Microsoft Word - IBB PAS Repository
advertisement

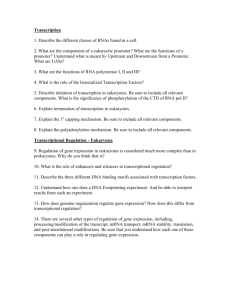
1. Title of the article. Coexistence of Gilbert’s syndrome with hereditary haemolytic anaemias. 2. Full name, postal address, e-mail, telephone number of the corresponding author. Professor Beata Burzynska, Institute of Biochemistry and Biophysics, Polish Academy of Sciences, ul. Pawińskiego 5A, 02-106 Warsaw, Poland; atka@ibb.waw.pl; 048 22 592 12 14 3. Full names, departments, institutions, city and country of all co-authors. Katarzyna Rawa1, Anna Adamowicz-Salach1, Michał Matysiak1, Anna Trzemecka2, Beata Burzynska2 1 Department of Paediatrics, Haematology and Oncology, Medical University of Warsaw, Warsaw, Poland 2 Institute of Biochemistry and Biophysics, Polish Academy of Sciences, Warsaw, Poland 4. Up to five keywords or phrases suitable for use in an index. Gilbert’s syndrome, hereditary haemolytic anaemia, UGT1A1genotyping, unconjugated hyperbilirubinemia, 5. Word count- excluding title page, abstract, references, figures and tables. 1447 ABSTRACT Background: Gilbert’s syndrome is an inherited disease characterised by mild unconjugated hyperbilirubinaemia caused by mutations in UGT1A1 gene which lead to decreased activity of UDPglucuronosyltransferase 1A1. The most frequent genetic defect is a homozygous TA dinucleotide insertion in the regulatory TATA box in the UGT1A1 gene promoter. Methods and results: A group of 182 Polish healthy individuals and 256 patients with different types of hereditary haemolytic anaemias were examined for the A(TA)nTAA motif. PCR reaction was performed using sense primer labelled by 6-Fam and capillary electrophoresis was carried out in an ABI 3730 DNA analyzer. The frequency of the (TA)7/(TA)7 genotype in the control group was estimated at 18.13%, (TA)6/(TA)7 at 45.05% and (TA)6/(TA)6 at 36.26%. There was a statistically significant difference in the (TA)6/(TA)6 genotype distribution between healthy individuals and patients with glucose-6-phosphate dehydrogenase deficiency (p=0.041). Additionally, uncommon genotypes: (TA)5/(TA)6, (TA)5/(TA)7 and (TA)7/(TA)8 of the promoter polymorphism were discovered. Conclusion: Genotyping of the UGT1A1 gene showed distinct distribution of the common A(TA)nTAA polymorphism relative to other European populations. Because of a greater risk of hyperbilirubinaemia due to hereditary haemolytic anaemia, the diagnosis of GS in this group of patients is very important. Gilbert’s syndrome (GS) is an inherited disorder characterised by mild unconjugated hyperbilirubinemia in blood. It has been estimated that 3-10% of the general population exhibit GS [1]. Unconjugated hyperbilirubinemia is caused by mutations in the UGT1A1 gene which encodes hepatic UDP-glucuronosyltransferase 1A1 (UGT1A1). Mutations lead to decreased activity of UDPglucuronosyltransferase 1A1 and lower bilirubin conjugation with UDP-glucuronic acid [2]. GS is a mild disorder and there is no requirement for treatment or long-term medical attention. The main symptom of the disease is increased level of serum unconjugated bilirubin usually diagnosed in routine laboratory tests. In Europeans, the most frequent genetic defect in the UGT1A1 gene described to date is a homozygous TA dinucleotide insertion in the regulatory TATA box - (TA)7/(TA)7 in the gene promoter [2, 3]. Healthy individuals have six TA repeats - (TA)6/(TA)6. The mutation leads to decreased activity of UDP-glucuronosyltransferase 1A1 by 30% and lower bilirubin conjugation with UDP-glucuronic acid and then the accumulation of serum bilirubin [4]. Hereditary haemolytic anaemias, such as hereditary spherocythosis, thalassaemias and glucose-6-phosphate-dehydrogenase deficiency are a group of disorders in which one of common symptoms is an increase level of serum bilirubin. The coexistence of Gilbert’s syndrome with haemolytic anaemia intensify hyperbilirubinemia and thus interfere with a exact diagnosis. Here, we report the prevalence of GS in patients with different types of haemolytic anaemia and in healthy individuals. We also discuss the presence of uncommon genotypes detected in Polish patients and healthy subjects. MATERIALS AND METHODS Analysis of the number of repeats in the UGTA1 gene promoter was performed on DNA samples from patients with confirmed hereditary haemolytic anaemia (65 with hereditary spherocytosis, 139 with β-thalassemia and 52 with glucose-6-phosphate dehydrogenase deficiency G6PD) from the Department of Paediatrics, Haematology and Oncology in Warsaw. Samples from 182 healthy individuals were collected in the Regional Centre of Blood Donation and Hemotherapy in Warsaw. Informed consent was obtained from all participants. This study was approved by the Ethical Committee of the Medical University of Warsaw, Poland. Genomic DNA was isolated from peripheral blood samples using the MagNA Pure Compact Nucleic Acid Isolation Kit I (Roche, Germany). The promoter region of the UGT1A1 gene was amplified by polymerase chain reaction (PCR) with F primer 5’ AAAGTGAACTCCCTGCTACC 3’ and R primer 5’ TGCTCCTGCCAGAGGTT 3’. The primers were designed basing on the GeneBank UGT1A1 sequence (NG_009254.1). The sense primer was labelled with 6-Fam on the 5’ end and with Tet on the 3’ end. PCR was performed using FastStart Taq DNA Polymerase with ready-to-use PCR Grade PCR Mix (Roche, Germany). Cycling conditions comprised 30 cycles of denaturation at 95º for 30 s, annealing at 52º for 30 s, and extension at 72º for 20 s. Following the PCR reaction samples were analysed in the DNA Sequencing and Oligonucleotide Synthesis Laboratory (Institute of Biochemistry and Biophysics, PAS). Samples were prepared for capillary electrophoresis by adding 1 µl of 5-times diluted PCR product to 5.7 µl of formamide and 0.3 µl of a GeneScan ROX 500 DNA ladder (Applied Biosystems, CA, USA) as an internal standard. The samples were then denatured for 5 min at 95°C and cooled to 4°C. Electrophoresis was performed in an ABI 3730 DNA Analyzer (Applied Biosystems, CA, USA) using a POP-7 polymer (Applied Biosystems, CA, USA). After electrophoresis the runs were analyzed visually using Peak Scanner Software v1.0 (Applied Biosystems, CA, USA). To confirm the obtained results, selected PCR fragments were sequenced directly with BigDye Terminators and appropriate primers using an ABI Prism 377 sequencer (Applied Biosystems, CA, USA). χ2 test was used to estimate allele frequencies in particular groups. Statistical analysis was done using STATISTICA data analysis software, version 9.1 (StatSoft, Inc., 2010, www.statsoft.com). RESULTS We determined the frequency of promoter polymorphisms of the UGT1A1 gene in 256 patients with hereditary haemolytic anaemia and 182 controls from the Polish population (Table 1). The frequency of the (TA)7/(TA)7 genotype in the control group was 18.13%, the (TA)6/(TA)7 genotype 45.05%, and (TA)6/(TA)6 -36.26%. Differences between all groups of hereditary haemolytic anaemias and healthy individuals were not statistically significant. However, the (TA)7/(TA)7 genotype was more prevalent in patients with spherocythosis (24.62%) and with G6PD deficiency (23.08%) in comparison with healthy individuals and thalassaemia patients. Additionally, we observed a statistically significant difference in the (TA)6/(TA)6 genotype distribution between healthy individuals and patients with glucose-6-phosphate dehydrogenase deficiency, where it was found in only 21.15% of patients (p=0.041). Table 1 Frequency of the UGT1A1 gene promoter variants in healthy individuals and in different groups of hereditary haemolytic anaemia in Polish population Patients Healthy individuals Hereditary spherocytosis β-thalassaemia G6PD Total (%) *p<0.05 Total Genotype - number of cases (%) 7/7 5/7 6/6 6/7 5/6 7/8 182 66 (36.26) 82 (45.05) 33 (18.13) 1 (0.55) 0 0 65 24 (36.92) 23 (35.38) 16 (24.62) 2 (3.08) 0 0 139 52 438 57 (41.00) 11 (21.15)* 158 (36.0) 55 (39.57) 29( 55.77) 189 (43.15) 25 (17.99) 12 (23.08) 86 (19.64) 0 0 3 (0.68) 1 (0.72) 0 1 (0.23) 1 (0.72) 0 1 (0.23) Extremely rare variants ((TA)5/(TA)6, (TA)5/(TA)7, (TA)7/(TA)8) of the promoter repeat were identified in Polish individuals (Figure 1). The (TA)5/(TA)6 and the (TA)7/(TA)8 genotypes was found only in the β-thalassaemia group but the (TA)5/(TA)7 genotype was found in the hereditary spherocytosis group and in the control group. These rare genotypes were not detected in the group of G6PD-deficient patients. DISCUSSION In this study we present the distribution of the most common TATA box genotypes in 438 Polish individuals. No similar data for Poland is available. The average frequency of the (TA)7/(TA)7 genotype, responsible for a decreased the expression of the UGT1A1 gene, was 19.64%. Several previous studies have reported the prevalence of the (TA)7/(TA)7 variant in European population of 610% [1, 4-8], significantly less than the result obtained in our study (Table 2). In contrast with European populations high frequency of (TA)7/(TA)7 allele was found in some area in Africa, like Nigeria [12], Cameroon, Ghana, southern Sudan and in Ethiopia [6]. On the other hand, there was no systematic, population-based studies on (TA)7 promoter sequence of UGT1A1 gene. Therefore, the discrepancy between our results and some published data may be due to differences between populations/ethnic groups or it may depend on the number of patients involved in the study. Table 2 Frequency of the UGT1A1 gene promoter variants in different European populations. ns - the A(TA)5TAA and A(TA)8TAA motifs were not studied/data of the A(TA)5TAA and A(TA)8TAA motifs not showed Population Polish Slovenian [1] Greek [4] Swedish [8] Sardinian [9] Scottish [10] Portuguese [11] Total 182 236 37 248 70 77 75 6/6 66 (36.26) 90 (38.10) 18 (48.65) 112 (45.16) 39 (55.71) 40 (31.00) 40 (53.33) Genotype - number of cases (%) 6/7 7/7 5/7 82 (45.05) 33 (18.13) 1 (0.55) 113 (47.90) 32 (13.6) 0 12 (32.43) 7 (18.92) ns 112 (45.6) 24 (9.68) ns 24(34.29) 7 (10.00) ns 38 (37.00) 12 (9.00) ns 29 (38.67) 5 (6.67) 1 (1.33) 5/6 0 0 ns ns ns ns 0 7/8 0 1 (0.40) ns ns ns ns 0 It has been reported that patients with hereditary spherocythosis or thalassemia minor and coinherited GS have a greater risk of developing gallstones [5, 7]. The knowledge of the possible coexistence of Gilbert’s syndrome and hereditary haemolytic anaemia would be crucial for an accurate diagnosis of the reason of an increased level of unconjugated bilirubin. Kaplan et al. [13] and Galanello et al. [10] have shown that there was no statistically significant difference in the frequency of (TA)7/(TA)7 among G6PD deficient patients and normal subjects. In our study, the distribution of the three common genotypes was similar in the control group and in the haemolytic anaemia groups. However, the occurrence of the normal (TA)6/(TA)6 genotype was statistically significant lower in G6PD-deficient patients than in healthy individuals and the number of G6PD-deficient patients with the (TA)7/(TA)7 genotype was higher in this group (statistically insignificant). This finding is important, because promoter variant has been shown to be responsible for hyperbilirubinemia during acute hemolytic anemia in G6PD-deficient patients [14]. In the present study we also discovered rarely observed A(TA)nTAA variants in the promoter region of the UGT1A1 gene. In an African population other variants of the TATA box have been identified: A(TA)5TAA and A(TA)8TAA [15]. The A(TA)5TAA motif does not affect transcriptional activity of the UGT1A1 gene, but patients with the A(TA)8TAA motif, similarly to those with the A(TA)7TAA motif, develop Gilbert’s syndrome [16]. (TA)5/(TA)6 causes a mildly elevated total serum bilirubin, (TA)5/(TA)7 prolonged neonatal jaundice, but (TA)7/(TA)8 genotype has a non-fasting total serum bilirubin that is even slightly higher than in most GS patients [10]. In fact, the (TA)7/(TA)7 variant is mostly observed in Caucasian and African populations whereas in Asians the prevalent mutation is G71R due to a change from G to A in nucleotide 211 in exon 1 of UGT1A1 gene [17]. Recently, several rare variants of the UGT1A1 gene promoter have been reported in Caucasians: a (TA)7/(TA)8 variant in an Italian girl [18], (TA)6/(TA)8 in a Greek boy [19], (TA)7/(TA)8 in two girls and (TA)5/(TA)7 in one subject in Portugal [11], and two subjects with (TA)7/(TA)8 and one with (TA)6/(TA)8 variant in Croatia [20]. Our investigation support the suggestion of Iolascon et al.[18] that the A(TA)8TAA motif in the UGT1A1 gene promoter is probably due to spontaneous mutation, because (TA)n repeats are particularly unstable and may be lengthened or shortened by a variety of mechanisms [18]. In conclusion, the genotyping of the UGT1A1 gene was carried out in the Polish population for the first time and the results showed a distribution of the common A(TA)nTAA variants slightly different than in other European populations. The present results could be relevant for Northern Europe as the earlier data were obtained mainly in the Mediterranean area. Additionally, we detected promoter variants that are very rare in the Caucasians. Moreover, the (TA)6/(TA)7 and (TA)7/(TA)7 genotypes occurred slightly more frequently in patients with G6PD deficiency. It is also noteworthy that such genotyping should be performed in hereditary haemolytic anaemia patients, as Gilbert’s syndrome is a risk factor for developing cholelithiasis. Competing interests: None declared. REFERENCES 1. Ostanek B, Furlan D, Mavec T, Lukac-Bajalo J. UGT1A1(TA)n promoter polymorphism - A new case of a (TA)8 allele in Caucasians. Blood Cells, Molecules, and Diseases 2007;38:7882. 2. Radu P, Atsmon J. Gilbert’s Syndrome – Clinical and pharmacological implications. IMAJ 2001;3:593-598. 3. Bosma PJ, Chowdhury JR, Bakker C, Gantla S, De Boer A, Oostra BA, Lindhout D, Tytgat GNJ, Jansen PLM, Ronald PJ, Elferink O, Chowdhury NR. The genetic basis of reduced expression of bilirubin UDP-glucuronosyltransferase 1 in Gilbert’s syndrome. The New England Journal of Medicine 1995;333(18):1171-1175. 4. Kalotychou V, Antonatou K, Tzanatea R, Terpos E, Loukopoulos D, Rombos Y. Analysis of the A(TA)nTAA configuration in the promoter region of the UGT1 A1 gene in Greek patients with thalassemia intermedia and sickle cell disease. Blood Cells, Molecules, and Diseases 2003;31:38-42. 5. Borgna-Pignatti C, Rigon F, Merlo L, Chakrok R, Micciolo R, Perseu L, Galanello R. Thalassemia minor, the Gilbert mutation, and the risk of gallstones. Haematologica 2003;88:1106-1109. 6. Horsfall LJ, Zeitlyn D, Tarekegn A, Bekele E, Thomas MG,5, Bradman N, Swallow DM. Prevalence of clinically relevant UGT1A allelesand haplotypes in African populations. Annals of Human Genetics 2011;75:236-246. 7. Rocha S, Costa E, Ferreira F, Cleto E, Barbot J, Rocha-Pereira P, Quintanilha A, Belo L, Santos-Silva A. Hereditary spherocytosis and the (TA)nTAA polymorphism of UGT1A1 gene promoter region--a comparison of the bilirubin plasmatic levels in the different clinical forms. Blood Cells Mol Dis 2010;44(2):117-119. 8. Mercke Odeberg J, Andrade J, Holmberg K, Hoglund P, Malmqvist U, Odeberg J. UGT1A polymorphisms in a Swedish cohort and a human diversity panel, and the relation to bilirubin plasma levels in males and females. Eur J Clin Pharmacol 2006;62:829–837. 9. Galanello R, Cipollina MD, Carboni G, Perseu L, Barella S, Corrias A, Cao A. Hyperbilirubinemia, glucose-6-phosphate dehydrogenase deficiency and Gilbert’s syndrome. Eur J Pediatr 1999;158:914-916. 10. Burchell B, Hume R. Molecular genetic basis of Gilbert’s syndrome. Journal of Gastroenterology and Hepatology 1999;14:960-966. 11. Costaa E, Vieirab E, Martinsc M, Saraivad J, Cancelae E, Costaf M, Bauerleg R, Freitash T, Carvalhoh JR, Santos-Silvai E, Barbotj J, dos Santosb R. Analysis of the UDPglucuronosyltransferase gene in Portuguese patients with a clinical diagnosis of Gilbert and Crigler–Najjar syndromes. Blood Cells, Molecules, and Diseases 2006;36: 91-97. 12. Kaplan M, Slusher T, Renbaum P, Essiet DF, Pam S, Levy-Lahad E, Hammerman C. (TA)n UDP-Glucuronosyltransferase 1A1 promoter polymorphism in Nigerian neonates. Pediatric Research 2008;63:109-111. 13. Kaplan M, Renbaum P, Levy-Lahad E, Hammerman C, Lahad A, Beutler E. Gilbert syndrome and glucose-6-phosphate dehydrogenase deficiency: A dose-dependent genetic interaction crucial to neonatal hyperbilirubinemia. Proc. Natl. Acad. Sci. USA 1997;94:12128-12132. 14. Beutler E, Gelbart T, Demina A. Racial variability in the UDP-glucuronosyltransferase 1 (UGT1A1) promoter: A balanced polymorphism for regulation of bilirubin metabolism? Proceedings of the National Academy of Sciences USA 1998;95:8170-8174. 15. Cappellini MD, Martinez di Montemuros F, Sampietro M, Tavazzi D, Fiorelli G. The interaction between Gilbert's syndrome and G6PD deficiency influences bilirubin levels. Br J Haematol 1999;104(4):928-929. 16. Mauro Y, Iwai M, Mori A, Sato H, Takeuchi Y. Polymorphism of UDP- Glucuronosyltransferase and drug metabolism. Current Drug Metabolism 2005;6:91-99. 17. Koiwai O, Nishizawa M, Hasada K, Aono S, Adachi Y, Mamlya N, Sato H. Gilbert's syndrome is caused by a heterozygous missense mutation in the gene for bilirubin UDPglucuronosyltransferase. Hum. Mol. Genet. 1995;4(7):1183-1186. 18. Iolascon A, Faienza MF, Centra M, Storelli S, Zelante L, Savoia A. (TA)8 allele in the UGT1A1 gene promoter of a Caucasian with Gilbert’s syndrome. Haematologica 1999;84:106-109. 19. Tsezou A, Tzetis M, Kitsiou S, Kavazarakis E, Galla A, Kanavakis E. A Caucasian boy with Gilbert’s syndrome heterozygous for the (TA)8 allele. Haematologica 2000;85:319-336. 20. Nikolac N, Simundic AM, Topic E, Jurcic Z, Stefanovic M, Dumic J, Goreta SS. Rare TA repeats in promoter TATA box of the UDP glucuronosyltranferase (UGT1A1) gene in Croatian subjects. Clinical Chemical Laboratory Medicine 2008;46(2):174-178. Figure 1. A chromatogram of the capillary electrophoresis of the UGT1A1 gene promoter. The red peak (139) represents an internal standard, the 135 peak (blue) represents the A(TA)5TAA motif, the 137 peak (blue) represents the A(TA)6TAA motif, the 139 peak (blue) the A(TA)7TAA motif, and 141 peak (blue) the A(TA)8TAA motif.