Pathology Update 2008
advertisement

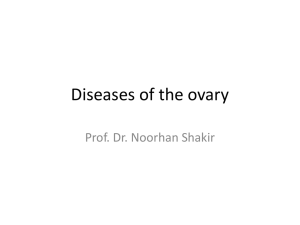
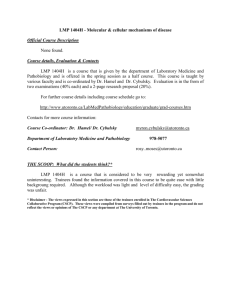
Pathology Update 2008 Gynecologic Pathology MUCINOUS TUMORS OF THE OVARY: Criteria and Considerations Session 2 - Friday, Nov. 21,2008 By: Terence Colgan, MD, FRCPC Head, Gynaecological Pathology & Cytology Pathology & Lab Medicine, MSH Professor, Laboratory Medicine & Pathobiology University of Toronto THE CHALLENGE : Identifying morphologic entities along a spectrum • Evidence based ? None available using strength of recommendation (A → E) and quality of evidence (1 → 3) • Consensus statements : NIH and WHO • The published literature • The “strong man” (or woman) 1 Pathogenesis of Mucinous LMP (Intestinal) Stepwise Progression Inclusion cyst or (germ cell?) Mucinous Cystadenoma Mucinous LMP Mucinous AdenoCa Mucinous LMP with Intraepithelial carcinoma Increasing prevalence of KRAS mutations at codons 12 & 13 Diagnostic Criteria for Mucinous Cystadenoma A cystic epithelial tumor lined by bland mucinous epithelium of endocervical type 2 Mucinous cystadenoma Mucinous cystadenoma 3 Mucinous cystadenoma Mucinous cystadenoma 4 Heterogenesity in mucinous tumor (LMP) Mucinous cystadenoma “reactive changes” 5 Diagnostic Criteria for Mucinous LMP’s (Intestinal) • Evidence of proliferative activity (mitotic activity, pleomorphism, and stratification), AND • Absence of stromal invasion Mucinous LMP 6 Natural History of Mucinous LMP’s (Intestinal) • Stage 1 Mucinous LMP’s , 100% survival • Stage 2,3 Mucinous LMP’s, reported survival - 50% - exclude pseudomyxoma peritonei (appendiceal) cases - exclude metastatic adenoca mimics from upper GI and cervix • Advanced Stage Mucinous LMP’s may not exist Mucinous LMP, intestinal type, necrosis 7 Mucinous LMP, intestinal type, necrosis The challenge of the mucinous cystadenoma with a “borderline component” NIH 2004 Consensus • • • • • ignore it? call it borderline? call it “cystadenoma with borderline”? call it “cystadenoma” with a note use a threshold of the proportion of “borderline” - 10% ? * Remember 100% of Stage 1 borderline tumours behave in a benign fashion! 8 Diagnostic Criteria for Mucinous LMP Tumour with Intraepithelial Carcinoma • Mucinous LMP tumour of intestinal type Plus • Severe cytologic atypia Note: Stratification + complexity alone are not sufficient 865Mc Intraepithelial carcinoma mucinous tumor (LMP) 9 Intraepithelial carcinoma in mucinous LMP Diagnostic Criteria for Mucinous LMP Tumour with Microinvasion • mucinous tumour of LMP Plus • focus (or foci) of stromal invasion ≤ 5 mm in greater linear measurement * * alternative dimensions: ≤ 3 mm or ≤ 10 mm2 10 Microinvasion in mucinous LMP, e.g. 1 Microinvasion in mucinous LMP, e.g.2 11 Diagnostic Criteria for Mucinous LMP Tumour, Mullerian type (a.k.a.- “endocervical type”) (a.k.a. – “seromucinous) • presence of mucinous epithelium of endocervical type • absence of enteric type epithelium • intracystic papillary architecture of eosinophilic, stratified epithelium • may/may not have serous type epithelium Mucinous LMP, Mullerian type 12 Mucinous LMP, Mullerian type Mucinous LMP, Mullerian type 13 Mucinous LMP, Mullerian type Mucinous LMP, Mullerian type 14 Diagnostic Criteria for Ovarian Mucinous Adenocarcinoma • An epithelial tumour with intracytoplasmic mucin that shows destructive stromal invasion ( > 5 mm)* OR Confluent, glandular expansile pattern of growth of > 5 mm in linear dimension • Absence of another acceptable primary origin (beware of the deceptive situation in unilaterality and no known primary) * Less common, but poorer prognosis “Borderline-like focus” in primary mucinous adenoCa 15 Primary mucinous adenoCa (expansile criterion e.g. 1) Primary mucinous adenoCa (expansile criterion e.g. 1) 16 Primary mucinous adenoCa (expansile criterion, e.g.2) Differential Diagnosis of Mucinous Ovarian Adenocarcinoma • Metastases from cervix, gall bladder, pancreas, appendix, colon, stomach ( CK7 + 20 of little value ) • Endometrioid carcinomas with mucinous differentiation (ovary + endometrium ) • Sertoli-Leytig cell tumour, heterologous type • Mucinous (goblet cell) carcinoid tumour (primary and secondary) • Signet-ring adenocarcinoma (think metastatic) 17 Metastatic mucinous AdenoCa to ovary Mucinous adenoCa to ovary – Criteria: sites of disease, bilaterality, Nodularity, LVI 18 Mucinous Ovarian Tumours in Association with Pseudomyxoma Peritonei • primary is almost invariably the appendix (or GIT) • always recommend appendectomy and examination of pancreatobiliary • ovarian tumours should be labelled as ‘secondary’ or ‘metastatic’ • avoid use of terms “borderline”, “LMP”, and “cystadenoma” • exception: ovarian tumour with pseudomyxoma peritonei – mucinous tumour arising in a dermoid cyst Appendix –Mucinous Neoplasia 19 Mucinous tumor with teratoma Mucinous tumor with teratoma 20 Mucinous tumor with teratoma Mucinous tumor with teratoma 21 Mucinous tumor with teratoma Mucinous tumor with teratoma 22 Assessment of Pseudomyxoma Peritonei • Are epithelial cells present or not? • Are any cells benign appearing (adenomucinosis), malignant (carcinomatosis), or borderline (indeterminate)? • Presence/absence of mucin dissection and fibrous reaction Pseudomyxoma peritonei 23 Pseudomyxoma peritonei Thank you ! *** L U N C H *** 24