ARTICLE IN PRESS
+
MODEL
Journal of Plastic, Reconstructive & Aesthetic Surgery (2008) xx, 1e7
The surgical repair of half-nose
Renato da Silva Freitas a,b,*, Nivaldo Alonso c, Thais de Freitas Azzolini b,
Luciano Busato a, André Ricardo Dall’Oglio Tolazzi b,
Gilvani Azor de Oliveira e Cruz b, Dov Goldenberg c
a
Assistance Center for Cleft Lip and Palate (CAIF), Curitiba-PR, Brazil
Division of Plastic and Reconstructive Surgery of Federal University of Parana, Curitiba-PR, Brazil
c
Division of Plastic and Reconstructive Surgery of Sao Paulo University, Sao Paulo-SP, Brazil
b
Received 3 January 2008; accepted 31 August 2008
KEYWORDS
Half-nose;
Heminasal aplasia;
Nasal reconstruction;
Nose;
Facial cleft
Summary Absence of half-nose is an extremely rare congenital malformation, which has
a devastating impact on the patient and the family. A review of indexed English-language literature found 91 cases of half-nose, including 50 patients with proboscis lateralis. Pathogenesis
is not clear, and the reported cases have sporadically occurred. Many aspects must be considered when reconstructing a congenital half-nose, such as timing of surgery, type of tissue to be
used and the need to reconstruct nasal airway. The aim of this article is to present personal
experience in seven cases of half-nose reconstruction, in order to review the literature
regarding to this rare entity, highlighting aspects of incidence, pathogenesis and surgical treatment. Nasal reconstruction was performed at ages of 5e7 years to minimise psychological
trauma. Forehead skin demonstrated to be an excellent donor site to re-surface the nose.
For the inner lining, contralateral cutaneous nasal flap was our preference. Concerning the
nasal framework reconstruction, alar contour was restored using a cartilage graft from the
lower portion of ear tragus and concha.
ª 2008 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published by
Elsevier Ltd. All rights reserved.
Absence of half-nose is an extremely rare congenital malformation, which has a devastating impact on the patient
and the family.1e5 Cleft nose, proboscis lateralis and nasal
agenesis are rare; whereas absence of half-nose is also
extremely rare.6 A review of indexed English-language
* Corresponding author. Address: R. 25 de Janeiro, 2460, Condominio
Anhangava (casa 23), Quatro Barras, Parana 83420-000, Brazil.
E-mail address: dr.renato.freitas@gmail.com (R. da Silva Freitas).
literature found 91 cases of half-nose e 50 of them with
proboscis lateralis.7e30 There were 31 males and 21 females
(39 cases were not defined). With regards to laterality, 37
cases were on the right side and 30 cases on the left side.
Twenty cases had isolated half-nose, without other associated anomalies, while 22 had eye and lacrimal system
malformations; 22 had orbital malformations, which were
associated with cleft lip and palate in nine patients; three
other cases presented isolated cleft lip and/or palate and
other unusual anomalies such as craniosynostosis,
1748-6815/$ - see front matter ª 2008 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.bjps.2008.08.040
Please cite this article in press as: da Silva Freitas R et al., The surgical repair of half-nose, J Plast Reconstr Aesthet Surg (2008),
doi:10.1016/j.bjps.2008.08.040
ARTICLE IN PRESS
+
MODEL
2
R. da Silva Freitas et al.
teratoma, encephalocoele and microtia. Reports of 22
cases did not mention associated deformities.
Pathogenesis is not clear, and the reported cases in the
literature have occurred sporadically. It has been suggested
that lack of nasal development probably results from
growth failure of medial and lateral nasal processes. Mazzola6 classified craniofacial malformations according to the
area of commitment: upper face, midcephalic borderline
and lower lateral region of the face. Nasal aplasia belongs
to the first group and may be subdivided into three
subgroups: arhinia, half-nose and half-nose with proboscis
lateralis.31,32 Any congenital anomaly of the nose can also
be accompanied by other facial and palatal anomalies.33 In
1993, Nicolaides et al. detected chromosomal abnormalities in 32% of cases with nasal hypoplasia, proboscis lateralis or single nostril.32
Nasal development starts in the third week of gestation
when the primordial structure first appears. Olfactory placode is the primary organiser of developing nose and is
responsible for olfactory nerves formation.12 Nasal placodes become apparent in the fourth week of intrauterine
life. These placodes soon sink below the surface to create
nasal pits, which subsequently form the nostrils. Medial and
lateral raised edges of the pits are called medial and lateral
nasal placodes, respectively. Nasal alae are formed by
fusion of lateral and medial nasal processes.34 Mesoderm
becomes heaped up in the median plane to form nasal
prominence. By means of evagination, placodes form nasal
pits, which are widely spaced on anterolateral area of
developing head. Nasal cavities are formed by extension of
nasal pits.16 Maxillary and lateral processes fuse to form the
nostrils. Defective development of the lateral nasal process
can result in alar rim anomaly.35 Medial nasal processes fuse
with each other, thereby forming the ridge, tip and columella of the nose, as well as the philtrum and medial part
of the upper lip. Fusing with maxillary processes, medial
nasal processes separate nasal cavities and mouth.
Table 1
Heminasal aplasia with or without proboscis lateralis seems
to be the result of one group of developmental disorders.16
Absence of nasal placodes probably leads to heminasal
aplasia. Nasal lacrimal system develops into the nasal
maxillary groove, but in half-nose cases it would be blind.
During facial development, maxilla generally has a growth
deficiency in both sagital and vertical dimensions. Malocclusion can be explained by growth arrest of nasomaxillary
complex.9
In 1976, Tessier36 postulated that it could be one of the
possible presentations of facial cleft no. 2, while OrtizMonasterio,27 in a large series of facial clefts, reported only
five cases of half-nose and classified this malformation as
a facial cleft no. 3. Other authors believe it is just a nasal
displasia.6,31 The aim of this article is to present personal
experience in half-nose reconstruction and review the
literature with regards to this rare entity, highlighting
aspects of incidence, pathogenesis and surgical treatment.
Clinical cases
Seven sporadic cases have been treated in our institutions.
Patients presented with different forms of commitment
(Table 1), and consequently, individualised surgical techniques have been used for nasal reconstruction.
Surgical technique
Half-nose reconstructions have been complex and multistaged. Our standard technique of reconstruction consisted
of three-stage procedures. First stage was usually performed between 4 and 6 years of age (Figure 1A). A foil
template of normal heminose was drawn and transferred to
the hypoplastic side. Distance from the midpoint of columellar base to alar base was determined in normal side and
transferred to affected side. Based on these marks, width
Epidemiological data and clinical findings of 7 cases with half-nose
Case
Agea
Gender
Side
PLb
Craniofacial malformations
Other findings
1
6y
Male
Left
No
Polycystic kidney;
Hidden bifid spine (C2, C3C4);
Interatrial communication
2
5y
Male
Right
No
3
9y
Male
Right
No
4
15 y
Female
Left
No
5
6
19 y
23 y
Male
Female
Left
Right
No
No
7
15
Female
Right
No
a
b
Hypertelorism;
Lateral and inferior orbital displacement;
Cleft orbital floor;
Lachrymal obstruction
Right hemifacial microsomia
Median cleft lip
Absence of lachrymal duct
Nasoethmoidal encephalocele
Microphtalmus
Nystagmus
Absence of lachrymal duct
Anophtalmus
Cleft lip and palate
Anophtalmus
Microphtalmus
Right cleft lip
Hypertelorism;
Lateral and inferior orbital displacement;
Lachrymal obstruction
Epispadia
No
No
No
No
No
Age of patient at the moment of first-stage surgical reconstruction.
PL: Proboscis lateralis.
Please cite this article in press as: da Silva Freitas R et al., The surgical repair of half-nose, J Plast Reconstr Aesthet Surg (2008),
doi:10.1016/j.bjps.2008.08.040
ARTICLE IN PRESS
+
The surgical repair of half-nose
MODEL
3
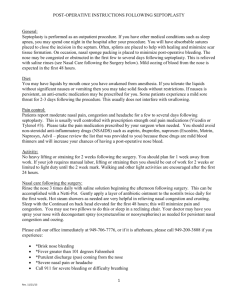
Figure 1
Patient 1. A. Preoperative frontal view. B. Schematic drawing of the nasal skin and forehead flaps. C. Incision of the
nasal flap to the inner lining. D. Flap rotation to the contralateral side. E. Silicone catheter through the nasal hole. F. Forehead flap
undermining. G. Final result.
Please cite this article in press as: da Silva Freitas R et al., The surgical repair of half-nose, J Plast Reconstr Aesthet Surg (2008),
doi:10.1016/j.bjps.2008.08.040
ARTICLE IN PRESS
+
MODEL
4
R. da Silva Freitas et al.
and length of a forehead flap was determined (Figure 1B
and C). For patients without any nasal cavity, anterior
piriform aperture was drilled out and an inferiorly based
local skin flap was rotated to line internal nostril (Figure 1D
and E). A silicone stent was used in the reconstructed
nostril and pyriform aperture for at least 6 months. A
cartilage graft from the lower portion of ear tragus and
concha was used to provide nasal-tip support. A forehead
flap was harvested, including frontalis muscle, along
a cleavage plane, superficial to the periosteum (Figure 1F).
At eyebrows level, a careful blunt dissection was performed
to preserve the suprathroclear vessels. The flap was rotated
180 to cover the whole external defect of the nose
(Figure 1G). Three weeks later, its pedicle was trimmed.
Third-stage refinements consisted of flap thinning and
nostril aperture revision.
In two cases we have used different approaches to nasal
reconstruction. In case 2, we opted to reconstruct only the
affected side using local mucosal and forehead flap
(Figure 2). In case 6, we performed a forehead expansion
prior to harvest of the frontal flap. Both of them did not
Figure 2
demonstrate any advantage over our standard approach
(Figures 3 and 4).
Discussion
We have classified half-nose malformation as a Tessier
facial cleft no. 2, due the absence of lower eyelid coloboma, medial canthus dystopia, lacrimal obstruction and
hypertelorism. The affected nose may be hypoplastic or
completely absent, and some cases may present unilateral
proboscis or a tissue tag.33 In our series, four patients were
male, and three female; four on the right side and three on
the left; proboscis lateralis was not present and five cases
of a non-functional eye globus were noted. Three of our
cases had hypoplastic maxilla with class III malocclusion.
Many aspects must be considered when reconstructing
a congenital half-nose, such as timing of surgery, tissues
available to reconstruct the defect and the necessity to
create an internal nasal passage.17,37,38 The most appropriate age to operate on the patients, and if nasal
Patient 2. A. Preoperative frontal view. B. Preoperative lateral view. C. Final result. D. Postoperative lateral view.
Please cite this article in press as: da Silva Freitas R et al., The surgical repair of half-nose, J Plast Reconstr Aesthet Surg (2008),
doi:10.1016/j.bjps.2008.08.040
ARTICLE IN PRESS
+
MODEL
The surgical repair of half-nose
Figure 3
5
Patient 3. A. Preoperative frontal view. B. Final result.
reconstruction will be definitive remains unanswered.
Management of psychological aspects is very important in
paediatric patients with nasal malformations. By about 5
years of age, children become self-conscious and develop
self-image and self-esteem. Some surgeons have suggested
reconstructing the nose at ages of 5e7 years in order to
minimise psychological trauma.6 Guided by social and
psychological reasons, we believe this age is the most
appropriate moment to reconstruct the nose and avoid or
minimise psychological problems. Two cases of this series
arrived in early age, and we followed this protocol.
The goals of total nasal reconstruction include restoration of aesthetic and functional aspects, which remains
a challenge for plastic surgeons. Basically, full-thickness
nasal defects require reconstruction of the inner lining,
internal support and external coverage.39 Burget and
Menick40 have proposed nine subunits for nasal repair,
while Giugliano41 divided the nose into three main areas:
Figure 4
tip, dorsum and ala. All these units and subunits should be
considered when reconstruction half-nose defects. There
are few adequate options to reconstruct external coverage
of the nose, including local flaps, forehead flaps, forearm
free flaps and also tissues of the proboscis lateralis. We
believe when proboscis lateralis is present, it is very useful
for external nasal reconstruction as the skin colour and
texture is more similar. When proboscis lateralis is absent
or insufficient, forehead skin is an excellent donor site to
re-surface the nose.
Majority of the articles using forehead flaps concern
adults. There are few reports mentioning its use in paediatric patients and usually with short-term follow-up.41 We
agree with Giugliano et al. that have used tissue expansion
only for cases with large nasal defect and proportionally
small donor site. Forehead expansion creates a large
capsule, which can contract in postoperative period,
leading to a short nose on long-term result. The pedicle
Patient 4. Preoperative frontal view.
Please cite this article in press as: da Silva Freitas R et al., The surgical repair of half-nose, J Plast Reconstr Aesthet Surg (2008),
doi:10.1016/j.bjps.2008.08.040
ARTICLE IN PRESS
+
MODEL
6
may be designed contralateral or ipsilateral to the primary
nasal defect. Historically, contralateral design has been
preferred because it results in less torsion on the pedicle.42
A thinner flap may improve the pliability of the flap with
better nasal contour. A third-stage procedure aiming to thin
the flap and revise the scars should be performed about 6
months later when wound healing and scar contractures are
definitive.
Local flaps such as contralateral cutaneous nasal flap,
nasolabial flaps, nasal or septal mucosal flaps are feasible
options to reconstruct the inner lining. Bhandari17 and
others22 demonstrated the use of a nasolabial flap for nasal
lining. Other authors have published the use of skin graft or
oral mucosal flap. Nasal airway lined by split-skin graft,
however, tends to be stenotic, needing splints or silicone
stents to prevent it. We have used contralateral cutaneous
nasal flap to reconstruct inner lining and a forehead flap to
cover external defect. As illustrated in case 2, forehead
flap can also be used for partial nasal reconstruction. Due
to limitations in the final aesthetic result, we believe that
partial nasal reconstructions should not be the first option.
For nasal framework reconstruction, surgeons have used
conchal or costal cartilage and rib or calvarium bone
grafts.8 In our patients, alar contour was restored using
a cartilage graft from the lower portion of ear tragus and
concha.43
Reconstruction of congenital half-nose has additional
challenges, as in the restoration of nasal airway. Its
reconstruction in the same first stage is even more
difficult and has scarcely been reported in the literature.17 Moreover, reconstructed airway tends to become
stenotic, and measures must be taken to minimise tissue
contraction. Nagase stated that nasal airway reconstruction might not be repaired in congenital hemi-nose,
because these patients usually do not have problems in
breathing when they have the contralateral nasal airway
intact.8 The author reconstructs pyriform aperture in
a second-stage procedure to achieve a natural shading of
the nostril floor, but not intending to have a second
pervious airway.
Regarding the lacrimal system reconstruction, it should
be ideally performed after complete nasal reconstruction,
once it allows tracking lacrimal duct into the new created
nasal cavity.19
Congenital half-nose is an extremely rare malformation.
Pathogenesis remains unclear, and reported cases have
occurred sporadically. Literature review found 91 cases of
half-nose, including 50 patients with proboscis lateralis.
This article presented other seven cases submitted to nasal
reconstruction. Most common form of reconstruction used
contralateral nasal skin flap to restore inner lining, conchaletragus cartilage graft to restore alar framework and
forehead flap to cover the external nasal defect. Follow-up
has demonstrated good results using these techniques for
half-nose reconstruction.
Conflict of interests
There was no financial interest by any of the authors, as
well as no product, device or drug was specifically tested in
this study.
R. da Silva Freitas et al.
References
1. Wicke W. Aplasia of one half of the nose. Monatsschr Ohrenheilkd Laryngorhinol 1972;106:438.
2. Krukeja HK. Half nose. J Laryngol Otol 1973;87:599.
3. Mahindra S, Daljit R, Jamwal N, et al. Lateral nasal proboscis. J
Laryngol Otol 1973;87:177.
4. Schweckendiek W, Hein J. Rare nose abnormalities: unilateral
aplasia in combination with cleft palates. HNO 1973;21:73.
5. Warkany J. Congenital Malformations. 2nd ed. Chicago: Year
Book Medical Publishers; 1975. p. 201e210, 587e596.
6. Mazzola R. Congenital malformations in the frontonasal area:
their pathogenesis and classification. Clin Plast Surg 1976;3:573.
7. van Kempen AAMW, Nabben FAE, Hamel BCJ. Heminasal aplasia: a case report and review of the literature of the last 25
years. Clin Dysmorphol 1997;6:147.
8. Nagase T, Kobayashi S, Ohmori K. Achieving natural shading of
the nostril in the reconstruction of a half nose. Br J Plast Surg
1998;51:131.
9. Motohashi N, Kuroda T, Cohen Jr MM. Half nose with ipsilateral
eye and ear anomalies and facial asymmetry: report of a case
with cephalometric analysis and orthodontic treatment. Cleft
Palate Craniofac J 1999;36:353.
10. Mehta L, Petrikovsky B, Tydings L, et al. Lateral nasal
proboscis: antenatal diagnosis and counseling. Obstet Gynecol
1999;94:815.
11. Salyer KE. Orbital Surgery, hypertelorism, and nasal reconstruction. In: Salyer KE, Bardach J, editors. Atlas of craniofacial & cleft
surgery, vol. I. Philadelphia: Lippincott-Raven; 1999. p. 135.
12. Yildirim SV, Ünal M, Barutçu Ö. Proboscis lateralis: a case
report. Int J Pediatr Otorhinolaryngol 2001;61:179.
13. Belet N. Proboscis lateralis: a case report. Clin Dysmorphol
2002;11:219.
14. Belet N, Belet Ü, Tekat A, et al. Proboscis lateralis: radiological
evaluation. Pediatr Radiol 2002;32:99.
15. Eroglu L, Uysal OA. Proboscis lateralis: report of two cases. Br J
Plast Surg 2003;56:704.
16. Mladina R, Manojlovic S, Markov-Glavas D, et al. An unusual
case of heminasal aplasia: proboscis lateralis or cystic teratoma. J Craniofac Surg 2003;14:41.
17. Bhandari PS. Simultaneous and symmetrical reconstruction of
heminose and restoration of nasal airway in congenital absence
of heminose. Br J Plast Surg 2004;57:575.
18. Abou-Elhamd KEA. Proboscis lateralis: a report of two cases.
Int J Pediatr Otorhinolaryngol 2004;68:503.
19. Boahene DKO, Bartley GB, Clay RP, et al. Heminasal proboscis
with associated microphthalmos and encephalocele. J Craniofac
Surg 2005;16:300.
20. Ugurlu K, Karsidag S, Ozcelik D, et al. Repair of proboscis lateralis. Scand J Plast Reconstr Surg Hand Surg 2005;39:184.
21. Chong JK, Cramer LM. Proboscis lateralis: staged management
with a four-year follow-up. Ann Plast Surg 1978;1:225.
22. Cotin G, Bodard M, Bouchenak B, et al. Reconstruction de
ĺorifice et du vestibule narinaire dans le proboscis lateralis.
Ann Chir Plast 1982;27:144.
23. Ployet MJ, Loustalot B, Moraine C, et al. Two uncommon
malformations of the nose. Attempt at an explanation. Ann
Otolaryngol Chir Cervicofac 1983;100:365.
24. Wang SJ, Wang YM, Roy FH. Proboscis lateralis, microphtalmos,
and cystic degeneration of the optic nerve. Ann Ophthalmol
1983;15:756.
25. Boo-Chai K. The proboscis lateralis e a 14-year follow-up. Plast
Reconstr Surg 1985;75:569.
26. Mugaddu EG. Proboscis lateralis e a rare congenital anomaly. A
case report. S Afr Med J 1985;68:45.
27. Ortiz-Monastério F, Fuente del Campo A, Dimopulos A. Nasal
clefts. Ann Plast Surg 1987;18:377.
Please cite this article in press as: da Silva Freitas R et al., The surgical repair of half-nose, J Plast Reconstr Aesthet Surg (2008),
doi:10.1016/j.bjps.2008.08.040
ARTICLE IN PRESS
+
MODEL
The surgical repair of half-nose
28. Govila A. Proboscis lateralis type I e a report from the Indian
subcontinent. Acta Chir Plast 1991;33:34.
29. Migueis A, Guillen G, Migueis C. Surgical treatment of proboscis
lateralis: apropos of a case. Rev Laryngol Otol Rhinol (Bord)
1993;144:193.
30. Jost G, Mookherjee R, Dionyssopoulos A. Proboscis lateralis:
treatment of two atypical cases. Aesthetic Plast Surg 1995;
19:165.
31. van de Meulen JC, Mazzola R, Vermey-Keers C, et al. A
morphogenetic classification of craniofacial malformations.
Plast Reconstr Surg 1983;71:560.
32. Nicolaides KH, Salvesen DR, Snidjers RJ, et al. Fetal facial
defects: associated malformations and chromossomal abnormalities. Fetal Diagn Ther 1993;8:1.
33. Beg MHA. Half nose. J Laryngol Otol 1984;98:915.
34. Albenaz VS, Castillo M, Mukherji SK, et al. Congenital arhinia.
AJNR Am J Neuroradiol 1996;17:1312.
35. Saraiya H. Isolated congenital unilateral alar defect: a rare
anomaly. Plast Reconstr Surg 1996;97:246.
7
36. Tessier P. Anatomical classification of facial, cranio-facial and
latero-facial clefts. J Maxillofac Surg 1976;4:69.
37. Shorey P, Lobo G. Congenital unilateral absence of orbit with
anophthalmos and partial arhinia. Indian J Ophthalmol 1991;
39:132.
38. David Jr D. Reconstruction: facial clefts. In: Mathes SJ, editor.
Plastic Surgery. 2nd ed., vol. IV. Philadelphia: Saunders; 2006.
p. 381.
39. Millard Jr R. Hemirhinoplasty. Plast Reconstr Surg 1967;40:440.
40. Burget GC, Menick FJ. Aesthetic Reconstruction of the Nose. St
Louis, Mo: Mosby-Year Book Inc; 1994.
41. Giugliano C, Andrades PR, Benitez S. Nasal reconstruction with
a forehead flap in children younger than 10 years of age. Plast
Reconstr Surg 2004;114:316.
42. Boyd CM, Baker SR, Fader DJ, et al. The forehead flap for nasal
reconstruction. Arch Dermatol 2000;136:1365.
43. Pereira MD, Marques AF, Ishida LC, et al. Total reconstruction
of the alar cartilage en bloc using the ear cartilage: a study in
cadavers. Plast Reconstr Surg 1995;96:1045.
Please cite this article in press as: da Silva Freitas R et al., The surgical repair of half-nose, J Plast Reconstr Aesthet Surg (2008),
doi:10.1016/j.bjps.2008.08.040