia that are visible on inspection. The mons pubis is the cushion of adipose and connective tissue covered by skin and coarse, curly hair in a triangular pattern over the symphysis pubis (the joint formed by the union of the pubic bones anteriorly). The labia majora border the vulva laterally from the mons pubis to the perineum (muscle, fascia, and ligaments between the anus and vulva). The labia minora, two moist lesser mucosal folds, darker pink to red, lie within and alongside the labia majora. When the labia is spread, the introitus (vaginal orifice) and the urethral meatus are visible. Less easily visible are the multiple orifices of Skene's glands, mucus-producing glands located on both sides of the urethral opening. Openings of the two mucus-producing Bartholin's glands are located laterally and posteriorly on either side of the inner vaginal wall. The hymen, a tissue membrane varying in size and thickness, may completely or partially cover the vaginal orifice. A disrupted hymen appears as remnants of uneven mucosal tissue tags, called myrtiform caruncles. Pap Training Guideline for Registered Nurses v.2015 -3- Internal Genitalia The vagina, a highly elastic muscular tube, is located between the urethra and the rectum and lies at a 45-degree angle to the long axis of the body. The uterus, a small, firm, pear-shaped, muscular organ, rests between the bladder and the rectum and usually lies at almost a 90-degree angle to the vagina. However, other locations may be normal. The membrane lining the uterus is called the endometrium, the muscular layer, the myometrium. In pregnancy, the elastic, upper uterine portion (the fundus) accommodates most of the growing fetus until term. The uterine neck (isthmus) joins the fundus to the cervix, the uterine part extending into the vagina. The fundus and the isthmus make up the corpus, the main uterine body. Although anteflexed or anteverted above or over the empty bladder in most women, the uterus can be midplane (its long axis parallel to the long axis of the body), retroverted, or retroflexed. (See illustration on page 24.) Two Fallopian tubes attach to the uterus at the upper angle of the fundus. Usually nonpalpable, these 4 - 14 cm. (2 3/4" - 5 1/2") long, narrow tubes of muscle fibres have fingerlike projections, called fimbriae, on the free ends that partially surround the ovaries. Fertilization of the ovum usually occurs in the outer third of the Fallopian tube. Oval, almond-shaped organs approximately 3 - 3.5 cm. (1 1/4 " - 1 1/2 ") long, 2 cm. (3/4") wide, and 1 - 1/5 cm. (1/4" - 1/2") thick, the ovaries usually lie near the lateral pelvic walls, a little below the anterosuperior iliac spine. View of external genitalia in lithotomy position Pap Training Guideline for Registered Nurses v.2015 -4- Lateral view of internal genitalia Anterior crosssectional view of internal genitalia B. Menstrual Cycle The average menstrual cycle usually occurs over 28 days, although the normal cycle may range from 22 to 34 days. The cycle is regulated by fluctuating hormone levels that, in turn, are regulated by negative and positive feedback mechanisms. The three phases are described below. Pap Training Guideline for Registered Nurses v.2015 -5- Menstrual (Preovulatory) Phase The cycle starts with menstruation (cycle day 1) which usually lasts 5 days. As the cycle begins, low estrogen and progesterone levels in the bloodstream stimulate the hypothalamus to secrete gonadotropin-releasing hormone (GnRH). In turn, this substance stimulates the anterior pituitary to secrete follicle-stimulating hormone (FSH) and luteinizing hormone (LH). When the FSH level rises, LH output increases. Proliferative (Follicular) Phase and Ovulation The proliferative phase lasts from cycle day 6 to 14. During this phase, LH and FSH act on the ovarian follicle (mature ovarian cyst containing the ovum), causing estrogen secretion, which in turn stimulates the buildup of the endometrium. Late in the proliferative phase, estrogen levels peak, FSH secretion declines, and LH secretion increases, surging at midcycle (around day 14). Then, estrogen production decreases, the follicle matures, and ovulation occurs. Normally, one follicle matures during the ovulatory process and is released from the ovary during each cycle. Luteal (Secretory) Phase During the luteal phase, which lasts about 14 days, FSH and LH levels drop. Estrogen levels decline initially, then increase along with progesterone levels as the corpus luteum (progesterone producing yellow structure that develops on the surface of the ovary, after the follicle ruptures) begins functioning. During this phase, the endometrium responds to progesterone stimulation by becoming thick and secretory in preparation for implantation of a fertilized ovum. About 10 to 12 days after ovulation, the corpus luteum begins to diminish as do estrogen and progesterone levels, until the hormone levels are insufficient to sustain the endometrium in a fully developed secretory state. Then the endometrial lining is shed (menses). Decreasing estrogen and progesterone levels stimulate the hypothalamus to produce GnRH, and the cycle begins again. C. Developmental Changes in the Uterus and Cervix Over a woman's lifetime, the size of the uterine corpus and cervix changes as does the percentage of space these parts occupy. For example, of the space filled by the whole uterus in a premenarchial female, one third may be uterine corpus, and two thirds may be cervix. In the adult multiparous female, the uterine corpus may occupy two thirds of the space available, whereas the cervix may fill a third. The central opening of the cervix (the external os), visible by speculum, is round and closed in a nulliparous woman. In a parous woman, the opening is an irregular shaped slit. Pap Training Guideline for Registered Nurses v.2015 -6- Adolescents During puberty the external genitalia increase in size and begin to assume adult proportions. The clitoris becomes more erectile and the labia minora more vascular. The labia majora and mons pubis become more prominent and begin to develop hair, often occurring simultaneously with breast development. If the hymen is intact, the vaginal opening is about 1 cm in size. The vagina lengthens, and the epithelial layers thicken. The vaginal secretions become acidic. The uterus, ovaries, and Fallopian tubes increase in size and weight. The uterine musculature and vascular supply increase. The endometrial lining thickens in preparation for the onset of menstruation (menarche), which usually occurs between the ages of 8 and 16 years. Just before menarche, vaginal secretions increase. Functional maturation of the reproductive organs is reached during puberty. Pregnant Women The high levels of estrogen and progesterone that are necessary to support pregnancy are responsible for uterine enlargement during the first trimester. After the third month, uterine enlargement is primarily the result of mechanical pressure of the growing fetus. As the uterus enlarges the muscular walls strengthen and become more elastic. As the uterus becomes larger and more ovoid, it rises out of the pelvis into the abdominal cavity. Uterine weight at term, excluding the fetus and placenta, will usually have increased more than tenfold, to a weight of about 1000 g. Hormonal activity is probably also responsible for the softening and strengthening of the pelvic ligaments. As a result the pelvic joints separate slightly, allowing some mobility. During pregnancy an increase in uterine blood flow and lymph causes pelvic gestation and edema. As a result, the uterus, cervix, and isthmus soften, and the cervix takes on a bluish color. The softness and compressibility of the isthmus results in exaggerated uterine anteflexion during the first 3 months of pregnancy, causing the fundus to press on the urinary bladder. The vaginal changes are similar to the cervical changes and result in the characteristic violet color. Both the mucosa of the vaginal walls and the connective tissue thicken, and smooth muscle cells hypertrophy. These changes result in an increased length of the vaginal walls, so that at times they can be seen protruding from the vulvar opening. The vaginal secretions increase and have an acidic pH due to an increase in lactic acid production by the vaginal epithelium. Pap Training Guideline for Registered Nurses v.2015 -7- Comparison of vulva and cervix in nullipara, A, and multipara, B, at the same stage of pregnancy and parturition. A B Older Adults Concurrent with endocrine changes, ovarian function diminishes during a woman's 40s, and menstrual periods begin to cease between 40 and 55 years of age although fertility may continue. Menopause is completed after 1 year of no menses. Just as menarche in the adolescent is one aspect of puberty, so menopause is only one aspect of this transitional phase of the life cycle. During this time, estrogen levels decrease, causing the labia and clitoris to become smaller. The labia majora also become flatter as body fat is lost. Pubic hair turns gray and is usually more sparse. The vaginal introitus gradually constricts. The vagina narrows, shortens, and loses rugation, and the mucosa becomes thin, pale, and dry, which may result in dyspareunia. The cervix becomes small and more pale. The uterus decreases in size, and the endometrium thins. The ovaries also decrease in size to approximately 1 to 2 cm. Follicles gradually disappear, and the surface of the ovary convolutes. Ovulation usually ceases about 1 to 2 years before menopause. The ligaments and connective tissue of the pelvis sometimes lose their elasticity and tone, thus weakening the supportive sling for the pelvic contents. The vagina walls may lose some of their structural integrity. Pap Training Guideline for Registered Nurses v.2015 -8- D. Common Abnormalities Premenstrual Syndrome (PMS) Premenstrual syndrome usually begins in a woman's late 20s and increases in incidence and severity as menopause approaches. It is characterized by edema, headache, weight gain, and behavioral disturbances such as irritability, nervousness, dysphoria, and lack of coordination. Symptoms occur 5 to 7 days before menses and subside with onset of menses. Infertility The inability to conceive over a period of 1 year of unprotected regular intercourse has many causes, including both male and female conditions. Contributing factors in the woman include abnormalities of the vagina, cervix, uterus, Fallopian tubes, and ovaries. Male infertility can be caused by insufficient, nonmotile, or immature sperm, ductal obstruction of sperm, and transportrelated factors. Factors influencing both women and men include stress, nutrition, chemical substances, chromosomal abnormalities, certain disease processes, sexual and relationship problems, and immunologic response. Endometriosis The presence and growth of endometrial tissue outside the uterus causes pelvic pain, dysmenorrhea, and heavy or prolonged menstrual flow. On bimanual examination tender nodules may be palpable along the uterosacral ligaments. Diagnosis is confirmed by laparoscopy. Older Adults Atrophic Vaginitis Atrophy of the vagina is caused by lack of estrogen. The vaginal mucosa is dry and pale, though it may become reddened and develop petechiae and superficial erosions. The accompanying vaginal discharge may be white, gray, yellow, green, or blood-tinged. It can be thick or watery, and although it varies in amount, the discharge is rarely profuse. E. Inflammatory and Infectious Conditions Human Papilloma Virus (HPV) Human papilloma virus (HPV) is the most common sexually transmitted viral infection in the world today and is transmitted by skin-to-skin (including sexual) contact. HPV is a family of viruses; researchers believe that there are over 200 types. Warty lesions on the labia, within the vestibule, or in the perianal region are the result of HPV infection. Genital warts are generally flesh-colored, whitish pink to reddish brown, discrete, soft growths. They may occur singly or in clusters and may enlarge to form cauliflower-like masses. HPV is one of the most frequent causes of cervical dysplasia, which if left untreated can progress to cervical cancer. Cervical dysplasia seldom causes any noticeable symptoms. It is usually detected through the Pap test or colposcopy. Pap Training Guideline for Registered Nurses v.2015 -9- Herpes Venereal herpes is a sexually transmitted infection that produces small clear vesicles. The lesions may itch and are usually painful. Initial infection is often extensive, whereas recurrent infection is usually confined to a small localized patch of the vulva, perineum, vagina, or cervix. Vulva and Vagina Inflammation of Bartholin Gland Inflammation of the Bartholin glands may be acute or chronic. Acute inflammation produces a hot, red, tender fluctuant that may drain pus. Chronic inflammation results in a nontender cyst on the labium. Condyloma Latum Lesions of secondary syphilis appear 6 to 12 weeks after infection. They are flat, round or oval papules covered by gray exudate. Syphilitic Chancre (Primary Syphilis) A syphilitic chancre is a firm, painless ulcer. Most chancres in women develop internally and often go undetected. Pelvic Inflammatory Disease (PID) Often caused by gonococcal and chlamydial infection, pelvic inflammatory disease may be acute or chronic. Acute PID produces very tender, bilateral adnexal areas; the patient may guard and find bimanual examination very painful. The symptoms of chronic PID are bilateral, tender, irregular, and fairly fixed adnexal areas. Movement of cervix is painful (cervical excitation) whereas palpation of a normal cervix does not cause discomfort. Salpingitis Inflammation or infection of the Fallopian tube is often associated with PID. Salpingitis causes lower quadrant pain with tenderness of bimanual examination. Pap Training Guideline for Registered Nurses v.2015 - 10 - Microorganism Discharge Erythema/ Itching Neisseria Gonorrhoeae Yellow/green or may be absent; from cervical os Cervix and vulva may be inflamed Chlamydia Trachomatis Most infections are asymptomatic; may have yellow mucopurulent discharge from cervical os; occurs with gonococcal infection, urethritis, mucopurulent cervicitis, and PID Scant to moderate; may be thin but usually thick, white, curdy, adherent Hypertrophic, edematous, friable area of cervical ectopy Candida Albicans Trichomonas Vaginalis Copious, frothy, gray/green; strong foul odor Gardnerella Scant or moderate; (Haemophillus Vaginalis) homogeneous, gray, foul odor Pap Training Guideline for Registered Nurses v.2015 Associated Symptoms Diagnosis Dysuria, frequency; discharge from Skene glands on milking; symptoms of pelvic inflammatory disease (PID) may be present Intermenstrual spotting, spotting after intercourse, asymptomatic urethritis, Bartholin gland discharge Culture Mild to severe itching and erythema of labia, thighs, perineum; cervix may be red and edematous Severe itching of vulva, with or without erythema petechiae of cervix and vagina ("strawberry spots") Dysuria, frequency, dyspareunia Potassium hydroxide (KOH) shows mycelia, spores Dysuria and dyspareunia with severe infection Mild or absent Strong fishy Wet mount shows large numbers of polymorphonucl - ear neutrophils (PMNs) and trichomonads Wet mount show "clue cells" vaginal odor, particularly after intercourse Tissue culture; chlamydia enzyme immunoassay; fluoresceinlabelled monoclonal antibody tests - 11 - SIGNS AND SYMPTOMS OF INFLAMMATORY AND INFECTIOUS CONDITIONS Pelvic Disorders Uterine Prolapse The uterus prolapses as the result of weakening of the supporting structures of the pelvic floor, often occurring concurrently with a cystocele and rectocele. The uterus becomes progressively retroverted and descends into the vaginal canal. In first-degree prolapse the cervix remains within the vagina; in second-degree prolapse the cervix is at the introitus; in third-degree prolapse the cervix and vagina drop outside the introitus. A) Normal uterus B) First degree prolapse C) Second degree prolapse D) Complete prolapse A C Pap Training Guideline for Registered Nurses v.2015 B D - 12 - Cystocele A cystocele is a hernial protrusion of the urinary bladder through the anterior wall of the vagina, sometimes even exiting the introitus. The bulging can be seen and felt as the woman bears down. More severe degrees of cystocele are accompanied by urinary stress incontinence. Rectocele Hernial protrusion of part of the rectum through the posterior wall of the vagina is called rectocele or proctocele. Bulging can be observed and felt as the woman bears down. Pap Training Guideline for Registered Nurses v.2015 - 13 - Health History Adequate and accurate data are keys to a successful health history. It is necessary to be sensitive to culture, language and age related concerns, which if recognized, helps the nurse to understand the patient's responses and behaviour. Sometimes a phrase like "I realize how uncomfortable / embarrassing this is for you, but to help you, I need to know…", encourages the patient to relax and assures her of the essential nature of such confidential information. Terminology and language pose further barriers: be certain of what the patient's statements mean. Repeat statements for verification, when necessary, so that misunderstandings can be corrected. For example, the patient might complain of "itching down there" - use pictures/drawings to identify location or ask patient to point to the area. If language presents a problem, use an interpreter. Because of the confidential nature of the health history questions, a family member might be unsuitable. There are many national, provincial and health system recommendations ensuring language and cultural access to quality health services. You may wish to reflect on the following recommendations for creating a climate that allows for cultural diversity. Acknowledge and explore your own biases, preconceived opinions and possible prejudices. Learn about traditions, culture, and rules of interaction, family and societal roles, health/illness beliefs and practices of the populations you serve. Determine the patient’s preferred language prior to the visit. Arrange for a professional medical interpreter to be present. Learn and use a few basic greetings in your patients’ primary languages as a means of establishing rapport and trust. Use a little small talk initially to establish a personal relationship. Use cross-cultural interview techniques to avoid profiling or stereotyping. Question the patient about beliefs relating to disease causation, treatment, and cure. Don’t ridicule or dismiss these beliefs or any advice or alternative treatment the patient may have been given by a traditional healer. Respect religious or cultural rules prohibiting touch or treatment by a person of the opposite sex. Learn and respect, as much as legally possible, patient health decision-making practices and preferences regarding the disclosure of bad news. Negotiate a treatment plan that is acceptable to the patient’s belief system and lifestyles as well as appropriate medical standards. Pap Training Guideline for Registered Nurses v.2015 - 14 - During the reproductive health history interview: Obtain health history data in a comfortable environment that protects the client's privacy. Conduct the interview at an unhurried pace; otherwise the client may overlook important details. Ideally, the client should remain seated and dressed until the physical assessment. This ensures client comfort and confidence. Always ask sensitive questions and complete the health history before the woman gets on the examination table for her Pap test as lying on the exam table puts her in a vulnerable position. Use terms that the client understands. Explain technical language. Focus questions on the reproductive system, but maintain a holistic approach by inquiring about the status of other body systems and psychosocial concerns. Reproductive system problems may cause the client other problems related to areas such as self-image, sexual functioning, and overall wellness. When choosing health history questions, consider their relevance and practicality for the client. For example, asking an 80 year-old woman the date of her last menstrual period is pointless. Conversely, asking her about menopause, irregular bleeding, and estrogen replacement therapy would be appropriate. Since this procedure is often done during a well-woman examination, questions regarding breast symptoms, health status and self-examination practices are also appropriate. IDENTIFICATION OF HEALTH PROBLEMS: Note: Nurse will usually not be completing a health assessment during a Well Woman's Clinic. However, if a woman does have a concern, it should be acknowledged, and the nurse should recommend assessment by a family practitioner. Pap Training Guideline for Registered Nurses v.2015 - 15 - A. PQRST When assessing a client with a symptom or health concern the nurse uses a symptom analysis to help the client describe the problem fully. A method for obtaining a systematic and thorough assessment, the symptom analysis is easy to remember with the mnemonic device, PQRST. The following questions serve as a guide to effective symptom analysis. P Q R Provocative or Palliative Quality or Quantity Region or Radiation What causes the symptom? What makes it better or worse? How does the symptom feel, look or sound? How much of it are you experiencing now? Where is the symptom located? Does it spread? - First occurrence. What were you doing when you first experienced or noticed the symptom? What seems to trigger it: stress? position? certain activities? arguments? - For a physical symptom such as discharge: What seems to cause it or make it worse? - For a psychological symptom: Does the depression occur when you feel rejected? - Quality. How would you describe the symptom – how it feels, looks or sounds? - Quantity. How much are you experiencing now? Is it so much that it prevents you from performing any activities? Is it more or less than you experienced at any other time? - Region. Where does the symptom occur? - Radiation. In the case of pain, does it travel down your back or arms, up your neck or down your legs? - What relieves the symptom? - What makes the symptom worse? Pap Training Guideline for Registered Nurses v.2015 S T Severity Scale Timing How does the symptom rate on a severity scale of 1 to 10, with 10 being the most extreme? When did the symptom begin? How often does it occur? Is it sudden or gradual? - Severity. How bad is the symptom at its worst? Does it force you to lie down, sit down or slow down? - Course. Does the symptom seem to be getting better, getting worse, or staying about the same? - Onset. On what date did the symptom first occur? What time did it begin? - Type of onset. How did the symptom start: suddenly? gradually? - Frequency. How often do you experience the symptom: hourly? daily? weekly? monthly? When do you usually experience it: during the day? at night? in the early morning? Does it awaken you? Does it occur before, during, or after meals? Does it occur seasonally? - Duration. How long does an episode of the symptom last? - 16 - B. Review of Related History General Considerations 1) Menstrual history a) Age at menarche b) Date of last menstrual period: first day of last cycle c) Number of days in cycle and regularity of cycle d) Character of flow: amount (number of pads or tampons used in 24 hours), duration, presence and size of clots e) Dysmenorrhea: characteristics, duration, frequency (occur with each cycle?), relief measures f) Intermenstrual bleeding or spotting: amount, duration, frequency, timing in relation to phase of cycle g) Intermenstrual pain: severity, duration, timing, association with ovulation h) Premenstrual symptoms: headaches, weight gain, edema, breast tenderness, irritability or mood changes, frequency (occur with every period?), interference with activities of daily living, relief measures 2) Obstetric history a) Gravity (number of pregnancies) b) Parity (number of births); term, preterm c) Number of abortions: spontaneous or induced d) Number of living children e) Complications of pregnancy, delivery, abortion, or with fetus/neonate 3) Douching history a) Frequency: length of time since last douche; number of years douching b) Method c) Solution used d) Reason for douching 4) Cleansing routines: use of sprays, powders, perfume, antiseptic soap, deodorants, or ointments 5) Contraceptive history a) Current method: length of time used, effectiveness, consistency of use, side effects, satisfaction with method b) Previous methods: duration of use for each, side effects, and reasons for discontinuing each Pap Training Guideline for Registered Nurses v.2015 - 17 - Infertility a) Length of time attempting pregnancy, sexual activity pattern, knowledge of fertile period of menstrual cycle b) Abnormalities of vagina, cervix, uterus, Fallopian tubes, ovaries c) Contributing factors: stress, nutrition, chemical substances d) Partner factors 6) Sexual History Difficulties, concerns, problems Satisfaction with current practices, habits, and sexual relationship(s) Number of partners Sexual preference 7) a) b) c) d) 8) Medications: prescription, over-the-counter, illegal 9) Date of last pelvic examination 10) Date of last Papanicolaou (Pap) test and results Present Problem 1) Abnormal bleeding a) Character: shortened interval between periods (less than 19-21 days), lengthened interval between periods (more than 37 days), amenorrhea, prolonged menses (more than 7 days), bleeding between periods b) Change in flow: nature of change, number of pads or tampons used in 24 hours (tampons/pads soaked?), presence of clots c) Temporal sequence: onset, duration, precipitating factors, course since onset d) Associated symptoms: pain, cramping, abdominal distention, pelvic fullness, change in bowel habits, weight loss or gain 2) Pain a) b) c) d) e) f) g) h) Temporal sequence: date and time of onset, sudden versus gradual onset, course since onset, duration, recurrence Character: specific location, type and intensity of pain Associated symptoms: vaginal discharge or bleeding, gastrointestinal symptoms, abdominal distention or tenderness, pelvic fullness Association with menstrual cycle: timing, location, duration, changes Relationship to body functions and activities: voiding, eating, defecation, flatus, exercise, walking up stairs, bending, stretching, sexual activity Aggravating or relief factors Previous medical care for this problem Effectiveness of treatment or medications (prescription or over-the-counter) Pap Training Guideline for Registered Nurses v.2015 - 18 - 3) Vaginal discharge a) Character: amount, color, odor, consistency, changes in characteristics b) Occurrence: acute or chronic c) Medications: birth control pills, antibiotics d) Douching habits e) Clothing habits: use of cotton or ventilated underwear and pantyhose: tight pants or jeans f) Presence of discharge or symptoms in sexual partner g) Associated symptoms: itching, tender, inflamed, or bleeding external tissues; dyspareunia; dysuria or burning on urination; abdominal pain or cramping; pelvic fullness 4) Urinary symptoms: dysuria, burning on urination, frequency, urgency a) Character: acute or chronic; frequency of occurrence; last episode; onset; course since onset; feel like bladder is empty or not after voiding; pain at start, through-out, or at cessation of urination b) Description of urine: color, presence of blood or particles, clear or cloudy c) Associated symptoms: vaginal discharge or bleeding, abdominal pain or cramping, abdominal distention, pelvic fullness, flank pain Past Medical History 1) Recent pregnancies, abortion, or gynecological procedures 2) Past gynecologic procedures or surgery (tubal ligation, hysterectomy, oophorectomy, laparoscopy, cryosurgery, laser therapy, LEEP, conization) 3) Sexually transmitted infections 4) Pelvic inflammatory disease 5) Vaginal infections 6) Diabetes 7) Cancer of reproductive organs Family History 1) Diabetes 2) Cancer of reproductive organs 3) Mother received DES while pregnant with patient 4) Multiple pregnancies 5) Congenital anomalies Older Adults 1) Age at menopause or currently experiencing menopause 2) Menopausal symptoms; menstrual changes, mood changes, tension, back pain, hot flashes 3) Post menopausal bleeding 4) Birth control measures during perimenopause 5) General feelings about menopause: self-image, effect on intimate relationships 6) Mother's experience with menopause 7) Symptoms related to physical changes: itching, urinary symptoms, dyspareunia 8) Changes in sexual desire or behaviour: in self, in partner Pap Training Guideline for Registered Nurses v.2015 - 19 - PHYSICAL EXAMINATION A. External Examination Sit at the end of the examining table and inspect and palpate the external genitalia. Look at the hair distribution and notice the surface characteristics of the mons pubis and labia majora. The skin should be smooth and clean, the hair free of nits or lice. The labia majora may be gaping or closed and appear dry or moist. The labia majora are usually symmetric and may be shrivelled or full. The tissue should feel soft and homogeneous. Labial swelling, redness, or tenderness, particularly if unilateral, may be indicative of a Bartholin gland abscess. Look for excoriation, rashes, or lesions, which suggest an infective or inflammatory process. If any of these signs are present, ask the woman if she has been scratching. Observe for discolouration, varicosities, obvious scratching, or signs of trauma or scarring. Separate the labia majora with the fingers of one hand and inspect the labia minora. Use your other hand to palpate the labia minora between your thumb and second finger. Then separate the labia minora, and inspect and palpate the inside of the labia minora, the clitoris, urethral orifice, vaginal introitus, and perineum. The labia minora should appear symmetric, and the inner surface should be moist and dark pink. Note the fourchette. Hyperaemia of the fourchette may indicate recent sexual activity. The tissue should feel soft and homogeneous, and no tenderness should be present. Look for inflammation, irritation, excoriation, or caking of discharge in the tissue folds, which suggests vaginal infection or poor hygiene. Discoloration or tenderness may be the result of traumatic bruising. Ulcers or vesicles may be symptoms of a sexually transmitted infection. Feel for irregularities or nodules. Inspect the clitoris for size and length. Generally the clitoris is about 2 cm. or less in length and 0.5 cm. in diameter. Enlargement may be a sign of a masculinizing condition. Observe for atrophy, inflammation, or adhesions. The urethral orifice appears as an irregular opening or slit. It may be close to or slightly within the vaginal introitus and is usually in the midline. Inspect for discharge, polyps, caruncles, and fistulas. Signs of irritation, inflammation, or dilation suggests repeated urinary tract infections or insertion of foreign objects. Ask questions about any findings at a later time - not during the pelvic examination when the woman feels most vulnerable. The vaginal introitus can be a thin vertical slit or a large orifice with irregular edges from hymenal remnants (myrtiform caruncles). The tissue should be moist. Look for swelling, discoloration, lesions, fistulas, or fissures. Maintaining separation of the labia, tell the patient that she will feel you pressing around the entrance to the vagina, palpate the lateral tissue between your index finger and thumb. Palpate the entire area, paying particular attention to the posteriolateral portion of the labia majora where the Bartholin glands are located. Note any swelling, tenderness, masses, heat or fluctuation. Observe for discharge from the opening of the Bartholin gland duct. Palpate and Pap Training Guideline for Registered Nurses v.2015 - 20 - observe bilaterally, since each gland is separate. Note the colour, consistency, and odor of discharge, and obtain a specimen for culture. Swelling that is painful, hot to the touch, and fluctuant is indicative of an abscess of the Bartholin gland. The abscess is occasionally gonococcal or staphylococcal in origin and is pus filled. A nontender mass is indicative of a Bartholin's cyst, which is the result of chronic inflammation of the gland. If indicated by the history or inspection, ask the patient to squeeze the vaginal opening around your finger, explaining that you are testing muscle tone. Some nulliparous women can squeeze fairly tightly, some multiparous women less so. Then ask the patient to bear down as you watch for bulging and urinary incontinence. Bulging of the anterior wall and urinary incontinence indicate the presence of a cystocele. Bulging in the posterior wall indicates a rectocele. Uterine prolapse is marked by protrusion of the cervix or uterus on straining. Inspect and palpate the perineum. The perineum surface should be smooth; episiotomy scarring may be evident in women who have borne children. The tissue will feel thick and smooth in the nulliparous women. It will be thinner and rigid in multiparous women. In either case, it should not be tender. Look for inflammation, fistulas, lesions, or growths. The anal surface is more darkly pigmented, and the skin may appear coarse. It should be free of scarring, lesions, inflammation, fissures, lumps, skin tags, or excoriation. If you touch the anus or perianal skin, be sure to change your gloves so that you do not introduce bacteria into the vagina during the internal examination. If indicated, check for urethral discharge. With the labia still separated, examine the Skene glands and Bartholin glands. Tell the woman you are going to insert one finger in her vagina and that she will feel you pressing forward with it. With your palm facing upward, insert the index finger of the examining hand into the vagina as far as the second joint of the finger. Exerting upward pressure, milk the Skene glands by moving the finger outward. Do this to both sides of the urethra, and then directly on the urethra. Look for discharge and note any tenderness. If a discharge occurs, note its color, consistency, and odor, and obtain a culture and smear. Discharge from the Skene glands or urethra usually indicates an infection, most frequently but not necessarily gonococcal. B. Internal Examination Speculum Examination 1. It is essential that you become familiar with how the speculum operates before you begin the examination, so that you do not inadvertently hurt the woman through mishandling of the instrument. Become familiar with both the reusable stainless steel and the disposable plastic specula, because the mechanism of action is somewhat different. 2. Select the appropriate size speculum. Lubricate the speculum with water or a very small amount of water-based lubricant. An advantage of using water as a lubricant is that a cold speculum can be warmed by rinsing in warm (but not hot) water. A speculum can also be warmed by holding it in your hand or under the lamp for a few minutes or by having Pap Training Guideline for Registered Nurses v.2015 - 21 - speculums on a warm heating pad. (Test temperature against wrist before inserting.) A cold speculum increases muscle tenseness. 3. Tell the patient that she is going to feel you touching her again and evaluate the vaginal outlet tone. Now, prepare to use the speculum. First, place the index finger and middle fingers of one hand inside the vaginal introitus to spread it apart about 2.5 cm. (1"). Exert downward pressure with the fingers. Ask the woman to breathe slowly and try to consciously relax her muscles. Wait until you feel the relaxation. With fingers still in place, introduce the closed speculum with the opposite hand. Holding the blades closed with the index and middle fingers of the introducing hand, insert the closed speculum at an oblique angle over your fingers and directed at a 45-degree angle downward. The downward angle matches the anatomic angle of the vagina when the woman is in the lithotomy position. This manoeuvre controls the blades as the speculum is inserted into the vagina and bypasses the sensitive urethra adjacent to the anterior vaginal wall helping to avoid trauma to the urethra and vaginal walls. Make sure not to pinch or pull skin or hair. 4. Once the blades pass the introitus, rotate the speculum to a horizontal plane and remove the fingers, exerting downward pressure. Maintain pressure in a downward posterior manner on the blades until the instrument is completely inserted. Avoid catching pubic hair or pinching labial skin. Pap Training Guideline for Registered Nurses v.2015 - 22 - 5. Open the speculum blades by pressing on the thumb piece. Sweep the speculum slowly upward until the cervix comes into view. Adjust the light source. If you cannot see the cervix, reposition the speculum more anteriorly, posteriorly, or laterally until the complete cervix appears. If the speculum was directed downward on insertion, you are ensured of finding the cervix and avoiding a lot of unnecessary up and down movement of the speculum, which is uncomfortable for the patient. The speculum may however have to be removed, the cervix located digitally, and the speculum reinserted. Tell the client when the speculum will be removed or reinserted. 6. Once the cervix is visualized, manipulate the speculum a little farther into the vagina so that the cervix is well exposed between the anterior and posterior blades. Tighten the thumbscrew on the thumb piece to stabilize the distal spread of the blades. During the speculum repositioning maneuvers, remind the client to relax. The cervix, with a diameter of about 2 to 3 cm. (3/4" to 1 1/4"), projects about 1 to 3 cm. (1/4" to 1 1/4") into the vagina. Projection greater than 3 cm. may indicate a pelvic or uterine mass. The cervix of a woman of childbearing age is usually 2 to 3 cm. in diameter. An enlarged cervix is generally indicative of a cervical infection. The cervix position correlates with the position of the uterus; it should be midline. Deviation to the right or left may indicate a pelvic mass, uterine adhesions, or pregnancy. The cervix will be more posterior with the anteverted or anteflexed uterus and more anterior with the retroverted or retroflexed uterus. (See illustrations page 24.) 7. Inspect the cervix for color, position, size, surface characteristics, discharge, and size and shape of the os. The cervix should be pink, with the color evenly distributed. A bluish color indicates increased vascularity that may be a sign of pregnancy. Symmetric circumscribed erythema around the os is a normal finding that indicates exposed columnar epithelium from the cervical canal. However, beginning practitioners should consider any reddened areas as an abnormal finding, especially if patchy or if the borders are irregular. A pale cervix is associated with anemia. Pap Training Guideline for Registered Nurses v.2015 - 23 - The surface of the cervix should be smooth. Some squamocolumnar epithelium of the cervical canal may be visible as a symmetric reddened area around the os. Nabothian cysts may be observed as small, white or yellow, raised, round areas on the cervix. These are retention cysts of the endocervical glands and are considered to be a normal finding. An infected Nabothian cyst becomes swollen with fluid and distorts the shape of the cervix, giving it an irregular appearance. Look for friable tissue, red patchy areas, granular areas, and white patches that could indicate cervicitis, infection, or carcinoma. Note any discharge. Determine whether the discharge comes from the cervix itself, or whether it is vaginal in origin and has only been deposited in the cervix. Normal discharge is odorless, may be creamy or white, may be thick, thin, or stringy, and is often heavier at midcycle or immediately before menstruation. The discharge of a bacterial or fungal infection will more likely have an odor and will vary in colour from white to yellow, green, or gray. The os of the nulliparous woman is small, round, or oval. The os of a multiparous woman is usually a horizontal slit or may be irregular and stellate. Trauma from induced abortion or difficult removal of intrauterine device may change the shape of the os to a slit. Obtain specimens for Papanicolaou smear, culture, or other laboratory analysis. Varying Positions of the Uterus Anteverted Position Retroverted Position Pap Training Guideline for Registered Nurses v.2015 Anteflexed Position Retroflexed Position - 24 - Midposition of Uterus 8. Obtaining a Papanicolaou Test (a) Conventional Cytology Method (Pap Test): After inspecting the cervix, retrieve a specimen from the ectocervix (the outer layer of the cervix) by scraping the cervix with the bifid end of the spatula. Place the curved end of the spatula in the os, apply pressure while turning it 360 degrees, transfer the scrapings to the slide. (See figures page 33.) Obtain an endocervical specimen by inserting an endocervical brush about 0.5 cm. into the cervical os and rotating the instrument 90-degrees clockwise. Then smear the specimen onto a glass slide with a smooth, rolling motion; too much pressure can destroy the cells. Then quickly spray the slide with cytologic fixative. (See figures page 33.) N.B. A brush is not advised during pregnancy. Please note: Following the use of a collection device (brush, spatula or broom), it is common for the cervix to bleed slightly. Pap Training Guideline for Registered Nurses v.2015 - 25 - If the client has no cervix, as after a complete hysterectomy, scrape the vaginal cuff and obtain a vaginal pool specimen with a cotton-tipped applicator from the posterior vaginal area. If the client has dry mucosa, the applicator tip can be moistened with normal saline solution. Prepare the slide specimen as described previously; label the slide to indicate where the specimen came from. If vaginal wall specimen is needed to evaluate maturation index (estrogen and progesterone influence on the cells), take this specimen by scraping the blunt end of a spatula along the lateral middle third of the vaginal wall. (Note: If the specimen is too thick, it may be inadequate for microscopic examination.) Refer to Screening for Cancer of the Cervix: An Office Manual for Health Professionals for more detail. (b) Liquid Based Cytology Method (Pap Test) 9. Pap Training Guideline for Registered Nurses v.2015 - 26 - After collecting all the specimens, unlock the speculum thumbscrew and begin to withdraw the speculum. As the speculum is withdrawn, the blades will tend to close themselves. Avoid pinching the vaginal mucosa, and maintain downward pressure of the speculum to avoid trauma to the urethra. Slowly rotating the blades in moderately open fashion, inspect the vaginal wall for abnormalities, such as lesions, discharge, swelling, abnormal color, and the presence or absence of rugae. Women with adequate estrogen levels have pink, moist, rugose vaginal walls. The color should be about the same pink as the cervix, or a little lighter. Reddened patches, lesions, or pallor indicates a local or systematic pathologic condition. The surface should be moist, smooth or rugated, and homogeneous. Look for cracks, lesions, bleeding, nodules, and swelling. Normal secretions that may be present are usually thin, clear or cloudy, and odorless. Secretions indicative of infection are often profuse; may be thick, curdy, or frothy; appear gray, green, or yellow; and may have a foul odor. Note the odor of any vaginal discharge that has pooled in the posterior place and obtain a specimen, if you have not already done so. Hook your finger over the anterior blade as it is removed. Close the speculum blades just before the distal ends reach the area adjacent to the urethral meatus and the introitus (to avoid trauma to the area), making sure that no mucosa, skin, or hair remains between the closed blades before withdrawing them. Place the speculum into a soaking solution or discard it if it is disposable. Pap Training Guideline for Registered Nurses v.2015 - 27 - Examining the Woman who has had a Hysterectomy1 Examination of a woman who has had a hysterectomy is essentially no different from the usual procedure. The same examination steps and sequence are followed, with minor variation in what you are assessing. Getting an accurate history before the examination will assist you in knowing what to look for. Determine whether the surgical approach was vaginal or abdominal, whether the woman had a total or subtotal hysterectomy, the reason for the hysterectomy, bladder or bowel changes since the surgery, and the presence of menopausal symptoms. Examine the external genitalia for atrophy, skin changes, decreased resilience, and discharge. In these patients, specimens for gonococci are often taken at the vestibule rather than internally. On speculum examination, the cervix may be absent. In the woman who had a vaginal hysterectomy, the surgical scar (vaginal cuff) will be visible at the end of the vaginal canal and will be an identifiable white or pink suture line in the posterior fornix. A Pap test should be taken from this suture line with the blunt end of the spatula or in the case of liquid-based cytology collection, the Cervex brush. Be sure to label the specimen as vaginal cells, otherwise the report may come back as incomplete or unsatisfactory because of a lack of endocervical cell sample. Assess the walls, mucosa, and secretions as you ordinarily would. The vaginal canal of a woman who has had a total hysterectomy might show the same changes as those that occur with menopause (such as decrease in rugae and secretions), especially if the woman is not receiving hormone replacement therapy. Examine for a cystocele or rectocele. Stress incontinence may be a problem, so observe for this when having the patient bear down. 1 1 Total hysterectomy: removal of the uterus and cervix. Sub-total hysterectomy: removal of the uterus only, leaving the cervix in situ. Partial hysterectomy: a layman’s term, usually used to connotate a hysterectomy (either total or sub-total) with preservation of the ovaries. Pap Training Guideline for Registered Nurses v.2015 - 28 - SECTION 2 - Preceptorship If a Preceptorship is completed, it is recommended that it is arranged with a local expert (physician or nurse) who are competent to perform the particular skill. The following are suggestions for preceptorship: o Observation/participation in a Well Woman Clinic/Pap screening environment. o Theory and practical skills training session with an experienced certified nurse provider or physician presenter o Session in a colposcopy clinic. o Exposure to a range of normal and abnormal appearing cervixes. If a preceptorship is completed, on completion of preceptorship, the learner should be able to: 1. Assemble all required equipment. 2. Label vial with name, health card number and site of specimen. 3. Locate cervix with finger and determined size of speculum. 4. Insert speculum, visualize cervix or vaginal wall. 5. Obtain ecto-cervical specimen using spatula, smear sample onto slide and spray with cytospray. 6. Obtain endocervical specimen using cyto brush, immediately 7. smear sample onto slide and spray with cytospray. 8. Place slide in cardboard holder after Cytospray has completely 9. dried. 10. Complete Pap test requisition and send to lab. For a sample proficiency standards skill checklist to assist with preceptorship training see Appendix B. Pap Training Guideline for Registered Nurses v.2015 - 29 - SECTION 3 - Critical Reflection on Quality All smear takers are encouraged to critically review their practice annually. In addition to reflecting on and reviewing particular cases the Nova Scotia Cervical Cancer Prevention Program provides feedback reports to smear takers on an annual basis. For more information on reports cards and how to receive a report card see Appendix C. Pap Training Guideline for Registered Nurses v.2015 - 30 - SECTION 4 - Practical Tips from Pap Test Providers to support conversations with women about Pap testing 1. When explaining a Pap test to a patient who has never had one before, show them the speculum, spatula and brush instead of telling them about them. Be sure to explain the difference between a Pap test and sexually transmitted infections (STIs) screening. It makes all the difference! 2. Take a breath and relax. 3. Everybody’s body is individual so don’t panic if you can’t find the cervix right away. 4. It is easier to move the speculum around when the patient is relaxed. Slow the process down if you don’t get it right away. Sometimes when you put the speculum in it isn’t in place but once the patient relaxes the speculum falls into place. 5. When examining individuals with multiple sexual partners, always offer to perform STI swabs along with the Pap test. 6. Don’t assume someone isn’t sexually active based on age! 7. It is important to firmly apply the spatula to the cervix when obtaining cells for the slide. Pap Training Guideline for Registered Nurses v.2015 - 31 - Appendix A: Glossary Abortion: Spontaneous or induced termination of pregnancy before the fetus becomes viable (about 20 weeks). Agency: Facility or organization where health services are provided or offered (e.g. regional health authorities, hospitals, community health centres, home care programs, etc.) Anovulation: Lack of ovulation. Anteflexed uterus: Normal position in which the uterine corpus is flexed forward. Breakthrough bleeding: Vaginal spotting or bleeding that occurs between periods and is caused by the failure of progestin (usually taken in combination with estrogen as an oral contraceptive) to support the endometrium adequately. Cervical ectropion: Eversion of the epithelium onto the cervix. Competence: The integration and application of knowledge, attitudes, skills and judgment required for performance in a designated role and setting. Cystocele: Herniation of the bladder through the anterior wall. Dysmenorrhea: Menstrual discomfort or pain. Dyspareunia: Painful or difficult sexual intercourse. Gravida: Number of pregnancies, regardless of their outcomes. Homogenous: Some consistency throughout. Human Papilloma Virus: The most common sexually transmitted infection in the world today. High risk types include types 16 and 18, responsible for 70% of all cervical cancers. Genital warts (condylomata accuminatum) are mostly caused by low risk HPV types 6 and 11. Liquid Based Cytology: A liquid based collection system for the Pap test (LBC). Menarche: Onset of menstrual periods, usually occurring between age 9 and 17. Menopause: Cessation of menstrual periods with the decline of cyclic hormonal production and function usually between the ages of 45 and 60 but may stop earlier in life, for example, as a result of illness or the surgical removal of both ovaries. Pap Training Guideline for Registered Nurses v.2015 - 32 - Glossary (continued) Multigravida: Woman who has been pregnant several times. Multiparity: Condition of having two or more pregnancies that resulted in viable fetuses. Nulliparity: Condition of never having delivered a viable infant. Osteoporosis: Loss of bone density, occurring most frequently in menopausal women. Papanicolaou test (or smear): Cytologic study of cervical cell sample performed most frequently to detect cervical cancer, and premalignant changes. Parity: Condition of having delivered an infant or infants, alive or dead, during the viability period (fetus weighing 500 g. or more or having an estimated 20week gestation): multiple birth is a single parity. Preceptorship: A preceptorship learning experience is a formal, one-to-one relationship between an experienced and competent staff and a novice, for the purpose of assisting the novice to successfully master a new skill. Premenstrual syndrome (PMS): A cyclic cluster of signs and symptoms, such as breast tenderness, fluid retention, and mood swings, usually occurring after ovulation and before or during menses; characterized by at least 7 symptom-free days, usually in the first half of the menstrual cycle. Puberty: Period when secondary sexual characteristics begin to appear and sexual reproductive ability occurs. Rectocele: Herniation of the rectum through the vaginal wall. Retroflexed uterus: Normal position in which the uterine corpus flexes toward the rectum at an acute angle. Retroverted uterus: Normal position in which the uterine corpus flexes toward the rectum, but at a less acute angle than if retroflexed. Shared competence: The identified areas of common ability between registered nurses and physicians to perform activities and provide services. The determination of shared competence is dependent on the context of practice. In general, additional education and experience is required to attain and maintain these competencies. Vaginitis: Inflammation of the vaginal mucosa. Pap Training Guideline for Registered Nurses v.2015 - 33 - Appendix B: Proficiency Standards Skill Checklist Name: Agency: YES NO 1) Assembled all required equipment. _____ _____ 2) Labeled vial with name, health card number and site of specimen. _____ _____ 3) Introduced self and explained procedure to patient. _____ _____ 4) Assisted patient onto examining table, placed feet in stirrups, and applied drape. _____ _____ 5) Washed hands and donned non-sterile gloves. _____ _____ 6) Located cervix with finger and determined size of speculum. _____ _____ 7) Inserted speculum, visualized cervix or vaginal wall. _____ _____ 8) Obtained ecto-cervical specimen using spatula, smeared sample onto slide and sprayed with cytospray. _____ _____ 9) Obtained endocervical specimen using cyto brush, immediately smeared sample onto slide and sprayed with cytospray. _____ _____ 10) Removed speculum. _____ _____ 11) Assisted the patient to sitting position. _____ _____ 12) Placed slide in cardboard holder after Cytospray has completely dried. _____ _____ 13) Completed Pap test requisition and sent to lab. _____ _____ Performed all criteria as described above without prompting. PASS YES _____ NO _____ Date: ___________________Preceptor:_____________________________________ Pap Training Guideline for Registered Nurses v.2015 - 34 - Appendix C: Report Cards/Specimen Adequacy Reports As part of the CCPP’s mandate, the program maintains a provincial registry of Pap smears dating back to 1978. This registry is used to monitor screening activity and provide report cards to healthcare providers that perform Pap tests. Report cards are automatically sent out to physicians who perform Pap tests. The process for obtaining a report is different for Nurse Practitioners, specially trained RNs and midwives, and is also different depending on which lab processes the Pap smears. Therefore follow the instructions below accordingly. If you are a Nurse Practitioner or specially trained RN interested in receiving a report, follow Process A. If you are a midwife interested in receiving a report, follow Process B. Process A: Procedure for Nurse Practitioners and Specially Trained Nurses Performing Paps Processed Outside of QEII Call the CCPP registry at 902-473-7593 or 902-473-2185 to obtain a registry ID number. Provide the following information when applying: Name Whether you are a RN or NP Address where you would like the reports sent If you are an RN, we also need the name of your manager You will be given an ID number to use on your Pap requests forms Print your name and ID number clearly on the cytology request from and also the physician of record. If you do not make it clear on the request form that you were the smear taker, the CCPP may record the physician as the smear taker and this Pap would not be included in your report card If you are an RN you will then receive annual reports with a copy to your manager If you are an NP you will then receive annual reports. Procedure for Specially Trained Nurses Performing Paps processed at the QEII Call the LIS office at 902-473-8408 with your request An LIS Physician Addition/Change form will be sent to you Complete the form and return to the LIS office It is very important to indicate in the changes/comment field that you have been trained to perform Paps and that why you are requesting a number. On average it takes LIS about one week to process this request Once LIS has assigned you a number, you will be contacted with your number Call the CCPP registry at 902-473-7593 or 902-473-2185 with: o Your name o QEII ID number Pap Training Guideline for Registered Nurses v.2015 - 35 - o Address where you would like reports to be sent o Date you were certified to perform Paps o Name and address of your manager Print your name and QEII ID number clearly on the cytology request form and also the physician of record. If yours is the only number/name on the request form, the lab will not process the Pap as a copy of the report must also go to a physician. If you do not make it clear on the request form that you were the smear taker, the CCPP may record the physician as the smear taker and this Pap would not be included in your screening report card. Procedure for Nurse Practitioners Performing Paps processed at the QEII Call the LIS office at 902-473-8408 with your request An LIS Physician addition/change form will be sent to you Complete the form and return to the LIS office On the form, provide the registration number you have been assigned by your college On average it takes LIS about one week to process this request Once LIS has added you to their contact Provider table, they will contact you with your number Call the CCPP registry at 902-473-7593 or 902-473-2185 with: o Your name o QEII ID number o Address where you would like reports to be sent Print your name and QEII ID number clearly on the cytology request form When requesting copies to be sent to another provider, it is important to make it clear on the request form that you were the smear taker; if not, the physician may be recorded as the smear taker and this Pap would not be included in your screening report card You will receive an initial screening report card from the CCPP registry on your first twenty Paps, followed by annual reports Process B: Procedure for Midwives Performing Paps processed outside of the QEII Call the CCPP registry at 902-473-7593 or 902-473-2185 with: o Your name o Address where you would like reports to be sent o Please indicate to the Registry office that you are a Midwife Clearly print your full name on each Pap smear request form and any other identifying information that the lab requires Procedure for Midwives Performing Paps Processed at QEII Follow the process for activation laboratory testing and reporting of results (April 2009) circulated by the Midwifery Regulatory Council of Nova Scotia Call the CCPP registry at 902-473-7593 or 902-473-2185 with: o Your name o QEII ID number o Address where you would like reports to be sent o Please indicate to the registry office that you are a midwife Pap Training Guideline for Registered Nurses v.2015 - 36 - SAMPLE – CCPP – Screening Report Date Range: 2009-JAN-01 to 2009-DEC-31 Age Summary Age Group Pap Interval Class Summary % of Total Count 15-19 5 4.6 20-24 16 14.8 25-29 17 15.7 30-34 22 20.4 35-39 20 18.5 40-44 9 8.3 45-49 10 9.3 50-54 6 5.6 55-59 2 1.9 60-64 1 .9 Total: CURRENTLY UNAVAILABLE 108 Result Summary Diagnosis Count NEGATIVE FOR INTRAEPITHELIAL LESION OR MALIGNANCY LOW GRADE SQUAMOUS INTRAEPITHELIAL LESION (LSIL) % of Total 107 99.1 1 .9 108 Total: Specimen Adequacy Summary Age<=50 % Sat. 100 Age>50 Total Satisfactory For Evaluation Rate: 99 9 Satisfactory For Evaluation: 80 9 Satisfactory For Evaluation But Limited By: Unsatisfactory For Evaluation: 19 0 0 0 % Sat. 100 Satisfactory But Limited By Qualifiers: Breakdown <=50 Breakdown >50 ABSENCE OF TRANSFORMATION ZONE COMPONENTS 8 BLOOD PART. OBSCURING CELL DETAIL 2 INFLAM CELLS PART. OBSC. CELL DETAIL 3 LIMITED CELLULARITY 2 OBSCURED BY BLOOD AND INFLAM CELLS 1 POOR FIXATION OR PRESERVATION 2 POORLY PREPARED/POORLY SPREAD 1 Pap Training Guideline for Registered Nurses v.2015 - 37 - REFERENCES Bellefontaine, Pat. Learning Module for Obtaining a Pap Smear. Queen Elizabeth II Health Sciences Centre Nursing Division, Nursing Clinical Policy & Procedure. April 1997. Medical Nursing Shared Procedures Nursing, Certification of Competence. Vaginal Examination: Pap Smear and Cervical Culture, A Self-Directed Learning Module. Grenfell, Newfoundland. Cervical Cancer Prevention Program, Screening for Cancer of the Cervix: An Office Manual for Health Professionals, 2014, Halifax, Nova Scotia. Registered Nurses' Association of Nova Scotia (1997) Guidelines for Shared Competencies & Delegated Medical Functions. Dartmouth, Nova Scotia. Rose, Joanne. A Women's Wellness Approach Project. Papanicolaou Smear – A Clinic Manual. Stephenville, Newfoundland, 1997. Schneider, Ruth. Cervical Cancer Prevention Program. Needs Assessment Results, May 1998. Video (VHS): How to Perform a Pap Test, 1997, 14 minutes. Medical Audio Visual Communications Inc. Scope of Nursing Practice: Definition, Decision-Making & Delegation. (2006) Association of Registered Nurses of Newfoundland and Labrador (www.arnnl.nf.ca) Guidelines for Delegated Medical Functions and Medical Directives (2005) www.crnns.ca Human Papillomavirus: The most common sexually transmitted infection. Society of Obstetricians and Gynecologists of Canada (2006) http://www.hpvinfo.ca/hpvinfo/pdf/overview_e.pdf Noorani HZ, Brown A, Skidmore B, & Stuart GCE. Liquid-Based Cytology and Human Papillomavirus Testing in Cervical Cancer Screening. Ottawa: Canadian Coordinating Office for Health Technology Assessment; 2003. Technology Report no 40. Clinical Management Guidelines (2007) Cervical Screening Initiatives Program, Newfoundland & Labrador. Gladstone CQ. Screening for Ovarian Cancer. Canadian Task Force on the Periodic Health Examination. Canadian Guide to Clinical Preventive Health Care. Ottawa: Health Canada, 1994; 870-81. Reference: Salimbene, Suzanne, Ten Guidelines for Cultural and Linguistically Appropriate Care. Medscape General Medicine. 2006;8(3) Pap Training Guideline for Registered Nurses v.2015 - 38 -