2002 - Health Sciences Authority")
August 2002 • Vol 4 No. 2
ISSN : 0219-2152
ADVERSE DRUG REACTION NEWS
HSA
Health Sciences Authority
Published by the Expert Panel on Adverse Drug Reactions and the Centre for Pharmaceutical Administration, HSA
ORAL COMBINED
HORMONE
REPLACEMENT
THERAPY
Study concludes oral HRT not beneficial for the
prevention of coronary heart disease in
postmenopausal women.
T
he US Women’s Health Initiative (WHI) trial for women
with intact uterus has been halted prematurely based
on health risks that exceeded health benefits over an
average follow-up of 5.2 years. This was a randomized
controlled primary prevention trial (planned duration of
8.5 years) designed to assess the major health benefits
and risks of the most commonly used combined hormone
preparation (0.625 mg conjugated oestrogen plus 2.5 mg
medroxyprogesterone) in the United States. About 16,000
postmenopausal women aged 50 – 79 years with an intact
uterus at baseline were recruited into the trial between the
period 1993 – 1998.
The key findings after five years relate to an increase in risk of
I Breast cancer (from 30 to 38 per 10,000 women years)
I Coronary heart disease (from 30 to 37 cases per 10,000
women years)
I Stroke (from 21 to 29 cases per 10,000 women years)
The benefits were reductions in
I Colorectal cancer (from 16 to 10 per 10,000 women
years) and
I Hip fracture (from 15 to 10 cases per 10,000 women
years)
Editorial Note
he Health Sciences
Authority (HSA) and the
Expert Panel on ADR
would like to take this
opportunity to thank all our
doctors and pharmacists who
reported the adverse drug
reactions (ADRs) of Slim 10 to
the Pharmacovigilance (PV) Unit.
T
Slim 10 was marketed as a
Chinese Proprietary Medicine for
slimming in December 2001. It
was withdrawn on 19th April 2002
following confirmation of
adulteration of the product with
undeclared substances. An
estimated 20,000 bottles of Slim
10 had been sold.
The first ADR report of acute hepatitis to Slim 10 was received
by the PV Unit in late March 2002. Three other ADR reports,
two of hyperthyroidism and one of menstrual irregularities
were subsequently reported in early April 2002. Based on
these reports, HSA initiated an investigation into the product
which revealed it to be adulterated with nicotinamide,
fenfluramine and thyroid gland components. Since then, HSA
has initiated enforcement action against the parties
responsible for the import, sale and distribution of the
adulterated product.
The cooperation of our healthcare professionals in alerting
HSA to a potential drug safety problem has enabled us to
take timely regulatory action to remove Slim 10 from the
market thereby significantly reducing the risk of exposure
to consumers and consequently the incidence of adverse
effects I
Ms Chan Cheng Leng
Editor-in-Chief
CONTENTS
Oral combined HRT
On-line ADR reporting
3rd generation OC & thromboembolism
Sibutramine (Reductil)
Kava-kava & liver toxicities
Epoetin alfa & pure red cell aplasia
1
2
2
3
3
4
Continued on page 4
Provide us with your full name and email address to receive HSA drug safety information. Email us at HSA_DRUGSAFETY@hsa.gov.sg
Volume 4 Number 2 2002
1
ON-LINE ADR REPORTING
T
➜
he Pharmacovigilance (PV) Unit is pleased to
announce the implementation of the on-line ADR
reporting which is now available at the Health
Sciences Authority (HSA)’s website. This new platform of
reporting allows our healthcare professionals to report
ADRs directly to the PV unit. The reporter inputs the
necessary data into the website and submits it through
the Internet; this information is then translated as an
e-mail to HSA_DrugSafety mail box of the officers in-charge.
A pilot run has been conducted and the quality of the
transmitted information was clear and instantaneous. This
mode of reporting reduces the possibility of reports getting
lost as well as delays in receipt of reports.
The online ADR reporting form is an addition to the other
standard modes of reporting which include reporting
through e-mail (HSA_DRUGSAFETY@hsa.gov.sg),
conventional mail, fax or telephone call to the PV Unit.
Check out the online ADR reporting form at
http://www.hsa.gov.sg/ADR_online.
The online ADR reporting form is at http://www.hsa.gov.sg/
ADR_online. It can also be found at the HSA website under
e-services and the pharmacovigilance webpages I
associated with COCs containing
desogestrel or gestodene with
30 mcg of ethinylestradiol (third
generation COCs) compared to
COCs containing levonorgestrel
with the same amount of
ethinylestradiol (second generation
COCs). For COCs containing
desogestrel or gestodene with
20 mcg of ethinylestradiol, the
epidemiological data do not
suggest a lower risk of VTE than
for those containing 30 mcg of
ethinylestradiol
THIRD GENERATION ORAL
CONTRACEPTIVES AND VENOUS
THROMBOEMBOLISM (VTE)
Although the risk of VTE with the use of third generation oral
contraceptives remains small, women should be advised that this group
of drugs is associated with an increased risk of VTE when compared to
the older ones.
T
he risk of developing venous
thromboembolism (VTE) is a
recognised
complication
associated with the use of combined
oral contraceptives (COCs). Over the
years, there has been ongoing debate
as to whether third generation COCs
(OCs containing gestodene or
desogestrel) are associated with a
higher risk of VTE than second
generation COCs (OCs containing
levonorgestrel or norethisterone).
The European Committee for
Proprietary Medicinal Products (CPMP)
has published the outcome of its
assessment of the risk of VTE associated
with the use of third generation COCs
in September 2001. This assessment
was based on the reviews of
epidemiological studies and studies on
blood clotting mechanisms from the
period 1995 to September 2001.
2
Volume 4 Number 2 2002
I
The estimates of the overall relative
risk for VTE for the third generation
COCs compared to the older ones
vary
considerably
among
epidemiological studies. On the
basis of a careful evaluation of all
available data, the best estimate
of the relative risk is in the range
of 1.5 – 2.0
I
The increased risk of VTE
associated with COCs is less than
the risk of VTE associated with
pregnancy
In summary, CPMP concludes that:
I
VTE is a rare adverse effect of all
COCs. The level of this risk is low
and the overall balance of benefits
and risks remains favourable with
all COCs
I
The risk of VTE is highest during
the first year that a woman ever
uses any COC
I
Evidence suggests that there is
a small increased risk of VTE
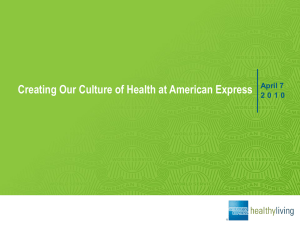
The risk of VTE can be expressed as follows when taken in relative perspective:
Risk Factor
Incidence of VTE
Healthy women between 15 – 44 yrs
old not taking COCs
5-10 cases per 100,000 women years
Women taking second generation
COCs
20 cases per 100,000 women years
Women taking third generation COCs 30-40 cases per 100,000 women years
Pregnancy
60 per 100,000 pregnancies
UPDATED REPORT ON SIBUTRAMINE (REDUCTIL)
The risk/benefit profile of
sibutramine remains positive when
used accordingly to labelled
indications.
n March 2002, the Italian
regulatory authority temporarily
suspended
the
sale
of
sibutramine (Reductil, Abbott), an antiobesity drug, due to the occurrences
of adverse drug reactions including two
reports of death in Italy suspected to
be associated with sibutramine. The
Italian authority also initiated a request
to the central European Committee for
Proprietary Medicinal Products (CPMP)
to reassess the efficacy and safety of
sibutramine.
I
HSA’s review
Pending CPMP’s outcome of the review,
HSA had reviewed the safety data of
sibutramine in March 2002 and
concluded that the risk/benefit profile
of sibutramine remains positive and it
would not be necessary to take similar
regulatory action to suspend the
marketing approval of the drug.
HSA’s stand was posted on its
website in March 2002 at http://
w w w. h s a . g o v. s g / h s a / c p a /
CPA_information_whatsnew.htm.
CPMP’s report
The CPMP has recently finalised its view on sibutramine in June 2002. It has given
a positive opinion on sibutramine, reaffirming the favourable risk/benefit profile of
sibutramine for the treatment of obesity. The opinion of the CPMP was supported
by analysis of data that included clinical studies of sibutramine, dating back to
1989 in about 12,000 obese patients.
To-date, none of the other regulatory agencies including the Medicines Control
Agency, UK, the Food & Drug Administration, USA and the Therapeutics Goods
Administration, Australia has taken any regulatory actions against the marketing
authorisation of the drug.
Use of sibutramine
Physicians are reminded that sibutramine should only be prescribed to patients
who have a body mass index (BMI) > 30 kg/m2 or patients with BMI > 27 kg/m2
with obesity related risk factors such as type II diabetes and dyslipidaemia who
have not responded adequately to an appropriately designed weight reduction
programme. Treatment must also be discontinued if a 5% weight reduction is not
achieved within three months. In addition, sibutramine should only be administered
as a component of a therapeutic approach to weight loss on the long-term, under
the supervision of a physician experienced in obesity treatment. The drug has also
been approved for adjunctive treatment of obesity for up to one year only.
Sibutramine can cause elevations in blood pressure and heart rate in some patients.
Hence it is necessary to monitor the blood pressure and pulse rate regularly
especially during the initiation of therapy. The drug should be discontinued if
blood pressure levels exceed 140/90 mmHg at two consecutive readings. It is
contraindicated in patients with inadequately controlled hypertension and in patients
with history of heart diseases such as congestive heart failure and irregular rhythms.
Detailed information regarding the use of sibutramine can be found in the product
information leaflet of Reductil.
All healthcare professionals are encouraged to report any adverse drug reactions
suspected to be associated to Reductil to the Pharmacovigilance Unit I
KAVA-KAVA AND LIVER TOXICITIES
Kava-kava health supplements are no longer available
in Singapore.
ava-kava containing health supplements were
voluntarily withdrawn in Singapore in January 2002.
This precautionary measure was taken pending a
decision by the German regulatory authority’s review of
reports of serious liver injuries suspected to be associated
with the product. No such adverse effects have been reported
in Singapore.
K
Kava-kava (Piper methysticum) is a plant indigenous to the
islands in the South Pacific. Supplements containing the herbal
ingredient kava are promoted for relaxation (e.g. to relieve
stress, anxiety and tension), sleeplessness and for ailments
affecting the bladder and digestive tracts.
Regulatory decisions
Recently, in June 2002, BfArM, the German drug regulatory
authority has finalised its decision on kava-kava and has
notified the marketing authorisation holders that all kavakava and kavaine containing products will be withdrawn from
the German market due to hepatotoxic risks and insufficiently
proven efficacy of these products. The kava-kava products
that have been associated with liver toxicities relate to the
chemically extracted ingredients of kava marketed as health
supplements.
The decision was based on an in-depth review of all the
reports of liver toxicities. To-date, there are more than 40
cases of liver toxicity with suspected links to consumption of
kava-kava. Of these cases, six led to complete liver failure
that required an organ transplant and three cases resulted in
death.
In the light of confirmation of the liver toxicity risk and to
enhance safeguards, HSA is proceeding to gazette kava-kava
and its active constituents as poisons under the Poisons Act.
This will prohibit the importation and sale of health products
containing kava-kava I
Volume 4 Number 2 2002
3
Continued from page 1
Oral Combined Hormone
Replacement Therapy
This new data confirms and adds to
information that is already known about the
benefits and risks of oral combined HRT in
women with intact uterus. The results of
the trial confirms and quantifies the small
increase in risk of breast cancer (significant
only after the fifth year of therapy onwards)
and provides new information on stroke. It
confirms the lack of protection from
coronary heart disease and shows instead
a small increase in risk. It also confirms the
protection against hip fracture and reveals
a reduced incidence of colorectal cancer.
On the whole, the percentage of women
who experienced adverse effects from the
combined HRT was small and therefore the
risk to the individual women in the trial was
small.
There is another arm of the WHI trial which
is still ongoing and it involves women who
had a hysterectomy and are treated with
oestrogen alone. This trial has not been
halted as the balance of risks and benefits
in the unopposed-oestrogen component
remains uncertain and there were no
significant adverse events in this study
group. The trial will go on as planned for
the duration of 8.5 years.
In UK, a major trial, the Women’s
International Study of Long Duration
Oestrogen after Menopause (WISDOM)
which began in 1999 will continue but no
new patients will be recruited until an
international team commissioned by the
British Medical Research Council has
reviewed the findings of the WHI trial. The
WISDOM trial which was planned till 2012
was intended to cover over 20,000
postmenopausal women from UK, Australia
and New Zealand. It sought to find out if
HRT lowers or increases the chances of
developing diseases and conditions such
as heart attacks, breast cancer, osteoporosis
and dementia. The HRTs studied involve the
combined HRTs and the oestrogen alone
preparations.
HSA has initiated communication with the
product license holders of the relevant oral
combined HRT preparations in Singapore
to update the new findings in the product
information leaflets. HSA in consultation
with medical experts in the
management of HRT has issued a public
advisory on the matter. Please refer to
http://app.internet.gov.sg/scripts/hsa/
communications/pressreleases.asp for more
information.
Healthcare professionals may also refer to
the websites from other regulatory agencies
for more information on the topic:
Australia Therapeutic Goods Administration
http://www.health.gov.au/tga/new/new.htm
UK Committee of Safety of Medicine
h t t p : / / w w w. m c a . g o v. u k / o u r w o r k /
monitorsafequalmed/safetymessages
US Food and Drug Administration
http://www.fda.gov/cder/whatsnew.htm
4
Volume 4 Number 2 2002
EPREX® (EPOETIN ALFA) AND
REPORTS OF PURE RED CELL
APLASIA
Majority of reports of pure red
cell aplasia are associated with
the subcutaneous route of
injection.
poetin alfa (Eprex, JanssenCilag) is indicated for the
treatment
of
anaemia
associated with chronic renal failure
(CRF),
cancer
chemotherapy,
autologous blood donation and during
major elective orthopaedic surgery.
E
Pure red cell aplasia (erythroblastopenia) has been reported in CRF
patients between 1-92 months from the
initiation of Eprex therapy (median
onset is 11 months).
From 1998 through April 2002, there
have been 124 such cases of suspected
pure red cell aplasia reported
worldwide of which 104 are reported
to have been confirmed by bone
marrow examination. Antibodies to
erythropoietin have been observed in
63 (out of 79 for whom results were
available) Eprex treated patients
diagnosed with PRCA. Most of the
worldwide reports of PRCA are
associated with the subcutaneous (SC)
route of administration, the
predominant route of administration
practised in most countries. The
estimated worldwide Eprex exposure
is 16 x 105 patient-years, giving a worldwide reporting incidence rate for
suspected PRCA of 7.5 per 100,000
patient-years.
Based on the company’s investigations,
no single trigger has been identified todate and a number of factors may have
contributed to the development of
immunogenicity. Eprex is approved to
be administered by subcutaneous and
intravenous injection. Available
scientific information suggests that the
subcutaneous route of administration
for some medicines, such as Eprex,
may increase the likelihood of the body
producing antibodies that could reduce
the effectiveness of the medicine and
possibly lead to events such as PRCA.
Whilst the company continues with its
investigations, Janssen-Cilag is
recommending that the product be
administered by the IV route in CRF
patients, where feasible.
The company advises that in patients
with worsening anaemia, other causes
(eg., iron, folate or vitamin B 12
deficiency; aluminium intoxication;
infection or inflammation; blood loss or
haemolysis) should be excluded. If
PRCA is suspected it should be
confirmed with bone marrow
examination and/or antibody testing.
Epoetin alfa should be discontinued,
and patients should NOT be switched
to another erythropoietin. PRCA may
respond to immunosuppressive therapy
and spontaneous resolution has
occurred occasionally. In many of the
cases, the patients become transfusion
dependent.
HSA is aware of several local cases of
PRCA associated with Eprex usage,
however the causality to Eprex has not
been established as yet. Healthcare
professionals are encouraged to report
the ADRs to Pharmacovigilance Unit
should they come across any such
cases. Antibody testing can be
arranged through Janssen-Cilag at
telephone 62658922. HSA will be
closely following the investigations by
the company I
Adverse Drug Reaction News is produced by the Expert Panel on Adverse Drug Reactions
and the Centre for Pharmaceutical Administration, Health Sciences Authority
Editor-in-Chief:
Editorial Board:
Ms Chan Cheng Leng, BSc Pharm (Hons)
Clinical Professor Goh Chee Leok,
Clinical Assoc. Professor Chng Hiok Hee, Dr Gilbert Lau,
Clinical Professor Ng Han Seong, Professor Vernon Oh
Enquiries, comments and suggestions to:
Ms Chan Cheng Leng, Pharmacovigilance Unit, Centre for Pharmaceutical Administration,
Health Sciences Authority
2 Jalan Bukit Merah, Singapore 169547, Tel: 6325 5604, Fax: 6325 5448
Website: http://www.hsa.gov.sg/cpa Email: HSA_DRUGSAFETY@hsa.gov.sg
Its contents are not to be reproduced in part or in whole, without prior written approval to the editor. The
mentioning of any product by the author does not imply any official endorsement of the product by the
Health Sciences Authority. Copyright 2002 Health Sciences Authority of Singapore. All Rights Reserved.
 2002 - Health Sciences Authority")