Failure of Reconstruction of the Anterior Cruciate Ligament Due to
advertisement

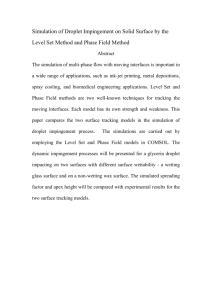
Failure of Reconstruction of the Anterior Cruciate Ligament Due to Impingement by the Intercondylar Roof*† BY MAJOR STEPHEN M. HOWELL‡ MEDICAL CORPS, UNITED STATES AIR FORCE RESERVE, AND CAPTAIN MICHAEL A. TAYLOR§, MEDICAL SERVICE CORPS, UNITED STATES AIR FORCE Investigation performed at the David Grant Medical Center Travis Air Force Base ABSTRACT: The relationship between impingement of the roof of the intercondylar notch on a reconstructed anterior cruciate ligament, and the subsequent stability and range of extension of the joint, was analyzed in fortyseven knees. The extent of the impingement was determined by analysis of the relationship of the tibial tunnel to the intersection of the line of slope of the intercondylar roof with the plane of the subchondral bone of the articular surface of the tibial plateau. These lines were drawn on a lateral roentgenogram that was made with the knee in maximum extension, two years after the operation. In all four knees in which the entire articular opening of the tibial tunnel was anterior to the slope of the intercondylar roof, there was severe impingement on the graft, and all four grafts failed. In the fourteen knees in which a portion of the articular opening of the tibial tunnel was anterior to the slope of the intercondylar roof, there was moderate impingement on the graft, and four grafts failed (an unacceptable rate of failure). There was no impingement in the knees in which the entire articular opening of the tibial tunnel was posterior to the slope of the intercondylar roof, and these knees were associated with the lowest rate of failure of the grafts (three of twenty-nine). Knees that had an impinged graft and regained a complete range of extension became unstable. Results from a biomechanical study suggested that the placement of the tibial tunnel may be important for the clinical success of reconstruction of the anterior cruciate ligament2. A graft that is placed in a tibial tunnel that is anterior to the slope of the intercondylar roof is subject to *One or more of the authors have received or will receive benefits for personal or professional use from a commercial party related directly or indirectly to the subject of this article. In addition, benefits have been or will be directed to a research fund or foundation, educational institution, or other non-profit organization with which one or more of the authors are associated. No funds were received in support of this study. †The views expressed herein are those of the authors and do not reflect the official policy or position of the United States Department of Defense or the United States Government. ‡7601 Timberlake, Suite 103, Sacramento, California 95823. Please address requests for reprints to Dr. Howell. §Department of Orthopedics (SGHT), David Grant Medical Center, Travis Air Force Base, California 94535-5300. 1044 higher tensile and compressive loads than is a graft in a tibial tunnel that is posterior to the slope of the intercondylar roof. Increased loads can occur as the knee nears full extension because of impingement of the intercondylar roof on an anteriorly placed graft. Thus, the clinical result may be related to the placement of the tibial tunnel and the severity of the impingement. Impingement by the roof substantially changes the appearance of an anterior cruciate-ligament graft on a magnetic resonance image,9,11,12,15. There is a predictable increase in the signal intensity of grafts that have been placed anteriorly, apparently because of the impact of the roof on the anterior surface of the graft during extension of the knee,9,11,13-15. Grafts that have been placed in tibial tunnels that are aligned posterior and parallel to the slope of the intercondylar roof retain a low signal intensity12,15. The purpose of this study was to determine the relationship between impingement on the graft by the roof and the stability and range of extension of the knee, and to assess whether there was any association be-tween the slope of the intercondylar roof, the placement of the tibial tunnel, or the range of extension or the stability of the knee two years after the reconstruction. Methods and Materials Selection of Patients Group I comprised twenty-six patients who had been operated on consecutively between December 1986 and December 1987. The senior one of us (S. M. H.) was either the primary surgeon or the first assistant at these operations. An extra-articular reconstruction was in-cluded in the procedure. Three patients were excluded from the study because intraoperative testing for isometry had not been done for them, and four patients were lost to follow-up. Thus, nineteen patients from Group I were included in this study. Group II comprised thirty-eight patients who had been operated on consecutively between March 1989 and March 1990. The senior one of us was the principal surgeon at these operations. For the patients in Group II, the orientation of the tibial tunnel was directed on the basis of an intraoperative roentgenogram, and the intercondylar notch was enlarged to accommodate the volume of the graft when THE JOURNAL OF BONE AND JOINT SURGERY FAILURE OF RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENT DUE TO IMPINGEMENT 1045 FIG. 1-A FIG l-B Figs. 1-A and l-B: A knee in which there was severe impingement on the anterior cruciate-ligament graft. The graft had been placed in a tibial tunnel, the entire width of which was anterior to the point of intersection of the slope of the intercondylar roof with the plane of the articular surface of the tibial plateau. Fig. 1-A: Lateral roentgenogram. Roof impingement was 167 per cent, and the angle of the roof was 36 degrees. f = longitudinal axis of the femur, r = slope of intercondylar roof, and o = plane of tibial plateau. Fig. 1-B: Sagittal magnetic-resonance image (repetition time, 1200 milliseconds; echo time, forty milliseconds). There was a high signal intensity in the graft that was diagnostic of roof impingement. The graft had been angulated and elongated by impingement from the intercondylar roof, but it appeared to be in continuity and was not completely ruptured. the knee was in maximum extension. An extra-articular reconstruction was not done for the patients in Group II. Ten Group-II patients were excluded from the study: eight patients could not return for follow-up, one patient had a chronic rupture of the anterior cruciate ligament in the contralateral knee, and the graft in one patient ruptured when the patient fell from a height of three meters. Thus, twentyeight patients from Group II were included in this study. Lateral roentgenograms of the knee were made at least two years after reconstruction of the anterior cruciate ligament. The roentgenograms were made with the patient supine and the heel on the side of the reconstructed knee elevated on a foam bolster, so that the popliteal fossa was suspended ten centimeters above the table. The patient was instructed to relax the lower limb, to allow gravity to pull the knee into maximum extension. The x-ray beam was directed medially, parallel to the joint line. Roentgenograms were made repeatedly until the lateral projections of the medial and femoral condyles were superimposed (Fig. l-A). Measurements were made from roentgenograms on which the offset of the overlap of the medial and lateral femoral condyles was six millimeters or less (Figs. l-A, 2-A, 3-A, 4-A, and 4-B)12. Impingement by the roof was assessed on the lateral roentgenogram by study of the relationship of the tibial tunnel to the point of intersection of the line of the slope of the intercondylar roof with the plane of the articular sur- VOL. 75-A, NO. 7, JULY 1993 face of the tibial plateau (Figs. l-A, 2-A, 3-A, 4-A, and 4-B). The plane of the tibial plateau was defined by a line between the most superior points of the anterior and posterior margins of the proximal end of the tibia. Impingement was considered to be severe when the posterior border of the superior end of the tibial tunnel (or its extension to the plane of the tibial plateau) was at, or anterior to, the intersection of the line of the slope of the intercondylar roof with the plane of the tibial plateau (Fig. 1-A). Impingement was considered to be moderate when a portion of the tibial tunnel was anterior to this intersection (Figs. 2-A, 4-A, and 4-B). No impingement was considered to be present when the anterior border of the tibial tunnel was at, or posterior to, this intersection (Fig. 3-A). The amount of impingement by the roof was calculated by measurement, on the lateral roentgenogram, of the distance on the line of the tibial plateau from the point where the line of the anterior edge of the tibial tunnel intersected the plateau, to the point where the line of the slope of the intercondylar roof intersected the plateau. This distance was then divided by the width of the tibial tunnel, and the result was expressed as a percentage. A positive ratio was used to indicate impingement and a negative one, no impingement. For example, the percentage of roof impingement was calculated to be 167 per cent in Figure l-A (severe impingement), 25 per cent in Figure 2-A (moderate im-pingement),0 per cent in Figure 3-A (no impinge- 1046 S.M. HOWELL AND M.A. TAYLOR ment), 20 per cent in Figure 4-A (moderate impingement), and 54 per cent in Figure 4-B (moderate impingement). The location of the central axis of the tibial tunnel was calculated by extension of the line of the central axis of the tibial tunnel to its intersection with the line of the tibial plateau: the distance from this intersection to the anterior end of the line of the tibial plateau was then measured. This distance was divided by the length of the line of the tibial teen of the seventeen had an extension deficit of 5 degrees or less. The relationship of the tibial tunnel to the point of intersection of the line of the slope of the intercondylar roof with the plane of the tibial plateau can be expected to be more posterior in a knee that is flexed than in a knee that is fully extended. It is possible that the initial calculation and classification of the severity of the impingement on the graft may have been underestimated in the knees in F IG. 2-A F IG. 2-B Figs. 2-A and 2-B: A knee in which there was moderate impingement on the graft. Fig. 2-A: Lateral roentgenogram. A portion of the tibial tunnel was anterior to the intercondylar roof. There was 25 per cent roof impingement, and the angle of the roof was 39 degrees. Fig. 2.B: Sagittal magnetic-resonance image (repetition time, 1200 milliseconds: echo time, forty milliseconds). A ruptured anterior bundle can be seen. There is no longer impingement on the ruptured bundle because it had been displaced into the anterior chamber of the knee, and it had a low signal intensity, characteristic of a graft on which there is no impingement. The remaining portion of the posterior bundle had a regionalized increase in the magnetic resonance signal, characteristic of impingement on a graft (arrow). (A delayed enlargement of the roof was performed later, and the posterior portion of the graft that appeared to be absent on the magnetic resonance image was found to be intact on probing. The knee remained stable two years after the initial operation.) plateau, and the result was expressed as a percentage15. The slope of the intercondylar roof was measured as the angle subtended by the line of the slope of the roof with the line of the long axis of the femur (Fig. 1-A). Four patients in Group I had severe impingement: thirteen, moderate impingement; and two, no impingement. No patient in Group II had severe impingement, one had moderate impingement, and twenty-seven had no impingement. Effect of Flexion Contracture on Classification of Impingement on the Graft The classification of severe, moderate, or no impingement on the graft was based on the percentage of roof impingement that was determined from the lateral roentgenogram of the maximally extended knee. Seventeen of the reconstructed knees had a flexion contracture, and fif- which there was a flexion contracture. The following analysis was performed to estimate the increase in the severity of impingement that could be expected if a knee in which there was a flexion contracture regained full extension. A lateral roentgenogram, made with the knee in maximum extension, was obtained for four volunteers who had normal knees: a man who was twenty-two years old, and three women who were twenty-two, thirty-six, and fiftytwo years old (Figs. 4-A and 4-B). A foam bolster was then placed posterior to the thigh and was adjusted proximally or distally to create the position of a flexion contracture. Additional roentgenograms were made for each subject, with the knee in 5 and 10 degrees of flexion. The locations of the tibial tunnel that would result in severe, moderate, and no impingement on the graft were represented on each roentgenogram by three nine-millimeter-wide tibial tunnels, drawn centrally at 22, 32, and 42 per cent of the dis- THE JOURNAL OF BONE AND JOINT SURGERY FAILURE OF RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENT DUE TO IMPINGEMENT tance from the anterior to the posterior edge of the tibial plateau. The percentage of roof impingement was calculated and used to determine the increase in the percentage that may result when the knee is moved in 5-degree increments from 10 degrees of flexion to full hyperextension. Operative Technique Group I An arthroscopically assisted reconstruction of the anterior cruciate ligament, with use of double-looped gracilis and semitendinosus autogenous grafts, was performed in 1047 the notch to prevent impingement). Bone was not removed from the roof of the intercondylar notch in these patients. An iliotibial-band extra-articular tenodesis was performed on each patient in Group I, by isolation of a twelvemillimeter-wide strip of the posterior portion of the iliotibial band. The strip was secured to the lateral aspect of the femur near the intermuscular septum with a washer and a 6.0-millimeter cancellous screw (Synthes, Paoli, Pennsylvania). Each patient wore a hinged brace that blocked the last 20 to 30 degrees of extension of the knee for four to six FIG. 3-A FIG. 3-B Figs. 3-A and 3.B: A knee in which there was no impingement on the graft. Fig. 3-A: Lateral roentgenogram. The tibial tunnel was posterior and parallel to the line of the slope of the intercondylar roof. There was no impingement. The angle of the roof was 40 degrees. Fig. 3-B: Sagittal magnetic-resonance image (repetition time, 1200 milliseconds; echo time, forty milliseconds). A low signal intensity confirmed that there was no impingement on this graft. The position of the graft and the dimensions of the notch had been adjusted so that the graft did not touch the intercondylar roof, even though the patient regained extension of the reconstructed knee that was equal to that of the contralateral knee. each knee. To place the tibial pin, the surgeon drilled through a front-entry guide (Acufex Microsurgical, Norwood, Massachusetts), with the knee in 90 degrees of flexion. The tibial landmark for placement of the tip of the guide was five millimeters anterior and medial to the center of the stump of insertion of the anterior cruciate ligament4. Intraoperative testing of the placement of the femoral and tibial pilot holes, which were 2.4 millimeters in diameter, was performed with a transarticular suture and a tensiometer. Maximum excursion of the transarticular suture was three millimeters or less in each knee, and the distance decreased as the knee was flexed. The graft was secured with the knee in 15 to 30 degrees of flexion. Osteophytes were removed from the medial wall of the lateral femoral condyle (the notchplasty that was recommended by Odensten and Gillquist in 1985, whereby bone is removed from the medial wall of the lateral femoral condyle to widen VOL. 75-A, NO. 7, JULY 1993 weeks after the operation. Use of the brace was then discontinued, and full extension was permitted. Group II Thirty-eight consecutive arthroscopically assisted reconstructions of the anterior cruciate ligament were performed with use of double-looped gracilis and semi-tendinosus autogenous grafts. The graft material, the technique for isometric testing, the method of fixation, and the postoperative braces were the same as in Group I, but an extraarticular reconstruction was not performed for Group II. Because of the high proportion of patients in Group I who had roof impingement, an effort was made to avoid this by drilling of the tibial pin so that it was aligned four to five millimeters posterior and parallel to the line of the slope of the intercondylar roof in the maximally extended knee. Intraoperative roentgenograms of the extended knee were 1048 S.M. HOWELL AND M.A. TAYLOR FIG. 4-A F IG. 4-B Figs. 4-A and 4-B: Lateral roentgenograms demonstrating the effect of a change in the extension of the knee on the percentage of roof impingement. Fig. 4-A: Roof impingement was 20 per cent with the knee in 3 degrees of hyperextension. (Clinically, the knee appeared to be in 10 degrees of flexion.) Fig. 4-B: When extension was maximum - increased 10 degrees -roof impingement increased to 54 per cent. made with the tibial guide-pin in place. The trajectory of the tibial guide-pin was changed until the desired alignment was achieved. Bone was resected from the intercondylar roof as well as from the medial wall of the lateral femoral condyle; progressive removal of bone from the intercondylar notch was carried out until a metal rod of the same diameter as that of the tibial tunnel could be advanced through the tibial tunnel and through the notch with the knee in maximum extension (or hyper-extension, if possible)12,15. The amount of bone that was removed varied from patient to patient and was not measured. Collection of Data at the Follow-up Evaluation One or the other of us personally collected all data at least two years after the reconstruction. A goniometer was used to measure the range of passive extension of both knees in each patient. The heel was placed on a bolster to allow gravity to hyperextend the knee. Hyper- extension (recurvatum) beyond 0 degrees was recorded as negative and a flexion contracture, as positive. The difference between the ranges of extension of the two knees, and the absolute point of maximum extension of the reconstructed knee, were determined for statistical analysis. For example, a patient who had 0 degrees of extension in the reconstructed knee and 5 degrees of hyperextension in the normal knee would have a difference in extension between the reconstructed and the normal knees of 5 degrees and an absolute extension of the reconstructed knee of 0 degrees. Stability was determined with the KT-1000 arthrometer (MedMetric. San Diego, California) and the pivot-shift test. The normal knee was tested first, followed by the reconstructed knee. Anterior displacements were recorded to the nearest 0.5 millimeter during application of an eightynine-newton anterior load and a man ual maximum translation. Stability of the knee was quantified by calculation of the difference in anterior translation between the recon- THE JOURNAL OF BONE AND JOINT SURGERY FAILURE OF RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENT DUE TO IMPINGEMENT 1049 TABLE I COMPARISON OF KNEES WITH SEVERE, MODERATE, AND NO IMPINGEMENT ON THE GRAFT Variable Age (yrs.) Time from injury to operation (mos.) Time from operation to follow-up (mos.) Center of tibial tunnel (per cent) Angle of intercondylar roof (degrees) Roof impingement (per cent) Absolute knee extension¶ (degrees) Difference in knee extension compared with normal knee (degrees) Ant. displace. with .89-N load# (mm) Manual maximum translation# (mm) Lysholm score (points) Single-leg-hop test (per cent of normal) Severe Impingement Moderate None Over-All Significance† Severe vs. Moderate‡ Severe vs. Unimpinged‡ Moderate vs. Unimpinged‡ 21 ± 4.0 17 ± 18 23 ± 4.8 16 ± 24 29 ± 6.5 37 ± 57 0.002 0.33 0.80§ 1.0§ 0.04 0.73§ 0.01 0.38§ 24 ± 1 26 ± 6 26 ± 3 0.13 0.29 0.84 0.20 22 ± 4.2 32 ± 4.7 42 ± 2.8 0.0001 0.0001 0.0001 0.0001 34 ± 3.7 35 ± 5.8 37 ± 3.0 0.27 0.93§ 0.46§ 0.43§ 123 ± 14.5 51 ± 15.4 -6 ± 9.4 0.0001 0.0001 0.0001 0.0001 -6 ±2.5 -1 ± 4.2 -4 ±2.5 0.001 0.01 0.49§ 0.005§ 1 ± 2.5 4 ± 3.0 1 ± 1.5 0.0004 0.15§ 0.88§ 0.0004 2.6 ±3 1.5 ± 2.1 0.5 ± 1.3 0.04 0.55§ 0.09§ 0.21§ 4.8 ± 1.0 1.8 ± 2.2 0.7 ± 1.7 0.001 0.03 0.001 0.23§ 88 ± 5 89 ± 3.1 94 ± 5 98 ± 4.7 96 ± 4 97 ± 6.7 0.002 0.060 0.057 0.07§ 0.003 0.09§ 0.26§ 0.90§ *Mean and standard deviation. †Analysis of variance (given as p values). ‡Post hoc test: Scheffé test (given asp values). §Not significant. ¶A negative value indicates extension beyond 0 degrees (recurvatum or hyperextension). #The value represents the measurement for the normal knee subtracted from the measurement for the reconstructed knee. structed and the normal knees with use of the manual maximum-translation test1,5. A knee was defined as stable when there was less than a three-millimeter difference compared with the normal side, as determined with the manual maximum-translation test. The lateral pivot-shift test was per-formed with the patient under anesthesia, before the reconstruction and at the two-year follow-up examina-tion. Lateral pivot shift was classified as absent (Grade O), trace (Grade l), positive (Grade 2), or gross with hang-up during reduction (Grade 3). We attempted to determine the mechanism of fail-ure, and we noted the time after reconstruction when the graft was first noticed to have failed. Laxity meas-urements and a pivot-shift test were performed rou-tinely at three, six, twelve, and twenty-four months after the operation. The satisfaction and the function of the patient were determined with use of the Lysholm scoring scale and the single-leg-hop test17. The one-leg hop for distance was designed to test both the strength of, and the patient’s confidence in, the reconstructed knee22. Statistical Analysis Over-all comparisons between the knees in which there was severe impingement, those with moderate impingement, and those with no impingement were made for con- VOL. 75-A, NO. 7, JULY 1993 tinuous data with use of a single-factor analysis of variance. The Scheffé test was then used to determine differences between the three groups. Ordinal data were analyzed for the three groups with use of the Kruskal-Wallis test, and differences between the groups were determined with the Mann-Whitney test. The chi-square test was used for nominal data. Stability of the knee was defined by the difference in the result of the manual maximum-translation test between the reconstructed and the normal knees. The five variables that were thought to be possible predictors of stability of the knee were absolute knee extension, difference in knee extension compared with the contralateral side, percentage of roof impingement, angle of the intercondylar roof, and location of the center of the tibial tunnel. We inserted all five of these variables into a multiple linear regression analysis and then removed the variable or variables that were not predictive (p > 0.05) of the difference in the result of the manual maximum-translation test between the reconstructed and the normal knees. The variables that remained constituted the best combination of variables that could be used to predict the difference in the result of the manual maximum-translation test between the reconstructed and the normal knees at two years. A one-factor analysis of covariance was used to determine if stability of the knee at the two-year follow-up evaluation was sig- 1050 S.M. HOWELL AND M.A. TAYLOR TABLE II ADDITIONAL COMPARISON OF KNEES WITH SEVERE, MODERATE, AND NO IMPINGEMENT ON THE GRAFT Variable Sex Pivot-shift test under anesthesia¶ Before reconstruction Grade 0 Grade 1 Grade 2 Grade 3 At 2 yrs. Grade 0 Grade 1 Grade 2 Grade 3 IliotibiaI-band tenodesis Severe Impingement Moderate None Severe vs. Moderate‡ Severe vs. Unimpinged‡ Moderate vs. Unimpinged‡ 3 M, 1 F 12M,2F 25 M,4F 0.84‡§ ‡§ ‡§ 0 0 0 4 0 0 7 6 3 3 9 13 0.13‡# ‡# ‡# 0 2 2 0 4 10 3 1 0 13 26 1 2 0 2 0.01# 0.0001# 0.13‡# 0.49‡ 0.0001 0.0001 *Number of knees. †Given as p values. ‡Not significant. &§Chi-square test. ¶Pivot-shift test: Grade 0 = absent. Grade 1 = trace. Grade 2 = positive, and Grade 3 = gross with hang-up during reduction, #Mann-Whitney test. nificantly affected by the presence of an extra-articular reconstruction. Statistical analyses were performed on a personal computer Macintosh IIx; Apple Computer, Cuppertino, California) with use of Statview II and SuperANOVA software packages (Abacus Concepts, Berkeley, California). The alpha level for significance was set at p < 0.05. Results The patients who had no or moderate impingement on the graft were slightly older than the patients who had severe impingement (Table I) (Scheffé test, p = 0.04 and p = 0.01, respectively); however, there was no significant overall difference in the time from the injury to the operation (p = 0.33), the follow-up time-interval (p = 0.13) (Table I), or the pivot-shift grade that had been determined before the reconstruction, with the patient under anesthesia (p = 0.17). There were more men than women in all three study groups (Table II). Roentgenographic Measurements (Table I) The center of the tibial tunnel was significantly more anterior in the knees in which there was severe impingement on the graft compared with those with moderate impingement (p = 0.0001), and the center of the tibial tunnel was significantly more anterior in the knees in which there was moderate impingement compared with the tunnel in the knees with no impingement (p = 0.0001). There was no difference in the slope of the intercondylar roof among the knees in which there was severe, moderate, or no impingement (over-all, p = 0.27). Stability of the Knee The knees with severe impingement were the least stable at the two-year follow-up examination (p = 0.001). A positive pivot-shift test (Grade 1 or greater) was found at two years in all four knees in which there was severe impingement, four of the fourteen knees in which there was moderate impingement, and only three of the twenty-nine knees in which there was no impingement, confirming that knees with roof impingement had an increased prevalence of instability (Table II). Ten of the eleven knees that had a positive pivot-shift test had an anterior displacement of three millimeters or more on manual maximum-translation testing when compared with the normal, contralateral knee. Thus, patients who had a positive pivotshift test also had a difference in the result of the manual maximum-translation test that was diagnostic of poor function of the anterior cruciate-ligament graft. Only three of the reconstructed knees were more stable—as determined by decreased anterior translation on manual maximum— translation testing than the normal knee (Fig. 5). Mechanism and Timing of Failure of the Graft The eleven patients in whom the knee was classified as unstable could not recall a reinjury. We therefore considered the time when the graft had failed to be the time of the follow-up examination when recurrent in-stability was first demonstrated by changes in the measurement of laxity with the KT-1000 device, or by the pivot-shift test. These studies were routinely performed at three, six, and nine months; one year; and at least two years after the operation. All four knees in which there was severe impingement on the graft were unstable by six months after the reconstruction; in contrast, three knees with moderate impingement became unstable more than six months after the operation. Seven of these patients who had recurrent instability of the knee THE JOURNAL OF BONE AND JOINT SURGERY FAILURE OF RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENT DUE TO IMPINGEMENT 1051 FIG. 5 Graph showing the percentage of knees with no, moderate, or severe impingement on the graft, according to the different amounts of anterior translation, as demonstrated by the manual maximum-translation test. The measurement indicates the difference compared with the amount in the contralateral, normal knee. The knees in which there was a difference of at least three millimeters were considered to be unstable. believed that the reconstruction had improved the stability, and all seven had improvement of at least one grade in the postoperative pivot-shift test Extension of the Knee (Table I) The patients who had severe or no impingement on the graft regained the same degree of hyperextension of the knee as each other (p = 0.49) and they regained extension of the knee that was nearly identical to that of the normal side. The patients who had moderate im-pingement on the graft had significantly less extension of the knee than those who had severe impingement (p = 0.01). The patients who had moderate impingement were found to have lost an average of 4 degrees of extension at the two-year follow-up visit when the reconstructed knee was compared with the normal knee. Function of the Knee (Table I) The function of the knees with moderate impinge-ment on the graft could not be distinguished from that of the knees with no impingement by comparison of the subjective analyses with use of the Lysholm scale (p = 0.26) or by FIG.6 Graph comparing the severity of roof impingement with the stability of the knee in the entire series at the two-year follow-up examination. The percentage of roof impingement was weakly predictive of stability of the knee. VOL. 75-A, NO. 7, JULY 1993 1052 S.M. HOWELL AND M.A. TAYLOR comparison of the objective results of the single-leg-hop test (p = 0.90). Regression Analysis of the Whole Group The variable that had the largest value of R2 for prediction of the difference in the manual maximum translation between the reconstructed and the normal knees in the over-all group of knees was the percentage of roof impingement (R2 = 0.20, p = 0.002) (Fig. 6). In order to control for confounding by the inclusion of knees in which an extra-articular augmentation had been done, a one-factor analysis of covariance was done to determine whether the values for instability at the two-year age and the difference in knee extension, were only weakly predictive of stability of the knee in the group as a whole (both R2 < 0.30). Regression Analysis of the Knees with Impingement on the Graft The difference in knee extension was the best single variable for prediction of the stability of the eighteen knees with impingement on the graft (R2 = 0.45, p = 0.001) (Fig. 7). The difference in knee extension, the slope of the intercondylar roof, and the location of the center of the tibial tunnel was the best combination of the five variables for the prediction of stability of the knees with impingement FIG. 7 Graph comparing the difference with respect to extension between the reconstructed and the normal, contralateral knees with the difference with respect to anterior tibial translation, as measured with the manual maximum-translation test. Only the eighteen knees with severe or moderate impingement on the graft are included. (Two knees that had moderate impingement had identical data and are represented by one data point.) Knees with impingement on the graft and a flexion contracture had the smallest difference in anterior tibial translation compared with the contralateral knee and were more likely to remain stable; knees with impingement on the graft and extension that was equal to the contralateral side were more likely to become unstable. follow-up examination were significantly affected by the variable of extra-articular tenodesis; they were not (p = 0.54). The covariate of the percentage of roof impingement was therefore a predictor of stability of the knee at two years (R2 = 0.21, p = 0.007). The best combination of variables for the prediction of stability of the knee was the percentage of roof impingement and the difference in knee extension (combined R2 = 0.29, p = 0.0003). Reconstructed knees were more likely to become unstable when there was impingement on the graft and extension of the knee equal to that of the normal knee was regained. Reconstructed knees were more likely to remain stable when there was less impingement on the graft and the knee had a persistent flexion contracture at the same time. It should be pointed out. however, that the percentage of roof impingement, and the combination of this percent- on the graft (R2 = 0.70, p = 0.001). Knees were thus more likely to be unstable when they had a combination of these factors: extension that approached that of the normal knee, a more vertical slope of the intercondylar roof, and a more anterior tibial tunnel. Knees were more likely still to be stable at the two-year follow-up examination if they had a combination of a flexion contracture, a more horizontal slope to the intercondylar roof, and a more posterior tibial tunnel. The difference in knee extension, and the combination of the three variables, were moderately to strongly predictive of stability of the knees with roof impingement (R2 = 0.45 to 0.70). Regression Analysis of the Knees with No Impingement on the Graft Absolute knee extension, the difference in knee ex tension, the percentage of roof impingement, the angle of the THE JOURNAL OF BONE AND JOINT SURGERY FAILURE OF RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENT DUE TO IMPINGEMENT intercondylar roof, and the location of the center of the tibial tunnel were not predictive of stability in the twentynine knees with no impingement on the graft (R2 = 0.01, p = 0.50). The statistical analysis did not determine the possible causes for failure of the graft in the knees without impingement. Effect of Flexion Contracture on Classification of Impingement on the Graft It was estimated, from the roentgenograms of the normal knees, that a reconstructed knee with a 5-degree flexion contracture may show an increase in the amount of impingement of 16 ± 3.7 per cent (mean and standard deviation) if full extension were regained. A knee with a 10-degree flexion contracture could have a 30 ± 4.2 per cent increase in the amount of impingement with resolution of the contracture (Figs. 4-A and 4-B). Therefore, the amount of roof impingement can be roughly estimated to increase about 3 per cent for each degree of flexion contracture within this range. On the basis of this conversion factor, no knee in which the impingement had been originally classified as severe or moderate would have been reassigned to a different group had it not had a flexion contracture. Only two of the twenty-nine knees in which the impingement had been originally classified as absent had a flexion contracture of 5 degrees, and one might conjecture that these knees would have been reassigned to the moderate-impingement group if full extension had been regained. However, in that event, the impingement in these two knees would have been only 15 per cent, which is more than two standard deviations below the mean percentage of impingement in the moderate-impingement group. It thus seems unlikely that any underestimation of the extent of roof impingement caused by a flexion contracture altered the conclusions of the study. Discussion The diagnosis of impingement by the roof of the intercondylar notch on an anterior cruciate-ligament graft can be made from a lateral roentgenogram of the fully extended knee at least two years after the operation. Roof impingement is present when the anterior border of the tibial tunnel is anterior to the slope of the intercondylar roof. The appearance of the graft on a magnetic resonance image can be used to confirm this diagnosis9-12,15. Stability of the knee was significantly affected by roof impingement. Knees in which there was severe impingement on the graft uniformly failed; knees with moderate impingement and those with no impingement were more likely to remain stable. From December 1986 to December 1987, we used an extra-articular reconstruction because, at that time, it was thought to improve stability of the knee by protecting an intra-articular reconstruction early in the postop-erative VOL. 75-A, NO. 7, JULY 1993 1053 period3. As early as six to twelve weeks after the graft had been implanted, serial magnetic-resonance images of the hamstring and patella-patellar ligament-bone autogenous grafts revealed that the extra-articular reconstruction did not prevent roof impingement on the graft, as demonstrated by an increase in the magnetic resonance signal in the graft12,13,15. These observations suggested that avoidance of roof impingement by correct placement of the tibial tunnel may be more important in the protection of the graft than the addition of an extra-articular reconstruction. We changed the location of the tibial tunnel and eliminated the extraarticular reconstruction in the thirty-eight patients in Group II who were operated on between March 1989 and March 1990. The knees with no impingement on the graft and no extra-articular re-construction had significantly better stability than the knees with roof impingement and an extraarticular re-construction. Our observations are in agreement with those of O’Brien et al., who also concluded that an extra-articular reconstruction did not improve stability of the knee. Laxity tests with the use of instrumentation and pivotshift tests both documented instability effectively. Ten of the eleven knees with a positive pivot-shift test had at least three millimeters of anterior displacement, as demonstrated by the manual maximum-translation test, when compared with the normal, contralateral knee. We consider a reconstruction of the anterior cruciate ligament to be stable objectively only after a manual maximum-translation test has demonstrated that the difference compared with the contralateral side is less than three millimeters. We believe that the grafts on which the roof im-pinged were forced to elongate gradually, rather than failing structurally, by the tendency of the reconstructed knee to reach the same point in extension as the contra-lateral knee. There is strong evidence that the grafts on which the roof impinged did not come apart, because the results of the pivot-shift test at the two-year follow-up examination were better than the preoperative results (p = 0.001). Most of the grafts on which the roof impinged were shown to be elongated and not completely ruptured on magnetic resonanceimaging studies (Figs. l-B, 2-B, and 3-B)9-14. Arthroscopic evaluation of grafts with roof impingement has shown that some anterior fibers rupture, resulting in fibrous nodules or so-called Cyclops formation, but the more posterior fibers remain in continuity9,16,18. A review of the mechanism and timing of the onset of instability in our series also reinforced the supposition that gradual elongation of the graft may have caused the recurrent instability. No patient recalled a traumatic reinjury. The instability of all four of the knees with severe impingement on the graft had developed insidiously by six months, and three of the knees with moderate impingement became unstable later, between six and forty months after the operation. 1054 S.M. HOWELL AND M.A. TAYLOR The knees that had impingement on the graft as well as a flexion contracture were still stable at the two-year follow-up examination. It is tempting to postulate that the flexion contracture protected the graft, but, to our knowledge, there is no reported evidence to support this association. On the contrary, an increase in the magnetic resonance signal in anterior cruciate-ligament grafts, which is pathognomonic of impingement by the roof and suggestive of weakening of the graft, is common in stable reconstructed knees with a flexion contracture9, 11,12,15. These studies have shown that the intercondylar roof directly impinges on the graft when the knee is in flexion. In our opinion, a postoperative flexion contracture is not a healthy sign that suggests that the graft is protected, but is instead an ominous sign that the graft is at risk. The delayed onset of instability between six and forty months after the reconstruction in the three knees with moderate impingement on the graft supports this view. We believe that the patients who had moderate impingement on the graft had less extension of the reconstructed knee than those who had severe impingement because some of the grafts on which there was moderate impingement were able to resist elongation. The im-proved stability in the knees with moderate impingement compared with that in the knees with severe impingement supports this observation. The more posterior position of the tibial tunnel in the knees with moderate impingement probably protected the integrity of the graft, because graft-roof contact occurs near terminal knee extension, when the tibial tunnel is moved posteriorly2. In contrast, in knees in which there was severe impingement on the graft, contact between the graft and the roof occurred at 10 to 15 degrees of flexion2, and this contact was associated with an increased occurrence of elongation of the graft. It was once believed that loss of extension was desirable to help to eliminate pivot shift18. It is now recognized that extension deficits are disabling and troublesome to the patient6,16,18,22 We believe that the position of the anterior cruciateligament graft should be such that the patient can regain extension of the reconstructed knee equal to that of the contralateral knee, without the graft touching the inter-condylar roof. This principle led to the operative tech-nique used for Group II in this study. The knees without impingement in this group regained extension equal to that of the contralateral knee while remaining the most stable. Our method to avoid impingement by the roof requires individualized placement of the tibial tunnel. To avoid late impingement by the roof caused by reconstruction of a knee with a flexion contracture, we prefer to delay the operation on a recently injured knee until extension that is equal to that of the contralateral side has been regained. In order to account for individual variations in the point of maximum extension and in the slope of the intercondylar roof, an eight to tenmillimeter- diameter tibial tunnel should be aligned four to five millimeters posterior and parallel to the slope of the intercondylar roof in the maximally extended knee. Bone should be progressively removed from the inter-condylar notch until a metal rod of the same diameter as the tibial tunnel can be advanced into the notch through the tibial tunnel, with the knee in maximum extension10,12,15. The adequacy of the space in the intercondylar notch can be confirmed before the graft is implanted. This technique is reproducible, and roof impingement was avoided in 96 per cent of the reconstructions that were treated with the method in this study. The technique has also prevented increases in the magnetic resonance signal that is seen in grafts on which there is impingement10,12,15. Roof impingement is not the only cause of failure of a graft. Three knees in which there was no impingement failed, and a cause was not identified. Factors such as the fixation of the graft, the rehabilitation technique, the activity level of the patient, and other unidentified variables may have played a role in these failures. Some failures can be caused by non-isometric placement of the graft. Studies have shown that the location of the femoral tunnel must be controlled to avoid exces-sive loads on the graft 7,8,21,24 In all knees in this study, however, the intra-articular distance between the femoral and the tibial holes for the graft was measured with the use of a tensiometer attached to a transarticular suture that had been threaded through 2.4-millimeter pilot holes in the femur and tibia. Excursion profiles were three millimeters or less from 0 to 90 degrees of flexion for both the knees with and those without impingement on the graft. It seems unlikely that placement of the femoral tunnel contributed to failure of a graft since the criteria for the location of the femoral tunnel were similar for all of the knees in the study. The relatively posterior tibial tunnel used in this study did not violate the principle of isometric placement of a graft11. NOTE: The authors Thank Goeff Patrissi, M.A.,for his review and assistance the statistical analysis of the data, and Brian Galinat, M.D., and Steven Barad, M.D.. for their review of the manuscript. References 1. Bach, B. R., Jr.; Warren, R. F.; Flynn, W. M.; Kroll, M.; and Wickiewiecz, T. L.: Arthrometric evaluation of knees that have a torn anterior cruciate ligament. J Bone and Joint Surg., 72-A: 1299-1306, Oct. 1990. 2. Berns, G. S., and Howell, S. M.: Roofplasty requirements in vitro for different tibial hole placements in anterior cruciate ligament reconstructions. Am. J Sports Med., 21: 292-298,1993. 3. Carson, W. G., Jr.: Extra-articular reconstruction of the anterior cruciate ligament: lateral procedures. Orthop. Clin. North America, 16: 191-211.1985. THE JOURNAL OF BONE AND JOINT SURGERY FAILURE OF RECONSTRUCTION OF THE ANTERIOR CRUCIATE LIGAMENT DUE TO IMPINGEMENT 1055 4. Clancy, W, G., Jr.; Nelson, D. A.; Reider, B.; and Narechania, R. G.: Anterior cruciate ligament reconstruction using one-third of the patellar ligament, augmented by extra-articular tendon transfers. J Bone and Joint Surg, 64-A: 352-359, March 1982. 5. Daniel, D. M.; Malcolm, L. L.; Losse, G.; Stone, M. L.; Sachs, R.; and Burks, R.: Instrumented measurement of anterior laxity of the knee. J. Bone and Joint Surg., 67-A: 720-126,June 1985. 6. Fullerton, L. R., Jr., and Andrews, J. R.: Mechanical block to extension following augmentation of the anterior cruciate ligament. A case report. Am. J. Sports Med., 12: 166-168,1984. 7. Fuss, F. K.: Optimal replacement of the cruciate ligaments from the functional-anatomical point of view. Acta Anat., 140: 260-268,199l. 8. Hefty, M. S.; Grood, E. S; and Noyes, F. R.: Factors affecting the region of most isometric femoral attachments. Part II: the anterior cruciate ligament. Am. J Sports Med., 17: 208-216,1989. 9. Howell, S. M.: Arthroscopic roofplasty: a method for correcting an extension deficit caused by roof impingement of an anterior cruciate ligament graft. Arthroscopy, 8: 375-379,1992. 10. Howell, S. M.: The Cruciate Ligaments, edited by J. Feagin. Philadelphia, Lea and Febiger, 1993. 11. Howell, S. M., and Clark, J. A.: Tibial tunnel placement in anterior cruciate ligament reconstructions and graft impingement. Clin. Orthop., 283: 187-195,1992. 12. Howell, S. M.; Berns, G. S.; and Farley, T. E.: Unimpinged and impinged anterior cruciate ligament grafts: MR signal intensity measurements. Radiology, 179: 639.643,199l. 13. Howell, S. M.; Clark, J. A.; and Blasier, R. D.: Serial magnetic resonance imaging of hamstring anterior cruciate ligament autografts during the first year of implantation. A preliminary study. Am. J. Sports Med., 19: 42-47,199l. 14. Howell, S. M.; Clark, J. A.; and Farley, T. E.: A rationale for predicting anterior cruciate graft impingement by the intercondylar roof. A magnetic resonance imaging study. Am. J. Sports Med., 19: 276-282.1991. 15. Howell, S. M.; Clark, J. A.; and Farley, T. E.: Serial magnetic resonance study assessing the effects of impingement on the MR image of the patellar tendon graft. Arthroscopy, 8: 350-358,1992. 16. Jackson, D. W., and Schaefer, R. K.: Cyclops syndrome: loss of extension following intra-articular anterior cruciate ligament reconstruction. Arthroscopy, 6: 171-178,1990. 17. Lysholm, J., and Gillquist, J.: Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sports Med., 10: 150-154,1982. 18. Marzo, J. M.; Bowen, M. K.; Warren, R. E; Wickiewicz, T. L.; and Altchek, D. W.: Intraarticular fibrous nodule as a cause of loss of extension following anterior cruciate ligament reconstruction. Arthroscopy, 8: 10-18,1992. 19. O’Brien, S. J.; Warren, R. F.; Pavlov, H.; Panariello, R.; and Wickieticz, T. L.: Reconstruction of the chronically insufficient anterior cruciate ligament with the central third of the patellar ligament. J Bone and Joint Surg., 73-A: 278-286, Feb. 1991. 20. Odensten, M., and Gillquist, J.: Functional anatomy of the anterior cruciate ligament and a rationale for reconstruction. J Bone and Joint Surg., 67-A: 257-262, Feb. 1985. 21. Penner, D. A.; Daniel, D. M.; Wood, P.; and Mishra, D.: An in vitro study of anterior cruciate graft placement and isometry. Am. J Sports Med., 16: 238-243,1988. 22. Sachs, R. A.; Daniel, D. M.; Stone, M. L.; and Garfein, R. F.: Patellofemoral problems after anterior cruciate ligament reconstruction. Am. J. Sports Med., 17: 760-765,1989. 23. Scheffé, H.: The Analysis of Variance. New York, Wiley, 1959. 24. Sidles, J. A.; Larson, R. V.; Garbini, J. B. Downey, D. J.; and Matsen, F. A., III: Ligament length relationships in the moving knee. J. Orthop. Res, 6: 593-610,1988. VOL. 75-A, NO. 7, JULY 1993