тheme № 4 a

MINISTRY OF THE HIGH AND MIDDLE EDUCATION OF THE REPUBLIC OF
UZBEKISTAN
MINISTRY OF HEALTH OF THE REPUBLIC OF UZBEKISTAN
TASHKENT MEDICAL ACADEMY
«Approved» by vice
rector on academic affairs
prof. Teshayev O. R._______
«_____» _________ 2013.
Chair: Traumatology orthopedics, MFS with neurosurgery.
Subject: Traumatology and orthopedics.
For medicol-prophylactic faculty
Subject: Basic principles of treatment of injuries of the chest and shoulder area.
SWS - Dyupyuitrena contracture. Tendon injuries of extremities
United methodical system
Practical occupation №4
TASHKENT-2013
Originators:
Head of the Traumatology - orthopedics, MFS with neurosurgery cathedra: MD Karimov. M Yu. manager of a teaching department: Salokhiddinov. F.B.
The technology of training is approved:
Azizova F.H. prof – chief of studying department of the TMA.
Discussed and recommended to approving
Head of the cycle subject section of medico-prophylactic faculty
Professor: B.M. Mamatkulov
Practical occupation No.4
Theme: Basic principles of treatment of injuries of the chest and shoulder area.
SWS - Dyupyuitrena contracture. Tendon injuries of extremities
Technology of studying lesson
Time: 225 min
Form and type of studying lesson
Students: 10-12
Practical lesson
Structure of Practical lesson
1. Introduction.
2. Theoretical part.
3. Analytic part.
- Case-study
- Tests and task
4. Practical part.
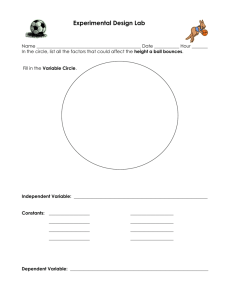
Aim of studying lesson: To form of skills and to improve knowledge of students in feature patient’s examination with damages of the musculoskeletal system. To teach interpretation of X-ray, prepare and set of splinting.
Student should know: - know, how to find anterior superior crista of iliac bone
- know, how to measure
- to find relative length
- to find absolute length
- to find length of the hip and shin
Student should know:
To make practical skills: to teach anthropometric methods exam traumatlogical patient.
Obligations of teachers:
To introduce, characterize, explain and teach anthropometric methods exam traumatlogical patient.
Methods and technique of studying
Form of studying lesson
Material of studying
Results of studying activity:
To count anthropometric methods:
Giving expand characteristics to each methods;
Name in steps anthropometric methods;
To make up, determine and plan methods investigation of traumatlogical patient.
Case, interactive games, lection
Individual work, group work, collective work.
Handbook, movies, photos, books.
Studying materials, X-rays, studying movies, tourniquet, splint material.
Condition of studying Auditoria for work with group.
Monitoring and assessment: Oral control: control questions, carry out tasks in group.
Writing control: control questions, to find relative and absolute length of lower extremity
Technological card of studying lessons in theme: «Fractures of pelvis bones»
Work stage Contain of activity
Teacher Students
The I stage –
Introduction in educational occupation
1.1. Calls an occupation subject, its purpose, tasks and planned results of educational activity.
Listen
Write down
(10 mines)
5 minutes
1.2. Acquaints with an operating mode on occupation and criteria of an assessment of results (see methodical instructions for students).
1.3. Explains appointment a case-study and its influence on development of professional knowledge.
Independently study contents of a case and individually fill a leaf of the analysis of situations.
1.4. case study materials also acquaints with a situation analysis algorithm (see methodical instructions for students).
1.5. Gives a task independently to carry out the analysis and to bring results in «A leaf of the analysis of a situation».
II stage 2.1. Carries out quiz on purpose to make active knowledge being trained on a subject:
Answer questions.
- features of inspection of patients with diseases the ODE;
- features of inspection of patients with damages the ODE;
- concept about diagnostics of injury of bones;
- concept about diagnostics of injury of joints;
- idea of a traumatism on production;
- measures of prevention of a traumatism on production;
2.2. Divides students into groups.
Reminds work rules in group and ruled discussions.
2.3. Gives a task:
Share on groups.
To carry out and discuss results of individual work with a case (sheets of the analysis of a situation) in mini-groups;
To estimate and choose optimum options of actions for measures of prevention of a traumatism on production;
Carry out educational task.
To be prepared for presentation.
Change an
2.4. Coordinates, advises, directs
Main 30 minutes. educational activity.
Checks and estimates results of individual work: sheets of the analysis of a situation.
2.4. Coordinates, advises, directs educational activity.
Checks and estimates results of individual work: sheets of the analysis of a situation.
2.5. Will organize presentation following the results of the done work on the solution of a case, discussion and a assessment.
Change
2.6. Makes comments, pays attention to the actions chosen in the course of the analysis for measures of prevention of a traumatism on production.
Groups hold presentation of results of work. Participate in discussion, questions, estimate. ask
2.7. Reports the version of the decision.
2.8. Will organize performance by students of practical skills
Measurement of relative and absolute length of the bottom extremity
Physical examination of patients
III stage final and estimated
10 minutes.
3.1. Sums up to occupation, generalizes results of educational activity, declares, estimates individual and collaboration.
Listen
3.2. Emphasizes value a case stage and its
influence on development of future expert.
3.3 Gives homework.
Express the opinion
Write down
1.
INTRODUCTION
1.1 PLACE OF LESSONS
Chair: Traumatology orthopedics, MFS with neurosurgery and auditoria.
Traumatology department of 2-nd clinics of TMA
Thematic patients and volunteers, plan of games, handbooks, materials, banners, movies and photos.
Modern investing technology, panel structure,
1.2. Motivation: knowing features Surgical methods of treatment in traumatology and orthopedics. Reparative regeneration of a bone fabric gives students possibility to complex exam patients and measure of prophylactics traumatism in industry.
1.3. between and intra subject relations: teach this theme is based at student’s knowledge by anatomy, topographic anatomy, radiology, surgery and reanimation.
2. theoretical part.
2. 1. Contain of lessons:
Theoretical part.
Injuries of a thorax - quite frequent type of damages, in practice of fast and urgently the help borrowing from 5,7 to 10 % of all injuries of a body of the person.
The thorax is a receptacle of such important bodies as heart and lungs, and plays a paramount role in the breath act. Therefore injuries of a thorax can represent big danger to life.
All injuries of a thorax share on opened and closed, on traumas with damage and without injury of bones, with injury of a pleura and an internal and without that.
Closed injuries of a thorax are a main type of damages of a peace time. At most, with what it is put damage, places of the appendix of this force and the trauma mechanism
(the blow, a thorax shock wave etc.) depend weight, depth, nature of damage and respectively its clinical manifestations (bruises, hematomas of a chest wall, an injecting of skin etc.).
On degree of a traumatization of a wall of a thorax it is impossible to judge gravity of an internal injury. So, it is wrong to consider that the usual fracture of edges can't be connected with serious injury of lungs.
The most frequent injury of a thorax are fractures of edges. Among all closed injuries of a thorax they make from 40 to 80 %.
On the trauma mechanism fractures of edges can be divided on direct, indirect and separated. At a direct change the edge breaks where the traumatization force damaging as well soft fabrics of a thorax is directly enclosed. At an impressing of the broken edge inside there is an angular shift fragments. If external force influences an edge closer to a backbone, it causes a change as shift: central fragment remains on a place, and peripheral - mobile and long - it is displaced inward. The double fracture of one edge occurs as a change (simultaneous impact of direct and indirect influence).
The multiple fracture of edges is usually accompanied by considerable shift fragment, especially at double changes. Separated fractures of edges (with IX and below) are characterized by big shift fragment, torn off from an edge.
At a fracture of edges them fragment can injure a pleura and a lung, and also intercostal vessels that is accompanied by bleeding in a cavity pleurae
(pheumothorax). Besides, hemorrhages in lungs (more often in the bottom shares) from small superficial to very extensive, occupying the whole share are possible.
Ruptures of a pulmonary fabric of the various sizes with damage of vessels and bronchial tubes aren't excluded also.
The fracture of edges always burdens and without that a serious general condition of the patient owing to hypoxemia development (a lack of oxygen).
Symptoms. Pain on a damage place, morbidity at a thorax impression in the front and back direction. Respiratory movements short and superficial. The pain syndrome sharply amplifies at cough. The patient feels in situation sitting better, than lying.
Treatment. First aid by the victim with fractures of edges and their further treatment are directed on knocking over (elimination) of a pain syndrome, simplification of external breath and prevention of pneumonia which very often develops at multiple
fractures of edges at elderly people. Carrying out this occupation gives the chance to the being trained the X-ray of pictures, local anesthesia a place of a change, preparation of plaster bandages, imposings of splint and circular plaster bandages, delivery of the preliminary diagnosis and definition of further tactics of maintaining the patient will familiarize with the basic principles of rendering of the first medical care, to inspection methods, types of anesthesia, principles of an immobilization, interpretation.
Training of students, on this this subject, is based on knowledge of human anatomy, topographical anatomy and operative surgery, radiology, anesthesiology resuscitation and sheathe surgeries.
To congenital defects of development of the musculoskeletal device, meeting at children of early and preschool age, the congenital clubfoot, congenital dislocation of a hip and a congenital muscular wryneck belong. The congenital clubfoot — is a contracture of joints of foot. The disease meets at boys more often, the clubfoot happens one - and bilateral. The main clinical signs of a congenital internal clubfoot are: plantar bending of foot in an ankle joint, turn of a plantar surface inwards with lowering of external edge of foot, mainly tarsi and metatarsuses, foot reduction in forward department at simultaneous increase in the arch of foot — hollow foot.
Congenital clubfoot treatment consists in special correlation gymnastics, bandaging which needs to be begun on the first month of life of the kid and at an easy form of deformation leads to an absolute recovery. Certainly, massage – very effective means is necessary. At averages and heavy forms of an illness plaster bandages are applied.
If treatment begins after 2х years, it demands operation before which to the child carry out treatment in the form of stage plaster bandages.
Congenital dislocation of a hip - most frequent of congenital deformations of the musculoskeletal device. When speak about frequency of this pathology, mean not only the created dislocation of a femur which is seldom observed in the first days of life, and a so-called displasy (the wrong arrangement of a head of a femur) against which dislocation subsequently can be formed. At children of early age meets twoand unilateral dislocation, and at girls more often than at boys. The outcome depends on timely diagnosing of an illness and an initiation of treatment. The diagnosis of a displasy of hip joints put in maternity hospital, with the same purpose in children's policlinic of all babies (till 3 months) the surgeon-orthopedist examines. The most frequent symptoms of a congenital displasy of a hip joint is the following: assignment restriction in hip joints; click; asymmetry of folds on a hip and buttock folds behind; shortening of the bottom extremity measured by eye. The listed symptoms can be observed either at the same time everything, or only a part, in the latter case it is necessary to suspect a congenital displasy of a hip joint and to make a X-ray. If at the baby the diagnosis of a displasy isn't established, when it starts to stand and go,
diagnostics of congenital dislocation of a hip comes easy. At children after a year one of characteristic symptoms is the late beginning of walking: the first steps in 14 — 15 months, and also typical gait — is noted instability, lameness — at unilateral dislocation, duck, rolling-over gait at bilateral dislocation. Treatment of a displasy of hip joints is necessary for beginning at once after diagnosis establishment on which term the way of treatment depends also. Treatment can be conservative and operative and if the diagnosis is established on the first year of life, conservative treatment is always applied. Congenital muscular wryneck: A wryneck — the neck deformation, being characterized the wrong position of the head (an inclination sideways and its turn). There is a wryneck owing to pathological changes in soft fabrics, mainly in
SCM muscle. The specified deformation is more often happens right-hand and meets at girls. There is also a bilateral wryneck. The congenital wryneck can be diagnosed on 2 — the 3rd week of life of the child. On the struck party as a result of changes
SCM muscle there is a swelling of a dense consistence), not soldered to subject soft fabrics. At the same time with the advent of dense there is a ducking towards the changed muscle, but the head to the opposite side is turned. It the same position of the head at such child — turn aside speaks. Treatment of a muscular wryneck should be begun at once as soon as the diagnosis is established. It consists in the basic in the gymnastic exercises which are carried out 3 — 4 times a day for 5 — 10 minutes.
Thus the head of the child lying on a back, clasp both hands and give it whenever possible the correct situation, i.e. incline aside, opposite to the struck muscle, and turn in the healthy. At the same time carry out massage healthy SCM muscle and also a course of physiotherapeutic procedures. It is necessary to put a bed of the newborn so that the child, watching the events in a room, could turn a head towards the changed muscle, involuntarily giving it the correct situation. At unsharply expressed form of a muscular wryneck timely and systematic conservative treatment leads to complete treatment on the first year of life. At heavier extent of deformation treatment proceeds till 3 years. In case of unsuccessful conservative treatment operative intervention is shown to children after 3 years. Carrying out this occupation gives the chance to the being trained the X-ray of pictures, local anesthesia a place of a change, preparation of plaster bandages, imposings of splint and circular plaster bandages, delivery of the preliminary diagnosis and definition of further tactics of maintaining the patient will familiarize with the basic principles of rendering of the first medical care, to inspection methods, types of anesthesia, principles of an immobilization, interpretation.
Training of students, on this this subject, is based on knowledge of human anatomy, topographical anatomy and operative surgery, radiology, anesthesiology resuscitation and sheathe surgeries. To congenital defects of development of the musculoskeletal device, meeting at children of early and preschool age, the congenital clubfoot, congenital dislocation of a hip and a congenital muscular wryneck belong. The
congenital clubfoot — is a contracture of joints of foot. The disease meets at boys more often, the clubfoot happens one - and bilateral. The main clinical signs of a congenital internal clubfoot are: plantar bending of foot in an ankle joint, turn of a plantar surface inwards with lowering of external edge of foot, mainly tarsi and metatarsuses, foot reduction in forward department at simultaneous increase in the arch of foot — hollow foot. Congenital clubfoot treatment consists in special correlation gymnastics, bandaging which needs to be begun on the first month of life of the kid and at an easy form of deformation leads to an absolute recovery.
Certainly, massage – very effective means is necessary. At averages and heavy forms of an illness plaster bandages are applied. If treatment begins after 2х years, it demands operation before which to the child carry out treatment in the form of stage plaster bandages.
Congenital dislocation of a hip - most frequent of congenital deformations of the musculoskeletal device. When speak about frequency of this pathology, mean not only the created dislocation of a femur which is seldom observed in the first days of life, and a so-called displasy (the wrong arrangement of a head of a femur) against which dislocation subsequently can be formed. At children of early age meets twoand unilateral dislocation, and at girls more often than at boys. The outcome depends on timely diagnosing of an illness and an initiation of treatment. The diagnosis of a displasy of hip joints put in maternity hospital, with the same purpose in children's policlinic of all babies (till 3 months) the surgeon-orthopedist examines. The most frequent symptoms of a congenital displasy of a hip joint is the following: assignment restriction in hip joints; click; asymmetry of folds on a hip and buttock folds behind; shortening of the bottom extremity measured by eye. The listed symptoms can be observed either at the same time everything, or only a part, in the latter case it is necessary to suspect a congenital displasy of a hip joint and to make a X-ray. If at the baby the diagnosis of a displasy isn't established, when it starts to stand and go, diagnostics of congenital dislocation of a hip comes easy. At children after a year one of characteristic symptoms is the late beginning of walking: the first steps in 14 — 15 months, and also typical gait — is noted instability, lameness — at unilateral dislocation, duck, rolling-over gait at bilateral dislocation. Treatment of a displasy of hip joints is necessary for beginning at once after diagnosis establishment on which term the way of treatment depends also. Treatment can be conservative and operative and if the diagnosis is established on the first year of life, conservative treatment is always applied.
Congenital muscular wryneck: A wryneck — the neck deformation, being characterized the wrong position of the head (an inclination sideways and its turn).
There is a wryneck owing to pathological changes in soft fabrics, mainly in SCM muscle. The specified deformation is more often happens right-hand and meets at
girls. There is also a bilateral wryneck. The congenital wryneck can be diagnosed on
2 — the 3rd week of life of the child. On the struck party as a result of changes SCM muscle there is a swelling of a dense consistence), not soldered to subject soft fabrics.
At the same time with the advent of dense there is a ducking towards the changed muscle, but the head to the opposite side is turned.
It the same position of the head at such child — turn aside speaks. Treatment of a muscular wryneck should be begun at once as soon as the diagnosis is established. It consists in the basic in the gymnastic exercises which are carried out 3 — 4 times a day for 5 — 10 minutes. Thus the head of the child lying on a back, clasp both hands and give it whenever possible the correct situation, i.e. incline aside, opposite to the struck muscle, and turn in the healthy. At the same time carry out massage healthy
SCM muscle and also a course of physiotherapeutic procedures. It is necessary to put a bed of the newborn so that the child, watching the events in a room, could turn a head towards the changed muscle, involuntarily giving it the correct situation. At unsharply expressed form of a muscular wryneck timely and systematic conservative treatment leads to complete treatment on the first year of life. At heavier extent of deformation treatment proceeds till 3 years. In case of unsuccessful conservative treatment operative intervention is shown to children after 3 years.
2.2. MODERN PEDAGOGIC TECHNOLOGY
Methodical recommendations game
" WEAK LINK "
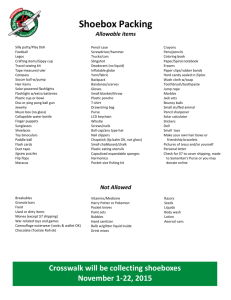
For work it is necessary:
1. A set of questions on «Treatment of injuries of a thorax and a humeral belt».
2. A sheet of paper and with the group list for maintaining the protocol of game.
Work course:
1. Game is carried out by the teacher and the assistant from among students –
"counter".
2. "Counter" on a leaf writes date, group number, faculty, the name of business game and the list of students of group.
3. The teacher asks questions to students consistently from a set of questions.
4. The student should for 5 seconds answer.
5. The teacher a word correctly" or "incorrectly" estimates the answer. At the
"incorrect" answer itself gives the right answer.
6. The counter puts opposite to a surname of the student «+» or "-", depending on correctness of the answer.
7. Students pass, thus, 2 rounds of questions.
8. After the 2nd rounds of questions game stops also students who received 2 minuses, leave game as «the WEAK LINK».
9. Game proceeds on a new circle with remained students. One new round of questions is again offered and again students who in the sum with the first round gathered 2 minuses are eliminated.
10. Round behind round is selected the strongest participant of game who correctly answered bigger number of questions.
11. On a leaf, against each surname, the teacher registers – who, in what round left and became «the WEAK LINK». Game is estimated as much as possible at 0,8 points. The students who have left after the first 2nd rounds of answers, receive for the game "0" of points,
- «0,2» points;
- «0,4» points;
after the 5th round of answers - «0,6» points;
12. The exposed points on a leaf of the protocol are considered at calculation
the current result of occupation as an assessment for a theoretical part.
13. In the lower free part of the magazine, the teacher makes entry about
to the carried-out business game, the head signs.
14. The protocol of game remains.
GAME «WEAK LINK»
1. In what intercostal and on what line the puncture of a pleural cavity is carried out at pheumothorax?
2. In what intercostal and on what line the puncture of a pleural cavity is carried out at hemothorax?
3. On what edge of an edge intercostal blockade is carried out?
4 whether it is possible to execute the 2nd foreign vagosympatic blockade?
5. What diagnostic method has advantage at diagnosis statement to the patient with a fracture of edges?
6. What shouldn't the bandage fix at a fracture of a clavicle?
7. List 3 rules shown to bandages at a fracture of a clavicle?
8. Call a pathognomonic symptom at dislocation of the acromion end of a clavicle?
9. What situation is given to the patient at injury of a thorax?
10. List types of dislocations of the acromion end of a clavicle?
11. Fixing term at a fracture of a clavicle without shift?
12. List indications to operative treatment at a fracture of a clavicle?
13. Call a bandage imposed at open pneumothorax?
14. List the main groups of the medicines used at an injury of a thorax?
15. In what projection the X-ray is carried out at an injury of a breast?
16. What researches are necessary for carrying out at inspection of the patient with an injury of a breast?
17. How types hemothorax by amount of the streamed blood are classified?
18. Value of intra pleural pressure?
19. List types of fractures of a shovel?
20. What method of research is shown at a change of an articulate surface of a shovel?
Case studies:
1 case studies
Patient A. 27l, complained of chest pains, shortness of breath and inability to fully cough. From the words beaten by unknown persons last night. On examination, frequent and shallow breathing in induced torso forward and to the left, the left half of the chest behind the act of breathing. On palpation - a sharp pain in the seventh intercostal space at the mid-axillary line, where there is a small swelling of the soft tissues. Tightness in the chest in the frontal and sagittal planes also cause a sharp local pain at the specified location.
1.Vash preliminary diagnosis
2.Osnovnye methods
3.With what damage must make a differential diagnosis
4.Taktika GPs
3.2. Analytical part.
Control test.
1. The indications for surgical treatment of clavicle fractures are
A. open fractures with damage or compression of the neurovascular bundle
B. comminuted fracture of the clavicle with the danger of injury to the skin
V. closed comminuted fracture
D. all of the above
D. Only B. and B.
2. Rehabilitation with a positive outcome after breaking his collarbone is through
A. 2-4 weeks
B. 1.5-2 months
B. 2-3 months
G. 3-4 months
D. 4-6 months
3. Clinically, there are the following fractures of the scapula
A body
B. angles
B. sprouts
G. neck and acetabulum
D. all of the above
4. Peripheral otlomok fracture neck blade moves
A. upward and inside
B. downward and medially
B. outward and upward
G. outwards and downwards
D. rotationally
5. Damage to the axillary nerve in shoulder fracture results
A loss of sensitivity
B. loss of movement in fingers
B. to the deltoid muscle paresis
G. to circulatory
6. Of these fractures is an intra-articular fracture of the scapula
A body
B. angles
B. sprouts
Mr. Awn
D. acetabulum neck
7. Characteristic symptom is the scapula fracture
A sign of Marx
B. symptom Chaklin
B. symptom Comolli
D. all of the above
8. When fractures of the shoulder blade is used to immobilize
A plaster cast by Turner
B. triangular bandage
B. compress desault
G. cast desault
D. Abductor bus
9 Viewing tapping away on the bus fracture of the neck of the glenoid cavity or blades shall be
A 30 °
B. 60 °
90 ° W.
G. 110 °
D. 160 °
10. immobilization time for fractures of the scapula is
A. 2 weeks
B. 4-5 weeks
B. 6-8 weeks
G. 10-12 weeks
D. 3 months
11. Pain associated with the position of the head, hands, cough, pain in the shoulder girdle and the interscapular region is characterized by
A. For cervical diskalgii
B. Syndrome anterior scalene muscle
B. Sudeck syndrome
G. vertebral artery syndrome
D. visceral syndrome case studies 1
Patient B. 34y, complained of severe pain in the chest, shortness of breath, wheezing, shortness of breath. Anamnesis was injured in a car accident an hour before the treatment. On examination, marked restlessness and fear of patients, frequent and shallow breathing with a whistling sound, swelling of the neck vessels. Palpation: sharp pain on the anterior axillary line at the right edge 5-6-7, subcutaneous emphysema of the right half of the chest above the 7 ribs with the transition to the neck.
1.Vash preliminary diagnosis
2.Osnovnye methods
3.With what damage must make a differential diagnosis
4.Taktika GPs case studies 2
Sick E. 25y, complained of pain in the left shoulder girdle, worse when trying to motion in the same shoulder. With the words fell while playing basketball for 3 hours prior to admission. On examination indicated moderate flattening of the supraclavicular fossa, the shortening of the left upper arm and a sharp local pain with pressure on the middle third of the left clavicle.
1.Vash preliminary diagnosis
2.Osnovnye methods
3.With what damage must make a differential diagnosis
4.Taktika GPs
4. Graphic Organizers: chest bruising T-circuit
Guidelines and new technology for the activity of T-scheme
- Universal graphic organizer to record binary (yes / no, for / against) or compare 2 aspects of one concept / information. This is a comparative table.
• Develop critical thinking skills.
• Used in the final lecture / completion thematic.
Acquainted with the rules for the T-schema. Individually issued T-circuit.
In the allotted time individually / in pairs fill pattern: the left side of her reasons for writing "for", and the right - causes / etc, the opposite ("against") the ideas set out in the left side.
Schemes can be compared / supplemented in pairs / groups.
The entire study group constituted a single T-circuit.
Rib fracture Clinic for thoracic injury
1. acute pain
2. difficult breathing
3. crepitus
4. forced attitude
5. Lag in breathing
1. acute pain
2.
difficult breathing
3. Weak vesicular breathing
Criterion of assessment:
Max point 20-17,2 17-14,2 ball 14-11 ball 10,8-7,4 ball 7,2 ball
Excellent Good Satisfactory Unsatisfactory
100%-86%
2.3. question for studying:
85%-71% 70-55% 54%-37%
1.
What situation is given to the patient at injury of a thorax?
Bad
36% and below
2.
List types of dislocations of the acromion end of a clavicle?
3.
Fixing term at a fracture of a clavicle without shift?
4.
List indications to operative treatment at a fracture of a clavicle?
5.
Call a bandage imposed at open pneumothorax?
6.
List the main groups of the medicines used at an injury of a thorax?
7.
In what projection the X-ray is carried out at an injury of a breast?
8.
What researches are necessary for carrying out at inspection of the patient with an injury of a breast?
9.
How types hemothorax by amount of the streamed blood are classified?
10.
Value of intra pleural pressure?
11.
List types of fractures of a shovel?
12.
What method of research is shown at a change of an articulate surface of a shovel?
Criterion of assessment:
100%-86% 85%-71% 70-55% 54%-37% 36% и ниже
3,6 and below
10-8,6
Excellent
8,5-7,1-
Good
7-5,5-
Satisfactory
5,4-3,7-
Unsatisfactory
3. Analytic part
3.1 graphic organizer: damage chest
Т-scheme
Clinic of rib’s fracture Clinics of bruise of chest
1. acute pain
2. severity breath
3. crepitation
4. forced condition
5. weakness act of breath
Max point 15-12,9
Excellent
100%-86%
1. acute pain
2. severity breath
3. weakness of vesicular breath
Criterion of assessment:
12,75 -
10,65 ball
10,5-8,25 ball
8,1-5,55 ball
Good Satisfactory Unsatisfactory
85%-71% 70-55% 54%-37%
5,4 ball
Bad
36% and below
4. Practical part
Practical skill - First-aid treatment at injury of a thorax and changes of a humeral belt.
Purpose: To master equipment of first-aid treatment at injury of a thorax and changes of a humeral belt.
Equipment: Volanter, couch, syringe, Novocain 0,5 %, Kramer's tire, bandage.
Carried-out stages (steps).
№ Actions
Stages
Incompletely It is completely correctly executed
1. Introduction analgesic
2. Novocaine blockade of the injury
3. Limb immobilization bus Cramer
4. Giving reclining
5. Transportation to a hospital.
6. only total
0
0
0
0
0
0
0
20
10
20
20
20
10
100
5. Forms of control of knowledge, skills and abilities.
- the oral;
- the written;
- situational tasks;
- to show abilities of performance of practical skill.
5.1. Criterion of assessment of knowledge and skills of students
№
Mark adopting %
Excellent Good
100%-
86%
85%-
71%
1
1.1
Theoretical part new pedagogic technology
1.2
Control question
2
2.1
Analytic part:
Case study
2.2
3
Tests
Practical part
20-17,2 ball
17-14,2 ball
10-8,6 ball
15-12,9 ball
15-12,9 ball
40-34,4- ball
8,5-7,1 ball
12,75-
10,65 ball
12,75-
10,65 ball
34-28,4 ball
Satisfactory
70-55%
14-11 ball
7-5,5 ball
10,5-8,25 ball
10,5-8,25 ball
28-22 ball
Unsatisfactory
54%-37%
10,8-7,4 ball
5,4-3,7 ball
8,1-5,55 ball
8,1-5,55 ball
21,6-14,8 ball
Criteria of an assessment of the current control on a subject
№
Progress in
%
Assessment Level of knowledge of the student
1 96-100% Excellent Depending on a situation can make the
Bad
36% and below
7,2 ball
3,6 ball
5,4 ball
5,4 ball
14,4 ball
2
3
4
5
6
7
91-95%
86- 90%
76-80%
71-75%
66-70%
61-65%
“5” correct decision and sums up.
By preparation for a practical training uses additional literature (as on native, and in
English) Independently analyzes essence of a problem at inspection of patients with damages and diseases the ODE. Can independently examine the patient and correctly makes the diagnosis. Shows high activity, a creative approach at carrying out interactive games. Correctly solves situational problems with complete justification of the answer. During SRS discussion actively asks questions, does additions. Practical skill carries out surely, understands essence
Excellent By preparation for a practical training uses additional literature (as on native, and in
English)
“5” Shows high activity at carrying out interactive games. Correctly solves situational problems, but can't appoint concrete treatment, confuses dosages of preparations. Knows AFO of bone and muscular system, tells surely. Has exact representations on an etiology, патогенезу, to clinic, can carry out differential diagnostics, to appoint treatment, but can't carry out traumatism prevention.
Good Practical skill carries out on steps.
Satisfactory Correctly collects the anamnesis, examines the patient, makes the preliminary diagnosis.
Can interpret these laboratory researches.
Actively participates in SRS discussion.
Satisfactory Commits mistakes at the solution of situational tasks (can't expose the diagnosis on classification). Knows clinic at inspection of patients with damages and diseases the
ODE, tells not surely. The ODE and a traumatism has exact representations on an
8 etiology damage and a disease, but can't connect clinic with the patogenezy.
Collecting the anamnesis not purposeful, survey not according to the scheme. Can't interpret data of laboratory researches. It is passive at SRS discussion.
55-60% Satisfactory Has the general representations about treatment methods in traumatology and orthopedics, tells not surely. Confuses AFO of bone and muscular system. Can't independently interrogate and examine the patient. Can't interpret data of laboratory researches. Doesn't participate in SRS discussion
9 30-54% Unsatisfactory The ODE has no exact representation of the basic principles inspection of patients with damages and diseases.
10 20-30% Unsatisfactory Doesn't know AFO of bone and muscular system.
SRS - damaging of vertebra.
Control questions.
1. Classification damaging of vertebra.
2. Etiology, pathogenesis damaging of vertebra.
3. Diagnostics methods damaging of vertebra.
4. Classification of injuries of sinews of extremities.
5. First aid at injuries of sinews of extremities?
6. Complications in a consequence of injuries of sinews of extremities?
6. Recommended literature
1. Yumashev G. S. «Traumatology and orthopedics of» M «, Medicine» 1990. - 575с.
2. Musalatov H.A. «Traumatology and orthopedics of» M «, Medicine» 1995. - page.
4. Sport medicine: book for students– М.: Gumanit. press. centre. Vlados, 1998. – 480 p.
Internet resourse; WWW.minzdrav.uz WWW.tma.uz. htt://web.tma TMA Wi-Fi zone ZiyONet : travmo_tma@mail.ru
.