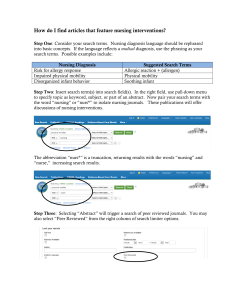
ABC 'S OF PASSING LOCAL BOARD EXAM
advertisement

ABC ‘S OF PASSING LOCAL BOARD EXAM (ADDITIONAL BULLETS FOR MS) Abdominal aortic aneurysm Main problem :Local distention / outpouching of the artery wall usually in the thoracic or abdominal area Initial manifestation :Initially asymptomatic; pulsating abdominal mass is a common sign, backache and auscultation of bruit are common manifestations ; abdominal or back pain Laboratory Data : Elevated BUN and creatinine levels MRI, CT scan and X-ray. UTZ is the best test to confirm AAA Nursing Diagnosis : Altered tissue perfusion Nursing Interventions : Avoid abdominal palpation, prepare patient for surgery Monitor for possible rupture preoperatively(signs of shock) Monitor MIO and laboratory studies Administer medications to decrease hypertension and control pain Monitor peripheral pulses postoperatively Acne Vulgaris Inflammatory disease of sebaceous follicles due to blockage of sebaceous glands Initial manifestation : Closed comedones( “ whiteheads “ ), open comedones ( “blackheads”) Nursing Diagnosis : Body image disturbance Nursing Interventions : Instruct patient to wash face gently with mild soap 1-2 times daily. Instruct patient to use benzoyl peroxide and never squeeze pimples Use of Isotretinoin ( Accutane ) for treatment can cause birth defects. Instruct patient to use contraceptives during the entire duration of the therapy unitl a month thereafter. Avoid exposure to sunlight and use sunblock when using these medications. Acromegaly oversecretion of growth hormone(anterior pituitary), long lasting stimulation affecting skeletal growth in adult by enlarging certain bones and tissues Initial manifestation : coarse facial features, increased shoe size, increased intracranial pressure due to tumor headache and blindness Laboratory Data : elevated serum human growth hormone and blood sugar levels Priority Nursing Diagnosis : body image disturbance Nursing Interventions : provide emotional support prepare client for surgery and deligently monitor VS and Neurologic Status post-op Monitor for signs and symptoms of diabetes octreotide ( Sandostatin) to decrease GH Acute gastroenteritis ( AGE ) / Diarrhea Increase in fluid , frequency and volume of stool usually associated with rotavirus, clostridium deficile, salmonella Initial manifestation : Frequent watery stool Laboratory Data : Decrease in Na and K, (+) blood cultures usually for salmonella, rotavirus and clostridium defficile Nursing Diagnosis : Fluid and electrolyte imbalance Nursing Interventions : Priority ; fluid replacement Remember : fluid loss is more critical in younger patients because they have higher body fluid percentage. Monitor the patient’s fluid status, weight is a critical indicator of fluid loss, 1 gram of weight equals 1 ml of body fluid. Initially offer oral rehydration solution such as pedialyte then progress to non-carbonated drinks ( Gatorade) limit apple juice since it can cause diarrhea. BRAT diet Acquired Immune Deficiency Syndrome ( AIDS) Slow degeneration of the immune system( defect in T- cell mediated immunity caused by the HIV) with the development of opportunistic infections, malignancies and frequent impairment of the central nervous system Initial Manifestation : Flu- like symptoms occur 2-4 weeks after infection Laboratory Data : Diagnosis of AIDS is based on laboratory evidence of HIV infection coexisting with one or more indicator diseases such as Pneumocyctis carinii Pneumonia , Kaposis Sarcoma( most common malignancy), Cytomegalovirus , Candidal infection ,Herpes Simplex Virus or AIDS dementia HIV (+) on ELISA, confirmed by Western Blot HIV antibodies are detectable by routine tests, 3-6 months after infection so instruct the patient to have an initial test 3-6 months after exposure. Patients who are initially negative should have a retest 12 weeks or less since a possible exposure CD4 lymphocytes , 200 / cu .mm Priority Nursing Diagnosis : Risk for infection Nursing Interventions : Instruct patient to practice safe sex, avoid needle sharing.Maintain Satndard Precautions Monitor for opportunistic infections.Monitor respiratory status and laboratory values.Maintain diet/nutrition Use 10 % household bleaching solution to cleanse areas with blood stains from an HIV (+) patient Assess the patient for signs and symptoms of dementia like incoordination. Addison’s Disease Adrenal hypofunction usually due to autoimmune disease Initial Manifestation :Hypotension; bronze skin pigmentation is a common sign Laboratory Data : Hyponatremia, hyperkalemia, hypoglycemia Nursing Diagnosis : Fluid volume deficit Nursing Interventions : Monitor fluid and electrolyte balance Explain the need for lifelong medications of glucocorticoids and mineralocorticoids Maintain high sodium, low potassium diet Advice patient to avoid infection , trauma or stress, it increases the risk for addisonian crisis( IV hydrocortisone and saline soln for addisonian crisis) Anemia , aplastic Main Problem : Bone marrow hypoplasia or aplasia resulting in pancytopenia( decreased WBC, RBC and platelets) Initial manifestation – abnormal bleeding( purpura , petechiae, ecchymosis,epistaxis , melena and dyspnea) Laboratory data: decreased WBC , RBC and Platelet Count Nursing diagnosis: risk for infection; risk for injury Interventions: prepare the patient for bone marrow transplant Assess for signs and symptoms of bleeding Anemia , folic acid deficiency Main Problem : Depletion of folate, which results to progressive anemia Initial manifestation: fatigue Laboratory data: decreased folate levels Nursing diagnosis: activity intolerance Interventions: teach patient to increase sources of folic acid in the diet like: green vegetables ( asparagus, broccoli and spinach), yeast , liver , organ meats and fresh fruits. Avoid overcooking of vegetables Teach the patient regarding oral folic acid replacement Anemia , iron deficiency Main Problem : Decreased oxygen carrying capacity of the blood. The condition is usually associated with nutritional deficiency of iron Initial manifestation: easy fatigability; poor sucking ( infants) chubby but pale babies ( milk babies)] Laboratory data : decreased Hgb and Hct, microcytic, hypocromic RBC’s Nursing Diagnosis:Activity intolerance Interventions: Instruct patient to have frequent rest periods Increase iron in the diet( organ meat , egg yolk) milk is a poor source of iron Administer oral iron supplements as ordered Anemia , Pernicious Main Problem : Reduced vitamin B 12 Absorption due to the absence of the intrinsic factor usually related to gastrectomy and atrophy of the gastric mucosa Initial manifestation : Fatigue ; beefy red tongue or glossitis a common sign Laboratory Data : Schillings test reveals low value urinary excretion of ingested vitamin B12 < 10% in 24 hours Nursing Diagnosis : Activity Intolerance Nursing interventions : Teach patient monthly IM Vit B12 injections for life. Inform patient to report tingling sensation in the lower extremities indicating complication – peripheral neuropathy ANAPHYLAXIS Main Problem : Dramatic widespread acute atopic/allergic reaction which causes vascular collapse Initial manifestation : Sudden onset of rapidly progressive urticaria , respiratory distress and hypotension which can lead to shock Diagnostic data : Skin testing to determine allergen Nursing Diagnosis : Risk for altered airway clearance related to bronchial edema Nursing Intervention : Observe for respiratory complications (laryngeal edema ), watch out for signs and symptoms of shock. Maintain airway patency – prepare suction and intubation set Early stages – no loss of consciousness – epinephrine IM with loss of consciousness – epinephrine IV CPR for cardiac arrest After emergency give antihistamines [diphenhydramine(Benadryl) ] and corticosteroids Prevent recurrence by avoiding exposure to known allergens 1) A major nursing responsibility prior to initial administration of antibiotics specifically penicillin and sulfa drugs is : a) Skin testing b) Assessing for sensitivity to iodine c) Assessing for food allergies d) Suction equipment at bedside Answer : a - antibiotic therapy is done after negative skin test results to prevent occurrence of hypersensitivity reactions Aphasia Main problem an acquired disorder of communication resulting from brain damage.Speech difficulty /change usually caused by right sided hemiplegia(left brain involvement) Initial manifestations : Expressive Aphasia – difficulty expressing self in understandable speech Receptive Aphasia – does not comprehend spoken or written word Global Aphasia – combination of both Nursing Diagnosis : Impaired Verbal Communication Interventions : Give the patient enough time to speak and respond and speak clearly and slowly while facing patient Provide visual cues like pictures and gestures when talking to the patient ( verbal and non-verbal) Approach on the visually unaffected side Arrythmias Main Problem : Abnormal electrical conduction or automaticity changes in the heart rate or rhythm which affects cardiac output and blood pressure Initial manifestation : Hypotension and deteriorating level of consciousness Diagnostic Data : ECG tracing reveals the following: Atrial Fibrillation- irregular atrial rhythm > 400 beats / min. indiscernible PR interval and no P waves Ventricular Tachycardia- ECG shows rate of 140 – 220 bpm, wide and bizarre QRS complex and no P waves Ventricular fibrillation - ECG shows rapid and chaotic ventricular rhythm, wide and irregular QRS complexes and no visible P waves. Premature Ventricular Contractions- irregular intervals between QRS complexes Asystole – no atrial or ventricular rate Nursing Diagnosis : Ineffective tissue perfusion: cardiopulmonary Decreased cardiac output Nursing Interventions : Watch out for hypotension and decreased urine output Assist with measures to treat underlying cause ( electrolyte replacement , oxygen therapy and pulmonary care) Hook on cardiac monitor and assess Level of consciousness, RR, PR , BP and fluid and electrolyte balance Perform ACLS measures Early defibrillation for VT and VF Cardioversion for atrial dysrhythmias Administer antiarrythmics (Lidocaine,Inderal,Cordarone) for arrythmias and PVC’s – hypotension common side effect Perform CPR and intubation prn prepare patient for possible pacemaker insertion 1) In a patient on antidysrhythmic drug therapy , the following intervention is necessary to monitor for the common side effect of the drug: a) Use of infusion pump for continous administration b) Ensure IV remains patent and check insertion site c) Check BP regularly d) Administer slowly and at a prescribed rate Answer : c – major side effect of anti arrthmics is hypotension Angina Pectoris Main Problem _ Insufficient coronary blood flow results to inadequate oxygen supply causing intermittent chest pain Initial Manifestation : squeezing , burning , pressing , chocking , aching or bursting left sternal chest pain lasting not more than 20 minutes. The patient often says , “It feels like gas or heartburn or indigestion “ . Laboratory Data : ECG reveals ST segment depression Nursing Diagnosis : Pain Administer nitroglycerine sublingually to relieve the pain. Teach the patient that a burning sensation under the tongue after nitroglyvcerine indicates that the drug is potent. The drug may also cause facial flushing or headache Prepare patient for PTCA ( percutaneous Transluminal Coronary Angioplasty ) by informing the patient that a balloon tipped catheter will be introduced through a guide wire into a coronary vessel . Appendicitis MAIN PROBLEM : Inflammation of the appendix due to obstruction of the intestinal lumen Initial manifestation : right lower quadrant abdominal pain with rebound tenderness. Lessenignof pain indicates rupture of the appendix Laboratory Data : Elevated WBC and urinalysis negative for UTI ( ruled out ) Nursing Diagnosis : Pain and Potential for injury Interventions : Place patient in any position of comfort if appendix has not yet ruptured , if it is ruptured place patient in high fowler’s position to prevent upward spread of infection. Administer antibiotics as ordered . Avoid applying hot compress on the RLQ . No analgesics , antispasmodics and enema during observation phase. Prepare patient for appendectomy and teach post op interventions/responsibilities. Arthritis , gouty Main Problem : Metabolic disorder of uric acid formation and excretion Initial manifestation : Initially asymptomatic . A common sign is dusky red hot swollen joint(inflamed painful), usually the big toe. Pathognomonic : Formation of Tophi Laboratory Data : Elevated urate crystals in synovial fluids and elevated serum uric acid Nursing Diagnosis : Pain Interventions : Teach patient to Maintain purine restricted diet ( avoid organ meats , alcohol , legumes, sardines). Increase oral fluid intake Avoid aspirin and diuretics as these interfere with uric acid excretion. Alkalanize urine – fruit, vegetables and milk. Use bed cradle to prevent linen from coming in contact with the inflamed joint which aggravates the pain Common Complication : Uric Acid Kidney stone formation Encourage compliance to anti gout medications: Allopurinol- blocks formation of uric acid, Colchicine – analgesic and anti-inflammatory, Probenecid – reduces uric acid Sulfinpyrazone – reduces uric acid in the blood Arthritis , osteo Degeneration of the articular cartilage in the joints Initial Manifestation : Pain and swelling in a weight bearing joint, usually aggravated by activity Laboratory Data : X – ray Nursing Diagnosis : Pain Interventions : Priority : Minimize Discomfort – Implement: W- eight control H- ot compress or ice packs A – spirin use T – runk assistive devices – cane Arthritis , Rheumatoid Main Problem : systemic recurrent inflammation of the synovial lining of the joints, usually upper extremities.More common in women Initial manifestation : Morning stiffness relieved by warm bath or soaks Laboratory Data : elevated ESR and (+) rheumatoid factor Nursing Diagnosis : Pain related to joint inflammation Interventions : Teach patient to take aspirin regularly as ordered even in the absence of symptoms , instruct the patient that tinnitus is a side effect of aspirin. Apply moist heat for 15 – 30 minutes to reduce muscle spasm. Use ice packs during acute phase to decrease pain Asthma Main Problem : Abnormal Bronchial hyperactivity to certain substances and conditions Initial manifestation : dyspnea and wheezing(asymptomatic between attacks) Laboratory data : PFT’s during attacks show decreased forced expiratory volumes , elevated immunoglobulin E , ABG reveals respiratory Acidosis, peak flow levels below normal Nursing diagnosis : Ineffective Breathing Pattern related to bronchospasm Interventions : Assess precipitating factor and eradicate these sources Instruct patient to avoid 3 E’s ( exercise specially in cold weather, environmental factors like dust , emotional factors ) Position patient in orthopneic position and encourage patient to do pursed lip breathing Administer medications – Bronchodilators and corticosteroids usually via nebulization Autonomic dysreflexia Main Problem : Exaggerated autonomic responses to local stimuli below the level of the spinal cord injury. Occurs in clients with lesions above T6 after spinal shock has subsided Initial manifestation : Pounding headache or severe hypertension Nursing Diagnosis : Urinary retention related to effects of spinal cord injury Interventions : Catheterize the patient to prevent bladder distention. Relieve fecal impaction and pressure on skin which can precipitate attacks . Place patient in sitting position to help lower blood pressure . Administer antihypertensives Benign prostatic hypertrophy Main Problem : enlargement of the prostate gland resulting to narrowing of urethral opening Initial manifestation : decreased force and amount of urine Laboratory data :elevated Ph of prostatic fluid rectal examination shows enlarged prostate Cystoscopy shows enlarged prostate gland, obstructed urine flow and urinary stasis Nursing Diagnosis: Altered bladder elimination related to enlarged prostate Interventions : Force fluids Pre-op – assess understanding of procedure and anticipated postoperative course. Explain TURP ( Transurethral Resection Prostatectomy) will not involve any incision. Post – op assess for pain , discomfort and complications ( bleeding and infections ) Monitor continous bladder irrigations Bleeding Esophageal Varices Main Problem : bleeding of dilated veins in the lower esophagus Initial manifestation : Hematemesis Nursing Diagnosis : Fluid Volume Deficit Interventions : Monitor the pateint’s airway Assist with the insertion of Sengstaken – Blakemore Tube ( keep a pair of scissors at the bedside, this is used to cut the port of the tube leading the balloon, to deflate it, in case aspiration occurs) Bronchiectasis Main Problem : Chronic abnormal dilation of bronchi and destruction of bronchial walls leading to multiple respiratory complications Initial Manifestation : Chronic cough that produces copious, foul smelling, mucopurulent secretions, possibly totaling several cupfuls daily Laboratory Data : Bronchoscopy helps identify source chest x-ray shows peribronchial thickening, areas of atelectasis and scattered cystic changes Pulmonary Function tests detect decreased volumes Nursing Diagnosis : Ineffective airway clearance related to secretions Impaired gas exchange related to alveolar exudate Nursing Interventions :Assess respiratory status and level of consciousness to detect early signs of hypoxia and decompensation Administer antibiotics as necessary Teach and perform Respiratory Physiotherapy - deep breathing and coughing, postural drainage and chest percussion(done early morning and before bedtime) Teach importance of quitting smoking and avoidance of milk products 1) Priority nursing diagnosis for patient with bronchiectasis is: a) Altered breathing pattern b) Potential for infection c) Knowledge deficit d) Ineffective airway clearance Answer: d - copious, foul smelling, mucopurulent secretions, possibly totaling several cupfuls daily Buergers disease ( thromboangitis Obliterans ) Main Problem : Vasculitis of the small and medium sized veins and arteries usually in the lower extremities. It is more common in men and in smokers Initial manifestation : Pain is an outstanding symptom, intermittent claudication is a common problem Laboratory Data : leg arteriography reveals inflammatory lesions Nursing Diagnosis : Altered peripheral Tissue Perfussion Interventions : Instruct patient to stop smoking and administer calcium channel blockers and peripheral vasodilators as ordered. Burns Main Problem : Traumatic injury caused by thermal , electrical , chemical or radioactive agents Initial Manifestations : 1st Degree – pinkish skin with pain 2nd degree – reddish with painful blisters 3rd degree – eschar , charred , painless Laboratory Data : Hyperglycemia , anemia Nursing Diagnosis : Decrerased cardiac output related to fluid shifts Interventions : On strict MIO . Administer fluids as ordered during acute phase by fluid replacement calculations using body weight multiplied by BSA burned based on rule of nines. ½ of the total volume to be infused on the first 8 hours then the remaining ½ infused in the next 16 hours. Maintain a high calorie , high protein diet Treat pain with IV narcotics, provide tetanus prophylaxis and topical antimicrobial therapy. Institute reverse isolation in severe cases. Administer pain medications prior to ROM ,ambulation and whirlpool therapy Cancer , Bladder Main Problem : Presence of malignant cells in the bladder Initial Manifestation : Painless hematuria Laboratory data : Elevated Acid Phosphatase Nursing Diagnosis: Altered urinary Elimination Interventions : Prepare patient for surgery and chemotherapy Encourage patient to verbalize fears Cancer Breast Main Problem : Presence of malignant tumors usually in the upper outer quadrant of the left breast. It is associated with nulliparity or having the first child after age 35 Initial manifestation : skin dimpling and edema(peau d’ orange .Painless mass most common sign Laboratory Data : Mammography reveals the presence of non – palpable lesion. Baseline mammography should be made between age 35 – 40 . Q2 years 40 – 50 years old if w/o predisposition ;yearly for high risk women;yearly after age 50. Nursing Diagnosis : Knowledge deficit of breast cancer and mastectomy Interventions : Prepare patient for chemotherapy , radiation and surgery. Teach patient how to perform Self Breast examinations. Done monthly , a week after menstruation since the breast are less tender at this time. The best position is lying down with pillow under shoulder of breast being examined. Inform the patient that Mammography will involve placing the breasts between two X-ray plates. Avoid use of deodorant ,lotions or powder In post mastectomy patient elevate affected arm to prevent lympedema and to avoid activities that increase infection like gardening and sewing. No BP taking , venipuncture and constrictive clothing on the affected arm Cancer , Cervix Main Problem : presence of malignant cells in the cervix associated with multiple sexual partners and history of sexually transmitted disease Initial manifestation : initially asymptomatic , postcoital bleeding is common manifestation Laboratory data : pap smear reveals presence of malignant cells Nursing Diagnosis : Knowledge deficit of cervical cancer and chemotherapy Interventions : Instruct patient to avoid douching and sexual intercourse 24 hours before Paps’ Smear Stress the importance of lifelong follow up visits to detect response to treatment. Prepare patient for chemotherapy , radiation and surgery Cancer , Esophagus Main Problem : Malignant tumor in the esophagus related to alcoholism and smoking Initial manifestation : Dysphagia – presenting symptom Laboratory Data : Barium Swallow with fluoroscopy reveals large masses. CT scans may be employed to evaluate extent of tumor Nursing Diagnosis : Altered Nutrition Interventions : Prepare patient for surgery , radiation therapy and chemotherapy. Administer antacids and analgesics as ordered Prepare patient for tube or gastroctomy feedings and short course hyperalimentation Post operatively instruct patient to avoid overeating raw fruits and vegetables Cancer ,Larynx Main Problem : presence of malignant cells in the larynx associated with smoking and alcoholism Initial Manifestations : Hoarseness or voice change, tickling sensation in the throat Laboratory data : Laryngoscopy and Biopsy reveals malignant cells Nursing Diagnosis : Knowledge deficit of laryngeal cancer Interventions : Prepare patient for radiation , chemotherapy and surgery . teach patient to avoid cold air Instruct patient that swimming is not recommended post – laryngectomy. Institute alternative modes of communication Cancer , Ovary Main Problem : Gynecologic cancer associated with high fat diet and nulliparity Initial Manifestation : Initial asymptomatic , vague abdominal discomfort like indigestion is a common symptom Laboratory data : laparoscopy and Ultrasound reveals the presence of mass Nursing Diagnosis : Pain Interventions : Prepare patient for surgery and chemotherapy Assist the patient to cope with change in body image Institute effective pharmacologic and non pharmacologic pain management Cancer , Prostate Main Problem : Malignant tumor in the prostate gland Initial Manifestation : Decreased size and force of urinary stream Laboratory data : Elevated Prostate Specific Antigen ( PSA ) , elevated acid phosphatase Nursing Diagnosis : Pain related to tumor metastases to bone Interventions : Support patient undergoing radiation therapy Inform the patient that radical prostatectomy, which involves the removal of the entire prostate gland, may cause impotence Cancer , colon( colorectal Ca) Primary or metastatic malignant tumor of the colon or rectum which infiltrate causing obstruction, ulceration and hemorrhage. Change in bowel habits, character of stools, diarrhea and constipation- fecal oozing ( melena or hematochezia) Barium enema locates mass, sigmoidoscopy / colonoscopy identifies and locates mass, positive for fecal occult blood and positive biopsy for Ca cells Altered bowel elimination Assess GI status, fluid and electrolyte studies, monitor for bleeding , infection and electrolyte imbalance Provide post-chemotherapeutic and post radiation therapy nursing care Provide adequate nutrition and administer antiemetics and anti - diarrheals Prepare for surgery and Teach ostomy self care Administer TPN as ordered 1) Among the following diagnostic results ,which is more suggestive of colorectal cancer? a) Painless hematuria b) Presence of occult blood in stool c) Increased level of acid phosphatase d) Indigestion Answer: b – lab test suggestive of colorectal cancer includes fecal occult blood and positive biopsy for Ca cells Cancer , lung ( Bronchogenic Ca ) Development of a neoplasm in the respiratory tract(squamous cell-slow growing; large and small oat cell – fast growing).Presence of malignant tumor in the epithelium of the respiratory tract usually related to smoking or exposure to asbestosis Chronic,nagging cough ( smokers cough) Sputum cytology positive for cancer cells CXR shows a lesion or mass Bronchoscopy confirms a positive biopsy Impaired gas exchange Impaired breathing pattern Monitor respiratory status and pulse oximetry Check for cyanosis suggesting respiratory failure and increase in sputum production indicates infection Provide adequate pain control Increase oral fluid intake and IVF as ordered Provide increased CHON, high caloric diet( TPN or enteral,prn) Perform and teach Respiratory Physiotherapy Provide rest periods and mouth care Prepare patient for surgery and chemotherapy Elevate head of bed to prevent fluid collection in the upper body 1) All the following except one are diagnostic procedures done to confirm bronchogenic cancer: a) Sputum cytology b) Chest X- ray c) Bronchoscopy d) Pulmonary angiography Answer : d - pulmonary angiography is the rapid injection of radiopaque dye into the pulmonary circulation useful in determining the site of pulmonary embolism, sputum cytology, CXRay and bronchoscopy are tests done to confirm lung cancer. Cancer, Skin Malignant primary tumor of the skin mainly caused by prolonged exposure to the sun or other carcinogenic agents Squamous cell carcinoma- small red nodular lesion that begins as an erythematous macule or plaque Skin biopsy shows positive cytology Impaired skin integrity Assess lesion and monitor skin punch test site for bleeding Pre and post chemotherapy or radiation therapy nursing care Teach patient to avoid contact with chemical irritants. Use sunblock and layered clothing when outdoors 1) Nursing interventions for patients undergoing radiation therapy include all of the following except: a) Monitoring the punch test site for bleeding b) Teach patient to avoid contact with chemical irritants c) Using sunblock when outdoors d) Using layered clothing when sun exposure is possible Answer : a - skin punch test / skin biopsy is a diagnostic procedure to confirm the presence of skin cancer Cancer , Testicular Main Problem : Malignancy in the testes usually associated with cryptorchidism Initial manifestations Painless swelling and enlargement of the testes , accompanied by sensation of heaviness in the scrotum Laboratory data : Elevated HCG and alpha feto protein Nursing Diagnosis : Knowledge deficit Interventions : Prepare patient for surgery and chemotherapy Teach patient about testicular self examination .It should be done once a month while having warm bath or standing in front of mirror. Suspect cancer when spongy upon palpation Cardiogenic shock Main Problem : Extensive damage of the left ventricle due to Myocardial Infarction Initial manifestation : decreased systolic pressure Laboratory Data : Elevated BUN , creatinine and liver enzymes Nursing diagnosis : Altered cardiac Output ( decreased related to impaired contractility of the heart Interventions : Monitor BP , MIO and weight . Evaluate serum electrolytes for hyponatremia and hypokalemia Cataract Main Problem : Opacity of the lens usually associated with aging , prolonged intake of steroids and chromosomal aberrations Initial manifestation : painless blurring of vision Laboratory data : Slit lamp test reveals milky white color of the pupils Nursing diagnosis : potential for injury related to visual loss Interventions : Prepare patient for surgery Postoperatively instruct patient to avoid activities that requires bending, report sudden eye pain, this indicates hemorrhage and increased IOP. Avoid lifting and rapid head movements Position in fowlers position or instruct patient to lie down on the unaffected side Cerebrovascular Accident (CVA) Sudden loss of brain function resulting from a disruption of blood supply to a part of the brain causing temporary or permanent dysfunction.(TIA warning sign of CVA – no neurovascular deficits / complete resolution of manifestation within 24 hours) Initial Manifestation : depends on the site of brain involvement Middle cerebral artery : hemiparesis Internal Carotid artery : hemiplegia Right hemispheric lesion : spatial disorientation Left Hemispheric lesion : language disturbances Common manifestations: Hemiplegia and homonymous hemianopsia Emotional and personality disturbances Aphasia Dysphagia Laboratory : Elevated Cholesterol Levels Nursing Diagnosis : Ineffective Breathing Pattern Unilateral Neglect Interventions : Maintain adequate airway Institute regular bowel and bladder training Establish means of communication Chest injury (Flail Chest ) Main Problem : Loss of stability of chest wall with subsequent respiratory impairment Initial manifestation : Dyspnea , Paradoxical Chest Movement may occur ( detached part of the chest will be pulled in on inspiration and blown out on expiration ) Laboratory data : X ray reveals rib fractures Nursing Diagnosis : Ineffective breathing pattern Interventions : Stabilize the flail portion of the chest with hands or cover with impermeable dressing with three sides taped Turn patient on affected side to provide space for the unaffected lung to reexpand Place 10 pound sandbag at the site of flail Cholecystitis / Cholelithiasis Infection of the biliary tract associated with the presence of gallstones (Cholelithiasis) . Predisposing factors includes Fat, Female, Age Forty and above, and Fair skinned. Intolerance to fatty foods and severe pain located on the RUQ of abdomen radiating to R scapula with nausea and vomiting. Indigestion, flatulence, belching, jaundice and clay colored stools Hepatobiliary tract UTZ Altered nutrition ; less than body requirements Position in semi-fowlers,provide rest and limit activity Small frequent meals low fat, low calorie, high carbohydrate and fiber , no gas forming foods. NPO on acute phase. Administer IV fluids / TPN as ordered Prepare client for Extracorporeal Shock Wave Lithotripsy or cholecystectomy- T – tube for biliary drainage placed Teach post-op procedures and care(incentive spirometry and deep breathing) Give medications as ordered: Analgesics-Demerol ( morphine contraindicated) Antibiotics-Ceftazidine, Clindamycin , Gentamycin Anticholinergics- Probanthine Anti-emetic- Compazine Anti-pruritic- Benadryl NGT to low suction to decompress stomach 1) Management for patient post cholecystectomy includes: a) Adequate fat diet b) Maintain NPO for 3 days c) Place patient in supine position d) Instruct and encourage use of incentive spirometry Answer : d – management for clients post cholocystectomy includes maintaining high fowlers position, deep breathing and coughing, pain management, NPO until peristalsis returns, administer IVF and T – tube monitoring and care. Cardiac Tamponade Main Problem : Fluid Accumulation in the pericardial sac Initial Manifestation : hypotension muffled heart sounds is a common sign Laboratory data : ECG reveals ST and T wave abnormalities Nursing Diagnosis : Altered cardiac Output Interventions : prepare the patient for pericardiocentesis. Tjis involves aspirating the fluid or air from the pericardial sac. Assess for complications Cor pulmonale A chronic heart condition, is the hypertrophy of the heart, right ventricle and associated structure that results from diseases affecting the function and the structure of the lungs Chronic productive cough , dyspnea on exertion, edema and fatigue ABG- decreased Pa O2 < 70 mmHg CXR and UTZ – suggests R ventricular hypertrophy ECG- shows arrhythmia during severe hypoxia Altered Tissue perfusion related to cardiopulmonary changes Measure ABG levels and administer O2 by mask or cannula as ordered. Monitor serum K if on diuretics Low salt , fluid restricted , small frequent feedings Monitor digoxin level and check radial pulse prior to cardiac glycoside administration to avoid complications Reposition and provide meticulous respiratory care 1) Then following are diagnostic tests done to assess the presence of cor pulmonale except: a. CXR b. ECG c. UTZ d. Venogram Answer : d – insertion of a dye into a vein for the purpose of outlining an obstruction or lesion. Chronic Bronchitis ( Blue Bloater ) Main problem : excessive mucus secretion with the airways and recurrent cough usually related to smoking , pollution and infection. Initial Manifestation : Cough with copious sputum Laboratory data : ABG reveals respiratory acidosis Nursing Diagnosis : Impaired breathing pattern Interventions : Increase Humidity Provide postural drainage before meals Relieve bronchospasm Teach the patient about breathing techniques like : blowing bubbles , blowing a trumpet , blowing a feather in the air Complete Heart Block Main Problem : altered transmission of wave impulses from the SA node to the AV node Initial Manifestation : Bradycardia Laboratory data : ECG reveals prolonged PR interval Nursing Diagnosis : Altered tissue perfusion Interventions : Monitor patients’ ECG Prepare patient for pacemaker insertion A common sign of pacemaker failure is hiccups Atropine Sulfate is given as a vagolytic Congestive Heart failure Main Problem : failure of the heart to pump blood to meet oxygen requirements. Initial manifestations : Right sided edema , hepatomegaly Left sided : dyspnea , rales Laboratory data : Elevated CVP above 12 mmHG for right sided failure. Elevated PAP and PCWP for left sided failure Nursing diagnosis : altered cardiac output related to impaired contractility Interventions : Maintain patient in semi – fowlers position Administer digitalis and diuretics as ordered Maintain low sodium and low cholesterol diet Monitor potassium levels Crohn’s Disease ( Regional Enteritis) Main Problem : Chronic Inflammatory Disease of the small intestines Initial manifestation : Crampy abdominal pain in the right lower quadrant of the abdomen Laboratory data : Barium Swallow reveals “string sign” Nursing Diagnosis : Pain and alteration in bowel elimination ;diarrhea Interventions : Maintain high protein , high carbohydrate , low fat diet Administer steroids as ordered Provide small frequent feeding Monitor input and output Cushing ‘s Syndrome Main Problem : Hypersecretrion of the glucocorticoids by the adrenal glands Initial Manifestation : Central type or truncal obesity with thin extremities, moon face , buffalo hump and hirsutism Laboratory data : Elevated serum cortisol levels, hypernatremia , hypokalemia , hypertension , hyperglycemia Nursing Diagnosis : Altered skin integrity related to impaired healing Interventions : Maintain patient on high potassium and low sodium diet Instruct patient that treatment will involve lifelong administration of glucocorticoid synthesis inhibitors ( Mitotane ) Inform patient about slow wound healing Cystitis Main problem : inflammation of the urinary bladder Initial Manifestation : Frequency and Urgency Laboratory data : Culture and sensitivity tests reveal the presence of bacteria usually E coli Nursing diagnosis ; Altered Urinary Elimination Interventions : Increase Oral Fluid Intake Instruct the patient to avoid bubble baths , silk underwear. Cotton underwear is preferred. Maintain acid ash diet ; (cheese , cranberry , prunes , plums , poultry , eggs) Diabetes Mellitus Main Problem : Chronic disorder of cardohydrate , protein and fat metabolism characterized by an imbalance between insulin supply and demand. Type 1 – IDDM ( no insulin ) ; Type 2 – NIDDM ( little insulin or insensitivity of cells to insulin) Initial manifestation : Polyuria , Polyphagia , Polydipsia and weight loss Laboratory data ; elevated FBS level above 120 mg / dl Nursing Diagnosis : Alteration in nutrition Interventions : D-IET : 50-60%cho , 20-30% FATS , 10-20% CHON I – NSULIN – TYPE 1 A – NTIDIABETIC AGENTS –TYPE 2 B – LOOD SUGAR MONITORING E - XERCISE T – RANSPLANT OF PANCREAS E – NSURE ADEQUATE FOOD INTAKE S – CRUPULOUS FOOT CARE STRICT MONITORING FOR COMPLICATIONS( DKA for IDDM and HHNKS for NIDDM) Diabetes Insipidus Main Problem : Hyposecretion of antidiuretic hormone Initial manifestation : Polyuria , polydipsia Laboratory data : fluid deprivation test confirms the disorder Nursing Diagnosis : Fluid Volume Deficit Interventions : Maintain Adequate fluid intake Monitor urine specific gravity Administer Desmopressin acetate or Vasopressin intranasally as ordered Dementia , Alzheimers Irreversible progressive impairment in the patients cognitive functioning, memory and personality Confusion, easy forgetfulness and memory loss( cannot retain or recall recent information)( confabulates to cover up memory loss) Cognitive assessment- deterioration of cognitive ability Mental status exam – reveals disorientation and recall difficulty. Functional Dementia Scale shows some degree of dementia Cortical atrophy seen on MRI / CT scan Altered thought processes Group therapy and increase social interaction - reminiscence therapy to increase self esteem ) Provide for a safe , highly structured environment. Maintain consistency and provide constant orientation When agitated – redirect focus Simplify communications , tasks and routines Diet adequate in folic acid and provide adequate fluids and nutrition Palliative medical management with: Anticholinesterase – Tacrine(Cognex), Donepezil (Aricept) Antipsychotics, Benzodiazepines,Antidepressants and Vitamin E supplements 1. Clinical manifestations more typical of dementia include all of the following except: a. wandering:becoming lost b. impairment of cognitive functioning c. memory impairment d. no personality changes answer : d - in dementia there is personality changes that interfere with ADL. Delirium Acute reversible disturbance of consciousness accompanied by a change in cognition not attributed to pre-existing dementia lasting several hours or days Altered psychomotor activity such as apathy, withdrawal and agitation with disorientation Result of a physiologic condition, metabolic imbalance, intoxication, substance withdrawal, toxic exposure, prescribed medicines or combination . No specific laboratory test. Multiple tests to rule out or confirm underlying factors Altered cerebral perfusion and high risk for injury Assess and correct underlying physiologic problem Create a structured safe environment Decresase sensory stimulation and administer medications as ordered: Tranquilizer Benzodiazepines Cholinesterase inhibitors Antipsychotics Risperidone(risperdal) 1) Clinical manifestations not typical of delirium : a) Slowed thought processes , confusion and disorientation b) Misperception of stimuli and incoherent speech c) “ sundowner’s syndrome” and dream like state d) memory impairment , aphasia and apraxia answer : d - memory impairment , aphasia and apraxia more associated with dementia Compartment Syndrome Pressure within a muscle and its surrounding structures increases causing circulation impairment or interruption caused by application of dressing, tight casting, burns, closed fractures and crushing injuries Pain increased with stretching and unrelieved by narcotic analgesics Paresthesias, pallor, pulseless and paralysis No specific diagnostic test Risk for peripheral neurovascular dysfunction Position the affected extremity lower than the heart to increase circulation to the area Bivalving or removal of dressings and constrictive coverings from area Monitor affected extremity and perform neurovascular checks. 1) In patient with complaining of intense pain on the casted extremity unrelieved by analgesics the nurse would : a) Ask the patient to wiggle the fingers or toes of the extremity b) The nurse would refer to patient to the AP for increase in narcotics c) check for distal pulses and elevate the extremity d) prepare the client for possible bivalving answer d : in compartment syndrome emergency bivalving is the most appropriate intervention done Disseminated Intravascular Coagulation ( DIC ) Main Problem : Wide spread coagulation all over the body resulting to subsequent depletion of clotting factors Initial Manifestation : petechiae and ecchymosis on the skin , mucous membrane , heart lungs and other organs Laboratory Data : Prolonged PT and PTT Nursing Diagnosis : Risk for Injury Interventions : Monitor for signs of bleeding ( tarry stool , hemoptysis , nosebleeding ) Administer heparin as ordered.heparin inhibits thrombin thus preventing further clot formation and allowing coagulation factors to accumulate. Administer Blood transfusion as ordered Instruct patient to avoid aspirin and aspirin containing compounds Diverticulitis Main Problem _ Inflammation of a pouch or saccular dilation in the colon ( diverticula) Initial Manifestation : Left lower Quadrant Pain Laboratory data : Sigmoidoscopy confirms the diagnosis Nursing Diagnosis : Pain Interventions : Provide Low Fiber Diet ( avoid vegetables) in diverticulitis, high fiber in Diverticulosis Administer Metamucil as ordered Administer meperidine for relief of pain Dumping Syndrome Main Problem : Rapid emptying of the stomach contents into the small intestine usually a complication of gastric surgery Initial manifestations : 3 D’s ( Diarrhea , Diaphoresis , Drowsiness) Laboratory data : non – specific Nursing Diagnosis : Altered Elimination Interventions : Maintain patient on supine position after Meals and withold fluids during meals Maintain high fat , high protein , dry diet, low in simple sugars ( fat delays emptying of the stomach Emphysema (Pink Puffer) Main problem : destruction of the alveoli , narrowing of small airways and trapping of air resulting in loss of lung elasticity Initial manifestation : shortness of breath ; barrel chest ( increase in anteroposterior diameter of the chest ) is a late sign Laboratory data : ABG reveals Respiratory Acidosis Nursing Diagnosis : Ineffective breathing Pattern Interventions : Keep the patient in orthopneic position / sitting Administer low flow oxygen Encourage patient to do pursed lip breathing Instruct patient to avoid powerful odors , extremes of temperature, pets , fireplace and feather pillows Endocarditis Main Problem : Infection of the inner lining of the heart caused by direct invasion of bacteria leading to deformity of the valve leaflets Initial Manifestation : Fever Laboratory data : elevated ESR Nursing Diagnosis : Altered Cardiac Output Interventions : Record daily weight Evaluate jugular vein distention, as this signifies the development of CHF Instruct the patient to take antibiotics before dental procedures that can cause bleeding Avoid sharing of needles Teach the women in child bearing years the risks of using IUD’s or other birth control ( source of infection ) Epileptic Seizure Main Problem : Abnormal sudden excessive discharge of electrical activity within the brain Initial Manifestation : Impaired Consciousness Laboratory Data : EEG ( abnormal brain waves ) , CT scan reveals brain lesions Nurisng Diagnosis : Altered tissue Perfusion Interventions: (On seizure precautions) Maintain Patent Airway Protect from injury Do not restrain Administer valium,drug of choice as prescribed ; & other anticonvulsants Oxygen equipment and suction at bedside Fractures Break in the continuity of the bone due to trauma, bone tumors and osteoporosis Acute pain, cyanosis, loss of function, swelling , deformity and crepitus Antero posterior lateral X-ray of the area Acute pain and impaired physical activity Rest Immobilize Cold compress and control bleeding Elevate Alleviate pain by giving adequate analgesics/narcotics except in presence of head injury Prepare patient for reduction and alignment ( Splinting , casting, application of traction and surgical fixation (CRIF/ORIF) Provide adequate care for clients with traction T-rapeze bar overhead R – equires free – hanging weights A – nalgesics is given to relieve pain C – heck circulation (pulse) T – emperature monitoring I – nfection prevention O – utput and intake monitoring N – utrition( appropriate diet) S – kin must be checked frequently 1) In management for fractures by closed reduction the bones are: a) Realigned through surgical means b) May involve removal of damaged bone c) Bone replacement with prosthesis d) Bones realigned without surgery and cast applied to hold bones in alignment Answer : d – closed reduction – bone realignment without surgery Glaucoma Main problem: increased intraocular pressure due to accumulation of aqueous humor Initial manifestation : Tunnel Vision , Gun Barrel Vision Closed angle – with pain Laboratory Data : Tonometer reading of 25 mm Hg and above Nursing Diagnosis : Potential for Injury related to visual impairment Interventions : Explain to the patient that glaucoma cannot be cured but it can be controlled Administer Miotics ( pilocarpine ) Mydriatics contraindicated(ATSO4) Instruct patient to avoid activities that can contribute to increased IOP Teach patient about trabeculoplasty – creation of an opening in the trabecular meshwork to increase the outflow of aqueous humor. Gastritis Acute and chronic inflammation of gastric mucosa causing edema, hemorrhage and erosion Abdominal cramping, epigastric discomfort, hematemesis and indigestion Occult blood in stool and vomitus, decreased Hgb and Hct Upper GI endoscopy confirms diagnosis when performed within 24 hours of bleeding Acute and chronic pain Risk for fluid volume defict Altered nutrition less than body requirements Give IVF and antiemetics. Monitor MIO Provide bland diet in smaller frequent meals Administer antacids(between meals) and H2 blockers to promote healing, anticholinergics and Vit B12 Angiography with vasopressin infused in NSS during bleeding Teach importance of smoking cessation , avoid spicy foods and caffeine, taking steroids with milk, foods or antacids and to avoid aspirin containing compounds 1) Complications of gastritis include a) gastric carcinoma and pernicious anemia b) bleeding and dehydration c) a and b d) b only answer : b - gastric carcinoma , pernicious anemia, bleeding and dehydration are complications of gastritis Guillain – Barre Syndrome Main Problem : acquired acute inflammatory disease of the peripheral nerves Initial Manifestation : ascending paralysis , weakness at first Laboratory Data :CSF exam reveals elevated total protein Nursing Diagnosis: Ineffective Breathing Pattern Interventions : Maintain a patent airway Monitor for respiratory involvement Instruct patient to avoid crowded areas Keep tracheostomy and suction equipment at bedside Hemophilia Main Problem : Deficiency of clotting factors. Sex –linked recessive trait ( type A and B ) more common in males. Von Willebrands disease is transmitted to both male and female offsprings of a carrier Initial Manifestation: Hemarthrosis ( bleeding joints) Laboratory Data : prolonged Bleeding Time Nursing Diagnosis: Altered tissue perfusion Interventions : Avoid Aspirin Control by : Rest Immoblize Cold Compress Elevate Hepatic encephalopathy / coma Main Problem : Decreasing level of consciousness related to accumulation of ammonia Initial manifestation : personality changes ; flapping tremors (asterexis) common sign Laboratory Data : Elevated serum ammonia Nursing Diagnosis : Altered Thought Process Interventions : Monitor LOC Maintain low CHON diet Hiatal Hernia Main Problem :A portion of the stomach is herniated through the esophageal hiatus of the diaphragm Initial Manifestation: initially asymptomatic , heartburn is a common complaint Laboratory Data: Endoscopy reveals herniation of a part of the stomach Nursing Diagnosis : Altered Nutrition Interventions : Maintain the patient in an upright position after meals Instruct patient to avoid bending Provide small frequent meals Avoid anticholinergic drugs and coughing Hip Fracture Main Problem : Break in the continuity of the hip bone Initial manifestation: Shortening and external rotation of the affected leg Laboratory : Hip X – ray Nursing Diagnosis : Impaired Physical Mobility Interventions : Prepare the patient for surgery Postoperatively maintain the legs in abduction by placing a wedge pillow between legs Monitor for signs and symptoms of complications ( petechiae over chest indicates fat embolism) Hyperparathyroidism Main Problem : hypersecretion of the parathyroid hormone Initial manifestation : bone pain Laboratory Data : elevated serum calcium levels Nursing Diagnosis : Risk for Injury Interventions : Prepare the patient for Surgery Increase oral fluid intake Provide low calcium diet Strain all urine Complication : renal calculi Hypertension Main Problem : Persistent BP above 140 / systolic and 90 / diastolic Initial manifestation : Asymptomatic , occipital headache is a common complaint Laboratory data : elevated BP Nursing Diagnosis : Altered Tissue Perfusion Interventions: Avoid Stimulants Low salt , low fat diet Stress reduction techniques Lifestyle , dietary and behavioral modification Compliance to HPN pharmacotherapy Specially maintenance meds Hyperthyroidism Main Problem : Hypersecretion of thyroid hormones Initial manifestation : Fine hand tremors , intolerance to heat is a common symptom Laboratory Data : Elevated T3 and T4 Nursing Diagnosis : Risk for Injury Interventions : Maintain a high calorie , High CHON Diet Provide adequate rest Provide acool environment Elevate head of bed Propylthiouracil medication is lifetime Prepare patient for thyroidectomy Post thyroidectomy – assess for hemorrhage by slipping the hand behind the neck Hyperlipidemia Increased serum levels of two plasma lipids; cholesterol and triglycerides above 200 mg/ dl. Factor causation of atherosclerosis and conductive to arteriosclerosis Initially asymptomatic Lipid Profile Test – elevated Non compliance to therapeutic regimen Instruct patient to eat salmon and tuna at least several times a week and increase intake of high fiber foods Administer antilipidemic drugs with meals – Clofibrate ( Atromid-S) and Cholestyramine ( Cuemid) 1) Management for patients with hyperlipidemia: a) Diet low in cholesterol and saturated fats b) Carbohydrate restricted diet c) A and b d) A only Answer : c – low saturated fat and low cholesterol diet can maintain serum cholesterol below 140 mg/dl. Carbohydrate restriction can lower serum triglyceride levels by reducing lipoprotein derived from carbohydrate Hypoparathyroidism Main Problem : Hyposecretion of parathyroid hormone Initial manifestations : Tingling sensation around the lips and upper extremities Laboratory Data : Decreased serum calcium levels Nursing Diagnosis : Potential ; altered cardiac output Interventions : Assess for increased signs of neuromuscular irritability ( Chvosteks’ and Trousseau’s Sign) Provide a quiet room , no stimulus Provide high calcium , low phosphorus diet Hypothyroidism Main Problem : Hyposecretion of thyroid hormone Initial Manifestation : Fatigue , facial edema is a common sign Laboratory Data : Decreased T3 and T4 levels Nursing Diagnosis : Activity Intolerance Interventions : Maintain low calorie , low cholesterol and low saturated fat diet Provide warm environment and avoid sedatives Provide frequent rest periods Instruct patient that administration of synthroid is lifelong Hypovolemic shock Main Problem : Loss of effective circulating blood volume leading to circulatory collapse resulting to inadequate tissue perfusion Initial manifestation : narrowing pulse pressure Diagnostic data ; Decreased BP and Decreased CVP Nursing Diagnosis : altered Tissue Perfusion Interventions : Maintain patent airway Keep patient in modified trendelenburg position Start fluid replacement immediately Administer vasopressors as ordered Hemorrhoids Varicosities or outpouching of the veins of the hemorrhoids plexus Internal- painless bleeding in defecation External – intense rectal itching with bleeding and pain upon defecation Rectal examination Pain related to irritation, pressure, sensitivity in recto-anal area Conservative treatment: Application of hot and cold compress Analgesic ointment(nupercaine) Hot sitz bath Prepare patient for treatment by ligation, injection of sclerosing agent or preop and post –op care for hemorroidectomy Position prone post hemorroidectomy, Watch out for hemorrhage 24 hours to 10 days post-op when sutures are sloughing off. Administer laxative, full diet until few hours before anesthetic is given. Stool softeners and bulk formers(Metamucil) Increase bulk and fluids 1) Post hemorrhoidectomy nursing care monitoring for potential complication includes observation for: a) Bleeding and urinary retention b) Bleeding and atelectasis c) Respiratory complications and urinary retention d) None of the above Answer : a – bleeding and urinary retention are possible complications of hemorrhoidectomy Increased intracranial pressure Main problem : increase in amount of CNS tissue or CSF fluid leading to an ICP greater than 15 mmHg Initial Manifestation : Widening pulse pressure , decreasing LOC Laboratory Data : elevated Blood pressure ( systolic) Nursing diagnosis : Potential for ineffective breathing pattern Interventions : Keep the patient in high – fowler’s position Administer dexamethasone and mannitol as ordered to decrease cerebral edema Monitor level of consciousness Liver Cirrhosis Main Problem : Normal liver tissues are replaced with scar tissues Initial manifestation : edema Laboratory data : elevated SGOT / SGPT ; AST / ALT Nursing Diagnosis: Altered Fluid Volume Interventions : Maintain A low protein diet Assess the patient for bleeding Prepare the patient for paracentesis Weigh the patient daily Asterixis indicates hepatic encephalopathy Meniere’s Disease Main Problem: Dilation of the endolymphatic system causing degeneration of the vestibular and cochlear hair cells in the inner ear . It affects cranial nerve VIII Initial Manifestations : Vertigo usually described by patients as “ I feel like I’m spinning “ , I feel as if the room is revolving “ Laboratory Data : Caloric Stimulation test reveals moderate nystagmus Nursing Diagnosis : Risk for Injury Interventions : Priority Safety Keep the patient in supine position during the attack Maintain low sodium diet Encourage the patient ot stop smoking Keep the room dark when photophobia is present Multiple Sclerosis Main Problem : Chronic Progressive disease of the CNS characterized by small patches of demyelination in the brain and spinal cord Initial Manifestations : Intentional Tremors and Diplopia Laboratory Data : MRI reveals small plaques scattered throughout the CNS Nursing Diagnosis : Impaired Physical Mobility related to nuscle weakness ; Risk for injury Interventions : Promote safety of the client Teach the patient certain stress management techniques Encourage daily exercise Myasthenia Gravis Main Problem ; Faulty Neuromuscular transmission of the voluntary muscles of the body due to a deficiency in acetylcholine receptor sites in the myoneural junction Initial Manifestation : Descending muscle weakness initially manifested by ptosis Laboratory Data : CT scan reveals hyperplasia of the thymus gland. Tensilon test ; increased muscle strength 30 seconds after administration of Endrophonium Nursing Diagnosis : Ineffective Breathing Pattern Interventions : Maintain Patent Airway Instruct the patient to avoid quinidine , morphine and antibiotics since these may trigger muscle weakness. Instruct the patient to avoid prolonged talking over the phone especially before meals since this will weaken the facial muscles which are also used for eating. Intestinal obstruction Blockage of intestinal lumen causing gas, fluid and digested material substance to accumulate near the obstruction and increase peristalsis.H2O and electrolytes are then secreted into the blocked bowel causing inflammation and inhibiting absorption Abdominal distention, cramping pain, decreased or absent bowel sounds Abdominal X-ray – increased amount of gas in the bowel Acute pain related to abdominal distention Constipation related to inability of stool to pass through obstructed area Place patient on NPO and fluid and electrolyte replacement through IVF infusion Assess bowel sounds,mio,vs and labs- stoll exams and measure abdominal girth to assess for distention Semi-fowlers for comfort , bedrest and quiet envt. Administer analgesics( Demerol)and antibiotics(Gentamycin) Teach and monitor pre-op and post –op care for bowel resection with or without anastomosis Avoid constipating food GI decompression using NGT, Miller abbott or cantor tubes maintained position and low intermittent suction 1) The priority nursing diagnosis for patients with bowel obstruction are Constipation related to inability of stool to pass through obstructed area and: a) Fluid volume deficit, potential for b) Pain c) High risk for infection d) Potential for non – compliance Answer : b : pain is an immediate problem the other choices are potential problems. Myocardial Infarction Main Problem : Destruction of the cardiac tissue due to reduced coronary blood flow Initial Manifestation : lower sternal pain not relieved by rest and nitroglycerine , characterized as crushing or excruciating Laboratory Data : Elevated CPK and Troponin , ECG reveals ST segment elevation or depression and T wave inversion Nursing Diagnosis : Pain related to decreased tissue oxygenation Interventions: Morphine / Demerol to relieve pain Oxygen Administration Nitroglycerine Aspirin Position in semi-fowler’s Maintain low fat , low cholesterol and low sodium diet Osteoporosis Main Problem : Loss of bone matrix leading to bone weakness predisposing it to fractures. Usually associated with smoking , menopause , immobility and hyperparathyroidism Initial manifestation : asymptomatic Laboratory Data : X- ray reveals decrease in bone density Nursing Diagnosis : Potential for Injury Interventions ; Increase Vit D and Calcium in the diet Estrogen replacement therapy for post menopausal women Encourage patient to perform active weight bearing exercises like brisk walking , jumping rope , hiking , tennis and bal;lroom dancing. Swimming does not meet criteria for resistance needed for prevention of osteoporosis Metabolic acidosis state of excess acid accumulation and deficient base bicarbonate drowsiness and Kussmauls respiration, CNS depression, lethargy and stupor ABG reveals pH < 7.35 and HCO3 level < 24 mEq / L Impaired gas exchange Assess and correct underlying cause Watch out for increased serum potassium,frequent monitoring of vital signs , labs and level of consciousness Keep sodium bicarbonate ready and institute seizure precautions. Teach urine and blood tests for sugar or acetone. Encourage strict adherence to OHA or insulin therapy 1) Hyperglycemia in patients with IDDM can cause what metabolic imbalance: a) Metabolic acidosis b) Metabolic alkalosis c) All of the above d) None of the above Answer : a – excess production of metabolic acids such as hyrglycemia in patients with IDDM warrants use of fats which liberates ketone bodies which is a metabolic acid precipitates metabolic acidosis. Metabolic Alkalosis Clinical state marked by decreased amounts of acid and increased amounts of base bicarbonate Confusion, hypoventilation, irritability, picking at bedlinens and twitching ABG pH . 7.45 and Bicarbonate level > 28 mEq / L High risk for injury related to metabolic alkalosis Alteration in tissue perfusion and Impaired gas exchange Assess and Treat underlying cause Measure I and O and watch out for tachycardia and hypotension indicating hypokalemia Avoid the use of alkaline agents such as antacids, bicarbonate of soda and no administration of IVF with increased concentration of bicarbonate or lactate Acidifying agent- ammonium Chloride IV and potassium Chloride – supplements IV ( not given to clients with hepatic and renal diseases and given on slow infusions to prevent hemolysis) 1) Most appropriate nursing intervention to correct metabolic alkalosis is to: a) infuse Potassium chloride b) Use of antacids and bicarbonate of soda c) IVF with bicarbonates and lactate d) All of the above Answer : a - Infusion of acidifying agents are beneficial to counteract metabolic alkalosis Respiratory alkalosis Deficiency of CO2 in the blood as indicated by decreased PaCO2 caused by alveolar hyperventilation which elevates blood Ph. Deep rapid breathing > 40 bpm( cardinal) Circumoral or peripheral paresthesias Carpopedal spasms and lightheadedness ABG – Pa CO2 < 35 mHg Impaired gas exchange Ineffective breathing pattern Eradicate underlying condition by treatment of CNS disease, fever, sepsis or removal of ingested toxins Teach effective deep breathing into a paper bag Watch out for twitching and cardiac arrythmias Monitor ABG’S and serum electrolyte levels 1) Common management for respiratory alkalosis includes: a) Oxygenation by nasal cannula b) Oxygen delivery by face mask at 10 LPM c) Teach deep breathing in a paper bag d) Encourage patient to breathe deeply in a pursed lip manner Respiratory Acidosis Acid – base disturbance characterized by excess CO2 in the blood( hypercapnia) >45 mmHg resulting from reduced alveolar ventilation Restlessness and confusion ABG – Ph below normal < 7.35 ; pCO2 > 45 Impaired gas exchange Ineffective breathing pattern Monitor pulmonary function tests Prepare patient for intubation and /or mechanical ventilation if with hypoxemia, decreased level of consciousness and respiratory distress. Administer antibiotics, sodium bicarbonate and bronchodilators as needed Chest physiotherapy, suctioning and O2 with humidification Eradicate underlyingt cause by intubation and Mech. Ventilation, removal of foreign body and dialysis to remove toxic drugs. 1) Respiratory acid – base imbalance caused by retention of CO2 which combines with H2O to form carbonic acid H2CO3 includes the following disorders except: a) COPD and Asthma b) hyperventilation c) CNS depression d) Pulmonary edema and respiratory paralysis Answer : b – hyperventilation causes alkalosis Pancreatitis Main Problem : Autodigestion of the pancreas Initial Manifestation : Periumbilical Pain Laboratory Data : Elevated Serum Amylase Nursing Diagnosis : Pain Interventions : Administer Demerol to relieve pain. Morphine contraindicated as it causes spasm of the spincter of oddi Maintain low fat diet , patient on NPO during acute phase Instruct patient to avoid coffee and alcohol Parkinson ‘ s Disease Main Problem : Progressive Neurologic Disorder affecting the brain centers responsible for control and regulation of movement due to depletion of dopamine Initial manifestation : Bradykinesia Laboratory data : No Specific Nursing Diagnosis : Risk for Injury Interventions ; Maintain Exercise program Maintain a low protein diet at daytime and high protein at night because absorption of levodopa which is usually taken at daytime is slowed down by intake of high protein foods and vitamin B6 Institute safety measures ( rubber soled shoes , low heels and grab bars ) Prepare patient for stereotaxic thalamotomy , surgery done to decrease tremors Peptic Ulcer Disease , Duodenal Main Problem : Increased in HCL acid levels in the stomach Initial manifestation : Right Epigastric Pain which occurs 2-3 hours after meals usually at night and is relieved by eating Laboratory Data : Gastric Analysis reveals elevated HCL Nursing diagnosis : Potential for fluid volume deficit Interventions : Maintain high fat , high carbohydrate and low protein diet. Instruct patient to avoid spicy and caffeine containing foods , alcohol and smoking Peptic Ulcer Disease , Gastric Main Problem : Weak Gastric Mucosa Initial Manifestation : Left epigastric pain which occurs 30 minutes – 1 hour after meals usually at day time and is relieved by vomiting Laboratory Data : Endoscopy reveals ulcer usually in the lesser curvature of the stomach Nursing Diagnosis : Potential for fluid volume deficit Interventions ; Maintain High fat , high carbohydrate and low protein diet Instruct the patient to avoid spicy , caffeine containing foods , alcohol and smoking Administer antacids separately from other drugs that the patient is taking , as ordered. Prepare patient for surgery ( Billroth 1 , 2 or gastrectomy or vagotomy) Raynauds disease Main Problem : VAsospastic condition of arteries of the hands tha occurs with exposure to cold or stress Initial Manifestation : Intermittent arteriolar vasoconstriction Laboratory Data : Allen’s test reveals circulatory problems Nursing Diagnosis : Altered Tissue Perfusion Interventions : Avoid cold weather Wear leather gloves when getting anything from the refrigerator Stop smoking Administer vasodilators as ordered Renal Colic ( Urolithiasis) Main Problem : Presence of renal stone in the urinary system Initial manifestation : Sudden severe pain that leads to shock, unrelieved by analgesics Laboratory Data : IVP reveals the presence of stone Nursing diagnosis : Pain Interventions : Strain all patients urine , to assess if the patient is passing out stones Increase Oral Fluid Intake Prepare Patient for Extracorporeal Shock Wave Lithotripsy- area submerged in water and electrically generated shock wave directed to the location of the stone. Pain medications given to minimize pain Maintain patient on low sodium , low protein diet Renal Failure , Acute Main Problem : Abrupt reversible cessation of renal function as a result of trauma , allergy and kidney stones Initial Manifestation : Oliguria ( U.O. , 400 ml / 24 hours ) Laboratory data : elevated BUN and creatinine Nursing Diagnosis : Alteration in Urinary Elimination Fluid and electrolyte imbalance Interventions : Monitor Intake and output Maintain a low protein , high carbohydrate , low sodium diet and fluid restricted during the oliguric phase and high protein , high calorie and fluid replacement during diuretic phase Renal Failure , Chronic Main Problem : Irreversible slow or progressive failure of the kidneys to function that results in death unless treatment is instituted Initial manifestation : GI manifestations like anorexia , nausea and vomiting Laboratory Data : Elevated serum creatinine level and low urine creatinine clearance Nursing Diagnosis : Alteration in urinary elimination Fluid Volume Excess Interventions : Maintain low protein , low sodium , low potassium diet Prepare patient for hemodialysis / peritoneal dialysis and monitor for complications Monitor for signs and symptoms of anemia Administer Epogen , diuretics and antihypertensives as ordered Pulmonary Embolism Obstruction of blood flow to pulmonary vessels by an undissolved substance( air, fat, emboli,thrombus) resulting in pulmonary hypertension and possible iinfarction Sudden onset of dyspnea, tachypnea, crackles and chest pain ABG – hypoxemia; pulmonary angiography shows location of embolism and filing defect CXR – shows pneumoconstriction pulmonary arterial dilation Lung scan shows VQ mismatch Impaired gas exchange Ineffective tissue perfusion; cardiopulmonary Monitor ABG and watch out for respiratory distress and assess cardiovascular status and CVP Irregular pulse – arrhythmia caused by hypoxemia Hyperthermia – pulmonary embolism caused by thrombophlebitis Monitor lab studies – maintain PTT at 1 ½ to 2 times control in patient with heparin – PT at 1 ½ to 2 times control or INR at 2 -3 in patient receiving coumadin Place patient in fowlers position, suction and administer IVF, analgesics, anticoagulants, diuretics and fibrinolytics as ordered 1) The nursing diagnosis with least significance for patients with pulmonary embolism is: a) Altered pattern of breathing related to dyspnea b) Impaired gas exchange related to decreased diffusion c) Pain related to pleural irritation d) Anxiety related to hypoxia Answer : d – physiological needs first Pulmonary Edema A condition characterized by excessive amount of fluid in the alveoli and pulmonary interstitial tissues which tends to interfere with effective diffusion of gases Dyspnea, orthopnea, crackles paroxysmal nocturnal dyspnea and pink frothy sputum Pulmonary function tests decreased VQ ratios, ABG’s indicate hypoxemia Impaired gas exchange related to right to left shunting and decreased V/Q ratios Fluid volume excess related to left ventricular failure in cardiogenic pulmonary edema Decreased cardiac output related to left ventricular failure in cardiogenic pulmonary edema Monitor blood gases If on ventilator , suction frequently. Maintain oxygenation with ventilator( on PEEP) or nasal cannula Restrict fluids and sodium for edema Administer inotropic drugs(Dopamine and dobutamine) and diuretics in cardiogenic pulmonary edema Prevent pulmonary infection with strict asepsis Maintain nutrition with parenteral or enteral feedings 1) An example of a drug used in pulmonary edema to decrease circulating fluid volume a) Dopamine ( Intropin) b) Dobutamine ( Dobutrex) c) Lasix( Furosemide) d) Digoxin ( Digitoxin) Answer : c – furosemide is a diuretic which decreases fluid volume by increasing renal water excretion Pneumothorax A restrictive respiratory disease occurs when air enters the pleural space as a result of pulmonary lesion, neoplasms, accidental or surgical opening through the chest wall. Collapse of the lung due to air in the pleural space. Hemothorax – blood Hydrothorax – water Pyothorax – pus and exudates Acute symptoms of dyspnea and paradoxical chest movement( absent or restricted movement on the affected side with decreased or absent breath sounds , may lead to mediastinal shift) Lung scan shows VQ ratio mismatches CXR showing decreased perfusion ABG showing hypoxemia Impaired gas exchange Monitor PFT’s and prepare patient for thoracentesis and observe for complications of chest tube placements ( constant bubbling in the water seal chamber– indicates leak; 3 days post insertion can indicate lung re-expansion) Place patient in high fowlers position and place on O2 therapy as indicated. Instruct patient to do valsalva maneuver during chest tube removal. 1) The following are measures to promote adequate respirations and maintain proper function of the drainage bottle system: a) Prevent movement to prevent displacement of the tube b) Keep drainage bottles below chest level and position patient flat on bed c) Constant clamping of the tubes d) Milking not routinely done Answer : d – patient is positioned in semi- fowlers,drainage bottles below chest level, milking not routinely done as it increases negative pressure, clamping of the tube done only when bottles are broken or must be raised above the chest. Systemic Lupus Erythematosus Chronic autoimmune multi-system disorder with periods of exacerbation and remission and increased production of antibodies to cellular DNA results in inflammatory process involving veins and arteries causing pain swelling and tissue damage. Pancytopenia and butterfly rash on the face, palmar erythema, psychosis and impaired cognitive function migratory pain and swelling, hypertension & carditis Positive rheumatoid factor and ANA test positive ESR elevated and serum globulins elevated Urine chemistry – proteinuria and hematuria High risk for injury Diet high in iron , CHON, vita.C Hemodialysis and kidney transplant if renal failure occurs Increase rest and sleep Monitor musculo skeletal, renal and cardiopulmonary status Administer antiemetics , and antidiarrheals Encourage expression of body image change Avoid infections, injury, sunlight exposure, OTC meds, oral contraceptives, hair spray and color Give medications as ordered – analgesics , anti-emetics, anti-rheumatics, cytotoxic drugs, steroids and NSAIDS. 1) Complications of SLE includes peripheral vascular disease which can be a cause of a. Loss of limbs b. COPD c. Congestive heart failure d. Stroke Answer : a – PVD as a complication of SLE can lead to peripjeral tisuue necrosis which warrants amputation Urinary Tract Infection Infection of the urinary tract as a result of urethral ascend of bacteria usually caused by E. Coli. Cystitis – inflammation of the urinary bladder Pyelonephritis inflammation of the kidney and its pelvis Flank pain, with frequency,burning and urgency Chills , muscle spasm, dysuria Urinalysis and urine C/ S confirms causative agent Pain alteration in comfort Stress the importance of medication compliance and bedrest during acute phase Relieve flank pain with analgesics , rest massage and external heat application Sulfonamides and broad spectrum antibiotics, urinary antiseptics ( Bactrim , Septra) and urinary analgesics ( Pyridium) Increase oral fluid intake up to 4 liters per day and follow up urinalysis every two weeks for a month then monthly until urine is sterile. 1.)the following statement is true about pyelonephritis except a. may follow cystitis b. clinical manifestation includes costovertebral angle tenderness c. most commonly caused by E coli d. all of the above answer : d – all statements are descriptive of pyelonephritis Retinal Detachment Main Problem : Separation of the sensory retina from the pigment epithelium of the retine Initial manifestation : Visual floaters described by patients as cobwebs or curtain in eyes Nursing Diagnosis : Potential for Injury Interventions : Immediate Bedrest Position patient with the affected side towards the bed , so gravity may help put the detached retina back into place . Avoid coughing ,sneezing and straining prepare the patient for eye surgery. Spinal Cord Injury Main Problem : Partial or complete disruption of nerve tracts and neurons resulting in paralysis and sensory loss Initial manifestation : Depends on the level of injury Cervical : Quadriplegia Thoracic : Paraplegia Lumbar : Paraplegia Laboratory Data : X – Ray reveals the location and extent of injury Nursing Diagnosis : Ineffective Breathing Pattern , Impaired Physical Mobility Interventions : Avoid hyperflexion and hyperextension of the spine . log roll the patient Keep a catheter at the bedside to prevent bladder distention which may stimulate autonomic dysreflexia Syndrome of Inappropriate antidiuretic Hormone (SIADH) Main Problem : Inappropriate continued release of antidiuretic hormone resulting in water intoxication Initial Manifestation : Mental Confusion Laboratory Data : Hyponatremia – Na , 120 mEq / L Nursing Diagnosis : Fluid Volume Excess Fluid and electrolyte imbalance Interventions : Fluid Restriction Assess for signs and symptoms of hyponatremia Ulcerative Colitis Main Problem : Ulceration of the mucosa of the lower colon and rectum Initial manifestation : Bloody Mucoid Diarrhea Laboratory data : Barium enema reveals lesions Nursing Diagnosis : Pain Altered Bowel Elimination ; diarrhea Interventions : Avoid dairy products Maintain Low Residue and High protein Diet , avoid cold fluids Teach patients about familial predisposition NURSING BULLETS MEDICAL SURGICAL NURSING In a patient with hypokalemia (serum potassium level below 3.5 mEq/L), presenting signs and symptoms include muscle weakness and cardiac arrhythmias. During cardiac arrest, if an I.V. route is unavailable, epinephrine can be administered endotracheally. Pernicious anemia results from the failure to absorb vitamin B12 in the GI tract and causes primarily GI and neurologic signs and symptoms. A patient who has a pressure ulcer should consume a high-protein, high-calorie diet, unless contraindicated. The CK-MB isoenzyme level is used to assess tissue damage in myocardial infarction. After a 12-hour fast, the normal fasting blood glucose level is 80 to 120 mg/dl. A patient who is experiencing digoxin toxicity may report nausea, vomiting, diplopia, blurred vision, light flashes, and yellow-green halos around images. Anuria is daily urine output of less than 100 ml. In remittent fever, the body temperature varies over a 24-hour period, but remains elevated. Risk of a fat embolism is greatest in the first 48 hours after the fracture of a long bone. It’s manifested by respiratory distress. To help venous blood return in a patient who is in shock, the nurse should elevate the patient’s legs no more than 45 degrees. This procedure is contraindicated in a patient with a head injury. The pulse deficit is the difference between the apical and radial pulse rates, when taken simultaneously by two nurses. To reduce the patient’s risk of vomiting and aspiration, the nurse should schedule postural drainage before meals or 2 to 4 hours after meals. Blood pressure can be measured directly by intra-arterial insertion of a catheter connected to a pressure-monitoring device. A positive Kernig’s sign, seen in meningitis, occurs when an attempt to flex the hip of a recumbent patient causes painful spasms of the hamstring muscle and resistance to further extension of the leg at the knee. In a patient with a fractured, dislocated femur, treatment begins with reduction and immobilization of the affected leg. Herniated nucleus pulposus (intervertebral disk) most commonly occurs in the lumbar and lumbosacral regions. Laminectomy is surgical removal of the herniated portion of an intervertebral disk. Surgical treatment of a gastric ulcer includes severing the vagus nerve (vagotomy) to reduce the amount of gastric acid secreted by the gastric cells. Valsalva’s maneuver is forced exhalation against a closed glottis, as when taking a deep breath, blowing air out, or bearing down. When mean arterial pressure falls below 60 mm Hg and systolic blood pressure falls below 80 mm Hg, vital organ perfusion is seriously compromised. Lidocaine (Xylocaine) is the drug of choice for reducing premature ventricular contractions. A patient is at greatest risk of dying during the first 24 to 48 hours after a myocardial infarction. During a myocardial infarction, the left ventricle usually sustains the greatest damage. The pain of a myocardial infarction results from myocardial ischemia caused by anoxia. For a patient in cardiac arrest, the first priority is to establish an airway. The universal sign for choking is clutching the hand to the throat. For a patient who has heart failure or cardiogenic pulmonary edema, nursing interventions focus on decreasing venous return to the heart and increasing left ventricular output. These interventions include placing the patient in high Fowler’s position and administering oxygen, diuretics, and positive inotropic drugs as prescribed. A positive tuberculin skin test is an induration of 10 mm or greater at the injection site. The signs and symptoms of histoplasmosis, a chronic systemic fungal infection, resemble those of tuberculosis. In burn victims, the leading cause of death is respiratory compromise. The second leading cause is infection. The exocrine function of the pancreas is the secretion of enzymes used to digest carbohydrates, fats, and proteins. A patient who has hepatitis A (infectious hepatitis) should consume a diet that’s moderately high in fat and high in carbohydrate and protein, and should eat the largest meal in the morning. Esophageal balloon tamponade shouldn’t be inflated greater than 20 mm Hg. Overproduction of prolactin by the pituitary gland can cause galactorrhea (excessive or abnormal lactation) and amenorrhea (absence of menstruation). Intermittent claudication (pain during ambulation or other movement that’s relieved with rest) is a classic symptom of arterial insufficiency in the leg. In bladder carcinoma, the most common finding is gross, painless hematuria. Parenteral administration of heparin sodium is contraindicated in patients with renal or liver disease, GI bleeding, or recent surgery or trauma; in pregnant patients; and in women older than age 60. Drugs that potentiate the effects of anticoagulants include aspirin, chloral hydrate, glucagon, anabolic steroids, and chloramphenicol. For a burn patient, care priorities include maintaining a patent airway, preventing or correcting fluid and electrolyte imbalances, controlling pain, and preventing infection. Elastic stockings should be worn on both legs. Active immunization is the formation of antibodies within the body in response to vaccination or exposure to disease. Passive immunization is administration of antibodies that were preformed outside the body. A patient who is receiving digoxin (Lanoxin) shouldn’t receive a calcium preparation because of the increased risk of digoxin toxicity. Concomitant use may affect cardiac contractility and lead to arrhythmias. Intermittent positive-pressure breathing is inflation of the lung during inspiration with compressed air or oxygen. The goal of this inflation is to keep the lung open. Wristdrop is caused by paralysis of the extensor muscles in the forearm and hand. Footdrop results from excessive plantar flexion and is usually a complication of prolonged bed rest. A patient who has gonorrhea may be treated with penicillin and probenecid (Benemid). Probenecid delays the excretion of penicillin and keeps this antibiotic in the body longer. In patients who have glucose-6-phosphate dehydrogenase (G6PD) deficiency, the red blood cells can’t metabolize adequate amounts of glucose, and hemolysis occurs. On-call medication is medication that should be ready for immediate administration when the call to administer it’s received. If gagging, nausea, or vomiting occurs when an airway is removed, the nurse should place the patient in a lateral position with the upper arm supported on a pillow. When a postoperative patient arrives in the recovery room, the nurse should position the patient on his side or with his head turned to the side and the chin extended. In the immediate postoperative period, the nurse should report a respiratory rate greater than 30, temperature greater than 100° F (37.8° C) or below 97° F (36.1° C), or a significant drop in blood pressure or rise in pulse rate from the baseline. Irreversible brain damage may occur if the central nervous system is deprived of oxygen for more than 4 minutes. Treatment for polycythemia vera includes administering oxygen, radioisotope therapy, or chemotherapy agents, such as chlorambucil and nitrogen mustard, to suppress bone marrow growth. A patient with acute renal failure should receive a high-calorie diet that’s low in protein as well as potassium and sodium. Addison’s disease is caused by hypofunction of the adrenal gland and is characterized by fatigue, anemia, weight loss, and bronze skin pigmentation. Without cortisol replacement therapy, it’s usually fatal. Glaucoma is managed conservatively with beta-adrenergic blockers such as timolol (Timoptic), which decrease sympathetic impulses to the eye, and with miotic eyedrops such as pilocarpine (Isopto Carpine), which constrict the pupils. Miotics effectively treat glaucoma by reducing intraocular pressure. They do this by constricting the pupil, contracting the ciliary muscles, opening the anterior chamber angle, and increasing the outflow of aqueous humor. While a patient is receiving heparin, the nurse should monitor the partial thromboplastin time. Urinary frequency, incontinence, or both can occur after catheter removal. Incontinence may be manifested as dribbling. When teaching a patient about colostomy care, the nurse should instruct the patient to hang the irrigation reservoir 18" to 22" (45 to 55 cm) above the stoma, insert the catheter 2" to 4" (5 to 10 cm) into the stoma, irrigate the stoma with 17 to 34 oz (503 to 1,005 ml) of water at a temperature of 105° to 110° F (40° to 43° C) once a day, clean the area around the stoma with soap and water before applying a new bag, and use a protective skin covering, such as a Stomahesive wafer, karaya paste, or karaya ring, around the stoma. The first sign of Hodgkin’s disease is painless, superficial lymphadenopathy, typically found under one arm or on one side of the neck in the cervical chain. To differentiate true cyanosis from deposition of certain pigments, the nurse should press the skin over the discolored area. Cyanotic skin blanches, but pigmented skin doesn’t. A patient who has a gastric ulcer is most likely to report pain during or shortly after eating. Widening pulse pressure is a sign of increasing intracranial pressure. For example, the blood pressure may rise from 120/80 to 160/60 mm Hg. In a burn victim, a primary goal of wound care is to prevent contamination by microorganisms. To prevent external rotation in a patient who has had hip nailing, the nurse places trochanter rolls from the knee to the ankle of the affected leg. Severe hip pain after the insertion of a hip prosthesis indicates dislodgment. If this occurs, before calling the physician, the nurse should assess the patient for shortening of the leg, external rotation, and absence of reflexes. As much as 75% of renal function is lost before blood urea nitrogen and serum creatinine levels rise above normal. When compensatory efforts are present in acid-base balance, partial pressure of arterial carbon dioxide (PaCO2) and bicarbonate (HCO3–) always point in the same direction: pH PaCO2 HCO3– = respiratory acidosis compensated pH PaCO2 HCO3– = respiratory alkalosis compensated pH PaCO2 HCO3– = metabolic acidosis compensated pH PaCO2 HCO3– = metabolic alkalosis compensated. Polyuria is urine output of 2,500 ml or more within 24 hours. The presenting sign of pleuritis is chest pain that is usually unilateral and related to respiratory movement. If a patient has a gastric drainage tube in place, the nurse should expect the physician to order potassium chloride. An increased pulse rate is one of the first indications of respiratory difficulty. It occurs because the heart attempts to compensate for a decreased oxygen supply to the tissues by pumping more blood. In an adult, a hemoglobin level below 11 mg/dl suggests iron deficiency anemia and the need for further evaluation. The normal partial pressure of oxygen in arterial blood is 95 mm Hg (plus or minus 5 mm Hg). Vitamin C deficiency is characterized by brittle bones, pinpoint peripheral hemorrhages, and friable gums with loosened teeth. Clinical manifestations of pulmonary embolism are variable, but increased respiratory rate, tachycardia, and hemoptysis are common. Normally, intraocular pressure is 12 to 20 mm Hg. It can be measured with a Schiøtz tonometer. In early hemorrhagic shock, blood pressure may be normal, but respiratory and pulse rates are rapid. The patient may report thirst and may have clammy skin and piloerection (goose bumps). Cool, moist, pale skin, as occurs in shock, results from diversion of blood from the skin to the major organs. To assess capillary refill, the nurse applies pressure over the nail bed until blanching occurs, quickly releases the pressure, and notes the rate at which blanching fades. Capillary refill indicates perfusion, which decreases in shock, thereby lengthening refill time. Normal capillary refill is less than 3 seconds. Except for patients with renal failure, urine output of less than 30 ml/hour signifies dehydration and the potential for shock. In elderly patients, the most common fracture is hip fracture. Osteoporosis weakens the bones, predisposing these patients to fracture, which usually results from a fall. Before angiography, the nurse should ask the patient whether he’s allergic to the dye, shellfish, or iodine and advise him to take nothing by mouth for 8 hours before the procedure. During myelography, approximately 10 to 15 ml of cerebrospinal fluid is removed for laboratory studies and an equal amount of contrast media is injected. After angiography, the puncture site is covered with a pressure dressing and the affected part is immobilized for 8 hours to decrease the risk of bleeding. If a water-based medium was used during myelography, the patient remains on bed rest for 6 to 8 hours, with the head of the bed elevated 30 to 45 degrees. If an oil-based medium was used, the patient remains flat in bed for 6 to 24 hours. The level of amputation is determined by estimating the maximum viable tissue (tissue with adequate circulation) needed to develop a functional stump. Heparin sodium is included in the dialysate used for renal dialysis. Paroxysmal nocturnal dyspnea may indicate heart failure. A patient who takes a cardiac glycoside, such as digoxin, should consume a diet that includes high-potassium foods. The nurse should limit tracheobronchial suctioning to 10 to 15 seconds and should make only two passes. Before performing tracheobronchial suctioning, the nurse should ventilate and oxygenate the patient five to six times with a resuscitation bag and 100% oxygen. This procedure is called bagging. Signs and symptoms of pneumothorax include tachypnea, restlessness, hypotension, and tracheal deviation. The cardinal sign of toxic shock syndrome is rapid onset of a high fever. A key sign of peptic ulcer is hematemesis, which can be bright red or dark red, with the consistency of coffee grounds. Signs and symptoms of a perforated peptic ulcer include sudden, severe upper abdominal pain; vomiting; and an extremely tender, rigid (boardlike) abdomen. Constipation is a common adverse reaction to aluminum hydroxide. For the first 24 hours after a myocardial infarction, the patient should use a bedside commode and then progress to walking to the toilet, bathing, and taking short walks. After a myocardial infarction, the patient should avoid overexertion and add a new activity daily, as tolerated without dyspnea. In a patient with a recent myocardial infarction, frothy, blood-tinged sputum suggests pulmonary edema. In a patient who has acquired immunodeficiency syndrome, the primary purpose of drugs is to prevent secondary infections. In a patient with acquired immunodeficiency syndrome, suppression of the immune system increases the risk of opportunistic infections, such as cytomegalovirus, Pneumocystis carinii pneumonia, and thrush. A patient with acquired immunodeficiency syndrome may have rapid weight loss, a sign of wasting syndrome. If the body doesn’t use glucose for energy, it metabolizes fat and produces ketones. Approximately 20% of patients with Guillain-Barré syndrome have residual deficits, such as mild motor weakness or diminished lower extremity reflexes. Hypertension and hypokalemia are the most significant clinical manifestations of primary hyperaldosteronism. After percutaneous aspiration of the bladder, the patient’s first void is usually pink; however, urine with frank blood should be reported to the physician. A urine culture that grows more than 100,000 colonies of bacteria per milliliter of urine indicates infection. A patient who is undergoing dialysis should take a vitamin supplement and eat foods that are high in calories, but low in protein, sodium, and potassium. In a patient who has chronic obstructive pulmonary disease, the most effective ways to reduce thick secretions are to increase fluid intake to 2,500 ml/day and encourage ambulation. The nurse should teach a patient with emphysema how to perform pursed-lip breathing because this slows expiration, prevents alveolar collapse, and helps to control the respiratory rate. Clubbing of the digits and a barrel chest may develop in a patient who has chronic obstructive pulmonary disease. A stroke (“brain attack”) disrupts the brain’s blood supply and may be caused by hypertension. In a patient who is undergoing dialysis, desired outcomes are normal weight, normal serum albumin level (3.5 to 5.5 g/dl), and adequate protein intake (1.2 to 1.5 g/kg of body weight daily). Intermittent peritoneal dialysis involves performing three to seven treatments that total 40 hours per week. In a patient with chronic obstructive pulmonary disease, the best way to administer oxygen is by nasal cannula. The normal flow rate is 2 to 3 L/ minute. Isoetharine (Bronkosol) can be administered with a handheld nebulizer or by intermittent positive-pressure breathing. Brain death is irreversible cessation of brain function. Continuous ambulatory peritoneal dialysis requires four exchanges per day, 7 days per week, for a total of 168 hours per week. The classic adverse reactions to antihistamines are dry mouth, drowsiness, and blurred vision. Because of the risk of paralytic ileus, a patient who has received a general anesthetic can’t take anything by mouth until active bowel sounds are heard in all abdominal quadrants. The level of alpha-fetoprotein, a tumor marker, is elevated in patients who have testicular germ cell cancer. Clinical manifestations of orchitis caused by bacteria or mumps include high temperature, chills, and sudden pain in the involved testis. The level of prostate-specific antigen is elevated in patients with benign prostatic hyperplasia or prostate cancer. The level of prostatic acid phosphatase is elevated in patients with advanced stages of prostate cancer. Phenylephrine (Neo-Synephrine), a mydriatic, is instilled in a patient’s eye to dilate the eye. To promote fluid drainage and relieve edema in a patient with epididymitis, the nurse should elevate the scrotum on a scrotal bridge. Fluorescein staining is commonly used to assess corneal abrasions because it outlines superficial epithelial defects. Presbyopia is loss of near vision as a result of the loss of elasticity of the crystalline lens. Transient ischemic attacks are considered precursors to strokes. A sign of acute appendicitis, McBurney’s sign is tenderness at McBurney’s point (about 2" [5 cm] from the right anterior superior iliac spine on a line between the spine and the umbilicus). When caring for a patient with Guillain-Barré syndrome, the nurse should focus on respiratory interventions as the disease process advances. Signs and symptoms of colon cancer include rectal bleeding, change in bowel habits, intestinal obstruction, abdominal pain, weight loss, anorexia, nausea, and vomiting. Symptoms of prostatitis include frequent urination and dysuria. A chancre is a painless, ulcerative lesion that develops during the primary stage of syphilis. During the tertiary stage of syphilis, spirochetes invade the internal organs and cause permanent damage. In total parenteral nutrition, weight gain is the most reliable indicator of a positive response to therapy. The nurse may administer an I.V. fat emulsion through a central or peripheral catheter, but shouldn’t use an in-line filter because the fat particles are too large to pass through the pores. If a patient who has a prostatectomy is using a Cunningham clamp, instruct him to wash and dry his penis before applying the clamp. He should apply the clamp horizontally and remove it at least every 4 hours to empty his bladder to prevent infection. If a woman has signs of urinary tract infection during menopause, she should be instructed to drink six to eight glasses of water per day, urinate before and after intercourse, and perform Kegel exercises. If a menopausal patient experiences a “hot flash,” she should be instructed to seek a cool, breezy location and sip a cool drink. Cheilosis causes fissures at the angles of the mouth and indicates a vitamin B2, riboflavin, or iron deficiency. Tetany may result from hypocalcemia caused by hypoparathyroidism. A patient who has cervical cancer may experience vaginal bleeding for 1 to 3 months after intracavitary radiation. Ascites is the accumulation of fluid, containing large amounts of protein and electrolytes, in the abdominal cavity. It’s commonly caused by cirrhosis. Normal pulmonary artery pressure is 10 to 25 mm Hg. Normal pulmonary artery wedge pressure is 5 to 12 mm Hg. After cardiac catheterization, the site is monitored for bleeding and hematoma formation, pulses distal to the site are palpated every 15 minutes for 1 hour, and the patient is maintained on bed rest with the extremity extended for 8 hours. Hemophilia is a bleeding disorder that’s transmitted genetically in a sex-linked (X chromosome) recessive pattern. Although girls and women may carry the defective gene, hemophilia usually occurs only in boys and men. Von Willebrand’s disease is an autosomal dominant bleeding disorder that’s caused by platelet dysfunction and factor VIII deficiency. Sickle cell anemia is a congenital hemolytic anemia that’s caused by defective hemoglobin S molecules. It primarily affects blacks. Sickle cell anemia has a homozygous inheritance pattern. Sickle cell trait has a heterozygous inheritance pattern. Pel-Ebstein fever is a characteristic sign of Hodgkin’s disease. Fever recurs every few days or weeks and alternates with afebrile periods. Glucose-6-phosphate dehydrogenase (G6PD) deficiency is an inherited metabolic disorder that’s characterized by red blood cells that are deficient in G6PD, a critical enzyme in aerobic glycolysis. Preferred sites for bone marrow aspiration are the posterior superior iliac crest, anterior iliac crest, and sternum. During bone marrow harvesting, the donor receives general anesthesia and 400 to 800 ml of marrow is aspirated. A butterfly rash across the bridge of the nose is a characteristic sign of systemic lupus erythematosus. Rheumatoid arthritis is a chronic, destructive collagen disease characterized by symmetric inflammation of the synovium that leads to joint swelling. Screening for human immunodeficiency virus antibodies begins with the enzyme-linked immunosorbent assay. Results are confirmed by the Western blot test. The CK-MB isoenzyme level increases 4 to 8 hours after a myocardial infarction, peaks at 12 to 24 hours, and returns to normal in 3 days. Excessive intake of vitamin K may significantly antagonize the anticoagulant effects of warfarin (Coumadin). The patient should be cautioned to avoid eating an excessive amount of leafy green vegetables. A lymph node biopsy that shows Reed-Sternberg cells provides a definitive diagnosis of Hodgkin’s disease. Bell’s palsy is unilateral facial weakness or paralysis caused by a disturbance of the seventh cranial (facial) nerve. During an initial tuberculin skin test, lack of a wheal after injection of tuberculin purified protein derivative indicates that the test dose was injected too deeply. The nurse should inject another dose at least 2" (5 cm) from the initial site. A tuberculin skin test should be read 48 to 72 hours after administration. In reading a tuberculin skin test, erythema without induration is usually not significant. Death caused by botulism usually results from delayed diagnosis and respiratory complications. In a patient who has rabies, saliva contains the virus and is a hazard for nurses who provide care. A febrile nonhemolytic reaction is the most common transfusion reaction. Hypokalemia (abnormally low concentration of potassium in the blood) may cause muscle weakness or paralysis, electrocardiographic abnormalities, and GI disturbances. Beriberi, a serious vitamin B1 (thiamine) deficiency, affects alcoholics who have poor dietary habits. It’s epidemic in Asian countries where people subsist on unenriched rice. It’s characterized by the phrase “I can’t,” indicating that the patient is too ill to do anything. Excessive sedation may cause respiratory depression. The primary postoperative concern is maintenance of a patent airway. If cyanosis occurs circumorally, sublingually, or in the nail bed, the oxygen saturation level (Sao 2) is less than 80%. A rapid pulse rate in a postoperative patient may indicate pain, bleeding, dehydration, or shock. Increased pulse rate and blood pressure may indicate that a patient is experiencing “silent pain” (pain that can’t be expressed verbally, such as when a patient is recovering from anesthesia). Lidocaine (Xylocaine) exerts antiarrhythmic action by suppressing automaticity in the Purkinje fibers and elevating the electrical stimulation threshold in the ventricles. Cullen’s sign (a bluish discoloration around the umbilicus) is seen in patients who have a perforated pancreas. During the postoperative period, the patient should cough and breathe deeply every 2 hours unless otherwise contraindicated (for example, after craniotomy, cataract surgery, or throat surgery). Before surgery, a patient’s respiratory volume may be measured by incentive spirometry. This measurement becomes the patient’s postoperative goal for respiratory volume. The postoperative patient should use incentive spirometry 10 to 12 times per hour and breathe deeply. Before ambulating, a postoperative patient should dangle his legs over the side of the bed and perform deep-breathing exercises. During the patient’s first postoperative ambulation, the nurse should monitor the patient closely and assist him as needed while he walks a few feet from the bed to a steady chair. Hypovolemia occurs when 15% to 25% of the body’s total blood volume is lost. Signs and symptoms of hypovolemia include rapid, weak pulse; low blood pressure; cool, clammy skin; shallow respirations; oliguria or anuria; and lethargy. Acute pericarditis causes sudden severe, constant pain over the anterior chest. The pain is aggravated by inspiration. Signs and symptoms of septicemia include fever, chills, rash, abdominal distention, prostration, pain, headache, nausea, and diarrhea. Rocky Mountain spotted fever causes a persistent high fever, nonpitting edema, and rash. Patients who have undergone coronary artery bypass graft should sleep 6 to 10 hours per day, take their temperature twice daily, and avoid lifting more than 10 lb (4.5 kg) for at least 6 weeks. Claudication pain (pain on ambulation) is caused by arterial insufficiency as a result of atheromatous plaque that obstructs arterial blood flow to the extremities. Pacemakers can be powered by lithium batteries for up to 10 years. The patient shouldn’t void for 1 hour before percutaneous suprapubic bladder aspiration to ensure that sufficient urine remains in the bladder to make the procedure successful. Left-sided heart failure causes pulmonary congestion, pink-tinged sputum, and dyspnea. (Remember L for left and lung.) The current recommended blood cholesterol level is less than 200 mg/dl. When caring for a patient who is having a seizure, the nurse should follow these guidelines: (1) Avoid restraining the patient, but help a standing patient to a lying position. (2) Loosen restrictive clothing. (3) Place a pillow or another soft object under the patient’s head. (4) Clear the area of hard objects. (5) Don’t force anything into the patient’s mouth, but maintain a patent airway. (6) Reassure and reorient the patient after the seizure subsides. Gingival hyperplasia, or overgrowth of gum tissue, is an adverse reaction to phenytoin (Dilantin). With aging, most marrow in long bones becomes yellow, but it retains the capacity to convert back to red. Clinical manifestations of lymphedema include accumulation of fluid in the legs. Afterload is ventricular wall tension during systolic ejection. It’s increased in patients who have septal hypertrophy, increased blood viscosity, and conditions that cause blockage of aortic or pulmonary outflow. Red blood cells can be stored frozen for up to 2 years; however, they must be used within 24 hours of thawing. For the first 24 hours after amputation, the nurse should elevate the stump to prevent edema. After hysterectomy, a woman should avoid sexual intercourse for 3 weeks if a vaginal approach was used and 6 weeks if the abdominal approach was used. Parkinson’s disease characteristically causes progressive muscle rigidity, akinesia, and involuntary tremor. Tonic-clonic seizures are characterized by a loss of consciousness and alternating periods of muscle contraction and relaxation. Status epilepticus, a life-threatening emergency, is a series of rapidly repeating seizures that occur without intervening periods of consciousness. The ideal donor for kidney transplantation is an identical twin. If an identical twin isn’t available, a biological sibling is the next best choice. Breast cancer is the leading cancer among women; however, lung cancer accounts for more deaths. The stages of cervical cancer are as follows: stage 0, carcinoma in situ; stage I, cancer confined to the cervix; stage II, cancer extending beyond the cervix, but not to the pelvic wall; stage III, cancer extending to the pelvic wall; and stage IV, cancer extending beyond the pelvis or within the bladder or rectum. One method used to estimate blood loss after a hysterectomy is counting perineal pads. Saturating more than one pad in 1 hour or eight pads in 24 hours is considered hemorrhaging. Transurethral resection of the prostate is the most common procedure for treating benign prostatic hyperplasia. In a chest drainage system, the water in the water-seal chamber normally rises when a patient breathes in and falls when he breathes out. Spinal fusion provides spinal stability through a bone graft, usually from the iliac crest, that fuses two or more vertebrae. A patient who receives any type of transplant must take an immunosuppressant drug for the rest of his life. Incentive spirometry should be used 5 to 10 times an hour while the patient is awake. In women, pelvic inflammatory disease is a common complication of gonorrhea. Scoliosis is lateral S-shaped curvature of the spine. Signs and symptoms of the secondary stage of syphilis include a rash on the palms and soles, erosion of the oral mucosa, alopecia, and enlarged lymph nodes. In a patient who is receiving total parenteral nutrition, the nurse should monitor glucose and electrolyte levels. Unless contraindicated, on admission to the postanesthesia care unit, a patient should be turned on his side and his vital signs should be taken. Edema is treated by limiting fluid intake and eliminating excess fluid. A patient who has had spinal anesthesia should remain flat for 12 to 24 hours. Vital signs and neuromuscular function should be monitored. A patient who has maple syrup urine disease should avoid food containing the amino acids leucine, isoleucine, and lysine. A severe complication of a femur fracture is excessive blood loss that results in shock. To prepare a patient for peritoneal dialysis, the nurse should ask the patient to void, measure his vital signs, place him in a supine position, and using aseptic technique, insert a catheter through the abdominal wall and into the peritoneal space. If more than 3 L of dialysate solution return during peritoneal dialysis, the nurse should notify the physician. Hemodialysis is the removal of certain elements from the blood by passing heparinized blood through a semipermeable membrane to the dialysate bath, which contains all of the important electrolytes in their ideal concentrations. Gangrene usually affects the digits first, and begins with skin color changes that progress from gray-blue to dark brown or black. Kidney function is assessed by evaluating blood urea nitrogen (normal range is 8 to 20 mg/dl) and serum creatinine (normal range is 0.6 to 1.3 mg/dl) levels. A weight-bearing transfer is appropriate only for a patient who has at least one leg that’s strong enough to bear weight, such as a patient with hemiplegia or a single-leg amputation. Overflow incontinence (voiding of 30 to 60 ml of urine every 15 to 30 minutes) is a sign of bladder distention. The first sign of a pressure ulcer is reddened skin that blanches when pressure is applied. Late signs and symptoms of sickle cell anemia include tachycardia, cardiomegaly, systolic and diastolic murmurs, chronic fatigue, hepatomegaly, and splenomegaly. A mechanical ventilator, which can maintain ventilation automatically for an extended period, is indicated when a patient can’t maintain a safe PaO2 or PaCO2 level. Two types of mechanical ventilators exist: negative-pressure ventilators, which apply negative pressure around the chest wall, and positive-pressure ventilators, which deliver air under pressure to the patient. Angina pectoris is characterized by substernal pain that lasts for 2 to 3 minutes. The pain, which is caused by myocardial ischemia, may radiate to the neck, shoulders, or jaw; is described as viselike, or constricting; and may be accompanied by severe apprehension or a feeling of impending doom. The diagnosis of an acute myocardial infarction is based on the patient’s signs and symptoms, electrocardiogram tracings, troponin level, and cardiac enzyme studies. The goal of treatment for a patient with angina pectoris is to reduce the heart’s workload, thereby reducing the myocardial demand for oxygen and preventing myocardial infarction. Nitroglycerin decreases the amount of blood that returns to the heart by increasing the capacity of the venous bed. The patient should take no more than three nitroglycerin tablets in a 15-minute period. Hemodialysis is usually performed 24 hours before kidney transplantation. Signs and symptoms of acute kidney transplant rejection are progressive enlargement and tenderness at the transplant site, increased blood pressure, decreased urine output, elevated serum creatinine level, and fever. After a radical mastectomy, the patient’s arm should be elevated (with the hand above the elbow) on a pillow to enhance circulation and prevent edema. Postoperative mastectomy care includes teaching the patient arm exercises to facilitate lymph drainage and prevent shortening of the muscle and contracture of the shoulder joint (frozen shoulder). After radical mastectomy, the patient should help prevent infection by making sure that no blood pressure readings, injections, or venipunctures are performed on the affected arm. For a patient who has undergone mastectomy and is susceptible to lymphedema, a program of hand exercises can begin shortly after surgery, if prescribed. The program consists of opening and closing the hand tightly six to eight times per hour and performing such tasks as washing the face and combing the hair. Signs and symptoms of theophylline toxicity include vomiting, restlessness, and an apical pulse rate of more than 200 beats/minute. The nurse shouldn’t induce vomiting in a person who has ingested poison and is having seizures or is semiconscious or comatose. Central venous pressure (CVP), which is the pressure in the right atrium and the great veins of the thorax, is normally 2 to 8 mm Hg (or 5 to 12 cm H2O). CVP is used to assess right-sided cardiac function. CVP is monitored to assess the need for fluid replacement in seriously ill patients, to estimate blood volume deficits, and to evaluate circulatory pressure in the right atrium. To prevent deep vein thrombosis after surgery, the nurse should administer 5,000 units of heparin subcutaneously every 8 to 12 hours, as prescribed. Oral anticoagulants, such as warfarin (Coumadin) and dicumarol, disrupt natural blood clotting mechanisms, prevent thrombus formation, and limit the extension of a formed thrombus. Anticoagulants can’t dissolve a formed thrombus. Anticoagulant therapy is contraindicated in a patient who has liver or kidney disease or GI ulcers or who isn’t likely to return for follow-up visits. The nurse can assess a patient for thrombophlebitis by measuring the affected and unaffected legs and comparing their sizes. The nurse should mark the measurement locations with a pen so that the legs can be measured at the same place each day. Drainage of more than 3,000 ml of fluid daily from a nasogastric tube may suggest intestinal obstruction. Yellow drainage that has a foul odor may indicate small-bowel obstruction. Preparation for sigmoidoscopy includes administering an enema 1 hour before the examination, warming the scope in warm water or a sterilizer (if using a metal sigmoidoscope), and draping the patient to expose the perineum. Treatment for a patient with bleeding esophageal varices includes administering vasopressin (Pitressin), giving an ice water lavage, aspirating blood from the stomach, using esophageal balloon tamponade, providing parenteral nutrition, and administering blood transfusions, as needed. A trauma victim shouldn’t be moved until a patent airway is established and the cervical spine is immobilized. After a mastectomy, lymphedema may cause a feeling of heaviness in the affected arm. A dying patient shouldn’t be told exactly how long he’s expected to live, but should be told something more general such as “Some people live 3 to 6 months, but others live longer.” After eye surgery, a patient should avoid using makeup until otherwise instructed. After a corneal transplant, the patient should wear an eye shield when engaging in activities such as playing with children or pets. After a corneal transplant, the patient shouldn’t lie on the affected site, bend at the waist, or have sexual intercourse for 1 week. The patient must avoid getting soapsuds in the eye. A Milwaukee brace is used for patients who have structural scoliosis. The brace helps to halt the progression of spinal curvature by providing longitudinal traction and lateral pressure. It should be worn 23 hours a day. Short-term measures used to treat stomal retraction include stool softeners, irrigation, and stomal dilatation. A patient who has a colostomy should be advised to eat a low-residue diet for 4 to 6 weeks and then to add one food at a time to evaluate its effect. To relieve postoperative hiccups, the patient should breathe into a paper bag. If a patient with an ileostomy has a blocked lumen as a result of undigested high-fiber food, the patient should be placed in the kneechest position and the area below the stoma should be massaged. During the initial interview and treatment of a patient with syphilis, the patient’s sexual contacts should be identified. The nurse shouldn’t administer morphine to a patient whose respiratory rate is less than 12 breaths/minute. To prevent drying of the mucous membranes, oxygen should be administered with hydration. Flavoxate (Urispas) is classified as a urinary tract spasmolytic. Hypotension is a sign of cardiogenic shock in a patient with a myocardial infarction. The predominant signs of mechanical ileus are cramping pain, vomiting, distention, and inability to pass feces or flatus. For a patient with a myocardial infarction, the nurse should monitor fluid intake and output meticulously. Too little intake causes dehydration, and too much may cause pulmonary edema. Nitroglycerin relaxes smooth muscle, causing vasodilation and relieving the chest pain associated with myocardial infarction and angina. The diagnosis of an acute myocardial infarction is based on the patient’s signs and symptoms, electrocardiogram tracings, and serum enzyme studies. Arrhythmias are the predominant problem during the first 48 hours after a myocardial infarction. Clinical manifestations of malabsorption include weight loss, muscle wasting, bloating, and steatorrhea. Asparaginase, an enzyme that inhibits the synthesis of deoxyribonucleic acid and protein, is used to treat acute lymphocytic leukemia. To relieve a patient’s sore throat that’s caused by nasogastric tube irritation, the nurse should provide anesthetic lozenges, as prescribed. For the first 12 to 24 hours after gastric surgery, the stomach contents (obtained by suctioning) are brown. GOODLUCK AND GOD BLESS…JLO