3d statistical analysis - Shattuck Research Group
advertisement

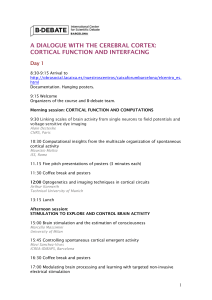
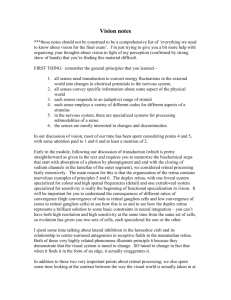
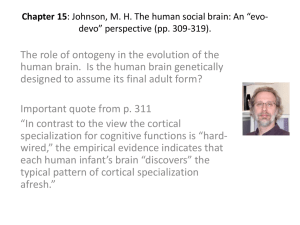
COMPUTATIONAL NEUROANATOMY: TOWARDS A COMPUTER-ASSISTED DIAGNOSIS OF DEGENERATIVE BRAIN DISEASES BASED ON MRI Giovanni Frisoni, John Ashburner, John Csernansky, Christos Davatzikos, Karl Friston, Martin Rossor, Paul Thompson A Review Article for: Lancet Neurology Text from Paul Thompson, April 19, 2002 Giovanni, Christa: Here is my text, to insert in the section “Cortical Morphometry” in your outline. -- Paul Giovanni’s Outline: 1. Whole-brain analysis 1.1 SPM-based methods: K Friston-J Ashburner 1.2 RAVENS: C Davatzikos 2. ROI-based analysis 2.1 Cortical morphometry: P Thompson 2.2 Hippocampus and other closed structures: J Csernansky 3. Analysis of change over tiime: 3.1 Whole brain changes and regional changes: M Rossor Each of the 5 subsections addresses: basic concepts of image processing and analysis (200 words) technical requirements/limitations (250 words) sensitivity to morphological differences (400 words) clinical studies: available evidence and potential usefulness (200 words) for a total of not more than 1050 words per subsection. …………….. Cortical Morphometry The quest to identify biological markers for Alzheimer’s disease has been greatly empowered by specialized methods for modeling the human cortex. These methods detect subtle changes in cortical shape, complexity, and gray matter distribution, all of which are affected in neurodegenerative disease. Composite maps of cortical features, generated for large populations, can reveal deficit patterns in clinically-defined groups, such as those at undergoing drug treatment or at genetic risk (Cannon et al., 2002). Disease-specific atlases are also rapidly being built to represent dementia populations (Thompson et al., 2000, 2001a,b). These are beginning to link population statistics on cortical changes with metabolic (Mega et al., 1997), cognitive (Thompson et al., 2002), genetic (Lehtovirta et al., 2000; Small et al., 2000) or medication effects (Thompson et al., 2001). Basic Concepts. If MRI datasets are averaged across subjects after global alignment, cortical features are washed away, 2 due to gyral pattern variations (see Fig. 1(a)). However, these gyral features can be retained in the group average using a technique known as cortical pattern matching (see Fig. 1; Thompson and Toga, 1996, 1997, 2001; Davatzikos, 1996; Fischl et al., 1999; Drury et al., 2000). With this approach, individual patients’ data can also be transferred to an atlas standard, and compared with other subjects, accommodating gyral pattern variations. Statistics and average maps of shape differences or tissue deficits are then computed, localizing systematic effects on cortical structure relative to gyral landmarks. Technical Requirements. Briefly, a 3D cortical surface model (Fig. 1(e),(f)) is extracted from each individual subject’s scan (Fig. 1(d)) after global alignment of individual MRI data into a standardized 3D coordinate space (this may also be a disease-specific space, e.g. Thompson et al., 2000; Janke et al., 2001). A set of 38 sulcal curves (Fig. 1(e),(f)) is then manually traced on the cortical models, representing each subject’s primary gyral pattern. These curves are used as anchors to create a deformation mapping (Fig. 1, panel 2), which distorts the anatomy of one subject onto another, matching sulcal features exactly. To compute this mapping, cortical models and curves are first flattened (Fig. 1, panel 1), and a flow field is computed in the flattened space, to drive individual sulcal features onto an average set of curves (panel 2). Using a mathematical trick, a color code representing 3D locations of cortical points in each subject (panel 3) is convected along with this flow (panel 4). Then these warped color images are averaged across subjects and decoded to produce a crisp group average model (panel 6; see Thompson et al., 2002 for more details). These deformation maps represent the complex distortion required to match one cortex to a group average (Fig. 2(b)). They store information on gyral pattern differences in a group of subjects, and their preferred directions (Fig. 2). By converting these differences into local measures of variance (covariance tensors, Fig. 2(b)), shape abnormalities can be calibrated against a statistical encoding of normal variation and mapped in an individual patient (abnormality map, Fig. 2(c); Thompson et al., 1996, 1997; Cao and Worsley, 1999). Sensitivity to Morphological Differences. Cortical pattern matching also makes it easier to detect gray matter deficits in regions where gyral pattern variation is greatest (e.g. perisylvian cortices, Fig. 2(e)). As with SPM and RAVENS maps, gray matter density can be compared across regions whose correspondences are defined by deformation mappings (Thompson et al., 1998). The significance of these differences can be plotted in color on the group average cortex (Fig. 3). As in SPM, the significance of statistical maps plotted on the cortical sheet can be assessed by analytical formulae for the distributions of 3 features in Gaussian fields on curved manifolds (Worsley et al., 1999; Taylor and Adler, 2002), or, more commonly, by permutation methods (e.g., Holmes et al., 1996; Bullmore et al., 1999; Thompson et al., 2000). As with SPM and RAVENS maps, one advantage of the cortical modeling approach relative to volumetric studies is the ability to localize effects on brain structure in the form of a map (Fig. 3). These changes can also be linked visually with measures of cognitive decline. Cortical pattern matching also increases signal to noise (Zeineh et al., 2001) by associating gray matter measures from corresponding cortical regions. In the resulting maps, regions of comparatively spared tissue may appear sharply delimited from regions with significant loss (Fig. 3(b)) or progressive loss (Fig. 3(d)-(i)). Cortical surface matching also adjusts for shape changes over time in longitudinal studies (Thompson et al., 2001, 2002), and quantifies them for subsequent analysis (Thompson et al., 2000). Hemispheric asymmetries in deficits are also readily detected, by matching cortical patterns in one hemisphere with the other (Thompson et al., 2001). New signal processing methods are also emerging to help in detecting cortical changes. These include algorithms to detect diffuse signals in the cortical sheet (see Thompson et al., 2000; Chung et al., 2000; Taylor and Adler, 2002 for methods based on Riemannian filters, scale space, and Beltrami flows). Powerful methods are rapidly being developed to estimate cortical thickness in human populations (e.g., MacDonald et al., 2000; Fischl et al., 2000), and these are likely to assist in identifying the earliest deficits. Clinical Studies. Cortical modeling shows considerable promise for early detection of dementia, for identifying medication effects on disease progression, and for isolating deficits associated with risk genotypes. We recently used cortical pattern matching to uncover deficit profiles in early AD (Thompson et al., 2001). We found pervasive gray matter loss in temporo-parietal association cortices (Fig. 3(b),(c)), while sensorimotor and occipital cortices were comparatively spared. At this early stage of AD, the pathologic burden may be greater in terms of functional deficits, and synaptic loss, in heteromodal cortex than in idiotypic cortex. The profile is also consistent with metabolic deficits commonly observed in FDG-PET studies, and with beta-amyloid and neurofibrillary tangle distribution in early AD (Mega et al., 1997, 1999). A prominent left-right asymmetry was also mapped, with more severe gray matter deficits in the left hemisphere. In a separate study of 17 more severely affected patients scanned longitudinally (Thompson et al., 2002), deficits became more diffuse over time, and progressed into frontal cortices (Fig. 3). This progression occurred over a 2.5-year period in which MMSE cognitive test scores declined from 17.76.2 to 12.98.2 (meanSD). Effect sizes for these cortical changes were comparable to those for tensor-based maps of hippocampal loss rates (Thompson and Toga, 2002) and ventricular shape differences mapped in the 4 same patients (Thompson et al., 2000). While the cortex lost gray matter at a rate of up to 4-5%/year locally, greatest dynamic change rates were found in the inferior ventricular horns (L:+14.75.8%/yr.; R:+16.33.5%/yr.), with significant expansion rates bilaterally even in controls (L:+3.71.2%/yr.; R:+1.71.2%; p<0.001,p<0.01; Thompson et al., 2002). These data suggest that cortical maps may be fruitfully combined with volumetrics, tensor maps and shape modeling, for comprehensive visualization of the disease process. Cortical maps also show promise in identifying structural deficits associated with distinct phases of AD. This offers advantages in staging the disease. Statistics on expected rates of decline are also valuable for mapping medication response in drug trials. The profound differences in AD brain shape, cortical patterning and tissue distribution identified here also underscore the need for disease-specific brain atlases to better reflect patients’ anatomy, and for calibrating individual loss against statistical data from normative populations (e.g. Thompson et al., 2002). Figure Legends: Fig. 1. Creating Average Cortical Models and Maps in Alzheimer’s Disease Populations. Before computing individual anatomical differences, it is often advantageous to create an average model of anatomy for a specific population. If MRI scans are mutually aligned and their intensities are averaged [(a); Evans et al., 1994], cortical features are washed away. To retain these features in the group average [(b),(c)], a procedure called cortical pattern matching can be used (see Thompson et al., 2000 for details). From each individual’s MRI scan (d) a cortical model [(e),(f)] consisting of discrete triangular elements (g) is created and flattened (panel 1), along with digital models of cortical sulci traced on the brain surface. A warping field drives the flat map (1), and a color code indexing corresponding 3D cortical positions (3),(4), to match an average set of flat 2D sulcal curves (2). If these color images are averaged across subjects and decoded before cortical pattern matching (3), a smooth average cortex (5) is produced. If they are warped first (5), averaged, and decoded, a crisp average cortex appears, with reinforced features in their mean stereotaxic locations (6). Such cortical averages provide a standard template relative to which individual differences may be measured (Fig. 2). Using warping (4), cortical data can be transferred, from anatomically different individuals, onto a common anatomic template for comparison and integration. Fig. 2. Measuring Individual Brain Differences and Population Variability. When a individual brain (brown mesh, (a)) is globally aligned and scaled to match a group average cortical model (white surface), a 3D deformation (d) can be computed to match its gyral anatomy with the group average (pink colors: large deformations, (d)). The 3D root mean square magnitude of these deformation vectors (variability map, (e)) shows that gyral pattern variability is greatest in perisylvian language areas (red colors). 3D confidence regions for gyral variations can be also stored locally to detect cortical abnormalities ((b), Thompson et al., 1997). Ellipsoids, (b), are elongated along directions in which normal variation is greatest (pink colors). Regions of significant atrophy can then be identified in individual patients (c), by reference to the normative atlas. The normative atlas is here based on a group 5 of 20 healthy elderly subjects, but can be recomputed for any population. Fig. 3. Mapping Gray Matter Deficits in a Alzheimer’s Disease Population. Measures of gray matter density (a) can be computed from MRI scans and compared across individuals and patient groups. Data from corresponding cortical regions are compared using cortical pattern matching (see text). Patients with mild to moderate Alzheimer’s disease show a severe loss of gray matter [(b),(c)] relative to matched healthy controls, especially in temporal cortices (deficits approach 30% locally – red colors). These structural measures are tightly correlated with worsening symptoms (Thompson et al., 2001, 2002), and offer a promising endophenotype (biological marker) for drug studies. Maps are also shown [(d)-(i)] for 17 more severely affected AD patients and 14 matched controls, who were scanned longitudinally with a 2.5-year interval between scans. At follow-up, the patients’ MMSE scores had deteriorated from 17.76.2 to 12.98.2 (meanSD). Notice how tissue losses intensified [(d),(e)] from 5-10% initially (h) to a 15% gray matter deficit (i) in frontal cortices. These losses were tightly linked with cognitive decline assessed using MMSE scores. Acknowledgments. Grant support to P.T. was provided by a P41 Resource Grant from the National Center for Research Resources, by the National Library of Medicine (LM05639), and by a Human Brain Project grant to the International Consortium for Brain Mapping, funded jointly by NIMH and NIDA (MH52176). ………………………………………… References 1. Cannon TD, Thompson PM, van Erp T, Toga AW, Poutanen V-P, Huttunen M, Lönnqvist J, Standertskjöld-Nordenstam C-G, Narr KL, Khaledy M, Zoumalan CI, Dail R, Kaprio J (2002). Cortex Mapping Reveals Regionally Specific Patterns of Genetic and Disease-Specific Gray-Matter Deficits in Twins Discordant for Schizophrenia, Proceedings of the National Academy of Sciences of the USA, vol. 99, no. 5: 3228-3233, February 26, 2002. 2. Thompson PM, Mega MS, Vidal C, Rapoport JL, Toga AW (2001a). Detecting Disease-Specific Patterns of Brain Structure using Cortical Pattern Matching and a Population-Based Probabilistic Brain Atlas, IEEE Conference on Information Processing in Medical Imaging (IPMI), UC Davis, 2001, in: Lecture Notes in Computer Science (LNCS) 2082:488-501, M Insana, R Leahy [eds.], Springer-Verlag. 3. Thompson PM, Vidal CN, Giedd JN, Gochman P, Blumenthal J, Nicolson R, Toga AW, Rapoport JL (2001b). Mapping Adolescent Brain Change Reveals Dynamic Wave of Accelerated Gray Matter Loss in Very Early-Onset Schizophrenia, Proceedings of the National Academy of Sciences of the USA, 98(20):11650-11655, September 25, 2001. 4. Thompson PM, Mega MS, Toga AW (2000). Disease-Specific Brain Atlases, Invited Chapter in: Brain Mapping: The Disorders, Toga AW, Mazziotta JC [eds.], Academic Press, July 2000. 5. Mega MS, Chen S, Thompson PM, Woods RP, Karaca TJ, Tiwari A, Vinters H, Small GW, Toga AW (1997) Mapping Pathology to Metabolism: Coregistration of Stained Whole Brain Sections to PET in Alzheimer's Disease, NeuroImage 5:147-153, February 1997. 6. Thompson PM, Hayashi KM, de Zubicaray G, Janke AL, Rose SE, Semple J, Doddrell DM, Cannon TD, Toga AW (2002). Detecting Dynamic and Genetic Effects on Brain Structure using High-Dimensional Cortical Pattern Matching, Proc. International Symposium on Biomedical Imaging (ISBI2002), Washington, DC, July 7-10, 2002. 6 7. Lehtovirta M, Laakso MP, Frisoni GB, Soininen H. How does the apolipoprotein E genotype modulate the brain in aging and in Alzheimer's disease? A review of neuroimaging studies. Neurobiol Aging. 2000 Mar-Apr;21(2):293-300. 8. Small GW, Ercoli LM, Silverman DH, Huang SC, Komo S, et al. Cerebral metabolic and cognitive decline in persons at genetic risk for Alzheimer's disease. Proc Natl Acad Sci U S A. 2000 May 23;97(11):6037-42. 9. Thompson PM, Toga AW (1996). A Surface-Based Technique for Warping 3-Dimensional Images of the Brain, IEEE Transactions on Medical Imaging, Aug. 1996, 15(4):1-16. 10. Thompson PM, MacDonald D, Mega MS, Holmes CJ, Evans AC, Toga AW (1997). Detection and Mapping of Abnormal Brain Structure with a Probabilistic Atlas of Cortical Surfaces, J. Comp. Assist. Tomogr. 21(4):567-581, Jul.-Aug. 1997. 11. Thompson PM, Cannon TD, Narr KL, van Erp T, Khaledy M, Poutanen V-P, Huttunen M, Lönnqvist J, Standertskjöld-Nordenstam C-G, Kaprio J, Dail R, Zoumalan CI, Toga AW (2001). Genetic Influences on Brain Structure, Nature Neuroscience 4(12):1253-8, Dec. 2001. 12. Davatzikos C (1996). Spatial Normalization of 3D Brain Images using Deformable Models, J. Comp. Assisted Tomography 20(4):656-665, Jul.Aug. 1996. 13. Drury HA, Van Essen DC, Corbetta M, Snyder AZ (2000). Surface-based analyses of the human cerebral cortex. Chapter 19 in: Arthur W. Toga, editor, Brain Warping, Academic Press, 2000. 14. Fischl B, Sereno MI, Tootell RBH, Dale AM (1999). High-Resolution Inter-Subject Averaging and a Coordinate System for the Cortical Surface, Hum Brain Mapp. 1999;8(4):272-84. 15. Thompson PM, Woods RP, Mega MS, Toga AW. Mathematical/computational challenges in creating deformable and probabilistic atlases of the human brain. Human Brain Mapping 9(2):81-92 (2000). 16. Janke AL, Zubicaray Gd, Rose SE, Griffin M, Chalk JB, Galloway GJ (2001). 4D deformation modeling of cortical disease progression in Alzheimer's dementia. Magn. Reson. Med. 46(4):661-6. 17. Thompson PM, Schwartz C, Toga AW (1996). High-Resolution Random Mesh Algorithms for Creating a Probabilistic 3D Surface Atlas of the Human Brain, NeuroImage 3:19-34. 18. Cao J, Worsley KJ (1999). The Geometry of the Hotelling's T-squared Random Field with Applications to the Detection of Shape Changes, Annals of Statistics, 27, 925-942. 19. Worsley KJ, Andermann M, Koulis T, MacDonald D, Evans AC (1999). Detecting changes in nonisotropic images, Hum Brain Mapp. 1999;8(23):98-101. 20. Taylor JE, Adler RJ. Euler characteristics for Gaussian fields on manifolds http://www.math.mcgill.ca/jtaylor/publications/index.html (2002). 21. Holmes AP, Blair RC, Watson JDG, Ford I (1996). Nonparametric analysis of statistic images from functional mapping experiments, J. Cereb. Blood Flow and Metabolism 16(1):7-22, Jan. 1996. 22. Bullmore ET, Suckling J, Overmeyer S, Rabe-Hesketh S, Taylor E, Brammer MJ (1999) Global, voxel, and cluster tests, by theory and permutation, for a difference between two groups of structural MR images of the brain. IEEE Trans. Med. Imag., 18, 32-42. 23. Thompson PM et al., Brain Image Analysis and Atlas Construction, in: Fitzpatrick, M. (ed.), Handbook on Medical Image Analysis, SPIE Press (2000). 24. Zeineh MM, Engel SA, Thompson PM, Bookheimer S (2001). Unfolding the Human Hippocampus with High-Resolution Structural and 7 Functional MRI, The New Anatomist (Anat Rec.) 2001 Apr15;265(2):111-20. 25. Thompson PM, Giedd JN, Woods RP, MacDonald D, Evans A, Toga AW (2000). Growth Patterns in the Developing Brain Detected By Using Continuum-Mechanical Tensor Maps, Nature 404(6774):190-193. 26. Chung MK, Worsley KJ, Taylor J, Ramsay J, Robbins S, Evans AC (2000). Diffusion Smoothing on the Cortical Surface, Proc. Human Brain Mapping, 2000. 27. MacDonald D, Kabani N, Avis D, Evans AC (2000). Automated 3-D extraction of inner and outer surfaces of cerebral cortex from MRI. Neuroimage. 2000 Sep;12(3):340-56. 28. Fischl B, Dale AM (2001). Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc Natl Acad Sci U S A. 2000 Sep 26;97(20):11050-5. 29. Thompson PM et al. Cortical change in Alzheimer's disease detected with a disease-specific population-based brain atlas. Cerebral Cortex 11, 116 (2001). 30. Mega MS, Chu T, Mazziotta JC, Trivedi KH, Thompson PM, Shah A, Cole G, Frautschy SA, Toga AW (1999). Mapping Biochemistry to Metabolism: FDG-PET and Beta-Amyloid Burden in Alzheimer's Disease, NeuroReport 10(14):2911-2917, Sept. 29 1999. 31. Thompson PM, Toga AW (2002). A Framework for Computational Anatomy [Invited Paper], Computing and Visualization in Science, 5:1-12. 32. Evans AC, Collins DL, Neelin P, MacDonald D, Kamber M, Marrett TS (1994). Three-Dimensional Correlative Imaging: Applications in Human Brain Mapping, in: Functional Neuroimaging: Technical Foundations, Thatcher RW, Hallett M, Zeffiro T, John ER, Huerta M [eds.], 145-162. …….. 8