Shouldice Hospital Operations Assessment: Capacity Expansion
advertisement

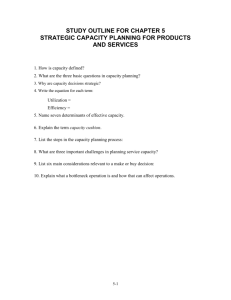
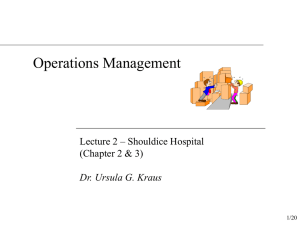
Shouldice Hospital: Operations Assessment Shouldice Hospital has been devoted to repairing hernias for over half a century. Although the Shouldice system has led to great competitive positioning, the hospital is falling victim to its own success. Demand for Shouldice services is so much higher than its current capacity of 89 beds that it is in a constant state of operations backlog, which grows by 100 patients every 6 months. Thus, Shouldice needs to find a solution to its single most critical question – how to expand the hospital’s capacity while simultaneously maintaining quality control of service delivery. The analysis below is designed to assess the current operations at the hospital, in addition to explaining our recommendation that Shouldice should invest $4MM in a new unit, which will increase bed capacity by 50% and require its surgeons to perform Saturday surgeries. As the financial analysis shows, this change will allow Shouldice to capture unmet demand without compromising its unique system of patient and employee care. Lastly, our recommendation will be also juxtaposed to other options we evaluated as potential solutions, but that neither make financial sense nor solve the current dilemma for the hospital. Hospital Overview Shouldice Hospital is a “focused factory:” a hospital with a specific area of expertise that gives it competitive strength resulting in lower cost, higher quality service for its patients, and better pay for and loyalty from its employees. Specializing in external abdominal hernias, Shouldice doctors execute the “Shouldice Technique” developed by founder Dr. Edward Earle Shouldice. This precise technique has resulted in early ambulation and higher success rates (greater than 99%) for Shouldice patients for over 55 years. However, what makes Shouldice so successful is that it is not just a hernia-healing hospital, it is an experience. To the delight of patients, Shouldice is more like a country club than a hospital: warm, inviting, and relaxing versus cold, sterile, and frightening. The main house, reminiscent of a mansion, is situated on a sprawling 130 acre estate outside of Toronto, Canada. The comprehensive patient experience includes orientation, evening tea, patient socializing, and encouraging nurses and housekeepers. The service continues beyond patient stays and continues at free annual check-ups and lavish patient reunions. Patients actually get this superior technique and remarkable environment for approximately half the cost of going elsewhere. Overall, the Shouldice experience is one that patients love and tell their friends and family about, making word-of-mouth the hospital’s primary marketing vehicle. Shouldice is also an experience for its employees. Shouldice employees are never fired, can participate in profit-sharing, and earn higher wages than union workers and other surgeons. Doctors make approximately 15% more than the average surgeon in Ontario, receive monthly bonuses, and are able to work regular hours leaving them time for personal lives and families. These human resource practices have led to extremely low turnover, which supports the administration’s goal of having very experienced staff that can properly and effectively execute the hospital’s practices and procedures. The Shouldice competitive advantage boils down to 4 keys to success, which are the following: Distinctive technique Experienced staff Comprehensive patient experience Thoughtful employee policies These 4 elements work in unison (See Appendix 1: Shouldice Advantage) at Shouldice to promote healthy and happy patients, in addition to content and loyal staff. As the hospital itself states, “Shouldice Hospital is a total environment.” Bottleneck Analysis (See Appendix 2: Analysis Assumptions) Process Flow 2 Incoming Patients Bottleneck Day 1 42 Exams 4 Sent Home 33 Surgeries 38 Surgery Candidates 89 Beds Available Day 2 Bottleneck 116 Extended Stay Day 2-5 Discharged Day 4-5 Bottleneck Shouldice has the capacity to perform 42 examinations per afternoon and send 38 eligible patients to the operation rooms. However, it only performs 33 operations per day, so the bottleneck between these 2 processes is the number of operations being performed per day. Shouldice performs 33 operations per day, which generate daily bed demand of 116 on Wednesday and Thursday, and 99 on Tuesday (See Appendix 3: Shouldice.xls), all exceeding the current bedding capacity of 89. So between these 2 processes, the number of available beds is the bottleneck. Overall, the bottleneck for Shouldice is the number of available beds. The hospital has to increase its bed capacity by 30% [(116-89)/(89)] to simply meet its current operation schedule. Current operation schedule Morning operations: (4/room)*(5 rooms) = 20/morning Afternoon operations - Assume 50-minute time slot (45min+overhead) - Number of available slots = 150min/50min*5 rooms = 15/afternoon - On average each operation takes (1*90%)+(2*10%) = 1.1 slots - Total operation capacity = (15)/(1.1) = 13/afternoon Actual operation capacity Consider morning operations between 8:30AM to 12:30 PM - Available slots per room = (4)*(60 min)/(50 min) = 4.8 - Total operation capacity = (4.8 slots)/(1.1 slot per operation)*(5 rooms) = 20 There is 1 operation per room before 8:30 AM Total operation capacity per morning = (20)+(5) = 25 Therefore, total operation capacity per day equals 38/day [(25/morning)+(13/afternoon)] without having to increase the number of surgeons and/or operating rooms. Bottleneck Solution 3 As we established above, the current bottleneck lies in the room capacity of 89 and that an increase in the number of rooms will fix this bottleneck. The next question then becomes – how many rooms should be added? To answer this, we asked ourselves how many operations the hospital could perform if the current 89 room capacity did not exist. In analyzing the “next” bottleneck, we found that the number of operating rooms would be the next constraining resource. Currently there are 30 to 36 operations performed daily at the clinic, for an average of 33 operations. Spread across the 5 existing operating rooms, this averages out to 6.6 operations per room, per day, with some rooms having 7 operations per day and some rooms having only 6. Broken down to the specific hours of the day, assuming that there are 4 operations performed in each room during the morning hours (from 7:30 AM to 12:30 PM), a total of 20 operations are performed before lunch each day at the clinic. After lunch, the remaining 13 operations are performed. We believe that this represents an opportunity for improvement. Since each of the normal operations take 1 hour, and there are 5 hours available during the morning, 5 operations could be scheduled in each operating room from 7:30 AM to 12:30 PM. This would represent an increase of 1 operation per room, or a total of 5 across the 5 operating rooms per day at the hospital. Currently we do not see any opportunity for improvement during the afternoon session, as there are only 3 hours available in each room and a small amount of slack must be built in to the model to allow for a small percentage of the procedures that take 90 minutes. The resulting model would have 25 operations performed each morning and 13 performed each afternoon, for a total of 38 operations each day. A comparison of the current model and the revised model is shown in the diagram below: 7:30am Current Throughput 7:30am 4 Surgeries x 5 rooms = 20 total Revised Throughput 5 Surgeries x 5 rooms = 25 total 12:30pm 12:30pm Lunch Lunch 1:00pm 1:00pm 3 Surgeries x 5 rooms – 2 90 min. ops = 13 total 3 Surgeries x 5 rooms – 2 90 min ops = 13 total 33 Operations Per Day 4:00pm 38 Operations Per Day 4:00pm The new model of 38 procedures per day, when scheduled across a 5 day week, results in a schedule that requires at least 133 rooms be available during peak days of the week. The diagram below illustrates the revised hospital admittance schedule and resulting peak day capacities: 4 Monday Tuesday Wednesday Thursday Friday Saturday Sunday Total Monday 38 0 0 0 0 0 38 Tuesday 38 38 0 0 0 0 38 Wednesday 38 38 38 0 0 0 19 Thursday 19 38 38 38 0 0 0 Friday 0 19 38 38 0 0 0 Saturday 0 0 19 38 0 0 0 Sunday 0 0 0 19 0 0 38 76 114 133 133 95 57 57 The new need for 133 rooms represents a 50% increase in capacity when compared to the current capacity of 89 rooms. Recommendation Analysis (See Appendix 4: Alternative, Non-Feasible Recommendations) Recommendation Shouldice should invest $4MM in a new unit, which will increase bed capacity by 50% and require its surgeons to perform Saturday surgeries. Bottleneck Since Saturday operations do not require higher bedding capacity, the result is the following: Bed capacity will increase to (89)*(1+50%) = 133, which exceeds the number of beds currently needed (116) thus eliminating bedding capacity as the bottleneck. With 133 beds available, 38 new patients can be accommodated per day, thus 38 operations can be performed per day. The daily examination capacity, daily operation capacity, and number of beds available all line up perfectly, with no individual factor as bottleneck. Cost/Revenue Current profit per operation = $571 (See Appendix 3: Shouldice.xls) Number of added operations per year = (7600/33)*(38)*(1+20%)-(7600) = 2901 Profit increase = ($571)*(2901) = $1,656,471/year Cost increase = 1 time investment of $4,000,000 Payback period for the investment = (4,000,000)/(1,656,471) = 2.4 years Conclusion Based on the qualitative and quantitative analysis provided herein, our recommendation is that Shouldice should invest $4MM in a new unit that will increase the hospital bed capacity by 50% and require its surgeons to perform Saturday surgeries. With this plan, the throughput rate increases to 38% (2901/7600 = 38%) and provides a payback period of only 2.4 years. Both financially and operationally speaking, adoption of this recommendation solves the hospital’s dilemma of how to increase capacity while simultaneously maintaining quality control of service delivery. Therefore, considering the increased throughput rate and short payback period, this recommendation is a sound plan for Shouldice Hospital to adopt. 5 Appendix 1: Shouldice Advantage Distinctive Technique Comprehensive Patient Experience Thoughtful Employee Policies Experienced Staff 6 Appendix 2: Analysis Assumptions Known 1. 2. 3. 4. 5. facts There are 6 exam rooms. Each examination takes 20 minutes. There are 5 operation rooms. There are total of 89 beds for patient accommodation. No surgeries on Saturday or Sunday. Assumptions 1. Surgeons examine incoming patients from 1:30 PM to 4:00 PM (150 minutes) Sunday through Thursday. 2. 10% of patients examined in the facility are sent back home. 3. 33 operations are performed each day Monday through Friday. 4. Primary operations take 45 minutes to finish, recurrence operations take 90 minutes to finish. 5. 10% of all the operations are recurrence operations. 6. Assistant surgeons, nurses and house keeping staff have no impact on the overall capacity. 7. Average patient hospital stay is 3.5 nights. 8. Adding number of operations doesn’t change net profit per operation. 9. Only operation process and financial performance are analyzed, human factor is not considered in this part of the analysis. 10. 1 new unit is included in analysis as an additional room, rather than separating 1 room for renovation and 1 room for a new unit. 11. Saturday surgeries will not increase surgeon’s weekly hours at the hospital. Calculations Maximum exams per room: (150)/(20) = 7 Maximum exams per day: (7)*(6) = 42 Maximum number of patients eligible for operation per day: (42)*(90%) = 38 Surgeon utilization in the morning: (5)/(10) = 50%(at most 5 surgeons working at any given time) Surgeon utilization in the afternoon: 100% (5 surgeons operating, the other 5 surgeons examining) 7 Appendix 3: Shouldice.xls Bed Capacity Daily Admit Rate Number of Beds Stay Length Inputs 33 89 3 Saturday Surgery No Monday Tuesday Wednesday Thursday Friday Saturday Sunday Total Number in Hospital Inputs: Admit rate, Number of Beds, Nights of stay, Saturday surgeries Outputs: Number of beds used each night Nights Arrived on Monday Monday 33 0 0 0 0 0 33 Tuesday 33 33 0 0 0 0 33 Wednesday 33 33 33 0 0 0 0 Thursday 0 33 33 33 0 0 0 Friday 0 0 33 33 0 0 0 Saturday 0 0 0 33 0 0 0 Sunday 0 0 0 0 0 0 33 66 99 99 99 66 33 33 Profit Analysis Process Total Operations/patients per year Operations per day Number of beds 7600 33 89 Budget Hospital Clinic Total Cost per operation Operations per doctor 8500000 3500000 12000000 1579 760 Revenue Room Charge for 3.5 nights Surgery Charge(all surgery) Total Charge per Operation Total revenue for operations Revenue for general anesthesia Overall revenue Revenue per operation Total Profit Profit per Operation 1440 650 2090 15884000 456000 16340000 2150 4340000 571 8 Appendix 4: Alternative, Non-Feasible Recommendations Additional Beds/Floor Cost High: $4MM Complexity High: Planning, construction, etc. High: Directly addresses the Capacity-Building bottleneck & increases beds by Potential 50% Constituent Impact Allows more patients to be serviced @ Shouldice Has minimal impact on staff Saturday Surgeries Low: Small increase in doctor’s salaries Franchising Moderate Low: Only impacts doctor’s schedules Moderate Moderate: Capacity +20% but does not address the bottleneck Low: Does not address capacity issues at current facility Chair of the Board & Chief Surgeon opposed along w/40% of older doctors Could create wedge between young & old in environment where experience is key Difficult to control quality of service Brand equity potentially compromised May take some business from current facility Alternative Recommendation #1 Invest $4MM in a new unit to increase bed capacity by 50%. Bottleneck Bed capacity will increase to (89)*(1+50%) = 133, which exceeds the number of beds currently needed (116) thus eliminating bedding capacity as the bottleneck. With 133 beds available, 38 new patients can be accommodated per day, thus 38 operations can be performed per day. In this scenario, the daily examination capacity, daily operation capacity, and number of beds available all line up perfectly, with no individual factor as bottleneck. Cost/Revenue Current profit per operation = $571 (See Appendix 3: Shouldice.xls) Profit increase after increasing bedding capacity and number of operations is ($571)*(7600/33*38-7600) = $657,515/year Cost increase is: 1 time investment of $4,000,000 Payback period for the investment = ($4,000,000)/(657,515) = 6 years Conclusion No. Operations: +15% Bottleneck: Eliminated Investment Payback: 6 years Alternative Recommendation #2 Perform Saturday surgeries without making other facility changes. Bottleneck Maximum number of beds needed remains the same at 116, but number of days that 9 bedding needs exceed bedding capacity increases from 3 (Tues, Wed, and Thurs) to 4 (Tues, Wed, Thurs, and Fri). Cost/Revenue Currently profit per operation = $571 (See Appendix 3: Shouldice.xls) Profit increase after adding operations = ($571)*(7600)*(20%) = $868,000/year No increase in cost Conclusion No. Operations: +20% Bottleneck: Aggravated No Upfront Investment, profit increase 20% Alternative Recommendation #3 Franchise additional, off-site locations to expand operational capacity. Bottleneck No initial bottlenecks would exist at franchised locations, but that will not last Cost/Revenue (qualitative) Rapid expansion – domestic and international – increases revenue flow Remove management and operational burden at main facility Remove potential conflict between older and younger doctors Lessens threat of disrupting corporate culture Meet competitive threat Conclusion Quality of service/brand is jeopardized due to outsourcing Loss of control and monitoring problems arise Current bottleneck in operations at main facility is not resolved 10