TU/e
advertisement

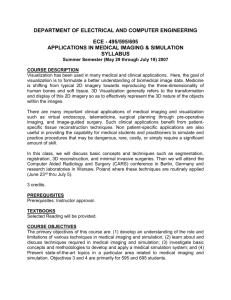
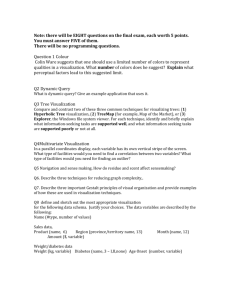
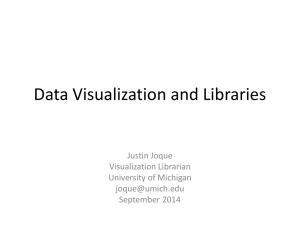
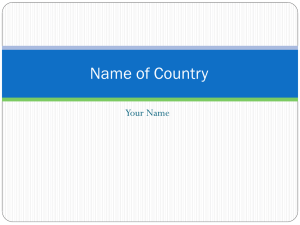
9 Image Processing on Diagnostic Workstations from simple PACS viewing into a really versatile BART M. TER HAAR ROMENY viewing environment. This chapter gives an overProfessor, Eindhoven University of Technology, Department of Biomedical Engineering, Image Analysis and Interpretation, PO Box 513, WH 2.106, 5600 MB Eindhoven, The Netherlands view of these developments, aimed at radiologists’ readership. Many references and internet links are given which discuss the topics in more depth than is possible in this short paper. This paper is CONTENTS necessarily incomplete. 9.1 Introduction 9.2 Hardware 9.3 Software 9.4 3D Visualization 9.5 Computer Aided Detection (CAD) 9.6 Atlases Syngo X, GE Advantage, etc.). There are dedicat- 9.7 CAD/CAM Design ed companies for viewing software (a.o. Merge 9.8 Diffusion Tensor Imaging (DTI) - Tractography eFilm) or OEM solutions (a.o. Mercury Visage, 9.9 Registration Barco). The application domain of workstations is 9.10 RT Dose Planning increasing. We now see them regularly employed 9.11 Quantitative Image Analysis in PACS and teleradiology diagnostic review, 9.12 Workstations for Life Sciences 9.13 Computer-Aided Surgery (CAS) 9.14 New Developments 9.15 Outlook Viewing stations are core business in a radiologist’s daily work. All big medical imaging industries supply professional and integrated environments (such as Philips ViewForum, Siemens 3D/3D-time (4D) visualization, computer-aided detection (CAD), quantitative image analysis, computer-assisted surgery (CAS), radiotherapy treatment planning, and pathology. Also the appli- References cations for medical image analysis in the lifesciences research are increasing, due to the inScientific terms marked with are explained in Wikipedia: www.wikipedia.org creased attention to small-animal scanning systems for molecular imaging, and the many types of advanced microscopes (such as confocal mi- 9.1 Introduction Medical workstations have developed into the superassistants of radiologists. The overwhelming production of images, hardware that rapidly became cheaper and powerful 3D visualization and quantitative analysis software have all pushed the developments croscopy and two-photon laser scanning microscopes), all giving huge 3D datasets. The focus of this chapter is on image processing (also termed image analysis or computer vision) applications. 9.2 Hardware plains why increasing the RAM of a slow computer can markedly upgrade its performance. In a Early systems were based on expensive hardware PACS system, the disk storage is typically done platforms, called workstations, often based on the on a ‘redundant array of inexpensive disks’ UNIX operating system . Today, most systems are (RAID), where many disks in parallel prevent based on readily available and affordable PC and loss of data in case of failure of a component. Mac hardware platforms (running MS-Windows or Mac-OS respectively), which are still following Moore’s law of increasing performance (a doubling every 24 months) at a stable price level. The central processor unit (CPU) is the core of the system, running today at several Gigahertz, and performance is expressed in Giga-FLOPS (109 floating point operations per second). Famous CPUs are the Intel Pentium chip, and the AMD Athlon processor. Today, we see the current 32 bit processors being replaced by 64 bit processors, which are capable of processing more instructions simultaneously and addressing a larger number of memory elements (232 = 4.2 × 109, so a 32 bit system cannot have more than 4.2 GB of memory(109 = Giga)). There is also a trend to have more CPUs (‘dualcore’) on the motherboard, paving the way to parallel processing, which is currently still in its infancy. The memory in the diagnostic workstation is organized in a hierarchical fashion. From small to large: the CPU has a so-called cache on its chip, as a local memory scratchpad for super-fast access, and communicates with the main RAM (random access memory, today typically 1–4 GB) through the data bus, a data highway in the computer. As the RAM is fully electronic, access is fast (nanoseconds), Fig. 9.1a–c. Brain aneurysm (a) and carotids (b): much faster than access to a local hard disk (milli- examples of volume renderings with a computer seconds). When the RAM is fully occupied, the CPU game graphics card (3Mensio Inc) (c) starts communicating with the hard disk. This ex- The speed of the network should be able to They have finally become fully programmable accommodate the network traffic. Typically the (and can be instructed by languages as DirectX workstation is part of a local area network (LAN). and OpenGL) and are equipped with 1– Today gigabit/second speeds are attained over wired 1.5 gigabytes of local memory. These ‘games’ networks, wireless is slower (30–100 Mbit/s) but hardware boards are now increasingly used in 3D convenient for laptops and ‘person digital assistants’ medical visualization applications (a.o. 3Mensio (PDAs). Many PACS installations can be serviced Medical Systems). There is also a community ex- remotely through LAN connections to the supplier, ploring the use of GPUs for general processing anywhere. (DICOM undated a). Networks are so fast nowadays that 3D vol- The viewing screens of diagnostic work- ume rendering can be distributed from a central stations have to be of special diagnostic quality. powerful computer to simple (and thus low cost) Excellent reviews of the important parameters viewing stations, called ‘thin clients’ (a.o. Ter- (resolution, contrast, brightness, 8, 10 or 12 bit arecon Aquarius). A powerful dedicated graphics intensity range, homogeneity, stability, viewing board (in this case the VolumePro 1000) with dedi- angle, speed, etc. are available in the so-called cated hardware runs several 3D viewing applications white papers by a variety of vendors (a.o. Barco – simultaneously, and is remotely controlled by the BARCO undated, Eizo – EIZO undated). users of the thin clients. Advantage is the capability to handle huge datasets (e.g. > 3000 slices) easily, but scalability (to e.g. dozens of users) is limited. cessing units’ (GPU , the processor on the video card (or graphics accelerator card) in the system) has increased even faster than CPU power, mainly due to the fact that GPUs form the core of the computer game industry. The millions of systems needed for this lucrative market and the high competition between the market leaders NVIDIA and ATI have created a huge performance/price ratio. A GPU has a 50 times faster communication speed of the data internally between memory and processor, and has dedicated hardware for rendering artificial environ Software The revolution in PACS (and teleradiology) view- Interestingly, the power of ‘graphical pro 9.3 ing stations was fired by the standard “Digital Imaging and Communications in Medicine” (DICOM) standard (DICOM undated a), 4000 pages). In the 1990s the ACR (American College of Radiology) and NEMA (National Electrical Manufacturers Association) formed a joint committee to develop this standard. The standard is developed in liaison with other standardization organizations including CEN TC251 in Europe and JIRA in Japan, with review also by other organizations including IEEE, HL7 and ANSI in the USA. It is now widely accepted. Convenient short ments, such as texture mapping , pixel shaders and tutorials are available (BARCO undated). As the an intrinsic parallel design with pixel pipelines . scanners and viewing software continue to devel- op, new features have to be added to the standard into lower languages, like C, C++, Java. When continuously. Vendors are required to make availa- ultimate speed (and limited variability) is required, ble their so-called conformity statements (see for the code can be implemented in hardware (GPU, example BURRONI et al. 2004), i.e. a specified list of field programmable gate array’s (FPGA), dedi- what conforms to the current version of the standard. cated chips, etc.). Many packages offer software The second revolution was the standardiza- development kits for joint development (e.g. tion of the internal procedural organization of medi- MevisLab by MEVIS, ‘Insight Segmentation and cal data handling in the ‘Health Level 7’ standard Registration Toolkit’ (ITK) by NLM, etc.). (HL7) (DICOM undated a). The basic function of a viewing station is the convenient viewing of the data, with a patient selection section. The functions are grouped in a so-called ‘graphical user interface’ (GUI). Versatile PC based viewing packages are now widely available (see RSNA 2006 for an extensive list), many also offering ‘extended ASCI’ character sets for the Chinese, Japanese and Korean markets. 3D Visualization The first breakthrough in the use of workstations has been by the invention of generating realistic 3D views from tomographic volume data in the 1980s. Now 3D volume rendering is fully interactive, at high resolution and real-time speed, and with a wide variety of options, making it a nontrivial matter to use it. Basic functions of the GUI include administrative functions as patient and study selection, report viewing and generation, and visualization functions as cine loop, ‘maximum intensity projection’ 9.4 Many dedicated companies are now established (such as Vital Images with Vitrea, Mercury Computer Systems with Amira, Barco with Voxar, 3Mensio with 3Vision, Terarecon with Aquarius, (MIP), ‘multi-planar reformatting’ (MPR ) including oblique and curved reconstructions, cut planes, etc.). Often a third party 3D viewing application is integrated in the PACS viewing application, and measurement tools for distances and angles, magni- supplied as a complete system by such an ‘original fying glass, annotations, etc. equipment manufacturer’ (OEM). The development of computer vision algorithms often follows a hierarchical pathway. The design process (rapid prototyping) is done in high- The principle of ray tracing (‘rendering’) (NOWINSKI et al. 2005) is actually based on mimicking the physics of light reflection with the level software (examples are Mathematica , Maple, Matlab), where very powerful statements and algebraic functionality make up for very short code, but his is difficult to extent to the huge multi- computer: the value of a pixel in a 2D image of a 3D view (also called a 2.5D view) is calculated from the reflected amount of light from a virtual light source, either bouncing on the surface of the dimensional medical images. When the formulas are 3D data (this process is called ‘surface render- understood and stable, the implementation is made ing’), or as the summation of all contributions Fig. 9.3. Virtual colonoscopy with unfolding enables inspection of folds from all sides. From VILANOVA ET AL. (2003) from the inside of the 3D dataset along the line of tings possible, users often get confused, and a the ray in question, composed with a formula that standard set of settings is supplied, e.g. for lung takes into account the transparency (or the in- vessels, skull, abdominal vascular, etc., or a set of verse: the opacity) of the voxels (this process is thumbnails is given with examples of presets, called ‘volume rendering’). from which the user can choose. Attempts are underway to extract the optimal settings from the statistics of the data itself (NOWINSKI et al. 2005). In virtual endoscopy (e.g. colonoscopy) the camera is positioned inside the 3D dataset. Challenges for the computer vision application are the automatic calculation of the optimal path for the fly-through through the center of the winding colon, bronchus or vessel. Clever new visualizations have been designed to screen the foldings in the colon for polyps at both the forward as backward pass simultaneously: unfolding (VILANOVA 2003) (see Fig. 9.3) and viewing an unfolded cube (VOS et al. 2003) (see Fig. 9.4). Fig. 9.2. Volume rendering of the heart and coronaries (Terarecon Inc) Segmentation is the process of dividing the 3D dataset in meaningful entities, which are The user can change the opacity settings then visualized separately. It is essential for 3D by manipulating the so-called ‘transfer func- viewing by, e.g. cut-away views, and also, unfor- tion’, this function giving the relation between tunately, one of the most difficult issues in com- the measured pixel value from the scanner and puter vision. It is discussed in more detail in the opacity. As there is an infinite number of set- Sect. 9.5. When clear contrasts are available, such as in contrast enhanced CT or MR angiography and bone structures in CT, the simple techniques of thresholding and region growing can be em- 9.5 Computer Aided Detec- tion (CAD) ployed, up to now the most often used segmenta- One of the primary challenges of intelligent soft- tion technique for 3D volume visualization. ware in modern workstations is to assist the human expert in recognition and classification of disease processes by clever computer vision algorithms. The often used term ‘computer-aided diagnosis’ may be an overstatement (better: ‘computer-aided detection’), as the final judgement will remain with the radiologist. Typically, the computer program marks a region on a medical image with an annotation, as an attention sign to inspect the location or area in further detail. The task for the software developer is to translate the Fig. 9.4. Unfolded cube projection in virtual colo- detection strategy of the expert into an efficient, noscopy. From VOS et al. (2003) effective and robust computer vision algorithm. Modern techniques are also based on (supervised This also explains the popularity of maximum intensity projection, where pixels in the 2.5D view are determined from the maximum along each ray from the viewing eye through the dataset (such a diverging set of rays leads to a so- and unsupervised) ‘data mining’ of huge imaging databases, to collect statistical appearances. E.g. learning the shape and texture properties of a lung nodule from 1500 or more patients in a PACS database is now within reach. Excellent called ‘perspective rendering’ ). As this may easily lead to depth ambiguities, often the more appealing ‘closest vessel projection’ (CVP) is applied, where the local maximum values closest to the viewer is taken. The sampled points of the (oblique) rays through the dataset are mostly located in between the regular pixels, and are calculated by means of interpolation. reviews exist on current CAD techniques and the perspectives for CAD (DOI 2006; GILBERT and LEMKE 2005). The field has just begun, and some first successes have been achieved. However, there is a huge amount of development still to be done in years to come. Some advances in CAD techniques that have brought good progress are in the following application areas. Fig. 9.5a–c. Virtual colonoscopy with surface smoothing. a Original dose (64 mAs); b 6.25 mAs; c 1.6 mAs. From PETERS (2006b) Mammography: this has been the first field where commercial applications found ceeding some threshold are possible candidates for further inspection. ground, in particular due to the volume produc- The location of the nipple is important as tion of the associated screening, the high resolu- a general coordinate origin for localization refer- tion of the modality and the specific search tasks. ences with, e.g. previous recordings. The general Typical search tasks involve the automated detec- statistical ‘flow’ of line structures points towards tion of masses, micro-calcifications, stellate or the nipple; the location can reasonably well be spiculated tumors, and the location of the nipple. found by modelling the apparent statistical line How do such algorithms work? Let us structure with physical flow models. look in some detail to one example: stellate tumor The role of MRI in breast screening is ris- detection (HOFMAN et al. 2006). As breast tissue ing. As in regular anatomical scans, too many consists of tubular structures from the milk- false negative detections are found, and current glands to the nipple, tumor extensions may pref- attention now focuses on dynamic contrast en- erably follow these tubular pathways. In a projec- hanced MRI. The rationale is the high vascularity tion radiograph this leads to a spiculated or star- of the neoplasm, leading to a faster uptake and shaped pattern. The computer will inspect the outwash over time of the contrast medium com- contextual environment of each pixel (say 50 × pared to normal tissue. Current research focuses 50 pixels) on the presence of lines with an orien- on the understanding of this vascular flow pattern tation pointing towards the relevant pixel. In this (e.g. by two-compartment modelling) and the way a total of 2500 ‘votes’ are collected for each optimal timing of the image sequence. pixel. The pixels with a voting probability ex- Polyp detection in virtual colonography: 9.6 Atlases polyps are characterized by a mushroom-like extrusion of the colon wall, and can be detected by The use of interactive 3D atlases on medical their shape: they exhibit higher local 3D curva- workstations is primarily focused on education ture (‘Gaussian curvature’) properties. These and surgery. As an example, K.-H. Höhne’s pio- can be detected with methods from ‘differential neering Voxel-Man series of atlases (HOFMAN et geometry’ (the theory of shapes and how to al. 2006) was initiated by the ‘visible human pro- measure and characterize them), and highlighted ject’. Atlases for brain surgery (e.g. the Cerefy as, e.g. colored areas as attention foci for further Brain atlas family; NOWINSKI et al. 2005) now inspection. become probabilistic, based on a large number of Methods have been developed to carry out patient studies. an electronic cleansing of the colon wall when contrast medium is still present. An interesting current target is possible to reduce strongly the radiation dose of the CT scan, and still be able to detect the polyp structures, despite the deterioration of the detected colon wall structures. Clever shape smoothing techniques and edge-preserving smoothing of the colon surface have indeed enabled a substantial dose reduction. Thorax CAD: here the focus is on the automated detection of nodules in the high resolution multi-slice CT (MSCT) data, on the detection of pulmonary emboli, and of textural analysis by Fig. 9.6. The famous Voxel-Man atlas explored classification of pixels, e.g. for the quantification many types of optimal educational visualization. of the extent of sarcoidosis. See SLUIMER et al. From HÖHNE (2004) (2006) for a review. Other CAD applications include calcium scoring, used to detect and quantify calcified cor- 9.7 CAD/CAM Design onary and aorta plaques, analysis of retinal fundus images for leaking blood vessels as an early Workstations can also assist in the creation of indicator for diabetes, and the inspection of skin implants from the 3D scans of the patients. This spots for melanoma (of particular attention in is a highly active area in ENT, dental surgery, Australia). orthopedic surgery and cranio-maxillofacial sur- gery. Many design techniques have been devel- ment and register the DTI data with anatomical oped to create the new shapes of the implants, data, and find fiber crossings and endings auto- e.g. by mirroring the healthy parts of the patient matically. An interesting development is the pho- of the opposite side of the body, 3D region grow- torealistic rendering of the tiny bundle structures ing of triangulated ‘finite element models’ in the (with specularities and shadows), based on the assigned space, etc. The ‘standard tesselation physics of the rendering of hair. language’ (STL) is a common format to describe surfaces for 3D milling equipment for rapid prototyping, such as stereolithography systems, plastic droplets ditherers, five-axes computerized milling machines, laser powder sintering systems, etc. Many dedicated rapid prototyping companies exist (e.g. Materialize Inc., see also www.cc.utah.edu/~asn8200/rapid.html). In the medical arena several large research institutes are active in this area (Ceasar, Berlin; Co-Me, Zürich). Fig. 9.7. Muscle fibers tracked in a highresolution DTI MRI of a healthy mouse heart. 9.8 Diffusion Tensor Imaging (DTI ) – Tractography Lighting and shadowing of lines combined with color coding of helix angle (h). From PEETERS et al. (2006a) Three-dimensional (3D) visualization of fiber tracts in axonal bundles in the brain and muscle fiber bundles in heart and skeletal muscles can 9.9 Registration now be done interactively. The images are no longer composed of scalar (single) values in the Registration, or matching, is a classical technique voxels, but a complete diffusion tensor (a 3 × 3 in image analysis (HAJNAL et al. 2001). It is em- symmetric matrix) is measured in each voxel. ployed to register anatomical to anatomical, or The three so-called eigenvectors can be anatomical to functional data, in any dimension. calculated with methods from linear algebra; Examples are MRI-CT, PET-CT, etc. The con- they span the ellipsoid of the Brownian motion struction of a PET and a CT gantry in a single that the water molecules make at the location of the voxels due to thermal diffusion. Complex mathematical methods are being investigated to group the fibers in meaningful bundles, to seg- system effectively solves the registration problem for this modality. The matching can be global (only translation, orientation and zooming of the image as a whole) or local (with local deformation, also of the imaging beam) can be enhanced by such called warping). Registration can be done by techniques as (adaptive) histogram equalization. finding correspondence between (automatically detected) landmarks, or on the intensity landscape 9.11 Quantitative Image itself (e.g. by correlation). There is always an Analysis entity (a so-called functional) that has to be minimized for the best match: e.g. the mean squared distance between the landmarks, a Pierson correlation coefficient, or others. In particular, for multi-modality matching, the mutual information (MI) has been found to be an effective minimizer. As an example, in MRI bone voxels are black and in CT white; they show as a This is the fastest growing application area of medical workstations. The number of applications is vast, every major vendor has research activities in this area, and many research institutes are active. To quote from the scope of ‘Medical Image Analysis’, one of the most influential scientific journals in the field: “The journal is interested in approaches cluster in the joint probability histogram of the MR vs CT intensities. The MI is a measure of entropy (disorder) of this histogram. that utilize biomedical image datasets at all spatial scales, ranging from molecular/cellular imaging to tissue / organ imaging. While not limited to 9.10 RT Dose Planning these alone, the typical biomedical image datasets of interest include those acquired from: magnetic The accuracy of radiotherapy dose calculations, based on the attenuation values of the CT scan of the patient, needs to be very high to prevent un- resonance, ultrasound, computed tomography, nuclear medicine, X-ray, optical and confocal microscopy, video and range data images. derexposure of the tumor and overexposure of the healthy tissue. Typically the isodose surfaces are calculated and viewed in 3D in the context of the local anatomy. Increasingly the images made in the linear accellerator with the electronic portal imaging device (EPID) are used for precise localization of the beam and repeat positioning of the patient, by precise registration techniques. The low contrast images (due to the high voltage The types of papers accepted include those that cover the development and implementation of algorithms and strategies based on the use of various models (geometrical, statistical, physical, functional, etc.) to solve the following types of problems, using biomedical image datasets: Fig. 9.8. Multimodality MRI of atherosclerotic plaque in the human carotid artery: (w1) T1-weighted 2D TSE, (w2) ECG-gated proton density-weighted TSE, (w3) T1-weighted 3D TFE, (w4) ECG-gated partial T2-weighted TSE, (w5) ECG-gated T2-weighted TSE. Middle: Feature space for cluster analysis. Right: classification result. From HOFMAN et al. (2006) Representation of pictorial data, visualiza- are MICCAI, CARS, IPMI, ISBI and SPIE MI. In tion, feature extraction, segmentation, inter-study the following some often-used techniques are and inter-subject registration, longitudinal / tem- shortly discussed. There are excellent tutorial poral studies, image-guided surgery and interven- books (MOLECULAR tion, texture, shape and motion measurements, YOO 2004) and review papers for the field. VISUALIZATIONS undated; spectral analysis, digital anatomical atlases, sta- Segmentation is a basic necessity for tistical shape analysis, computational anatomy many subsequent viewing or analysis applica- (modelling normal anatomy and its variations), tions. Mostly thresholding and 2D/3D region computational physiology (modelling organs and growing are applied, but these often do not give living systems for image analysis, simulation and the required result. Proper segmentation is noto- training), virtual and augmented reality for thera- riously difficult. There are dozens of techniques, py planning and guidance, telemedicine with such as model-based segmentation, methods medical images, tele-presence in medicine, tele- based on statistical shape variations (‘active surgery and image-guided medical robots, etc.” shape models’), clustering methods in a high- See also the huge amount of toolkits for dimensional feature space (e.g. for textures), his- computer vision: http://www.cs.cmu.edu/~cil/v- togram-based methods, physical models of con- source.html. Important conferences in the field tours (‘snakes’, level sets), region-growing methods, graph partitioning methods, and multi- e.g. MUSICA (‘Multi-Scale Image Contrast Am- scale segmentation. plification’, by Agfa), and the Swedish Con- The current feeling is that fully automated textVision (http://www.contextvision.se/). En- segmentation is a long way off, and a mix should hancement is often used to cancel the noise- be made between some (limited, initial) user- increasing effects of substantially lowering the X- interaction (semi-automatic segmentation). ray dose, such as in fluoroscopy and CT screen- Feature detection is the finding of specif- ing for virtual colonoscopy. ic landmarks in the image, such as edges, corners, Quantitative MRI is possible by calculat- T-junctions, highest curvature points, etc. The ing the real T1 and T2 figures from the T1 and T2 most often used mathematical technique is multi- weighted acquisitions, using the Bloch equation scale differential geometry (TER HAAR ROMENY of MRI physics. Multi-modal MRI scans can be 2004). It is interesting that the early stages of the exploited for tissue classification: when different human visual perception system seem to employ MRI techniques are applied to the same volume, this strategy. each voxel is measured with a different physical Image enhancement is done by calculat- property, and a feature space can be constructed ing specific properties which then stand out rela- with the physical units along the dimensional tive to the (often noisy) background. Examples axes: e.g. in the characterization of tissue types in are the likeness of voxels to a cylindrical struc- atherosclerotic lesions with T1, T2 and proton ture by curvature relations (‘vesselness’), edge density weighted acquisitions, fat pixels tend to preserving smoothing, coherence enhancing, cluster, as do blood voxels, muscle voxels, calci- tensor voting, etc. Commercial applications are, fied voxels, etc. Pattern recognition techniques like neural net- set of variable shapes and performing a ‘principal works and Bayesian statistics may find the component analysis’, a well known mathemati- proper cluster boundaries. cal technique. The first eigenmode gives the main Shape can be measured with differential variation, the second the one but largest, etc. Fit- geometric properties, such as curvature, saddle ting an atlas or model-based shape on a patient’s points, etc. It is often applied when, e.g. in the organ or segmented structure becomes by this automated search for (almost) occluded lung ves- means much more computationally efficient. sels in pulmonary emboli, polyps on the colon Temporal analysis is used for bolus track- vessel wall, measuring the stenotic index, spicu- ing (time-density quantification), functional maps lated lesions in mammography, etc. A popular of local perfusion parameters (of heart and brain), method is based on ‘active shape models’, contrast-enhanced MRI of the breast, cardiac out- where the shape variation is established as so- put calculations by measuring the volume of the called shape eigenmodes by analyzing a large left ventricle over time, multiple sclerosis lesion growth / shrinkage over time, regional cardiac ity. The source images are from two-photon wall thickness variations and local stress/strain microscopy, where the collagen is specifically calculations, and in fluoroscopy, e.g. the freezing colored with a collagen specific molecular imag- of the stent in the video by cancellation of the ing marker. motion of the coronary vessel. Another example is the detailed study of the micro-vascular structure in the goat heart 9.12 Workstations for Life Sciences from ultra-thin slices of a cryogenic microtome (degree of branching, vessel diameter, diffusion and perfusion distances, etc.). Typical resolution In life sciences research a huge variety of (high dimensional) images is generated, with many new types of microscopy is 25–50 micron in all directions, with datasets of 20003. (confocal , two-photon , cryogenic transmission electron microscopy, etc.) and dedicated (bio-) medical small animal scanners (micro-CT, mini PET, mouse-MRI, etc.). The research on molecular imaging and molecular medicine is still primarily done in small animal models. Fig. 9.10. A 3D visualization of a microtome stack (40×40×40 m) of the micro-vasculature of a goat heart (VAN BAVEL et al. 2006) [BENNINK 2006] This research arena will benefit greatly in Fig. 9.9a,b. Two-photon florescence microscopy of collagen fibers of tissue-engineered heartvalve tissue. a Result of structure preserving de- the near future from the spectacular developments in the diagnostic image analysis and visualization workstations. noising. From DANIELS et al. 2006 There is great need for quantitative image analysis. An example is, e.g. the measurement of quantitative parameters that determine 9.13 Computer-Aided Surgery (CAS) the strength of newly engineered heart valve tissue of the patient’s own cell line, such as collagen fiber thickness, local orientation variation and tortuos- In the world of CAS some very advanced simulation and training systems (KISMET, Voxel-Man) have been created. Especially in dental implants, craniofacial surgery and laparoscopic surgery there are many and highly advanced systems today. Surgical navigation workstations are routinely displaying the combination of the anatomy and the position and orientation of the instruments in the operating theatre. Fig. 9.12a–c. Abdominal aorta aneurysm: a color coding of displacement (mm); b Von Mises strain; c Von Mises stress (kPa). From DE PUTTER et al. (2005) 9.14 New Developments The visual perception of depth (when viewing 3D) data is helped enormously if the viewer can Fig. 9.11. Virtual laparoscopy trainer (Origin: For- move the data himself. There are many depth schungszentrum Karlsruhe KISMET) cues (stereo, depth from motion, depth from per- An interesting development is the use of complex fluid dynamics modelling, which enables the prediction of rupture chances in abdominal aorta surgery, and selecting optimal therapeutic procedures with bypass surgery in the lower aorta. In neurosurgery workstations can be employed in the calculation of an optimal (safest) insert path for electrodes for deep brain stimulation (DBS), based on a minimal costs path avoiding blood vessels and ventricles, and starting in a gyrus. Workstations assist in inter-operative visualization by warping the pre-operative imagery to the real situation in the patient during the operation, by intra-operative MRI, or ultrasound. spective), but depth from motion is the strongest. That is why maximum intensity projections (MIP) are preferably viewed dynamically. By self-tracking also the muscle’s proprioceptors are giving feedback to the brain, adding to the visual sensation. The combination with human’s superb eye-hand coordination has led to the concept of the Dextroscope (www.dextroscope.com), where a (computer generated) view or object can be manipulated under a half-transparent mirror, through which the viewer sees the display. Displays can also be equipped with haptic (tactile) feedback systems, which are now commercially available. References Fig. 9.13. Stereo viewing and manipulation with haptic feedback Super-large screens, and touch screens are becoming popular; a new trend is the multi-touch screen (http://cs.nyu.edu/~jhan/ftirtouch/ with movie), where multiple positions to interact simultaneously make more complex transformations possible, such as zooming, multiple simultaneous objects interactions, etc. 9.15 Outlook We have actually just started with exploiting the huge power these super assistants can add, in any of the fields discussed above – hardware, software and integration. Image processing plays an essential role, be it for visualization, segmentation, computer-aided detection, navigation, registration, or quantitative analysis. There will be an ever greater need for clever and robust algorithms: it is the conviction of the author that the study of human brain mechanism for the inspiration for such algorithms has a bright future to come (TER HAAR ROMENY 2004). The radiologists will benefit from these super-assistants, and finally: the patient has the best benefit of all. Barco (2007) White Papers Barco (screens, DICOM): http://www.barco.com/medical/en/downloads/whit epapers.asp?dltype=15 Bovik AC (ed) (2000) Handbook of image and video processing (communications, networking and multimedia). Academic Press Burroni M et al. (2004) Melanoma computer-aided diagnosis: reliability and feasibility study. Clin Cancer Res 10:1881–1886 Daniels F, ter Haar Romeny BM, Rubbens MP, van Assen HC (2006) Quantification of collagen orientation in 3D engineered tissue. In: Ibrahim F (ed) Proc Int Conf on Biomedical Engineering BioMed 2006, Kuala Lumpur, Malaysia, pp 344–348 de Putter S, Breeuwer M, Kosea U, Laffarguec F, Rouet J, Hoogeveen R, van den Bosch H, Buthe J, van de Vosse F, Gerritsen FA (2005) Automatic determination of the dynamic geometry of abdominal aortic aneurysm from MR with application to wall stress simulations. Proc CARS, International Congress Series 1281, pp 339– 344 DICOM (2007a) standard: http://medical.nema.org/ DICOM (2007 b) conformance statement (example): https://www.merge.com/RESOURCES/pdf/dcs/dc s_efilm21.pdf Doi K (2006) Diagnostic imaging over the last 50 years: research and development in medical imaging science and technology. Phys Med Biol 51:R5–R27 Eizo (undated) White Papers Eizo (screens): http://www.eizo.com/support/wp/index.asp Gilbert FJ, Lemke H (eds) (2005) Computer-aided diagnosis. Special issue of British Journal of Radiology, vol. 78, British Institute of Radiology GPGPU (undated) General-purpose computation using graphics hardware, http://www.gpgpu.org/ Hajnal JV, Hill DLG, Hawkes DJ (eds) (2001) Medical image registration. CRC Health Level 7 (undated) Health Level 7, http://www.hl7.org/. See also regional sites: (Australia http://www.hl7.org.au/, UK http://www.hl7.org.uk/, Canada http://www.cihi.ca/hl7, etc.) Hofman JMA, Branderhorst WJ, ten Eikelder HMM, Cappendijk VC, Heeneman S, Kooi ME, Hilbers PAJ, ter Haar Romeny BM (2006) Quantification of atherosclerotic plaque components using in-vivo MRI and supervised classifiers”, Magn Reson Med 55:790–799 Höhne K-H (2004) VOXEL-MAN 3D-Navigator” (CDROM). Springer, Berlin Heidelberg New York Karssemeijer N (1995) Detection of stellate distortions in mammograms using scale-space operators. Proc. Information Processing in Medical Imaging, pp 335–346 Kaufman, Müller K (2005) Overview of volume rendering. The visualization handbook. Elsevier Molecular visualizations (undated) Molecular visualizations: http://molvis.sdsc.edu/visres/index.html Nowinski W, Thirunavuukarasuu S, Benabid G (2005) The Cerefy clinical brain atlas. Enhanced edition with surgical planning and intraoperative support (CDROM). Thieme Peeters THJM, Vilanova A, Strijkers GJ, ter Haar Romeny RBM (2006b) Visualization of the fibrous structure of the heart. Proc. 11th workshop on Vision, Modelling and Visualization. Aachen, Germany Peeters THJM, Vilanova A, ter Haar Romeny RBM (2006a) Visualization of DTI fibers using hairrendering techniques. In: Lelieveldt BPF, Haverkort B, de Laat CTAM, Heijnsdijk JWJ (eds) Proc ASCI 2006. Lommel, Belgium, pp 66–73 Peters JF, Grigorescu SE, Truyen R, Gerritsen FA, de Vries AH, van Gelder RE, Rogella P (2005) Robust automasted polyp detection for low-dose and normal-dise virtual colonoscopy. Proc CARS 2005, International Congress Series 1281, Berlin, Germany, pp 1146–1150 RSNA 2006 Exhibitor list: http://rsna2006.rsna.org/rsna2006/V2006/exhibitor _list/home.cfm Schaefer-Prokop CM, van Delden OM, Bouma H, Sonnemans JJ, Gerritsen FA, Lameris JS (2006) To assess the added value of a prototype computer-aided detection (CAD) system for pulmonary embolism (PE) in contrast-enhanced multi-detector computed tomography (CT) images. Proc Eur Conf of Radiology, Vienna, Austria, EPOS Poster Sereda P, Vilanova A, Gerritsen FA (2006) Automating transfer function design for volume rendering using hierarchical clustering of material boundaries. In: Sousa Santos B, Ertl T, Joy K (eds) Eurographics/IEEE VGTC Symposium on Visualization (EuroVis),Lisboa, Portugal, pp 243–250 Siggraph (undated) Ray tracing tutorial (SIGGRAPH): http://www.siggraph.org/education/materials/Hype rGraph/raytrace/rtrace0.htm Sluimer IC, Schilham AMR, Prokop M, van Ginneken B (2006) Computer analysis of computed tomography scans of the lung: a survey. IEEE Transactions on Medical Imaging, vol. 25, pp. 385–405 Sonka M, Michael Fitzpatrick J (eds) (2000) Handbook of medical imaging – vol. 2. Medical image processing and analysis. SPIE, Belligham, WA ter Haar Romeny BM (2004) Front-end vision and multiscale image analysis. Springer, Berlin Heidelberg New York ter Haar Romeny BM (2004) Front-end vision and multiscale image analysis. Springer, Berlin Heidelberg New York van Bavel E, Bakker EN, Pistea A, Sorop O, Spaan JA (2006) Mechanics of microvascular remodelling. A review. Clin Hemorheol Microcirc 34(1/2):35– 41 Vilanova A, Gröller E (2003) Geometric modelling for virtual colon unfolding. In: Brunnett, Harmann, Müller, Lisen (eds) Geometric modeling for scientific visualization. Springer, Berlin Heidelberg New York, pp 453–468 Vos FM, van Gelder RE, Serlie IWO, Florie J, Nio CY, Glas AS, Post FH, Truyen R, Gerritsen FA, Stoker J (2003) Three-dimensional display modes for CT colonography: conventional 3D virtual colonoscopy versus unfolded cube projection. Radiology 228:878–885 Voxel Man surgical workstation: http://www.uke.unihamburg.de/medizinische-fakultaet/voxelman/index_ENG.php Whitby J (2006) The DICOM Standard”, White paper Barco Inc, 2006. URL: http://www.barco.com/barcoview/downloads/Whit ePaper_DICOM.pdf Yoo TS (2004) Insight into images: principles and practice for segmentation, registration, and image analysis. AK Peters