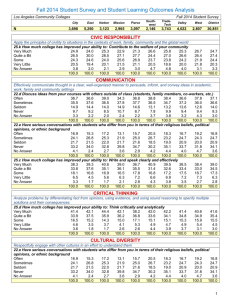
student information - Los Angeles Southwest College
advertisement

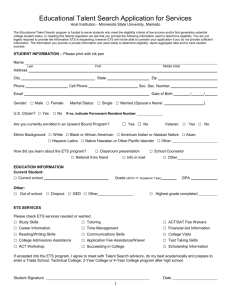
EDUCATIONAL TALENT SEARCH @ LOS ANGELES SOUTHWEST COLLEGE 1600 W. IMPERIAL HWY., Los Angeles, CA 90047 ▪ (323)242-5523 ▪ Fax: (323) 242-5524 (Complete in Blue or Black Ink Only) Return complete applications to ETS staff or school counselor PARTICIPANT & LIABILITY WAIVER Student’s Name: ____________________________ Birth date:_____________________________ Parent/Guardian Name:_____________________________________________________________ PARENTAL CONSENT As a parent and/or legal guardian of the student listed above, I/we authorize and permit my child to participate in any and all academic year and summer component activities (classes, tutorials, advisement sessions, workshops, field trips, work study internships, meetings, field trips, etc.) sponsored and/or conducted by the Educational Talent Search Program at Los Angeles Southwest College. I/we also give permission for my child to be transported between his/her school, the college campus, and the scheduled events when the ETS program has scheduled events for its participants. I/we do hereby grant permission to the Educational Talent Search Program at Los Angeles Southwest College and its authorized representatives, to furnish first aid as my son/daughter may require, as well as to seek medical attention through the nearest medical facilities when students are on field trips, on campus, or other authorized activities. This permission is conditional upon the understanding that in the event of serious illness or the need for hospitalization and/or major surgery, ETS will use all reasonable efforts to contact me. Failure in such efforts should not prevent ETS from providing emergency STUDENT SCHOOL RECORDS RELEASE AUTHORIZATION I/we authorize Educational Talent Search Program at Los Angeles Southwest College to obtain documents relative to and consistent with my child’s education. Such documents may include: a copy of my child’s school transcript, test scores, ACT/SAT or CAHSEE/GED scores, and school lunch program eligibility. I/we authorize ETS to obtain documents related to my child’s application to or receipt of student financial aid assistance (federal, state, or other), a copy of my award notification from college financial aid office, and college admissions information. I/we understand the information above will be used to monitor my child’s academic performance, assist in providing academic advisement, determine program eligibility, and help with their college planning. I/we understand school records will only be used by ETS and will not be shared with any other group. The Family Educational Rights and Privacy Act (FERPA)e 20 U.S.C. 1232g, is the federal law providing for review and disclosure of student educational records. The TRIO Programs at Los Angeles Southwest College will not permit access to or the release of personally identifiable information contained in the student educational records to any party without the written consent of the student, except as authorized by FERPA. I certify by signing below I am agreeing to all the information below. Parent/Guardian Signature:* ___________________________ Date: _______________ EDUCATIONAL TALENT SEARCH @ LOS ANGELES SOUTHWEST COLLEGE 1600 W. IMPERIAL HWY., Los Angeles, CA 90047 ▪ (323)242-5523 ▪ Fax: (323) 242-5524 Return complete applications to ETS staff or school counselor (Complete in Blue or Black Ink Only) STUDENT INFORMATION * REQUIRED INFORMATION _______________________________ Last Name ________________________________ First Name _______________________________ Middle Name Street Address* ______________________________________ Apt#________ City* _______________________________ Zip Code*____________ Date of Birth*____________ * Email ___________________________________________Facebook:________________________________________ Home* (______)_____________________________ Gender* Male Female Cell (______)_______________________ Alt (_____)________________________ Do you have any learning disabilitues? Yes No Unknown Ethnicity:* African- American (Black) Asian Caucasion Hispanic (Latino) Native American Pacific Islander Other Citizenship Status:* US Citizen Permanent Resident If yes, what is your Alien Registration #: _____________________ Other _______________________ EDUCATIONAL BACKGROUND * REQUIRED INFORMATION School Attending:* Do you participate in any of the following programs? Check all that apply: Washington Preparatory Animo-Locke 1 Animo Locke 2 Animo Locke 3 Animo-Locke Tech Middle School 3 Middle School 4 Bret Harte Other _____________ Educational Talent Search MESA Gompers Other_________________ *Do you wish to attend college/university after high school? Yes Grade:__________ AVID Upward Bound No Uncertain If yes, where ______________________ Grade Point Average: __________ PARENT OR GUARDIAN INFORMATION * REQUIRED INFORMATION ___________________________________________ Print Father/Guardian’s name* ___________________________________________ Print Mother/Guardian’s Name* ___________________________________________ Relationship to Student* ___________________________________________ Relationship to student* (_____)________________ Phone Number * (______)____________________ Cell Phone (______)_______________ Phone Number * (_____)__________________ Work ___________________________ Email Address (______)_________________ Work (______)__________________ Cell Phone __________________________ Email Address DO YOU HAVE A U.S. FOUR-YEAR COLLEGE DEGREE?*: DO YOU HAVE A U.S. FOUR-YEAR COLLEGE DEGREE?*: Y ES NO YE S NO HOUSEHOLD INFORMATION * REQUIRED INFORMATION Does anyone in your household receive any of the following? *SIZE OF FAMILY?: __________(# LIVING IN HOUSEHOLD) (please check all that apply). WHAT IS YOUR TAXABLE FAMILY INCOME FOR LAST CALENDAR YEAR?: *Please check the appropriate $0-16,335 $16,336-22,065 $22,066-27,795 $27,796-33,525 $33,526-39,255 taxable income box:* $39,256-44,985 $44,986-50,715 $50,716-56,445 $56,446+ Unemployment Disability Public Assistance Veteran’s Benefits Social Security Free/Reduced Lunch Program at School Ward/Dependent of court Otro: ______________ All information is kept confidential. This data is used to determine if your child is eligible for this federally funded program. I certify the information provided above is correct to the best of my knowledge. Incomplete applications will not be accepted and returned to student. Student Signature:*_____________________________________________ Parent/Guardian Signature:* _____________________________________ Date___________ Date___________ This program is 100% federally funded by U.S. Department of Education ($232,780 per year). Information provided above is necessary to determine if your child is eligible to participate in program. Information is protected by Privacy Act. For Office Use Only: Date of entry: ________________ Class of: ___________ Letter Sent: _________________ Eligibility: LI/FG LI FG OTHER Application Complete Academic Advisor: _________________________ Program Coordinator: ______________________