Tinnitus
advertisement

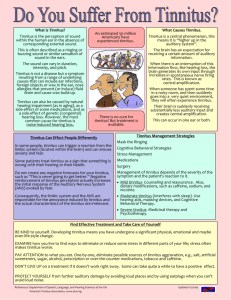
Tinnitus Grand Rounds – 1/20/99 Edward D. Buckingham, M.D. Jeff Vrabec, M.D., Faculty Sponsor Francis Quinn, M.D., Series Editor Introduction Tinnitus is defined as the perception of a sound produced involuntarily within the body. It may be the most prominent symptom of a disease process which is threatening the patient’s physical well being, or merely an associated symptom of a benign condition. The psychological effects of benign tinnitus can severely affect quality of life of the patient and their entire family. In severe cases, the psychological affects of tinnitus may even precipitate suicide. The physician must be knowledgeable of the causes of tinnitus, aware of the severe conditions associated with the symptom, able to make the diagnosis, and offer definitive treatment or symptomatic relief. Definition and Epidemiology Tinnitus, as defined above, may be divided into two major categories; objective, or tinnitus produced by paraauditory structures, usually from vascular or myoclonic sources; and subjective, or tinnitus generated by the sensorineural auditory system. 1,2 In general, tinnitus prevalence and severity increases with age mostly affecting those in the 40 to 70 year old age group and with equal sex distribution. A study by Axelsson and Ringdahl (1987) noted that 337 people with tinnitus were identified in a population of 2378 Swedes 1. Also of note was that the severity of effect on quality of life increased with age. In general, subjective or sensorineural auditory tinnitus is much more prevalent than objective tinnitus. For the practicing otolaryngologist these factors have important implications in today’s aging population. Objective Tinnitus Strictly, the definition of objective tinnitus is that which is audible to the physician or another person, but in practice this encompasses all causes which are paraauditory in nature; it may be pulsatile or non-pulsatile. The differential diagnosis includes; vascular abnormalities such as, neoplasms, arteriovenous malformations, arterial bruits, and venous hums; and muscle contraction tinnitus such as palatomyoclonus. The diagnosis of objective tinnitus begins with a thorough history and physical examination. The patient should be questioned about the nature of the tinnitus and its relation to the heart rate. Asking the patient to perform light physical activity may confirm the pulsatile nature. Physical exam should include a thorough otolaryngologic exam paying particular attention to the otoscopic exam looking for retrotympanic mass. Additionally, a thorough search should be made for an audible bruit with auscultation of the external canal, orbit, mastoid process, skull, and neck using both the bell and the diaphragm or electronic stethoscope if available. The remainder of the work-up will be lead by the history, physical findings, and the suspected diagnosis. All patients should receive an audiogram. Pulsatile tinnitus The list of causes of pulsatile tinnitus is extensive. It includes causes of increased intracranial pressure, carotid artery atherosclerosis, vascular tumors, heart murmers, arteriovenous fistulas, and others including idiopathic. An algorithm for the diagnosis of pulsatile tinnitus was recently published by Sismanis.3 The article recommends evaluation first by otoscopy. A retrotympanic mass requires a CT of the temporal bones looking for glomus tympanicum, aberrant carotid artery, and jugular bulb abnormalities. Glomus jugulare suspicion requires a CT of the neck and carotid angiography. If no retrotympanic mass is present, a decision must be made between suspicion of increased intracranial pressure, or carotid artery/cardiac abnormality. To evaluate suspicion of increased ICP a MRI-MRA and a neuroophthalmology consult should be obtained looking for intracranial abnormality or papilledema. If no hydrocephalus or other intracranial abnormality is present, lumbar puncture confirms the diagnosis of benign intracranial hypertension (pseudotumor) if the ICP is greater than 200 mm H 2O. Respectively, if carotid artery or cardiac abnormality is suspected a duplex ultrasound or echocardiogram should be performed. These may support the diagnosis of atherosclerotic carotid artery disease (ACAD), carotid tortuosity, or valvular heart defect with murmur. If a carotid lesion is still suspected and the duplex and 2 echo are normal an MRI-MRA or a carotid angiogram may be necessary. In general, the study found that history and physical examination are the two most important factors in evaluating patients with pulsatile tinnitus. BIH syndrome, ACAD, and glomus tumors compose two thirds of definable causes. 3 Benign intracranial hypertension (pseudotumor cerebri) syndrome BIH syndrome was the most common cause of pulsatile tinnitus in Sismanis’s recent study.3 The condition is characterized by increased ICP without focal neurologic signs, except for an occasional sixth or seventh nerve palsy. The pathophysiologic mechanism responsible for PT in these patients probably is secondary to the transmission of systolic pulsations of the CSF to the exposed medial aspect of the dural venous sinuses and the resulting periodic compression of their walls, which convert the normally laminar blood flow to turbulent. Diagnosis is made by LP and measurement of CSF pressure after a head imaging to rule out other etiologies of intracranial hypertension. Patients with BIH tend to be female age 20 – 50 and overweight. Pulsatile tinnitus subsides with light digital pressure applied over the ipsilateral internal jugular vein of the side with tinnitus. Other symptoms include blurred vision, fronto-occipital headache, and lightheadedness-disequilibrium. A mild low-frequency hearing loss may be present with excellent discrimination. The hearing loss normalizes after the elimination of the PT by applying light pressure over the ipsilateral IJV. Treatment of this syndrome consists of weight loss and administration of acetazolamide and furosemide. If these fail a subarachnoid-peritoneal shunt may be placed, and some patients have been relieved by gastric bypass for weight reduction.3 Vascular neoplasms The classic vascular tumors associated with pulsatile tinnitus are glomus tympanicum and glomus jugulare. Characteristics of vascular tumors on physical exam and radiography include the following. A bruit, if found, is not altered appreciably by light pressure on the neck, head position, posture, or Valsalva maneuver. Tympanometry may be useful showing regular perturbations which when plotting compliance as a function of time may be compared to the patient’s pulse rate. On otoscopy, a bluish or reddish mass is highly suggestive of a glomus tumor. Obvious pulsations of the mass and paling when positive pressure is applied by a pneumatic otoscope support this diagnosis, however, hemotympanum, dehiscent jugular bulb, and carotid artery abnormality must be considered, and radiographic studies should precede any surgical procedure such as myringotomy or exploratory tympanotomy. The physician should check the entire head and neck for masses. Cranial nerve and cerebellar function should be assessed as these tumors may involve these areas. If a glomus tumor is suspected, a CT scan should be obtained. It may show a mass in the middle ear space or erosion of the jugular spine. Additionally, arteriography should be performed to delineate feeder vessels and the tumor’s extent. MRI is also playing an increasingly important role. Treatment of these lesions is usually surgical. Arteriovenous malformations AVMs may be diffucult to differentiate from neoplasms. AVMs are developmental abnormalities and often are considerably more extensive than their symptoms suggest. These lesions may enlarge rapidly and tend to recur. They may impinge on adjacent structures, causing deformation by mass effect. The most common AVMs are those of the posterior fossa between branches of the occipital artery and transverse sinus. AVMs of the mandible are uncommon, but are notorious for causing tinnitus. Communications between the carotid artery and cavernous sinus, most often resulting from trauma, are infrequent but have serious consequences. Pulsatile tinnitus is often the initial complaint of the patient, but other symptoms include headache, and papilledema. They usually have a bruit and when palpable, exhibits a thrill and is generally more compressible than a tumor. If associated with a sufficiently large arteriovenous shunt, the heart rate may actually slow with compression. Treatment is usually surgical preceded by angiography and selective embolization of feeding vessels. As a general rule the lesion are larger than they appear on angiography. When adjuvant embolization is used, maximal benefit will be achieved if subsequent surgery is performed within 72 hours.1 3 Venous hum This entity results partially from the eddy currents in the jugular vein and are normally heard in the neck of many children and some adults, most notably, young women. These hums have been attributed to the transverse process of the second cervical vertebra, and states of increased cardiac output, such as anemia, thyrotoxicosis, and pregnancy. Often diagnosed when a hearing loss occurs in which external background noise is attenuated, once diagnosed, they are significant only for the tinnitus they produce. Placing gentle pressure on the anterior neck that does not occlude the carotid artery may eliminate the tinnitus. Turning the head toward the uninvolved side decreases the sound and turning toward the involved side makes it louder, as do deep breathing and Valsalva maneuver. Management consists simply of reassuring the patient and treating the underlying disorder.1 The complete list of causes of paraauditory tinnitus is quite extensive including atherosclerotic carotid artery disease, otosclerosis, jugular bulb abnormalites, abnormal condylar and mastoid emissary veins, and many more. All of these share a common pathphysiology of increased turbulence of blood flow. Pulsatile tinnitus should be called idiopatiic only after an extensive workup has been completed and specific diagnosis has not been reached. Palatomyoclonus The myoclonus form of tinnitus is described as an irregular clicking sound heard within the ear. The sound is rapid (20 to 400 beats per minute) and occurs intermittently. It is caused by the mucous membranes of the eustachian tube snapping together in response to the movement of the palatal musculature. Patients may also complain of fullness in the ear and distortion of hearing, and may have histories of other muscle spasm, including postoccipital spasm, temporomandibular joint problems, and blepharospasm. Diagnosis is made by auscultating the ear canal with a Toynbee tube for audible clicking. Tympanogram may show recording movement synchronous with the contraction, and electromyographic studies of the palatal musculature may confirm the diagnosis. Observable palatal fasciculation is associated with a CNS lesion in which there is hypertrophic degeneration of the inferior olive; these patients warrant an MRI to search for this lesion. Palatomyoclonus must be differentiated from tensor tympani spasm, which will have similar symptoms and findings except without palatal muscle contraction; tensor tympani spasm is usually transient. Treatment of palatomyoclonus initially consists of medications that include muscle relaxants such as clonazepam or diazepam, warm liquids, and stress management. Botulinum toxin injection into the active muscle may help in severe cases.2,4 Idiopathic stapedial muscle spasm This condition, in contrast to palatomyoclonus, tends to be a rough, rumbling, or crackling noise often accentuated or triggered by external noises such as voices, rattling of paper, or running water. The symptoms generally follow this exposure, are brief and intermittent, and rarely become disruptive and prolonged. Diagnostic studies include variable-intensity tympanometry in an effort to stimulate the spasm and aid diagnosis, and acoustic reflex testing which may demonstrate a prolonged, continued increased impedance during and after the sound stimulus.5 Primary treatment consists of muscle relaxants, clonazepam or diazapam. Because the symptoms may last only 2 or 3 months and then disappear for long periods, the use of surgery to divide the stapedius tendon should be used very conservatively.4 Subjective Tinnitus Subjective tinnitus, tinnitus originating within the auditory system, is far more common than objective tinnitus. As previously mentioned its prevalence increases with age and is related to hearing loss. Many theories exist and have been published about the underlying physiologic mechanisms that cause subjective tinnitus, but little is known. Generally, theories involve hyperactive hair cells or nerve fibers activated by a chemical imbalance across cell membranes or decoupling hair cell stereocilia.1 An alternate 4 theory proposes that injury to cochlear integrity from any cause reduces the suppressive influence of the central nervous system, allowing increased neuronal activity higher in the auditory system. 2 Whatever the cellular mechanism it appears that tinnitus can be caused by abnormal conditions in the cochlea, the cochlear nerve, the ascending auditory pathway, or the auditory cortex. Basic science review topics Auditory pathway Sound travels from the cochlear hair cells, which are innervated by the bipolar neurons of the spiral ganglion in the modiolus of the cochlea. The spiral ganglion cells make up the eighth nerve which then terminate on the cochlear nucleus. The axons of the cells in the cochlear nucleus stream out along three pathways: the dorsal acoustic stria, the intermediate acoustic stria, and the trapezoid body. The most important pathway is the trapezoid body. It contains fibers destined for the superior olivary nuclei on both sides of the brain stem. Axons arising from the superior olivary nuclei join the crossed and uncrossed axons from the cochlear nucleus to form the lateral lemniscus. Thus from the outset there is extensive bilateral auditory input in the central nervous system, so that lesions of the central auditory pathway do not cause monaural disability. The lateral lemniscus courses through the nuclei of the lateral lemniscus, where some fibers synapse, once again with crossing from the two sides through Probst’s commissure. All the fibers in the lateral lemniscus eventually synapse in the inferior colliculus. The inferior colliculus receives binaural input and its cells are arranged tonotopically. Most of the cells in the inferior colliculus send their axons to the medial geniculate body of the thalamus in the ipsilateral side of the brain. The cells in the medial geniculate body then send their axons to the ipsilateral primary auditory cortex in the superior temporal gyrus (Brodmann’s areas 41 and 42).6 Auditory brainstem response Auditory evoked responses are electrophysiologic recordings of responses to sound. With proper test protocols, the responses can be recorded clinically from activation of all levels of the auditory pathway from the cochlea to the cortex. The ABR or BAER, brainstem auditory evoked response is applied most often clinically. ABR wave components arise from the eighth cranial nerve and auditory regions in the caudal and rostral brainstem. Wave I unquestionably represents the synchronously stimulated compound action potentials from the distal (cochlear) end of the eighth cranial nerve. Wave II may also arise from the eighth nerve, but near the brainstem (the proximal end). Waves I and II are generated by structures ipsilateral to the ear stimulated. All later ABR waves have multiple generators within the auditory brainstem. Wave III, which is usually prominent, is generated within the caudal pons, with likely contributions from the cochlear nuclei, the trapezoid body, and the superior olivary complex. The most prominent and rostral component of the ABR, wave V, is thought to arise in the region of the lateral lemniscus as it approaches the inferior colliculus, probably on the side contralateral to the ear stimulated. 7 Of note, Ikner and Hassen (1990) found little difference between the auditory brainstem response in tinnitus and nontinnitus patients matched for hearing loss. Other work in this regard is ongoing. At present no measurements of sensorineural tinnitus or perceptual descriptions are pathognomonic of a single lesion.1 Evaluation In evaluating tinnitus patients several etiologic factors should be explored; these include otologic, cardiovascular, metabolic, neurologic, pharmacologic, dental, and psychological factors. A history of noise exposure and related symptoms such as hearing loss and vertigo should be obtained including the exact characterization of the tinnitus quality (buzzing, rushing, ringing, roaring, whistling), and perceptual location (one ear, both ears, head location). 1 Tinnitus has been related to head injury and whiplash injuries as well as a past history of meningitis. Multiple sclerosis can also have severe tinnitus in its constellation of symptoms. Many medications may produce tinnitus most notably aspirin and aspirin-containing compounds, aminoglycoside antibiotics, nonsteroidal antiinflammatory drugs, and heterocycline antidepressants. Temporomandibular joint disorders and dental abnormalities are prevalent in tinnitus 5 patients and some describe an increase in their TMJ complaints to be concurrent with an increase in their tinnitus. Psychologic factors play a major role in the patient’s perception of the tinnitus severity, and tinnitus is a prevalent symptom in somatoform disorder.8 Patients with concurrent depression should be treated for this disorder as well, which in some cases also shows reduction in tinnitus. 2 Audiometry should be performed on all patients, and anyone with asymmetrical hearing loss or unilateral tinnitus should undergo an MRI to rule out posterior fossa tumors. Additionally, the patient should be asked to complete one or more of the many questionnaires designed to evaluate the perceived severity of the tinnitus. Measurement of tinnitus Many tinnitus programs attempt to quantify four aspects of the tinnitus: pitch, loudness, minimum masking level, and residual inhibition or post-masking effects. The most clinically useful of these is probably minimum masking level, which may indicate the probability for success of a masking device. Briefly, although tinnitus does not usually resemble a single tone, most patients are able to equate the pitch elicited by a pure tone with the most prominent pitch of their tinnitus. However, most patients are unable to perform this task reliably with a high standard deviation and tendency to choose tones in one octave difference if tested repetitively. The loudness of tinnitus has been measured by having the subject adjust the level of a pure tone so that is has about the same loudness as the tinnitus. Most tinnitus is less than 7-db sensation level. Unfortunately, for some patients disabled by their symptoms, this loudness level may be as little as 2 dB. A band of noise centered at the pitch-masked tinnitus is presented from threshold to the level at which the patient’s sound is masked. The number of decibels of sound required to cover the tinnitus is the minimal masking level. Residual inhibition describes the phenomenon of patients experiencing periods of decreased or no tinnitus after having been exposed to masking. Post-masking effects published by Tyer took one of five wave forms: 1) returned to normal loudness immediately, 2) returned immediately but initially was softer, 3) was absent before gradually returning to normal, 4) was absent before abruptly returning to normal, 5) was louder before gradually returning to normal. 1 Diagnostic tests No diagnostic test is yet available to objectively measure or confirm the presence of tinnitus. However, many investigators have looked at such modalities as ABR, PET, spontaneous otoacoustinc emissions, and magnetic activity of the auditory system to determine an association with the complaint. Otoacoustic emissions OAEs are low-intensity sounds produced by the cochlea in response to an acoustic stimulus. Outer hair cell motility affects basilar membrane biomechanics, resulting in a form of intracochlear energy amplification, as well as cochlear tuning for more precise frequency resolution. The outer hair cell motility generates mechanical energy within the cochlea, which is propagated outward, via the middle ear system and the tympanic membrane, to the ear canal. Vibration of the tympanic membrane then produces an acoustic signal, which can be measured by a sensitive microphone. The two most studied subcatagories of OAEs in relation to tinnitus are spontaneous otoacoustic emissions (SOAE), and distortion product otoacoustic emissions (DPOAE). SOAEs, measurable in the external ear canal without stimulation, are present in only about 60% of persons with normal hearing, and are found twice as commonly in females as in males. Because tinnitus represents a spontaneous perception without any stimulus, it was quite reasonable to search for a direct correlate of the tinnitus that was emitted into the ear canal. Unfortunately, at present the relationship between spontaneous emission and tinnitus is unclear.1 DPOAEs, which are produced when two pure-tone stimuli at different frequencies are presented to the ear simultaneously, are present in all normal hearing individuals. When outer hair cells are structurally damaged or at least nonfunctional, OAE cannot be evoked by acoustic stimuli. For example, up to 30 % of a population of outer hair cells may be damaged without substantially affecting the simple audiogram. In such cases the evoked OAEs invariably are abnormal and can be used to detect this damage. While no 6 correlation between tinnitus patients and DPOAEs has been observed, many clinical applications for DPOAEs currently exist, and hope exists for a correlation to tinnitus. Norten et al have observed an oscillating or prolonged evoked emission in five of six tinnitus subjects, but none in two subjects without tinnitus. They suggested that “...the evoked emission and the tinnitus might be related to the same underlying pathology, but the former is not the cause of the latter.” 1,2 Treatment Counseling Initially, a general discussion with the patient regarding all the etiologic factors connected with the tinnitus should take place. The patient is reassured after the workup as to the unlikelihood of tumor or lifeendangering disease. The patient is told that in 25 percent of cases symptoms improve significantly or go away. In 50 percent of patients the symptoms decrease over a period of months, in only 25 percent do the symptoms persist at the same level, and reassurance is given that only a very small portion will have increased symptoms. Patients should be advised to avoid loud noise, or if unavoidable, to wear appropriate ear protection. They should restrict caffeinated beverages or any stimulants. Coffee, tea, colas, and chocolate are excluded or reduced. They should quit smoking as many patients report a decrease in their tinnitus with smoking cessation.4 Medications Medications the patient is currently taking may be the cause of the tinnitus; these should be reviewed. Aspirin-containing compounds, non-steroidal anti-inflammatory medications, and heterocycline antidepressants should be limited, reduced in dosage, or changed to attempt relief of tinnitus. The use of medication for the treatment of tinnitus has been largely ineffective. Drugs such as nicotinic acid (vitamin B6), carbamazepine, baclofen, and others have been tried and some even tested in double-blind placebo-controlled trials. None has been shown to be beneficial.1,9,10 Lidocaine has been studied in several carefully controlled double-blind studies and shown to be beneficial, however, lidocaine must be given intravenously, has a very short half-life, and is sometimes accompanied by undesirable side effects. Oral analogs of lidocaine such as tocainide and flecainide acetate were also attempted for relief without benefit. Melatonin, 3.0 mg qhs, was recently studied in a double-blind placebo-controlled trial and found to be no better than placebo at relieving tinnitus. However, among patients reporting difficulty sleeping attributable to their tinnitus, 46.7% reported an overall improvement after melatonin compared with 20.0% for placebo (p=0.04). Benzodiazepines also may be beneficial; clonazepam, oxazepam, and alprazolam; may all provide benefit, especially for patients with concurrent depression. In recent study 76% of patients taking alprazolam had a reduction in the loudness or their tinnitus while only 5% of the placebo group showed benefit.12 Overall, medication should not be the major strategy for the treatment of tinnitus, however for certain sufferers medication may provide some benefit in conjunction with other therapy. Environmental masking For cases of mild tinnitus, especially in individuals where the tinnitus is only bothersome in quiet situations, such as reading or sleeping, home environmental masking techniques may prove beneficial. This usually involves music or broad-band masking by placing the dial on the radio between FM stations at a loudness level to mask the tinnitus. This is particularly useful at night. The sound required to mask the tinnitus is soft and not necessarily disturbing to the patient or other family members.4 Hearing aids and maskers Because an external noise can render tinnitus inaudible in many patients, it seems reasonable to introduce such a noise to provide temporary relief. Saltzman and Ersner (1947) observed that a hearing aid amplified background noise that could successfully mask the tinnitus. Hearing impaired patients with 7 tinnitus probably should try a hearing aid before trying a tinnitus masker. A hearing aid interferes less with speech, does not produce an intense noise that could produce damage, and can improve speech understanding.1 Commercially available tinnitus maskers are also available either alone or in combination with a hearing aid. When using these devices the noise can either completely mask the tinnitus or partly mask it, so that both noise and tinnitus are heard, but the tinnitus is reduce in loudness. There are no clear guidelines for selecting the spectrum characteristic of the masking noise and no indications that measurements of pitch, loudness, or postmasking characteristics can be used to select an appropriate spectrum for the tinnitus masker. Narrwband noises (less than a half-octave bandwidth) have a tonal character, and those with a prominent tonal component are more annoying than broadband noise. A conservative approach would be to urge the patient to use the lowest level masker that provides adequate relief and to inform the patient that the masker need not be worn continuously. Additionally, there is no available protocol for deciding which ear to fit with a masker, and any combination, unilateral or bilateral may be affective. Electrical stimulation In the past several experiments were conducted on the use of electrical current to reduce tinnitus. Several authors have demonstrated that the use of direct current applied to the round window or promontory could reduce tinnitus. Unfortunately, direct currents (DC) may produce permanent damage and, therefore, cannot be used clinically. Other work has focused on using alternating current from an external stimulator with electrodes placed on the tympanic membrane, transtympanically on the promontory, and transcutaneously in the preauricular and postauricular regions of the ear. The results from these studies were mixed, but with some promising results even leading to one extracochlear wearable device to reduce tinnitus being marketed in the U.S. in 1985. However, Dobie et al. (1986) demonstrated that only 1 patient out of 20 clearly received benefit from the device. The product has been removed from the market.1 Fewer investigators have explored the use of intracochlear electricity to suppress tinnitus. Most of these reports have been observations that some cochlear-implant patients report a reduction in their tinnitus while listening to speech. A few patients have received a cochlear implant explicitly for tinnitus reduction and not to improve their hearing ability. JW House (1984) reported that WF House implanted devices in five severe-to-profoundly-hearing-impaired patients for tinnitus relief. No special stimuli were administered to these patients, and only one reported a reduction in tinnitus while listening to speech through the cochlear implant. Hazell et al. (1989) reported on six totally deaf patients who had received an intracochlear implant and additional experimental trials with sinusoidal stimuli. They were able to reduce the tinnitus in all six patients using a 100-Hz sinusoid. At least two of the patients elected to forego their speech processors and to use their implant to suppress their tinnitus. One reported that turning on the current turned off his tinnitus “like a light switch.”1 Surgery While surgery is effective in treating conditions for which tinnitus is an associated symptom, such as otosclerosis, acoustic neuroma, and glomus jugulare, destructive surgical lesions into the peripheral auditory system are mostly ineffective. Case reports exist in the literature describing successful selective cochlear neurectomy in patients who have lost all serviceable hearing in the affected ear, fail to respond to medical management, and accept the fact that their tinnitus may persist despite surgery. Additionally, microvascular decompression of the cochlear nerve has reported success in certain cases. A recent study by Vasama in patients with severe hearing loss, severe tinnitus, abnormal brainstem auditory evoked potentials, and in some abnormal acoustic middle ear reflex response claims in 22 patients: 7 had relief of their tinnitus, 8 were slightly improved, 4 did not change, and 2 worsened. This procedure, if performed, at all should be kept in the hands of surgeons experienced in the technique.14 Results from either of these techniques are at best inconsistent, and few otologists advocate their usage; validating the hypothesis that somehow tinnitus generators are centralized and are not consistently relieved by uncoupling the end organ. 1 8 Neurophysiological approach to Tinnitus and Habituation The neuorphysiological model of tinnitus has not been discussed previously and has been reserved until now because of its differences with the other theories of tinnitus production and how to treat it. The previously discussed theories share the beliefs that processes resulting in tinnitus were restricted to auditory pathways, and more-over, in the dominant majority of models, to the cochlea; and all models were focused on and concerned only with tinnitus generation, treating auditory pathways as passive, unchangeable transmitters of the signal to the auditory cortex. Consequently, diagnostic efforts were concentrated on psychoacoustical descriptions of tinnitus (its loudness, pitch, and maskability). Psychoacoustical characterization of tinnitus, however, did not turn out to be of any help in predicting treatment outcome, or explaining why people with similar descriptive characteristics had drastically different annoyance levels. The neurophysiological model postulates that tinnitus emerges as a result of the interaction of a number of subsystems in the nervous system. Auditory pathways play a role in the development and appearance of tinnitus as sound perception, whereas other systems, predominantly the limbic system are responsible for the tinnitus annoyance. The problem occurs when the perception of tinnitus is associated with negative emotions, induces fear, and has qualities of threat. Typical fears are expressed as, “I have a brain tumor; I am going deaf; etc.” The limbic system in turn activates the autonomic nervous system resulting in the feeling of annoyance. Because annoyance evoked by tinnitus in this model is primarily dependent on the activation of the limbic system, which is a perception by the individual and an associated emotional state, the psychoacoustical characterization of tinnitus is irrelevant. Habituation is traditionally defined as: the disappearance of reactions to sensory stimulus because of repetitive exposition of a subject to this stimulus and the lack of positive or negative reinforcement associated with this stimulus. In ordering tasks to be performed, the brain uses the following principles: 1) the importance of the signal, particularly if a signal has a negative connotation indicating danger; and 2) its novelty. If a signal has not been associated with any significant event or does not indicate danger, and is not new, it gradually undergoes habituation, and after a number of repetitions, a person does not consciously perceive its presence. This is accomplished by directive counseling aimed at educating the patient of the potential mechanisms of tinnitus, presented within a background of the physiology of the auditory nervous system. As part of the counseling, the results of all audiologic and medical tests are presented, and their relevance discussed. Once the patient feels that he or she understands the mechanisms of tinnitus and its impact, the level of annoyance decreases and by repetitive, less intensive counseling during follow-up visits, it is possible to eliminate the negative associations initially evoked by tinnitus. Beginning the process of habituation by directive counseling is an essential step of the treatment, but it is not sufficient to achieve permanent habituation. To facilitate the habituation to tinnitus perception, it is advisable to enhance the level of auditory background surrounding the patient, ie. partial masking, particularly when he or she is in a quiet environment. This procedure increases the background level of spontaneous and evoked activity within the auditory pathways, and by reducing the contrast of the tinnitus signal versus background, the process of habituation is facilitated. It is of utmost importance, however, to avoid masking tinnitus completely. By definition, once a tinnitus signal is masked it cannot be habituated to. This supposition reflects the fact that habituation is basically a reconditioning of connections within subcortical centers, and this process cannot occur if the stimulus (tinnitus) is absent. An example of this is a patient who had undergone tinnitus masking for fifteen years without any changes in his tinnitus, any indications of habituation of tinnitus perception, or tinnitus-induced annoyance. After about a year of habituation therapy with the use of low- level broad-band noise, this patient is only aware of tinnitus for a small percentage of the time, and the annoyance induced by tinnitus decreased significantly as well. Patients are fitted binaurally with broad-band noise generators, which have a reasonably stable amplitude of sound and allow for a smooth increase of sound from the zero level. The patients are advised to use the devices for at least 6 h per day, particularly when they are in a quiet environment. In patients with hearing loss, hearing aides are also used with instructions on how to create the proper auditory environments (to use the hearing aid not as an aid in communication, but as a tool for enhancing the 9 auditory input to the brain). The process of habituation typically requires 12 months and Jastreboff insists that the patients continue for another 6 months to ensure that plastic changes within the brain are firmly established. After that time period use of the noise generators is no longer necessary. He reports approximately 83% of patients exhibit significant improvement with this combined therapy .15 Summary It is important to differentiate between the different types of tinnitus. A physician must recognize when tinnitus is a symptom of a potentially life threatening condition verses a problematic annoyance for the patient. Patience and understanding of what the patient is experiencing, including their fear is essential. Tinnitus produced by paraauditory structures is usually treatable through accepted medical therapy. The treatment of sensory neural tinnitus is less clear, but recent advances in theory and management are encouraging. 10 References 1) 2) 3) 4) 5) 6) 7) 8) 9) 10) 11) 12) 13) 14) 15) Tyler, Richard S., Babin Richard W., Tinnitus, In Cummings, editor: Otolaryngology Head and Neck Surgery, 2nd ed., Mosby, 1993. Schleuning, Alexander J., Tinnitus, In Bailey, B.J., editor: Head and Neck Surgery – Otolaryngology, 2nd ed., Lippincott – Raven, 1998. Sismanis, Aristides, Pulsatile Tinnitus, The American Journal of Otology, 19:472-477, 1998, July. Schleuning, Alexander J., Tinnitus, In Gates, editor: Current Therapy in Otolaryngology Head and Neck Surgery, 5th ed., Mosby, 1994. Marchiando, Albert, Tinnitus Due to Idiopathic Stapedial Muscle Spasm, Ear, Nose, and Throat Journal, 62:8-13, Jan 1983. Kelly, James P., Hearing, In Kandel, editor: Principles of Neural Science, 3rd ed. Appleton & Lange, 1991. Hall, James W., Assessment of Peripheral and Central Auditory Function, In Bailey, B.J., editor: Head and Neck Surgery – Otolaryngology, 2nd ed., Lippincott – Raven, 1998. Wolfgang, Hiller, Association Between Tinnitus and Somatoform Disorders, Journal of Psychosomatic Research, 43:613-624, 1997. Westerberg, Brian D. A Double-Blind Placebo-Controlled Trial of Baclofen in the Treatment of Tinnitus, The American Journal of Otology, 17:896-903, 1996. Hester, T. Oma, Cyclandelate in the management of tinnitus: A randomized, placebo-controlled study, Oto HNS, 118(3 Pt 1):329-332, 1998 Mar. Rosenberg, Seth I., Effect of Melatonin on Tinnitus, The Laryngoscope, 108:305-310, March 1998. Johnson, Robert M., Use of Alprazolam for Relief of Tinnitus, Arch Otolaryngol Head Neck Surg, 119:842-845, 1993 Aug. Wazen, Jack J., Selective Cochlear Neurectomy for Debilitating Tinnitus, Ann Otol Rhinol Laryngol, 106: 568-570, 1997. Vasama, Juha-Pekka I., Microvascular decompression of the cochlear nerve in patients with severe tinnitus. Preoperative findings and operative outcome in 22 patients, Neurological research, 20:242247, 1998 Apr. Jastreboff, Pawel J., Neurophysiological Approach to Tinnitus Patients, The American Journal of Otology, 17:236-240, 1996 Mar. 11