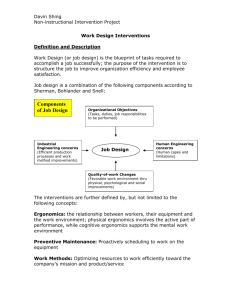
Design Guidelines Paper - Ergonomic Society of Australia
advertisement

37th Annual Conference Ergonomics Society of Australia Inc. Injuries Attributed to “Human Error”, Contributory Negligence or Reasonable Responses to Demand Characteristics of the Task or Workplace. Neil L Adams Dr Neil Adams & Associates, Sydney Keywords: Occupational Injuries; proximal and distal causes. ABSTRACT Having prepared “expert witness” reports on some 6,000 injury occurrences, the majority being occupational injuries, the author is becoming more and more aware of the relationships between distal causes (what James Reason referred to as “hidden pathogens”) in the work system or macroergonomics and the behavior which results in an accident and injury. Too often, the behavior that is seen as the immediate or proximal cause of the accident/injury is a response to the demand characteristics of the situation. Those demand characteristics, which almost unavoidably evoke the high-injury-potential behavior, are a direct function of and reflection of the distal causes that could be regarded as setting both the scene and the tone that then encourage, or at least permit, unsafe acts to be performed. Rather then blaming the injured person for contributory negligence (unless it really is blatant and directly contrary to adequate training and/or direct instruction) we should be working on identifying and counteracting the distal causes. Pure macroergonomics! 1. INTRODUCTION This is not an academic paper quoting or citing numerous previous authors although undoubtedly the conceptualisation in this presentation is not entirely original and can probably be traced back and attributed to relevant published papers or conference presentations by learned academics or researchers. It does to a certain extent develop the theme that was the basis of my presentation at the ICOSHE Conference in China a couple of years ago. The paper is based not on formal academic research but on the many reports that I have prepared over the last 15 years dealing with injuries that were, in the main, occupationally engendered. I have to confess that, sadly, I have not kept up with the research literature. The ideas generated by my involvement with persons who suffered occupational injuries reflect an increasing concern and even anger that despite the efforts of legislators and bodies such as WorkSafe, and in NSW, WorkCover, employers continue to inflict on employees systems of work and/or equipment which result in the employees suffering injury. As a precursor to the thoughts and observations offered in this paper, I specify some basic assumptions that, it seems to me, should be self-evident. 33 Better Integration 27-30 November 2001 2. BASIC ASSUMPTIONS. 2.1 Very few employees who suffer incapacitating injuries either want or intend to hurt themselves. 2.2 Generally, employers have better access to information about injury causation and preventative strategies than do their employees. This assumption, I suspect, applies more validly to larger employers and may not be so true of smaller employers, although the responsibilities of both, with respect to the needs to provide safe places of work and safe systems of work are, quite legitimately, identical. 2.3 An action which results in a worker suffering injury may reasonably be attributed to human error. That error may have been made by the person who suffers injury. It may have been made by some other member(s) of the system at some time antecedent to the injury occurrence. It may also have been made by a fellow worker contemporaneous with the injury occurrence. There is rarely a single error to which an injury occurrence can be strictly attributed. 2.4 Human error, at whatever level or remove in time it may be involved, is a simplistic and insufficient explanation. Even if the reliance on human error incorporates series or strings of consecutively dependent errors culminating in an accident or injury it is insufficient to rely on the human error explanation. 2.5 Unfortunately, legitimate application of the principles of risk management contributes significantly to the occurrence of occupational injuries. Employers transfer the risk associated with occupational injuries to the workers’ compensation insurer. Sadly, this action simultaneously transfers the risk to the workers, who individually bear the cost of injuries they may suffer. In consequence of the legislation that is currently passing through NSW Parliament, the cost to be borne by a worker who is injured will substantially increase, transferring even more of the cost of the risk to the employee him/herself. 2.6 Every accident or injury is a function of, and a clear symptom of some system failure. Even with regard to such apparently “simple” injury occurrences such as a worker falling from a ladder known to be unstably erected; or slipping while carrying a tub across a wet smooth concrete floor known to be slippery, one should seek answers not to the question “why did he attempt that task in those hazardous circumstances?”, but “why was he required, obliged or permitted to perform that task in those conditions?” 3. BASIC MODEL I want now to elaborate upon and define more clearly the basic model which I have applied to my analyses of injury occurrences over most of the 6,000 or so injuries which I have analysed over the last decade and a half. I must acknowledge at the outset that most of these analyses are based on information that is, to a certain extent, one-sided. Probably more than 80% of the reports would be based on information obtained primarily from the person who suffered injury although a substantial proportion of that 80% would have been aided by direct inspections of the workplace and, where relevant the equipment involved. Similarly, in those cases in which the report was prepared for a defendant’s solicitors there would have been no 34 37th Annual Conference Ergonomics Society of Australia Inc. contact with the injured person and all of the information about the system of work and the injury occurrence would have come from the defendant, again, most frequently, with an inspection of the workplace being included. Nevertheless, every analysis has been undertaken with as much dispassionate scientific objectivity as could be brought to bear, since every report is prepared with the full awareness that it may be attacked in court and I may be obliged, in the witness box, to defend the opinions I have expressed about such important matters as causation. That having been said, I offer these thoughts about the basic model of the injury occurrence or accident which results in a worker suffering injury. Such unwant6ed occurrences can almost always be described in terms of the immediate or proximal cause(s) and the more fundamental, antecedent or distal cause(s). The proximal causes include: The immediate task demands. The present conditions or characteristics of the materials and equipment involved, with emphasis on defects and faulty operation. The immediate task objective and overriding goals or targets (including quotas, which may be determinants of the speed with which the action is attempted). Importantly, the workers’ perceptions in the task situation – what is perceived by the worker as relevant and/or available and what is not so perceived. More colloquially, we would be concerned with what the worker has noticed as well as what he has failed to notice. The distal causes include: The training (or absence of training) and the relevance and thoroughness of that training. (For example, too often training in safe manual handling consists of workers attending a training session during which they may watch a video or have some demonstrations of lifting by a qualified trainer but absolutely no follow-up in terms of supervised on-the-job practice for some days afterwards with the supervision being given by the same qualified trainer). The job design and system of work. The original selection and choice of equipment and its appropriateness for the tasks for which it will be used. The quality of maintenance of the equipment and machinery. Specific instructions or directions given to (or not given to) the worker in relation to the task in question. “Ho hum,” I hear you say. “So what’s new about any of the above.” These are all obvious potential causal factors or contributory to an injury occurrence. What ties the distal and proximal causes together is what is so often overlooked in attempts to explain or understand 35 Better Integration 27-30 November 2001 the actions that result in a worker suffering injury. Having had a background (many years ago) in social psychology I believe that the integration of distal and proximal causes – an integration that gives rise to the demand characteristics to which a worker is responding when he produces the behavior that results in an accident or injury – may be found in the term attitudes. (Not having kept up with the scientific literature, I do not know whether the term “attitudes” is still acceptable in social psychology. However, I believe it to be directly relevant and applicable). And this is also where macroergonomics comes in. There are two sets of interacting/interdependent attitudes that it is important to understand. From the individual worker’s side there are the attitudes he has to the task and to the job; his attitudes towards himself and his competencies as a worker and his attitudes to the employer. His attitudes will, unavoidably, influence what he perceives in any particular task situation as being relevant to his performance and to the way in which he should be performing a task. On the organisational side there are the attitudes which derive from and simultaneously contribute to the organisational culture or climate as it relates to safety. There are also the more specific management attitudes to safety including investment in safety and responsibility for safety. (And by “management” I mean every level of manager from C.E.O. to ganger or leading hand, even though the latter may be little better trained or intellectually equipped to conceptualise about safety than those he supervises.) It is this meld of attitudes, distal causes and proximal causes that, in every individual work situation, determines the demand characteristics of that situation as experienced by the worker while performing his work in that situation, and may stimulate the producing of behavior which enables an accident or injury to occur. In the time that remains let me illustrate this concept and its pervasive influence on safe or unsafe behavior with several relatively common examples. 4. EXAMPLES OF INJURY OCCURRENCES IN WHICH THE PROXIMAL CAUSES OF THE INJURY CAN BE CLEARLY RELATED TO THE DEMAND CHARACTERICS OF THE SITUATION. 4.1 The nurse/carer engaged in “specialling” an adult with schizophrenic symptoms living in a residential care situation. 4.2 Tipping gravel (and self) into a truck from a 240 litre wheelie bin. 4.3 Playing “skip into the lift” with a fully laden hospital trolley. 4.4 What better than a large “Stilson” wrench for wrenching a man’s back? In hindsight, all four of the examples described above and illustrated with photographs in the verbal presentation reflect both the sets of organisational attitudes and individual attitudes that 36 37th Annual Conference Ergonomics Society of Australia Inc. have combined (conspired) to produce a set of demands in the immediate work situation which evoke totally injurious behavior. I firmly believe that, that as ergonomists and interventionists, we need to appreciate the possible demand characteristics at, in any job situation or job performance could be conducive to unsafe behaviour. Based on that appreciation, we should encourage employers to make whatever modifications are necessary to the system so that it will be safe rather than unsafe behavior or movements that are most likely to be evoked. In short, we must anticipate and deliberately design the demand characteristics in every work situation in such a way that the worker will almost automatically (quite possibly – let’s be honest – unthinkingly) – produce a safe act or behaviour, rather than an unsafe one. To paraphrase the old Julius Sumner Miller’s favorite question: “Why is it [not already] so?” 37 Better Integration 27-30 November 2001 38 37th Annual Conference Ergonomics Society of Australia Inc. Conquering the Coat Hanger OHS Issues for Toll Collectors on the Sydney Harbour Bridge Christine Aickin Workability Pty Ltd, Sydney, NSW, Australia Keywords: hazards, musculoskeletal, toll collection, aggression. ABSTRACT Toll plaza officers on the Sydney Harbour Bridge sustain sprains and strains, slips and falls, contusions and illness resulting from dealing with aggressive motorists at work. Demographic data shows that toll plaza officers represent over 90% of the population in terms of height are both male and female and can be either left or right handed. General hazards observed or reported in toll plaza work include: Working near traffic; Manual handling containers; Repetitive and sustained postures during toll collection; Physical and verbal abuse from motorists; Traffic noise; Vehicle emissions; Weather including heat, cold, sun, wind, rain and Security issues. A number of identification and assessment tools were used in this case study. These included consultation with staff; review of injury statistics; questionnaire; review of shift rosters; observation of work; task and posture analysis; productivity measures and toll plaza booth assessment. The results of the risk identification and assessment indicate that job design, booth design, vault and metal tin design, as well as maintenance of booths, vaults and metal tins require attention. Poor motorist behaviour and traffic are also involved. 1. INTRODUCTION In November 2000 the RTA sought assistance in conducting an assessment of OHS issues affecting toll plaza officers. While issues of exposures to noise and vehicle emissions had been assessed in the past and measures taken to address air quality issues, other issues relating to the design of workstations and work design including increasing aggression and violence from motorists had been identified by the Toll Plaza OHS Committee for attention. The work reported here was undertaken over the period from early December 2000 to February 2001 and involved close cooperation with all toll plaza officers, the toll plaza OHS Committee, toll plaza management and specialist RTA staff. 39 Better Integration 27-30 November 2001 Around 125,000 vehicles pass through 24 toll cabins per day on the Sydney Harbour Bridge. The cabins are situated at the northern and southern end of the Sydney Harbour Bridge. Eighteen of the cabins are permanent and 6 cabins, at the southern end, are mobile and are used in the mornings between 6:00-10:00 am. There are automatic collection cabins and manual collection cabins. It is possible to process around 200 vehicles every fifteen minutes manually and 140 every fifteen minutes through the automatic booths. At present the automatic booths are being used for hand collection of exact change during peak times. During this project E-Tag was being trialled. This is new technology, which allows vehicles equipped with an E-Tag to travel across the bridge while an automatic toll reader in the roadway registers and charges for each crossing. Full implementation of the E-Tag system is expected to take some years. 2. METHODS The project addressed OHS hazards on the north and south Toll Plaza. Particular attention was given to working near traffic, manual handling, repetitive tasks and motorist aggression. A variety of methods were used. 2.1 Consultation Staff were consulted to gain information on the way work was organised, tasks were performed and to identify hazards associated with the work and possible solutions. A questionnaire was distributed requesting input to the hazard management process. 2.2 Review of Injury Statistics Workers Compensation records were reviewed. 2.3 Review of Shift Rosters Shift rosters were reviewed. 2.4 Task Analysis Observation was made of the toll plaza officers to identify work organization and job design factors. Toll plaza officers were observed over periods of 20 - 120 minutes. Behaviours were noted and the jobs were broken into tasks, postures, frequencies of tasks and duration. An assessment of carrying tasks was also undertaken (Snook and Ciriello, 1991). Video recordings were made of toll plaza officer work for later analysis of postural load using Ovako Working Posture Analysis System (OWAS). The working postures adopted during the work were classified according to the basic OWAS method, which defines the positions of the back, neck, upper and lower limbs as well as force (Karhu et al, 1981). Rapid upper limb assessment (RULA) is a survey method used where work-related upper limb disorders are reported. This method assesses the postures of the neck, trunk and upper limb along with muscle function and the external loads experienced by the body (McAtamney 40 37th Annual Conference Ergonomics Society of Australia Inc. and Corlett, 1993). A number of postures were identified from the video recordings of toll plaza work and these were assessed using RULA. 2.5 Productivity Measures The productivity measurements were made from the videotape recordings of toll collection work to identify frequency of arm movement in hand collection in automatic booths, exact change collection and providing change, at different times of the day. 2.6 Toll Plaza Cabin Assessment The workstations ware evaluated using ergonomic principles relating to office workstation design found in AS /NZS 4443 - 1997. An evaluation was completed on the chairs using the Worksafe Australia Ergonomic Design of Adjustable Chairs Checklist, 1990 as a guide. An evaluation was completed on the footrest using the Worksafe Australia Ergonomic Design of Footrests Checklist, 1990. 3. RESULTS 3.1 Work Organisation Toll plaza officers work shift work, including morning, afternoon, evening and split shifts. A group leader supervises them. Toll plaza officers arrive on shift and collect their metal box from the locker. They proceed to the toll plaza via a passage and stairway. They cross the lanes of traffic to reach the cabin. They work in blocks of time ranging from 30 minutes to 105 minutes throughout their shift. They have crib breaks and meal breaks and work in a number of different cabins during this time. At the end of the shift they calculate their takings, transfer their takings to a coin bag or a note bag and weigh the coin. They then deposit the bags in the strong room. They carry a metal box, fitted with a removable lid and coin tray, to and from the toll plaza. It weighs 3.8 kg empty. Boxes were weighed at 13.4 kg – 14.2 kg following toll collection. The box is designed to be slipped into the metal runners below the desk in the booth and secured with a time delay mechanism. The toll plaza officer also handles vaults when operating the automatic booths manually. The vault weighs 4.8 kg empty. Vaults were weighed at 7kg – 22 kg following collection. The vault is designed to be slipped in and out of the base of the automatic mechanism. 3.2 Review of Injury Statistics The most frequent accidents were sprains and strains followed by slips and falls and mental strain. The mental strain is most often the result of aggressive driver behaviour. Driver aggression appears to be on the increase. 41 Better Integration 27-30 November 2001 3.3 Questionnaire The toll plaza officers indicated that job design, booth design, vault and box design, as well as maintenance of booths, vaults and boxes require attention. Poor motorist behaviour and traffic are also involved. 3.4 Review of Shift Rosters It was reported that full-time staff can work permanently on one shift or perform rotating shifts. Rotating shifts do not follow morning, afternoon, and night pattern. Casual staff can work split shifts. 3.5 Task Analysis The hazards observed for the toll plaza officer include traffic, manual handling of containers, repetitive and awkward postures during toll collection, physical and verbal abuse from motorists, traffic noise, vehicle emissions, hold up and weather conditions. It was also noted that the tasks which, cause delays to drivers are those which require forms to be filled out. The following forms are completed: Fare evasion form, Deferred fare form; Vault docket in an automatic booth used manually and Supervisor log. Other delays are caused by requests for directions, requests for change and receipts at an automatic booth used manually, follow-up on underpayment, interruption by drivers when a nearby automatic breaks down and requests for small change from other lanes. The tasks, which involved the repetitive movement and handling of weight were identified and analysed. They include: Carrying the metal box to and from the toll plaza and Collecting toll either in an automatic booth being used for hand collection, or a correct change collection booth or in a change given booth. A carrying analysis (Snook and Ciriello, 1991) was conducted on carrying the metal box (13.4-14.2 kg) to and from the toll plaza over 8.5 metres. The calculations indicate that a load of 15 kg exceeds the maximum recommended weight for 90% of the healthy adult population for females but not males. The acceptable weight is 14 kg where carrying occurs every 30 minutes. The most common posture noted was standing. Time spent with the back twisted during manual collecting and providing change (30%) and during hand collecting in an automatic cabin (40%) is considered stressful for the back. Reduction in this time is necessary in the near future. This twisting occurred because the officer had to reach (past the automatic chute) to the motorist and cross the midline when providing change. Evaluation of neck and upper limb postures using the RULA methodology reinforces this finding. It indicated that lifting the arm out to the side and forward to accept the toll and 42 37th Annual Conference Ergonomics Society of Australia Inc. crossing the midline to put the toll away and collect change causes the most strain on the shoulder. 3.6 Productivity Toll plaza officers process between 6.7-12.6 vehicles per minute. This frequency of movement is considered repetitive for the shoulder when it is performed for an hour or more (Kilbom, 1994). 3.7 Toll Plaza Cabin Assessment Observation and measurement of the toll booth indicated that in the manual booths the work surface is too low for the tall officers and too high for shorter officers in standing (900 mm) (Kroemer and Grandjean, 1997). There is a difference in height between the window (930 mm) and the top of the work surface and some officers have to raise the shoulder to clear the window ledge. The door handle obstructs the free movement of the arm in and out of the cabin when the door is shut. Reach to the vehicle could be reduced slightly if the door slides outside the cabin rather than inside it. There is a ridge on the floor for the sliding door. This is a trip hazard and throws the officers off balance when standing with the door open. The console is thick and the officer has to raise the arm and the wrist to use it. The leg space is obstructed by the drawer for the metal box and the reach distance to a clipboard for holding notes is too long for the average male to use frequently (700 mm) (Kroemer and Grandjean, 1997). There is no thermal or noise insulation. There are similar issues in the automatic cabin used manually. In addition, the leg space is obstructed by the automatic mechanism and there is no writing surface. Access to the intercom and the emergency button is at arms reach. The chair used in the cabin is a long stemmed ergonomic chair. It has Australian Furniture Research and Development Institute accreditation for ergonomic stability and strength and durability. If this chair is used correctly, it will adapt to the variety of seated postures required by the toll plaza officer. The footrest selected for use with the workstation is wooden. It is provided in addition to the ring on the chair. The footrest is suitable especially when teamed with the adjustable height ring on the chair. 4. DISCUSSION AND CONCLUSIONS The results of the assessment provided some insight into the causes of the identified hazards. 4.1 Traffic Safety Walkway surfaces were reported to be slippery and uneven in places. In some instances it is not clear where the walkway is. Compliance with procedures for working in traffic was also observed to be patchy. 43 Better Integration 27-30 November 2001 4.2 Manual Handling of Containers The hazards observed with carrying the metal tin to and from toll plaza include weight of the metal tin, need to climb or descend stairs, condition of walkways and stairs, walking through traffic lanes, design of pay-in room and security when walking. Analysis of carrying the tin from the toll plaza indicates that a weight of 14 kg is the maximum recommended weight for the healthy adult female population. Design and maintenance of the metal box and vaults require review. 4.3 Repetitive and Sustained Postures during Toll Collection Analysis of toll collection indicates that risk of injury to the back is associated with arms crossing the midline when providing change, twisting to reach around the automatic coin chute and prolonged standing. Lifting the arm out to the side as well as forward to accept the toll is associated with shoulder neck and arm strain. The frequency of movement is considered repetitive for the shoulder when it is performed for an hour or more. 4.4 Cabin Design Analysis of cabin design indicates that improvement is required. A number of design factors require attention including work surface height, window height, position of door handles, position and design of side door, console thickness and general design, leg space, storage of notes, insulation and illumination and light control. Automatic cabins also require refurbishment if they are to be used manually. In particular the provision of a work surface, removal of the automatic chute and the provision of shock absorbing matting require attention. If the chair and footrest provided is used correctly and well maintained it will adapt to the variety of seated postures required by the toll plaza officer. Chairs will not be used in automatic cabins operated manually because there is no leg well space. 4.5 Motorist Aggression Delays, which may cause aggressive behaviour in motorists, were observed. They relate to job design and equipment design including the requirement for paper work to be filled out, request for services not available at a particular cabin, requests for directions, follow up of motorists who underpay, malfunction of automatics and requests for change from one toll plaza officer to another. 5. CONCLUSION The issues identified by the study were fully reported with recommendations set out in terms of practical measures that could be implemented immediately, changes to be addressed in the medium term and those that need longer term planning to effectively address the problems. The report has been provided to the toll plaza management and OHS committee as the basis for an action plan. 44 37th Annual Conference Ergonomics Society of Australia Inc. The work undertaken provides a useful case study of the role professional ergonomists can play in empowering stakeholders in the workplace through the provision of technical data as a sound basis for developing practical approaches to solving workplace hazards. 6. ACKNOWLEDGMENTS I would like to thank the RTA and in particular Mr Mark Collins, Mr Tony Bird, Mr Adam Lea, Mr Dennis Murphy, Ms Marta Ayling, Mr Rudi Englert, Ms Milise Sotiriou, Ms Nazim Sintic, Mr Geoffery Sanford, Mr Julian Attard, Mr Tony Gigliotti, Ms Mary Wright, and Mr Jude Singarayar and the rest of the staff of the Sydney Harbour Bridge Toll Plaza for their input to this project and paper. 7. REFERENCES AS/NZS 4443 Office panel systems-Workstations 1997. Ergonomic Design of Adjustable Chairs, Worksafe Australia, 1990. Ergonomic Design of Footrests, Worksafe Australia, 1990. Kroemer, K. and Grandjean, L, 1997, Fitting the Task to the Human – A Textbook of Occupational Ergonomics, 5th Edition, (Taylor and Francis, London), 53-67. Karhu, O., et al, 1981, Observing working postures in industry. A practical method for analysis. Applied Ergonomics, 12, 13-17. McAtamney, and L., Corlett, N., 1993, RULA: A survey method for the investigation of work-related upper limb disorders. Applied Ergonomics, 24, 91-99. Snook, S. H., and Ciriello, V. M., 1991, The design of manual handling tasks: Revised tables of maximum acceptable weights and forces. Ergonomics, 34, 1197-1213. 45 Better Integration 27-30 November 2001 46 37th Annual Conference Ergonomics Society of Australia Inc. Designing Workplaces for the Safer Handling of Patients & Aged Care Residents Fiona Begg Melbourne Health (Royal Melbourne Hospital) Mark Hennessy Hennessy Services Pty Ltd Keywords: Health, workplace design, patient handling ABSTRACT There is a link between the layout and design of a workplace, and the risk of musculoskeletal disorders. The health sector has traditionally experienced high claims rates, particularly back related claims arising from patient handling tasks. In 1998, WorkSafe Victoria facilitated an industry Workplace Design Working Party to document best practice information and minimum standards in the building design & layout of the main areas where patient handling occurred. As an outcome, a publication titled “Designing workplaces for safer handling of patients/residents – Guidelines for the design of health & aged care facilities” was developed and released in December 1999. The guidelines provide information about how ergonomics and effective consultation can add value to the design phases of a health facility construction project. In the long term, good building design will lead to a reduction of injuries and workers compensation costs. This paper provides information about the contents of the publication, and outlines case studies and practical lessons learned when using the design guidelines in a health facility. Recommendations regarding the future use of the guidelines at workplace level, as well as industry level are made. This paper illustrates how research can integrate with practical workplace activity in a strategic sense. 1. INTRODUCTION Musculoskeletal disorders have been a priority occupational health and safety (OHS) issue in the health industry for many years. One study found that nurses had almost 30% more sick leave compared to other occupational groups (Pheasant and Stubbs, 1992). Many studies have identified the lifting and transferring of patients as the most frequent precipitating factor or cause of low back pain amongst health care workers (Garg, 1992; Engkvist, 1992; Engkvist et al, 2001). Given the huge cost in terms of workers compensation and quality of life for injured workers, the health industry (both employee and employer groups) and OHS regulators are keen to find sustainable preventative mechanisms to reduce the number and severity of claims. This paper provides information about an innovative strategic initiative of WorkSafe Victoria (WorkSafe), aimed at providing guidance on the design and layout of the main patient/resident handling areas within hospitals and aged care facilities. The key output of the initiative was the publication of an information booklet, “Designing Workplaces for Safer Handling of Patients/Residents” (the Design Guidelines). This paper complements a 47 Better Integration 27-30 November 2001 presentation to an Annual Conference of the Ergonomics Society of Australia by the same authors early on in the project, and prior to finalisation of the Design Guidelines (Begg, Kenningham and Hennessy, 1998). 2. BACKGROUND ISSUES In Victoria, the health industry has identified the “No Lifting” System (sometimes called “Minimal Manual Handling”) as a best practice approach to the prevention of patient handling related injuries. Some $6.2 million from the Victorian Department of Human Services (DHS) has been allocated to public hospitals and aged care facilities to assist in the implementation of No Lifting programs. A key component of a successful No Lifting program is the provision, maintenance and use of patient handling equipment. An evaluation of the No Lifting program at the Royal Melbourne Hospital one year after implementation, showed that the costs of manual handling related claims in No Lifting units reduced by an average of 80%. With such encouraging results, the number of facilities adopting No Lifting programs and in turn making more use of patient handling equipment, is growing. One limiting factor is that the physical design and layout of many health facilities does not accommodate some of the recommended No Lifting equipment or safe work practices, and will therefore impact on the potential results of such initiatives. The project team inspected 8 facilities newly constructed or refurbished in the previous two years - all conformed with building codes and standards, but most had ergonomic shortcomings in relation to working space and storage space for patient/resident handling equipment. 3. FACTORS INFLUENCING HEALTH FACILITY DESIGN Why does the design of our current health facilities not measure up when it comes to staff safety, and particularly, patient handling? 3.1 Focus on Patient Care The most important key performance indicator for health care workers and their managers alike, is the quality of patient care. With the focus being squarely on patients, building designers and health workers involved in the design of health facilities will strive to ensure the patient is comfortable and safe, sometimes at the expense of staff safety. For example, many new healthcare facilities are built with carpet throughout corridors and bedrooms. This is of course very homely and comfortable for the patient, and reduces noise in the facility. For staff, however, the carpet may be a problem in terms of cleanliness and infection control, and increases the forces required to manoeuvre wheeled equipment. 3.2 Expanding Range of Patient Handling Equipment The use of patient handling equipment is a key component of any No Lifting program. In recent years, suppliers have responded to users needs, in expanding the variety, useability and versatility of patient handling equipment. With the typical life of a health facility being some 30 years, many of today’s facilities were not designed to take into account the use of patient handling equipment. Some equipment, such as mobile hoists and shower trolleys, require 48 37th Annual Conference Ergonomics Society of Australia Inc. considerable space while being used and safely stored. Attachments for the equipment also require adjacent storage space. Other items, such as overhead tracking and drop down grab rails, require substantial structural support. 3.3 Changing Systems of Work The systems of work in health care are continually changing to match community demand. In the acute sector, there is a faster throughput of patients, and in the aged care sector, residents are only admitted when they can no longer be maintained at home with the assistance of community nursing. Inpatients are more dependent today than they were some years ago, and hence, more physically demanding for staff. Changing systems of work may also impact on the movement of equipment within the design of a health facility. For example, to reduce number of transfers, patients are often moved around the hospital on beds, rather than trolleys. Beds are considerably wider than trolleys, and sometimes the doorways and corridors in the existing facility may not be wide enough for easy mobility. 3.4 Need for Flexibility Hospitals and aged care facilities require maximum flexibility in using their workspace. In aged care, the Commonwealth Ageing in Place Policy means that on admittance to a nursing home, residents should remain in the one bedroom through the progressive stages of their illness, making it feel more like their home. Therefore, the design of the bedroom needs to be able to accommodate the progressive stages of dependency, from the point when the resident is admitted to the facility. In acute hospitals, depending on demand, wards may need to accommodate different patient needs, ranging from patients who are totally dependent to fully independent, from month to month, or indeed day to day. 3.5 Current Building Regulations Current building regulations and Australian Standards provide little guidance in relation to these specific issues. The Building Code of Australia (BCA) sets performance based standards for designers, in the context of structural and fire safety provisions. It refers to Australian Standard 1428.2 -1992 Design for Access and Mobility, to take account of the needs of disabled persons. AS1428 was written with the independent disabled person in mind, (ie. someone who can manage his/her own transfers from a wheelchair). It does not therefore cater adequately for dependant disabled persons, (ie. those requiring assistance from carers and patient handling equipment to undertake daily living tasks). 3.6 Ineffective Consultation and Post Occupancy Evaluation Most project managers and architects understand the importance of consultation with end users as an opportunity to add value to the design. Many designers build in a phase of consultation during the design process, but often this does not yield the desired result. Even in new facilities, design faults arise – for example, doors built too narrow to accommodate equipment and storage space which is too small for the equipment to be stored. And often, the user’s perception of what they thought would be built is vastly different to what they end up with. Such results are often due to shortcomings in the communication processes, and the level of understanding of the user in regard to technical jargon, technical drawings, meeting procedures, inadequate information or inadequate time to consider information. Post 49 Better Integration 27-30 November 2001 occupancy evaluation is often not carried out extensively after the users have had a chance to work in the new space. Hence, architects and project managers may miss the opportunity to learn from past successes and failures. 4. DEVELOPMENT OF THE DESIGN GUIDELINES 4.1 Key Stakeholders’ Input In March 1998, WorkSafe convened the Health and Aged Care Consultative Committee, with representation of all key stakeholders in the health sector. Reporting to this Consultative Committee, the Workplace Design Working Party (chaired by Fiona Begg, then a WorkSafe Ergonomist) was established in April 1998, with representatives from the health sector having experience and technical knowledge in health facility design. WorkSafe contracted an architect, Michael Harbour, and a Certified Professional Ergonomist, Mark Hennessy to provide technical support to the working party. The aim of the Workplace Design Working Party was “to document best practice information in the building design and layout of the main areas where patient handling occurs”. 4.2 Research and Industry Consultation The working party researched the problem and gained input from the health sector by: Reviewing literature, guidelines and standards relating to health facility design; Visiting eight new health facilities to gather information on patient handling and how this is impacted by the design of the facility; Holding a consultative health industry workshop to obtain input and guidance on industry needs from key stakeholders. 4.3 Drafting the Design Guidelines The Design Guidelines were drafted by the working party, using information gained during the research and consultation phase of the project. A key source of technical information was a report by the Swedish Institute for Hospital Planning and Rationalisation. 4.4 Industry Feedback on Draft Design Guidelines After distribution of the draft Design Guidelines, a second consultative health industry workshop was held to gain feedback on the document. 4.5 Testing the Design Guidelines Spatial recommendations in the guidelines were tested in a simulated trial. Patient handling equipment and techniques were used in a full scale mock up to test for practicability. 4.6 Finalisation and Launch of the Design Guidelines After incorporating industry feedback, the Design Guidelines were finalised and published. The document was formally launched by the Minister for WorkCover in December 1999 at the Royal Melbourne Hospital. It has since been available from WorkSafe in hard copy. 50 37th Annual Conference Ergonomics Society of Australia Inc. 5. OVERVIEW OF THE DESIGN GUIDELINES Information presented in the Guidelines includes: 5.1 Generic Functional Requirements & Operational Issues General influences on handling patients/residents (such as work practices, the type of facility, organisational culture and resources). Functional capacity of the patients/residents (minimal to full assistance) General design considerations (patient handling equipment, furniture & fittings, doors and door openings, floors and floor coverings, nurse call systems, electrical and mechanical fittings, lifts, grabrails and handrails). 5.2 Specific Spatial Requirements Information and architectural drawings relating to spatial requirements in bedrooms (single and multiple), ensuites and assisted toilets, assisted bathrooms, lounge/dining rooms, corridors and storage areas. 5.3 Effective Consultation with Direct Care Staff Information about why, when, how and who to consult during the design process. 5.4 Checklists A “Workplace Design Process Checklist”, and a “Safety Audit Checklist” are located in the Appendices. 6. PRACTICAL USE OF THE DESIGN GUIDELINES IN HEALTH SERVICE 6.1 Communication Strategy To introduce the Design Guidelines to a network of some 35 health facilities across Melbourne, Northern and Western Health Services, a communication strategy was implemented which included: Identification of key stakeholders influencing building design (Project Managers, Infrastructure Managers, Facilities Managers, Capital Works Managers, Architects), Distribution of the Design Guidelines, with an accompanying Memorandum to the identified key stakeholders, Follow up presentations to identified key stakeholders on the content of the Design Guidelines, and key recommendations, and Provision of ongoing advice and assistance as required. 6.2 Early outcomes Whilst it will take some time before recommendations from the Design Guidelines are adopted as a matter of course, early outcomes are encouraging: Feedback - the identified key stakeholders provided positive feedback about the new information gained from the Design Guidelines. They commented that the Guidelines raised 51 Better Integration 27-30 November 2001 awareness of the link between building design and health and safety, and gave detailed and specific information about how to manage design risks relating to patient handling, Consultation with direct care staff – project managers are endeavouring to consult with direct care staff during the design process. Working parties are set up to facilitate the consultative process. Anecdotal evidence suggests that this is sometimes difficult to achieve using the comprehensive model presented in the Guidelines, given the tight deadlines around building design, Consultation with Health and Safety Representatives – a procedure has been established where Health & Safety Representatives are consulted prior to any building works commencing, Overhead tracking – both acute and aged care facilities have embraced the best practice concept of overhead tracking, including it in the redesign of a number of areas, including Intensive Care, Radiology, Aged Care and Rehabilitation, Use of drop down grab rails and space either side of the toilet - has been employed in dependent aged care units, and Spatial requirements for the use of equipment – with the No Lifting program in place, staff are more aware of the need for space to manoeuvre equipment, and this is being raised during the consultative process. Requests for the document –WorkSafe reports a continuing stream of requests for the publication from Victorian and interstate parties to facility design, including architects, managers of facilities and large companies who commission and run facilities. Feedback on the publication is uniformly positive. 6.3 Challenges in Implementation As with most new initiatives, there remain some challenges for successful implementation: Effective consultation & post occupancy evaluation is difficult to achieve with the limited resources available, Even after consultation has occurred, users sometimes have a different understanding to designers of what was agreed during the design process, Storage space for equipment is still often underestimated, as space for activity around patient care is considered the highest priority with the funds available, and To ensure maximum flexibility of the workspace over the lifetime of the facility, designers should build to accommodate the worst case scenario, ie. dependent patients/residents. On observation, this is not being done, and designers are building to accommodate the functional needs of the current clients. 7. RECOMMENDATIONS 7.1 Industry Level Recommendations for maximising the impact of the initiative at industry level include: Influencing the Building Code of Australia to refer to information in the Design Guidelines, Influencing Standards Australia to compile new information to take into account the needs of dependant persons with disabilities, Influencing health facility accreditation processes to take account of building design, and end user consultative processes during design, 52 37th Annual Conference Ergonomics Society of Australia Inc. Influencing OHS Regulators to use the Design Guidelines during health facility inspections, and to refer to the Guidelines in health industry information relating to Manual Handling legislation, Information campaign to key stakeholders about the Design Guidelines (eg. health architects, health engineers, project managers, OHS managers, CEOs), and Health industry employee and employer groups used as a vehicle to deliver information to their members about the Design Guidelines. 7.2 Workplace Level The Checklists in the Appendices of the Design Guidelines provide practical tools for health facilities to evaluate and improve their design processes. Effective consultation with end users is crucial to ensuring manual handling risks are taken into account. Project Managers need to build in time for effective consultation at all stages of the design project. Workplaces should make more use of their trained Health and Safety Representatives as a mechanism for ensuring health and safety issues are resolved during the planning stage. The principles in the Guidelines can also be applied to the design of other areas in healthcare facilities, including treatment rooms, acute or sterile areas such as emergency, theatre, post operative rooms, so that use and storage of equipment can be optimised in areas where the condition of patients is generally not ambulatory or independent. 8. CONCLUSION The publication of the Design Guidelines is an excellent first step in influencing health facility design to take account of patient handling issues. However, more needs to be done if real results are to flow. State Regulatory bodies for OHS are in an ideal position to influence the various standard setting agencies for the health industry, as well as individual health facilities. An integrated approach is needed to fully capitalise on the good work done to date. 9. ACKNOWLEDGMENTS The authors would like to thank Claire Gabriel and David Scott (Melbourne Health Work Environment Unit), and Ros Kushinsky (WorkSafe Victoria Ergonomics Unit) for their input into this paper. 10. REFERENCES Australian Building Codes Board, 1996, Building Code of Australia, CCH Australia. Begg, F., Kenningham, L., and Hennessy, M., 1998, A Strategic approach to improve health facility design for safer handling of patients and aged care residents, Ergonomics Society of Australia Annual Conference Proceedings. Engkvist, I-E, Hagberg, M et al, 1992, Overexertion back accidents among nurses aides’ in Sweden, Safety Science, 15, 97-108. 53 Better Integration 27-30 November 2001 Engkvist, I-E, Kjellberg, A et al, 2001, Back injuries among nursing personnel – identification of work conditions with cluster analysis, Safety Science, 37, 1-18. Garg, A, Owen, B & Carlson, B., 1992, An ergonomic evaluation of a nursing assistant’s job in a nursing home. Ergonomics, 35, 979–995. Pheasant, S & Stubbs, D., 1992, Back pain in nurses: epidemiology and risk assessment, Applied Ergonomics, 23, 226–32. Standards Association of Australia, 1992, AS1428.2 – 1992, Design for Access and Mobility, Standards Australia. Swedish Institute for Hospital Planning and Rationalization, 1979, SPRI Report 21, Hygiene Rooms - functional space for personal hygiene in long term. 54 37th Annual Conference Ergonomics Society of Australia Inc. What Workers Did: Lost Leaders in Organisational Change Verna Blewett New Horizon Consulting Pty Ltd, Adelaide Keywords: Organisational change, workers of influence, occupational health and safety (OHS), autonomy and job control, power, collaborative management, worker involvement, worker participation. ABSTRACT Australian Robens-style OHS legislation requires that management assess the possible OHS consequences of organisational change and it encourages a collaborative approach to problem-solving between management, workers and their representatives to make the working environment healthy and safe. Ensuring that collaboration is effective and that workers and management are able to resolve workplace difficulties is therefore a focus of activity for many organisations. Organisational theory presents organisational change as being led by powerful, transformational leaders and change agents at senior management level. However, organisational change does not necessarily emanate from senior management, nor is it necessarily controlled or even guided by them. The role of shop-floor workers as change agents is critical in organisational change, but rarely recognised; they are the lost leaders of organisational change. Shop-floor workers are significant people in any organisation but they have little or no positional power, and they may have limited autonomy and job control. Nonetheless, in certain circumstances they can be a powerful influence for change towards improved working environments, this is particularly so when their boundaries of power and autonomy are allowed to increase. This paper reports on a three-year, longitudinal, processual action research study into the role of worker-level change agents in the generation and implementation of organisational change. Drawing on the literature, it concludes that healthier workplaces can be the outcome when management recognises the value of worker-level change agents and when workers and management collaboratively manage the internal political environment of organisations. 1. INTRODUCTION The literature on organisational change, change agency and leadership has long been weighted towards the role of powerful elites and the formation of dominant coalitions as a means of influencing management decision-making on organisational transition (Child 1972). Board members, people in senior management and even supervisors are well represented as significant players who can influence political process and shifts in the balance of power and interests within management (see for example Pettigrew 1973; Dunphy and Dick 1981; Kanter 1983; and Buchanan and Boddy 1992). By focussing on dominant coalitions within management, little attention has been given in the literature to the place of those less powerful members of the organisation, the workers, as shapers of change processes. The research described in this paper shifts the spotlight from those with legitimate or positional power in the organisation (French and Raven 1959) and places it on less powerful, but nonetheless 55 Better Integration 27-30 November 2001 influential players; worker-level leaders. It does this using data collected over a three-year period in an automotive components manufacturer that employed about 200 people. The company, called by the pseudonym MoCo in order to preserve confidentiality, was located in the suburbs of an Australian capital city and was a division of an Australian-owned company with an interstate head office. 1.1 Power and influence Two concepts are critical to this research: power and influence. As Child (1984: 136) suggests, the concepts of power, influence and control share the paradox that while they are terms in ‘common everyday use [they are] nevertheless surrounded by ambiguity’. They tend to be defined in terms of each other, with overlapping meaning, or as Dawson (1996) suggests, as antecedents for each other. In order to describe the nature of the relationships that were observed in the data, it is useful to distinguish between power and influence. Many authors have pondered over these concepts, from the classic work of French and Raven (1959) to more recent researchers such as Dawson (1996); Morgan (1997); and Willer Lovaglia, and Markovsky (1997). Buchanan and Badham’s (1999) definition of power as ‘the capacity of individuals to exert their will over others’; that is, power as a potential for action is the one that is used here. All managers and some workers at MoCo had power (as a noun) however, the mere possession of power does not necessarily equate to the exercise of power (as a verb). The exercise of power can be regarded as coercive in nature (although this is not necessarily negative). Power may be expressed in many different ways; managers at MoCo sometimes used power as authority and control, where as the power of workers tended to be expressed as influence. Influence, as defined by Willer et al 1997, is ‘the socially induced modification of a belief, attitude, or expectation effected without recourse to sanctions’. It is a much softer concept than power, but may be no less effective in attaining individual or group goals. The notion of the generation of influence from power and power from influence as Willer et al further describe, is also important to this research, as the possession of power enabled influence to be exercised by some workers. Despite the existence of a literature on worker participation in the management of organisations, relatively little has been written on the role of workers at the peer level within organisational change processes, although Dunphy and Dick identified such people as ‘organisational activists’ (Dunphy and Dick 1981: xiii). Within the literature, people at shopfloor level tend to be regarded as passive contributors, resistors or acceptors of change, rather than as active and influential participants in organisational change, or their place in organisational change is ignored altogether (Burns and Rus 1979; Wilson 1992). In an early study on management and organisations, Etzioni (1961: 90-91) pointed out that whether one holds a position of power and authority is not solely determined by the location of that person within a formalised organisational hierarchy. He identified informal leaders who, although they had no formal organisational power, were able to influence others through the consensus of their followers. His was almost a passing reference to such people; this research builds on this early work using the findings from the case study data to develop criteria for identifying who these leaders are in an organisation as well as what they do. This research identifies a group of workers who could be identified as leaders and change agents and who, by using various strategies, were able to influence management decision-making. These strategies are outlined later in this paper. 56 37th Annual Conference Ergonomics Society of Australia Inc. 2. RESEARCH METHOD 2.1 Data Collection The data for this research were collected over a three-year period in the case-study enterprise using a mix of semi-structured interviews, long-term participant observation, non-participant observation and document analysis. The method allowed the author to observe the company and its people as well as participate in and influence the changes in the organisation as it progressed through a period of planned change over the research period. The method adopted is called processual action research, being a combination of processual research and action research. Processual research considers the element of time in the examining the process of transition and regards change as non-linear and discontinuous, in contrast with other qualitative modalities in which change is considered to be sequential and linear (Pettigrew 1987: 332; Hinings 1997). Using this research method demands that change be regarded as a fluid process where different histories and competing events can overlap and be accommodated in the story of transition. That is, organisations are ‘studied “as-it-happens” so that processes ...[can be viewed]...over time and in context’ (Dawson 1994: 4). It is this concern with the context, substance and politics of change and their temporal framework, which comprises the processual approach to explaining organisational change (Dawson 1994: 41). Lewin (1946) originally coined the term ‘action research’ and his original description still underpins more recent descriptions of the method. Lewin defined it as a process of planning, taking action and then fact-finding about the results of that action in order to plan and take further action; an iterative pattern that can continue indefinitely (Lewin 1946). Action research is a modality in which the researcher and the researched actively participate and collaborate in the work; it is therefore concerned with intervention and implementation (Gummesson 1991:103). In this research, the iterative, consultative and participative techniques of action research were employed and serve to cast light on the development of process while at the same time steering process through active intervention and consultation. The research method crosses boundaries and because of this, the new term ‘processual action research’ best describes the research approach that was undertaken. Inherent in this term are the concepts that the processes of organisational change were the foci of the research and that there was emphasis on an iterative, but non-mechanistic, process of implementation. In this regard, ideas were drawn from the realm of action research, but not rigidly adhered to. That is, the iterative cycle of planning, action and evaluation in collaboration with the participants in the organisation occurred, but not always in that prescribed order because events sometimes took place that inevitably led to an abandonment or disruption of the cycle of action research activity. 2.2 Data Analysis All data sources were rigorously catalogued during the data collection process. Data were then coded as memos written on Post-It Notes® and referenced back to the data catalogue. Data analysis was conducted using a visual assembly of the coded memos, grouped according to themes that generated meaning from the data after the method described by Huberman and Miles (1994: 432). The visual assembly enabled the memos to be moved around during the analysis process as new themes arose within the ‘situational and structural contexts’ (Strauss 1987: 2) within and external to, the organisation. 57 Better Integration 27-30 November 2001 3. RESEARCH FINDINGS 3.1 Workers of influence The data from this case study draw attention to a distinct non-managerial group who, despite their lack of positional power, had influence over management decision-making and were thus able to influence the outcomes of change initiatives. These workers are called workers of influence. There are two dimensions used to identifying workers of influence: firstly, individuals have some power vested in them by their peers in the workforce and secondly, they have access to the processes of management decision-making within the organisation. To put it simply, workers of influence were individual shop-floor level workers who had influence over others at various levels in the organisation, including senior management. Workers of influence were found in a wide range of non-supervisory roles in the company and the data reveal that their role was an important influence on management decision-making. Different categories of workers of influence could be identified: representative, advocate and informal workers of influence. Their tenure varied temporally and three categories were identified: transient, short-term and long-term. Despite their identifiable and important role in organisational change in the company, the workers of influence did not recognise or organise themselves as a group, nor did the general body of workers or the management. Nonetheless they were leaders and change agents who were central to the process of change in the organisation. These people are the lost leaders of organisational change; lost in the literature and lost in practice, as their role is unrecognised. 3.2 What Workers Did How did workers of influence get things done? The following strategies used to shape change were identified in this research. Demonstrating trust in and respect for management that was in keeping with the culture of the organisation. They were able to be forgiving when management made errors; they were open with their criticism of management actions on the understanding that there was no threat to their security to do so. Accepting increased power. They were not “empowered” by management; their peers gave them power. They accepted this power, the responsibility and the accountability that accompanied it, with no financial incentive. Accepting power enabled workers of influence to be active participants in the change processes in the company and help shape the organisation through both formal consultative processes and production-process improvement. Using information wisely. Workers of influence who participated in consultative fora were given significant, confidential information about the profitability and markets of the company. They preserved this confidentiality rigorously. They advised management on how to prepare performance indicator data for dissemination to the shop floor. Introducing new policy ideas. Workers of influence introduced new policies to the company and shaped their content in areas such as overtime, accredited training policy and literacy training. Maintaining solidarity amongst workers. There was a cohesive relationship between workers in the company, although this was not without conflict. Generally, workers were after the same objectives: a healthy and safe working environment, fair wages and a positive social environment in which workers had a legitimate say in the operation of the business. They stifled potential conflict by ensuring that the role of the union was kept separate from the role 58 37th Annual Conference Ergonomics Society of Australia Inc. of consultative fora. Administration people were largely non-unionised; despite this, they were included in enterprise bargaining helping to keep factory and office workers united. Being persistent. They kept on keeping on. If workers of influence thought that an issue needed dealing with, but management failed to take action, they did not let it drop. There were times when management behaved as though inaction might mean that the problem would just go away. This was no barrier to the workers of influence. For example, over a period of 8 months they dealt with the issue of casual labour, winning agreement to short casual timeframes that were described in the enterprise agreement. Being ambassadors for the company. Workers of influence ‘talked up the company’ and acted as ambassadors for the company in front of people from other enterprises. The line generally taken was to admit that things were not perfect, but that they were pleased with some of the things that had happened and were confident that the company would continue to improve with its collaborative approach to management. Acting ‘backstage’. The workers of influence in the company were politically astute. They knew how to perform to achieve change in the open, formal settings of committees, but they also demonstrated canny political ways behind the scenes. The processes they used were the daily informal conversations between workers of influence and others (workers and managers) on the factory floor during work time and the informal discussions that were held during work breaks. These presented opportunities for workers of influence to sow seeds of change (and sometimes discontent) amongst fellow workers. Through such interactions they were able to hear opinions and ideas from fellow workers and either counteract them or modify their own approach. They were able to make links (of the type: ‘you should talk to … about this, she’s keen to know more’). The information flow around the factory floor was a constant, general murmuring that was barely evident, but very real. These methods were essentially covert, not unscrupulous because they were subject to the quiet mass scrutiny of the body of workers; but they could be artful and shrewd. Acting as the corporate conscience. The workers of influence, as change agents, had an important role as the corporate conscience when management did not do what they said they would do. An important tool for achieving this was through the development of policy, as already discussed. Policies were binding on both workers and management; they were written agreements about approaches to particular situations giving agreed and specific courses of action. They effectively set the fence posts of the boundary of control into concrete. The treatment of casual labour, discussed above, is a good example of the workers of influence using policy to behave as the corporate conscience. This research introduces workers of influence and is a definitive piece of work in that it establishes a beginning, not an end. This work was conducted in one organisation, albeit in great depth and over a long period of time, however, the experience of one is not necessarily the experience of all. There is still much to research and understand about workers of influence and their activities, although experience in many other organisations suggests that this information can be generalised. However, there are likely to be other strategies used by other workers of influence in different organisations. 4. RELEVANCE OF RESEAR CH TO HEALTH AND SAFETY Robens-style legislation is used throughout Australia and in many other countries. South Australia has arguably the strongest legal provisions relating to consultation and participation in OHS in Australia. Participation and consultation are stated as two of five chief objects of the Occupational Health, Safety and Welfare Act, 1986. The first three being about securing 59 Better Integration 27-30 November 2001 the health and safety of people at work, protecting the public and eliminating at their source, risks to health and safety. The Act and Regulations detail the mechanics of consultation and participation; that is, how workers and management can work collaboratively to solve workplace problems. In this context, health and safety representatives are representative workers of influence who have power vested in them, not only by their peers, but also through legislation. Many factors impede effective consultation and participation by workers; for example, production pressures, lack of funds, lack of commitment and antagonistic industrial relations. But it is power and influence that are fundamental to effective consultation and participation. For there to be collaborative problem-solving there must be a sharing of power so that the party’s working together can do so from equal positions. 5. CONCLUSION – WHAT WE KNOW AND WHAT WE CAN DO Power and influence are importantly linked to autonomy and control in the workplace. Autonomy tends to be described in terms of the capacity for independent action (Borum 1995: 156), while control has connotations of directing, dominating and commanding. Both autonomy and control are associated with power. In the organisational setting, autonomy is exercised as job control at both management and worker level. That is, autonomy occurs when individuals have the power to control aspects of their job. We know that increasing autonomy and control makes workplaces healthier places (Marmot 1998). We know that increasing autonomy and control can reduce the health impact of organisational change (Karasek 1990). We understand that organisational change is a constant in our society. We know that participative organisations are healthier and we know there are links between participation and productivity (Shannon 1998; Hale and Hovden 1998). So what action is needed to see an improvement in OHS in this country? Workers of influence (and thus health and safety representatives) need to recognise themselves as potentially central to change processes and value the contribution that they can make. Managers need to understand and appreciate the value of workers of influence and work with them. However, none of this is necessarily easy for players on either side of the industrial fence. This is particularly so in organisations where deliberate steps have been taken to demoralise and disunite the workforce, where unions have been discouraged and where collective action by workers is effectively prevented. The challenge is to establish effective collaborative relationships build on power-sharing, trust and mutual respect. 6. REFERENCES Borum, F. 1995, Handelshøjskolens). Organization, Power and Change, Vol. 5, (Copenhagen: Buchanan, D. and Badham, R., 1999, Power, politics, and organizational change: winning the turf game, (London: Sage),. Buchanan, D. and Boddy, D, 1992, The expertise of the change agent: public performance and backstage activity, (Hemel Hempstead: Prentice Hall International). 60 37th Annual Conference Ergonomics Society of Australia Inc. Burns, T. R. and Rus, V, 1979, Introduction and overview, in T. R. Burns, L. E. Karlsson and V. Rus (eds) Work and power: the liberation of work and the control of power, (London: Sage). Child, J, 1972, Organizational structure, environment and performance: the role of strategic choice, Sociology 6(1): 1-22. Child, J, 1984, Organization: a guide to problems and practice, (London: Paul Chapman Publishing). Dawson, P, 1994, Organizational change: a processual approach, (London: Paul Chapman). Dawson, S, 1996, Analysing organisations, 3rd Edition, (London: Macmillan Press). Dunphy, D. and Dick, R, 1981, Organizational change by choice, (Sydney: McGraw-Hill). Etzioni, A, 1961, A comparative analysis of complex organizations: on power, involvement and their correlates, 1st Edition, (New York: The Free Press). French Jr, J. R. P. and Raven, B, 1959, The bases of social power, in D. Cartwright (ed) Studies in social power, (Ann Arbor: University of Michigan). Gummesson, E, 1991, Qualitative methods in management research, (Newbury Park, CA: Sage). Hale, A. R. and J. Hovden, 1998, Management and culture: the third age of safety. A review of approaches to organizational aspects of safety, health and environment. In Occupational Injury: Risk, Prevention and Intervention. A.-M. Feyer and A. Williamson. (Eds) (London, Taylor & Francis), 129-165. Hinings, C. R, 1997, Reflections on processual research, Scandinavian Journal of Management, 13(4): 493-503. Huberman, M. A. and M. B. Miles, 1994, Data management and analysis methods, in Handbook of qualitative research. N. K. Denzin and Y. S. Lincoln (Eds) (Thousand Oaks, Sage) 209-19. Lewin, K, 1946, Action research and minority problems, The Journal of Social Issues 2(4): 34-46. Kanter, R. M, 1983, The change masters: corporate entrepreneurs at work, (Boston: Unwin Paperbacks). Karasek, R, 1990, Lower health risk with increased job control among white collar workers. Journal of Organizational Behaviour 11 171-85. Marmot, M. G, 1998, Improvement of social environment to improve health. Lancet 351 5760. 61 Better Integration 27-30 November 2001 Morgan, G, 1997, Images of organization, 2nd Edition, (Thousand Oaks: Sage Publications). Pettigrew, A. M,. 1973, The politics of organizational decision-making, (London: Tavistock). Pettigrew, A, 1987, The management of strategic change, (Oxford: Blackwell). Shannon, H. S, 1998, Workplace organizational factors and occupational accidents, in Occupational Injury: Risk, Prevention and Intervention. A.-M. Feyer and A. Williamson (Eds) (London, Taylor & Francis) 171-178. Strauss, A, 1987, Qualitative analysis for social scientists, (Cambridge: Cambridge University Press). Willer, D., Lovaglia, M. J. and Markovsky, B, 1997, Power and influence: a theoretical bridge, Social Forces, 76(2): 571-603. Wilson, D. C, 1992, A strategy of change: concepts and controversies in the management of change, (London: Routledge). 62 37th Annual Conference Ergonomics Society of Australia Inc. Home Based Work – A Health & Safety Challenge for Employers Heidi Brandis CRS Australia, Perth, Western Australia Allison Crunden CRS Australia, Melbourne, Victoria Keywords: Home based work, employee health & safety, ergonomic / OHS assessment, telecommuting ABSTRACT The introduction of electronic communication has facilitated more flexible work practices in the Australian workforce. There is a growing trend towards home based work which offers a range of benefits to both employees and employers. These include flexible working hours and conditions which can assist with family and other commitments. Additional benefits include savings in travel costs and commuting time, less distraction and fewer interruptions. This may lead to increases in productivity for the employee and subsequent increases in profitability for the employer. There are also some disadvantages involving human or financial costs to bear in mind, which may impact on the decision to conduct work from home. One of the issues requiring consideration is the health and safety of the employee working from home. This paper outlines an employer’s responsibilities towards home based workers and how an ergonomic/OHS evaluation can assist employers to meet these responsibilities and achieve compliance with OHS legislation. A photographic case study is included to illustrate the benefits of an OHS evaluation prior to the commencement of home based work. 1. INTRODUCTION With the advent of electronic communication and the promotion of flexible work practices, office workers are no longer “chained to their desk”. Using a range of media such as laptop computers, facsimile machines, electronic mail, mobile phones, and the internet, the physical location of the employee becomes irrelevant when conducting day to day work tasks. Consequently, working from home or “telecommuting” (McClay, 1998) is becoming more popular for employees and employers, as it can provide greater flexibility and balance between work, family commitments and personal needs. Australia’s home based workers increased by 29% to 4% of the workforce between 1989 and 1995. The largest increases were seen in the finance and business services, wholesale and retail and manufacturing (Hartmann and Patrickson 2000). In view of this developing trend, there are a range of pros and cons of home based work that should be considered, including the impact of this type of work on the employee’s occupational health and safety. 63 Better Integration 27-30 November 2001 2. ADVANTAGES AND DISADVANTAGES The opportunity to increase productivity and flexibility via home based work can be attractive to both employees and employers. The nature of home based work allows employees the benefits of flexible working hours and conditions which can assist with family and other commitments. Additional benefits include savings in travel costs and commuting time, less distraction and fewer interruptions thus increasing productivity (Working from Home Guide, 2000). Additionally, reduction in office overheads such as rental costs can have a significant impact on profitability for the employer (Banham, cited in McClay, 1998). With such a range of benefits it is easy to see why home based workers report greater job satisfaction than their office-based peers (McClay, 1998; Sturgeon 1996). To summarise, home based work gives employees greater control and flexibility which are significant factors in reducing stress and will ultimately result in a more satisfied and productive employee. Home based work can also reduce an organisation’s costs and increase profitability from improved productivity. Employers who adopt home based work arrangements have the potential to attract and retain valued and experienced employees. In the past, many parents remained at home with their children, often until they reached school age. This meant the loss of skilled, experienced employees from the workforce. It also made it difficult for those parents to re-enter the workforce after a long break, faced with changes in technology, work practices, expectations, etc, which may have caused anxiety or stress. Home based work can facilitate a gradual reintroduction into the workforce, which may have a positive impact on the organisation’s productivity and savings in recruitment and new staff induction/training. It is necessary to weigh the benefits of home based work for employees and employers against the human and financial costs and the need to clearly measure quality and quantity of work output. Home based work may not suit employees who require close supervision or high levels of interaction with other staff. The cost of setting up and maintaining an employee in a home based work environment is another consideration. Employees undertaking home based work are likely to experience less social interaction and greater isolation (Tassie, 1997; Hobbs & Armstrong 1998), with reduced access to personal supervision, training and development opportunities. Employers may be reluctant to approve home based work due to concerns about ergonomic hazards, OHS and security issues amongst others (Vassie, 2000; Standen, cited in Hartmann & Patrickson, 2000). This paper endeavours to address some of these concerns relating to employee health and safety. 3. THE IMPORTANCE OF OCCUPATIONAL HEALTH AND SAFETY FOR HOME BASED WORKERS “Normally, safety at home is primarily a family concern. However, when home becomes a satellite workplace, it becomes an employer safety concern as well” (Banham, cited in McClay 1998, p 40). Evidence suggests that home based workers do not always receive the health and safety protection due to them (Vassie, 2000). Creating a safe working environment in the home is essential. The home, unlike the office, has rarely been designed for use as a workplace. The home is primarily a domestic dwelling and as a result, work equipment and work areas may have to compete with household items. If home based work is undertaken, other members of 64 37th Annual Conference Ergonomics Society of Australia Inc. the household may be exposed to hazards and risks that would normally not exist if work was undertaken outside the home. Similarly, the home based worker may be exposed to domestic hazards not usually encountered in an office environment. The home based worker may therefore be increased risk of injury due to the combination of physical and psychological hazards outlined in the preceding sections. In addition, the limited ability of the employer to monitor the home environment may allow hazards to go unidentified and unaddressed. 5. LEGISLATION The state and federal OHS legislation in Australia aims to promote and protect the safety and health of people at work, which includes people working from home. Employers are responsible for providing and ensuring safe systems of work for employees, a responsibility which is not diminished regardless of the physical location of the work Employers must, as far as reasonably practicable: Provide and maintain a working environment in which employees are not exposed to hazards Provide the information, training and supervision necessary to ensure the health and safety of employees at work Keep information and records relating to the health and safety of employees Employ or engage suitable OHS persons to provide advice In some states, employers are required to notify WorkSafe of injuries or disease as prescribed in the Regulations. Employees, including those who are working from home, must co-operate with employers in their efforts to comply with occupational health and safety legislation. There are various offences and penalties specified in the OHS Acts / Regulations for employers and employees who do not comply with these requirements. 6. EMPLOYER’S RESPONSIBILITIES 5.1 Working From Home Policy Any employer accommodating home from Home Policy prior to the work Home Guide, 2000; Vassie, 2000). employees with clear guidelines on including: based work for their staff should develop a Working commencing (Home safe home, 1999; Working from This policy should provide an organisation and its how to conduct working from home arrangements, A definition of working from home The organisation’s employment policies and procedures eg. reporting of injuries/incidents/hazards The work hours, days and duties for working from home Provision, maintenance and ownership of equipment Responsibility of employees working from home for maintaining a safe work environment How work is to be monitored and by whom 65 Better Integration 27-30 November 2001 How the employee will obtain the information and training necessary to do the work safely Establish communication procedures & performance expectations Access and inspection including the employer’s rights to enter the home (adapted from Working from Home, Queensland Government Workplace Health & Safety, 2000) Employers should also ensure that home based workers are provided with a copy of the Home Based Work Policy and that they understand their obligation to adhere to the policy guidelines 5.2 Home Based Work OHS Assessment Employers should arrange an OHS assessment of the home workplace, which can be done by a qualified Occupational Health and Safety professional. The assessment should be carried out taking into account the work tasks, the materials used and the working environment. The assessment should also consider who else lives at the home. The following risk management approach should be taken: Identify any hazards Assess the risks and Take appropriate action to eliminate or reduce risks as far as possible Record the findings in a report to the employer for further follow up if required eg purchase or replacement of recommended equipment To complement the OHS assessment, it is recommended that employees be provided with comprehensive safety training in hazard identification, particularly with regard to electrical, fire, ergonomic and security issues. This training should occur prior to the commencement of home based work. It may also be useful for the employee to conduct regular (6 or 12 monthly) self-assessment checklists to be provided to the employer to ensure ongoing suitability of the home workplace. Another support mechanism to facilitate ongoing compliance with OHS requirements is contact with home based workers by “cyberspace safety representatives” (Gates, 1996, p 19) who can offer on-line information and guidance. Alternatively, home based workers can have telephone contact with a health and safety representative based at the usual office workplace with whom they could raise any health and safety concerns. 5.3 Provide And Maintain Safe Equipment There should be agreement on what equipment the employee will be using, who will provide it, who is responsible for maintaining it, and who is responsible for loss or damage to the equipment. Employers who provide equipment for their employee to carry out their work are responsible for its maintenance (Working from Home Guide, 2000). If employees use their own equipment and furniture, it must meet minimum workplace safety and health requirements and standards relevant to the type of work being done. Any information and training provided to office-based employees on how to use the equipment correctly and safely should also be provided to home based workers. Equipment may include, but is not limited to, office furniture such as the desk, chair, footstool, and 66 37th Annual Conference Ergonomics Society of Australia Inc. computer or safety related items such as fire extinguishers, smoke detectors, first aid kit and electrical surge protectors. 5.4 Communication Employers also need to consider the most appropriate means of communicating with workers who are based at home. In some home based arrangements, workers may be completely isolated from their colleagues. Employers should ensure that there are opportunities for workers to interact and meet with their co-workers on a regular basis to reduce feelings of isolation. 7. OHS ASSESSMENT TOOL Home based work presents a challenge to employers in terms of risk assessment and control, since the environment is not visible to them or easily accessed by the supervisor/manager. CRS Australia, Australia’s largest provider of injury management and prevention services, provides OHS assessments to assist employers to meet their legal obligations for home based workers. The assessment is conducted by an Occupational Therapist, Physiotherapist or Ergonomist and helps to reduce the risk of injury by identifying and then eliminating or reducing home workplace hazards. The assessment consists of a number of sections including the following: Office work environment Workstation layout and furniture/equipment Environmental factors (eg lighting, noise and thermal comfort) Manual handling & Postural issues Duties, Hours and Days of work Policies & Administrative requirements Housekeeping & Storage General safety issues including emergency evacuation procedure, first aid & fire safety 8. CASE STUDY To demonstrate the benefits of conducting a home based work OHS assessment, we will now present a photographic case study. Jane is a 32 year old manager with a Commonwealth Government department. Her role involves coordinating a team of 10 staff who are located around the state. Jane asked to work from home since her Department recently relocated 1.5 hours drive from her home. She has since arranged to work from home with her employer’s approval. Jane had a desk and chair at home, and the employer provided a laptop computer for e-mailing, word processing, database access, and Excel spreadsheets. Jane estimated that she spent approximately 4-5 hours per day operating the computer and the remainder completing paperwork and answering/making telephone calls. She attends the office for team meetings on a weekly basis. 67 Better Integration 27-30 November 2001 7.1 Problems Identified & Recommendations Implemented Prior to the assessment, Jane used the laptop at a small rectangular clerical desk featuring 100 mm thickness. The chair had inadequate lumbar and lateral trunk support, and did not adjust in seat base or backrest angle. Jane reported that it gave her low back pain. The desk thickness did not allow for Jane to elevate the chair adequately for keyboarding causing sustained elbow and wrist flexion. Documents were located to the left of the keyboard encouraging sustained neck flexion and rotation which Jane reported to be uncomfortable. The use of a laptop encouraged neck, elbow and wrist flexion due to fixed screen height and keyboard thickness. Following the ergonomic / OHS assessment, we recommended the provision of an L shaped desk, with an external monitor and keyboard to facilitate correct keying posture. A spare desk and fully adjustable ergonomic office chair was located at the office and provided to Jane at home. A height and angle adjustable footstool and document holder were also provided. Jane reported that the new workstation set-up was significantly more comfortable than using the laptop at the clerical desk. The use of a document holder between the keyboard and monitor also promoted symmetrical work posture, reducing neck and shoulder muscle strain. Lighting, noise and thermal comfort were all considered acceptable by the worker. Lighting could be controlled through curtains, task lighting and overhead lighting. Adequate storage space was available in file cabinets and bookshelves. Emergency access and egress was available through the front door approximately 5 metres from the home office. Smoke detectors had been installed in the passageway outside the room and Jane was aware of the need to evacuate the home in the case of a fire. The OHS assessment identified the main hazards as workstation layout and equipment, which were rectified following the assessment via provision of appropriate equipment and furniture. The goals of promoting improved comfort, posture, and satisfaction and reduced risk of injury were achieved. 9. WORKERS COMPENSATION An employee based at home is eligible for workers’ compensation and rehabilitation in the same way as any other employee. An organisation’s rehabilitation policies may need to be reviewed to include employees who work from home. 9. CONCLUSION The growth of home based work in Australia will see new opportunities for ergonomists to assist organisations to meet their OHS duty of care obligations. The case study presented today has illustrated the benefits of conducting a home workplace OHS/ergonomic assessment as part of an overall health and safety strategy to ensure that the risk of injury to home based workers is minimised. 10. ACKNOWLEDGMENTS Thank you to Leith Hoffmann and Sharyn Moore from CRS Australia (WA) and CRS Australia library staff (QLD), for assistance with background research. Thank you to Sandina 68 37th Annual Conference Ergonomics Society of Australia Inc. Bailey, CRS Australia (NSW) for presenting the paper on our behalf and to Stephen and Carol Thomas for assistance with the case study photographs. 11. REFERENCES Gates, E, 1996, Home alone? Occupational Safety & Health. July.14-19. Hartmann, L., and Patrickson, M, 2000, Externalising the workforce: Australian trends and issues for HRM. International Journal of Manpower 21 (1) 7-20 Hobbs, D., and Armstrong, J, 1998,. An experimental study of social and psychological aspects of teleworking. Facilitie,. 16 (12/13) Home Safe Home, 1999, Journal of Occupational Health & Safety – Aust NZ. 15(5)402-403 McClay, C.J, 1998, The development of work-at-home safety programs. Professional Safety. American Society of Safety Engineers. (January). Sturgeon, A, 1996, Telework: threats, risks and solutions. Information Management and Computer Security, 4(2) 27-38 Tassie, J, 1997, Home based workers at risk: outworkers & occupational health and safety. Safety Science, 25(1)179-186 Vassie, L, 2000, Managing homeworking: health and safety responsibilities. Employee Relations, 22 (6). Working from home guide, 2000, Queensland Government Workplace Health & Safety. May 2000. http://www.whs.qld.gov.au/guide/gde47.pdf 69 Better Integration 27-30 November 2001 70 37th Annual Conference Ergonomics Society of Australia Inc. Occupational Fitness, Standards, and Tests - Cautionary Tales from the Bush John R Brotherhood School of Exercise and Sports Science, The University of Sydney, Australia Keywords: Work, stress, strain, work capacity, fitness standards ABSTRACT This paper reviews some concepts of stress and strain in physical work, how they are applied to occupational ergonomics, and how they may be applied to occupational fitness. Workers' physiological and subjective responses to physically demanding work are determined by the demands of the work and the workers' capacities to perform the work. The conventional role of occupational ergonomics is to design work, or control work demands, so that they can be performed by the majority of workers with acceptable levels of strain and productivity. In some occupational tasks such as firefighting it is not possible to control work demands. In these circumstances fitness standards may be recommended in an attempt to reduce the risk of overstress. Recent research on bushfire fighters in Australia has shown that firefighters appear to pace themselves at similar levels of strain, regardless of a wide range of individual fitness. Physical fitness determined work performance rather than work strain. Furthermore, because the firefighters' work strains were considerably greater than common recommendations, the research suggests that fitness standards may not ensure that firefighters work within conventionally acceptable limits of strain. 1. INTRODUCTION Ergonomics is concerned with relationships between humans and their various domestic, occupational and leisure time activities. The study of these relationships is essential to enable the design of implements and machines, and the organisation of activities, to fit human capacities so that they promote performance and satisfaction without posing risk to health and safety. The fundamental relationship between the demands of activities and human function may be simply described in engineering terms of stress, strain and capacity. These relate the strain in a system to the ratio of the load or demand on the system to the capacity of the system to withstand that load, thus: Strain Load /Capacity As applied to humans strains are any relevant human responses to an activity. These responses may be physiological, biochemical, psychological, mechanical, and their level may range from trivial to pathological. The load or demand of the activity can be viewed as the 'effort' required to perform the activity. However, since many activities involve pace of performance, task demands may often be expressed as 'work rate'. Capacity is the maximal ability of the human function that is engaged in the activity imposing the load. 71 Better Integration 27-30 November 2001 2. STRESSES AND STRAINS IN PHYSICAL WORK These concepts are particularly applicable to the analysis of muscular activity. Task demands, indicated by force generation in static exercise and energy expenditure or oxygen uptake in dynamic exercise, can be easily identified and measured. Similarly, exercise 'capacities' indicated by the force of Maximal Voluntary Contraction (MVC) or maximal aerobic power (VO2max) are readily assessable. Both strength and aerobic power vary widely with body size, age, gender, health and fitness. Indeed, MVC and VO2max are measures of 'physical fitness'. Muscular exercise is also associated with the familiar subjective responses of exertion and fatigue, and with physiological responses such as heart rate, blood pressure, pulmonary ventilation, and lactic acid production, that are commonly used as measures of strain. The practical implications of these stress, strain relationships are illustrated in Figures 1-3. Although straight lines have been used in these figures to indicate the general direction of associations, some strains, and endurance, in fact show curvilinear relationships with stress. A Strain Response B Strain Response Average Low High Task load Performance Relative load % capacity C In A and B, the three lines indicate individual work capacities: low capacity average capacity high capacity Endurance Relative load (% capacity) or Strain Figure 1. Basic relationships between work stress and strain, and endurance Figure 1 summarises the basic relationships. Figure 1A, shows that for any individual strains increase as task load or intensity of performance increases. Figure 1A also shows that for any given absolute level of task load an individual with a relatively low capacity will suffer a greater level of strain than individuals with greater capacities. That is, among individuals strain is inversely proportional to capacity. Figure 1B, on the other hand, shows that if task load is expressed as a proportion of the functional capacity it is found that individual strains are similar. Thus when assessing the impact of task loads on individuals the 'relative load', that is, the fraction of capacity engaged by the load, is a more appropriate expression of the stress imposed by the task. Since strain and fatigue are directly proportional to work stress the ability to maintain work output over the work day, that is endurance, will be inversely 72 37th Annual Conference Ergonomics Society of Australia Inc. proportional to work stress (Figure 1 C). It follows that if an individual increases functional capacity, for example by increasing physical fitness, the relative load imposed by a fixed task will be lower and the strain experienced by the individual will be correspondingly lower. For ergonomics to succeed in 'fitting work to the worker', in addition to defining task demands and loads, and understanding human functional capacities, acceptable levels of strain must also be defined. Presumably acceptable levels of strain are those that are associated subjectively with absence of undue discomfort (yet may allow more or less moderate degrees of subjective effort), and physiologically do not lead to premature fatigue or injury. Broad recommendations for upper limits for physical work rates and physiological strains that are considered tolerable for an eight hour day are 35-50 % VO2 max and corresponding heart rates 100-130 beats per min. The grading of physical work intensity and criteria for acceptable work strains are discussed in detail in, e.g. , Grandjean (1988), and Asfour et al. (1988). 2.1 Fixed pace work In a number of circumstances physical demands may be set at a fixed level (Figure 2A). The effects can be clearly demonstrated in the laboratory when a diverse group of people perform the same task such as walking on a treadmill at fixed speed and gradient. A Task load Performance A fixed work load B, C hypothetical levels of acceptable stress and strain Low Average High Capacity B C Relative load % capacity Strain Response Low Average High Capacity Low Average High Capacity Figure 2. Stresses and strains in fixed pace work. Figures 2B & C show that individuals with low work capacity experience greater levels of stress and strain than individuals with greater capacities. In the real world, if task demands are externally fixed, similar responses will be found. For example, in soldiers carrying standard packs and marching at a fixed pace. The less fit individuals in the squad will fatigue more rapidly, and indeed are at greater risk of heat illness, than their fitter comrades. Likewise fixed-pace production line work, or any 73 Better Integration 27-30 November 2001 occupational task where the work rate is set externally to the worker, will be more stressful for some than for others (Figure 2B). For some people the work stress and their strains may exceed tolerable levels. Standards or guidelines for controlling stress in physically demanding tasks such as manual handling must be based on this fixed work rate model. However, because such recommendations must be applicable to the majority of the work force in which work capacities vary widely the recommended work demands must be kept at a conservatively low level. 2.2 Self-paced work In contrast to the artificially controlled conditions set in the laboratory, and those imposed by military discipline and industrial engineers, most human activities allow self-pacing. Figure 3 summarises the likely consequences of self-pacing for work stresses, strains and performance. A B Relative load % capacity Strain responses Task load Performance Productivity Low Average High Capacity Low Average High Capacity recommended level of acceptable strain Figure 3. Stresses, strains and performance in self-paced work The most familiar example of self-pacing is found in athletic competition where athletes exercise at levels close to their maximal capacities. By and large the levels of strain are similar amongst athletes but their performances vary according to their capacities , for example, with VO2 max for endurance runners (Noakes 1988). Similar evidence for selfpacing has been found in various types of occupational work (eg, Astrand 1967, Davies et al. 1976, Brotherhood et al. 1997). Thus it seems that in strenuous work people pace themselves to achieve acceptable levels of subjective and physiological strain. Figure 3B shows that in these circumstances work load and performance, and not work strains, are associated with work capacity. While the principle role of occupational ergonomics is generally viewed as 'fitting work to the worker' there are some occupations where the physical work demands may be high, cannot always be predicted and cannot be controlled. This is the case for some occupations such as firefighting. In these circumstances 'fitting the worker to the work' might be considered. That is, workers might be selected according to their physical capacities or fitness in attempt to reduce the risk of excess work strain. In this case, knowledge about the demands of the job are required in order to determine the work capacity that workers require to do the job without becoming overstressed. 74 37th Annual Conference Ergonomics Society of Australia Inc. 3. OCCUPATIONAL FITNESS REQUIREMENTS Traditionally, the determination of occupational fitness requirements has followed the fixed work model illustrated in Figure 2. First, the energy demands of the job are measured and assumed to be similar for all workers. Then, since the stress of physical work that must be maintained for the working day should not exceed about 50% capacity, an aerobic fitness requirement (usually assessed as maximum aerobic power in relation to body mass) is set at twice the energy cost of the job. This is the basis of the fitness standard used for the selection of wildland firefighters in the USA. Preliminary research found that the average oxygen cost of a variety of forest firefighting activities was about 22.5 ml O2. kg body mass-1. min-1. Accordingly, the fitness requirement was set at twice this level as a VO2max of 45 ml O2. kg body mass-1. min-1. (Sharkey 1997). Similarly, in Canada, fitness recommendations for wildland firefighters have been based on the energy costs of firefighting tasks performed by an elite firefighting crew (McFadyen et al 1994). 3.1 Stress, strain and productivity in Australian bushfire fighters Recent research in Australia on stress, strain and productivity in male firefighters suppressing large scale experimental bush fires has shown that the laboratory model (Figure 2) utilised in North America may be inappropriate for setting fitness standards (Budd et al. 1997). In firefighters working at self-selected pace physiological strains differed little between individuals, despite a two fold range of individual fitness levels. Furthermore, the average levels of physiological strain: heart rates >150 bt min-1 and body core temperatures >38.3C, were well in excess of recommendations for prolonged occupational work. By contrast, however, individual energy expenditures ranged about twofold and productivity was strongly related to work capacity. It seems, therefore that the firefighters were behaving according to the model shown in Figure 3. Apparently they selected their work pace according to their fitness, so that, rather than controlling their physiological strains, their fitness determined their productivity. Even the least fit men were generally considered to be adequately productive. Thus a nearly two fold range of physical fitness was apparently adequate for satisfactory task performance.. 4. LIMITATIONS TO OCCUPATIONAL FITNESS STANDARDS These Australian observations suggest that in self-paced work energy expenditure will reflect the work capacity of the people doing the work. Thus if a fitness standard is to be based on the energy cost of the job it will be important to base the standard on the energy expenditure and performance of typical members of the population from which the work force will be selected. The Canadian fitness standard proved too high for otherwise effective standard crews. Possibly because it was based on the performance of elite firefighters. In the US, although the wildland firefighting fitness standard does not discriminate against women because it is relative to body mass (45 ml O2. kg body mass-1. min-1. ), the productivity and performance of women achieving the standard tend to be significantly lower than men of the same ‘fitness’. This is because on average women are smaller than men and are not able to generate as much strength and power for tasks such as carrying equipment, shovelling and dragging hoses (Sharkey 1997). 75 Better Integration 27-30 November 2001 Bushfirefighters clearly must be healthy and fit. However, while fitness standards could be invoked they may not ensure that firefighters work only within conventionally acceptable limits of strain. On the other hand they may result in exclusion of people who by virtue of experience, knowledge and other qualities may otherwise be effective firefighters. Current recommendations for bushfire fighters in Australia emphasise the importance of achieving work fitness by regular exercise which has been demonstrated to markedly reduce physiological strain while firefighting (Budd et al. 1996). 5. REFERENCES Asfour, S.S., Genaidy, A.M., and Mital A., 1988, Physiological guidelines for the design of manual lifting and lowering tasks: the state of the art, Am. Ind. Hyg Assoc. J, 49(4), 150-160. Astrand, I., 1967, Degree of strain during building work as related to individual aerobic work capacity, Ergonomics, 10(3), 293-303. Brotherhood, J.R., Budd, G.M., Hendrie, A.L., Jfery, S.E., Beasley, B.A., Costin, B.P., Wu Zhien, Baker, M. M., Cheney, N.P., and Dawson M.P. , 1997, Project Aquarius 11. Effects of fitness, fatness, body size and age on the energy expenditure strain and productivity of men suppressing wildland fires, Project Aquarius Special Issue, Int. J.Wildland Fire, 7(2), 181199. Budd, G. M., Brotherhood, J., Hendrie, L., Cheney, P., Dawson, M., 1996, Safe and Productive Bushfirefighting with Hand Tools (Australian Government Publishing Service, Canberra). Budd, G.M., Brotherhood, J.R., Hendrie, A.L., Jfery, S.E., Beasley, B.A., Costin, B.P., Wu Zhien, Baker, M. M., Cheney, N.P., and Dawson M.P. , 1997, Project Aquarius. Stress, strain and productivity in wildland firefighters, Special Issue, Int. J. Wildland Fire 7(2), 69-218. Davies, C.T.M., Brotherhood, J.R., Collins, K.J., Dore, C., Imms, F., Musgrove, J., Weiner, J.S. et al., 1976, Energy expenditure and physiological performance of Sudanese cane cutters. Brit. J. Industr. Med. 33, 181-186. Grandjean, E., 1988, Fitting the Task to the Man (Taylor & Francis, London), 82-103. McFadyen, P., Pethick, W., Sleivert, G.G., and Wenger H.A., 1994, Physiological cost of wildland firefighting and bona fide occupational fitness requirements, Department of Physical Education, University of Victoria, B.C. 32 pages. Noakes, T. D., 1988, Implications of exercise testing for prediction of athletic performance: a contemporary perspective. Med. Sci. Sports Exerc. 20, 319-330. Sharkey, B., 1997, Fitness and work Capacity, second edition (Tech. Rep. 9751-2814 MTDC.: US Department of Agriculture, Forest Service, Missoula, MT). 76 37th Annual Conference Ergonomics Society of Australia Inc. Effects on Performance of Anxiety and Depression in the Working Population Susan Brown, Sarah Hastings, Roger A Haslam Health and Safety Ergonomics Unit, Department of Human Sciences, Loughborough University, UK. Cheryl O Haslam Department of Health Studies, Brunel University, Osterley Campus, UK. Keywords: Anxiety and depression, focus groups, prescribed medication, psychotropic drugs, work performance. ABSTRACT It is not clear to what extent medication taken for psychiatric illness affects a person’s quality of work and productivity. Perhaps more importantly very little is known about the possible consequences for workplace safety. The use of focus groups in this study produced data on the personal experiences of mental health problems and the impact of psychotropic drugs on work performance from members of the working population. Focus group discussions also gathered information from a range of work sectors, on the organisational perspectives of mental health in the workplace. Initial analysis of the data indicated similarities in the symptoms of anxiety and depression, and the side effects of the medication, experienced by participants. Compliance with drug regimes was affected by the amount of information respondents were given about their medication and the side effects they experienced. Workers’ concerns about drug dependency also affected their use of medication causing them to take less than their prescribed dose or to discontinue the treatment. The people experiencing anxiety and depression relied upon managers or colleagues for support and rehabilitation in the workplace but felt that their lack of knowledge and understanding of mental health issues made it difficult for them to offer appropriate help. Participants considered practical help from people within the workplace most beneficial to enable them to cope at work. 1. INTRODUCTION The extent to which medication is used to treat depression and anxiety in the working population is unknown, although levels are thought to be considerable (Dunn et al. 1986; Potter, 1990). Studies have highlighted the poor knowledge that exists concerning the effects of prescribed medication on work performance (Dunn et al. 1986; Tilson, 1990). Psychotropic medicines impair performance on a wide range of laboratory measures, with effects found for attention, vigilance, memory and motor coordination (Dunn et al. 1986; Potter, 1990). However, it is not clear how these findings translate to performance in the workplace (Dunn et al. 1986; Nicholson, 1990). There are problems with generalising from laboratory studies as they are often limited to testing with young, healthy subjects and minor decrements in performance on sensitive laboratory tasks may have little relevance to real 77 Better Integration 27-30 November 2001 world activities (Nicholson, 1990; Cohen, 1984). It is not, therefore, clear to what extent medication may affect quality of work, productivity and safety. Lack of treatment for psychiatric illnesses may actually be a greater problem in terms of work performance than the side effects of medication (Potter, 1990). Employees suffering with depression or anxiety are likely to experience a range of symptoms that would impair performance at work, including: tiredness, lack of motivation, poor concentration and forgetfulness, poor timekeeping and attendance. Failure to seek or comply with treatment may arise from the stigma associated with mental ill health or, alternatively, some people may be reluctant to take medication because of fears about side effects. Studies do support the view that the workplace is implicated as one cause or source of mental ill health (Cox, 1993). Good management of stressors such as incorrect workload, role ambiguity etc in the workplace can lead to improved mental health (Maguire, 1997). This research collected new and in-depth data on anxiety and depression and the use of psychotropic medication among the working population. The aim was to improve understanding of the impact of mental health problems and the treatment for these conditions on performance and safety in the workplace. 2. METHOD This research used focus groups. A focus group is a group interview whereby the data obtained arise from the discourse generated by a discussion (Morgan, 1997). Topics are supplied by the researcher who acts as ‘moderator’ for the discussion, the moderator should facilitate discussion rather than interview. This is a very useful exposure assessment technique for measuring psychosocial factors. The technique is well suited to this study, which aimed to elicit information about the personal experience of mental health problems and the impact of drugs on work performance. Focus groups also afford participants a degree of anonymity. Participants were recruited throughout the United Kingdom. A total of fourteen focus groups were planned across a broad spectrum of employment sectors, each group having a minimum of six and up to ten participants; the discussions were recorded and fully transcribed. Data from the focus groups were sorted into thematic categories for analysis. Organisational perspectives including: recruitment, support and rehabilitation were explored with two focus groups, comprising staff from Human Resources, Personnel, Occupational Health and Occupational Health and Safety departments, representing a variety of organisations. Two groups were run with participants from anxiety and depression management courses conducted by clinical psychology services, these participants had a wide range of occupations and responsibilities. The remaining groups will recruit employees from various employment sectors in either managerial or non-managerial roles. Employment sectors known to be at high risk for mental health problems are being targeted (healthcare, education, manufacturing) and other sectors such as construction and transport to explore any differences in experience resulting from various working practices and organisational structure. Participants will also be grouped according to their managerial and supervisory responsibilities. 78 37th Annual Conference Ergonomics Society of Australia Inc. 3. RESULTS 3.1 Focus Groups Participants were allocated to focus groups according to their occupation or level of managerial or supervisory responsibility, table 1. Table 1. Profile of focus group samples Focus group Gender Organisational 1 5 female 2 male Organisational 2 7 female 3 male Clinical 1 8 female Clinical 2 5 female 2 male Education 2 female 5 male Support workers 7 females Age range Occupations 25 – 50+ occupational health; occupational safety & health personnel/HR; counselling & support mixed mixed 20 – 50+ 19 – 50+ 28 - 63 30’s – 60’s teachers (non-managerial); education support staff 29 – 50+ mixed (non-managerial) Due to limited numbers of volunteers by geographical location or occupation, criteria were used to select participants who had similar levels of managerial or supervisory responsibilities in their work. A summary of the work sectors represented within the groups is shown in table 2. Table 2. Employment sectors represented in focus groups Public sector Private sector Organisational groups Defence Local authority Local government National Health Service Engineering Heavy industry Retail Pharmaceutical Clinical groups Further education tutor Local authority administration NHS – Scientific Officer Electrician Garage foreman Office worker - SME Photographic assistant Retail – large company Telesales Vet Unemployed 79 Occupation groups Higher Education support work Local government Police support work Teachers (nonmanagerial) Voluntary sector Better Integration 27-30 November 2001 3.2 Symptoms and Side Effects Preliminary results indicate that the symptoms of anxiety and depression were often reported to be similar to the side effects of medication including: confusion, dizziness, forgetfulness and difficulties with decision-making. Participants found it difficult to differentiate between the effects of the medication and the condition itself. Medication caused feelings of nausea and a constantly dry mouth for many workers, headaches and shaking hands were also identified as side effects. 3.3 Medication Participants were often diagnosed and prescribed medication only when they became unable to continue at work. Non-compliance with drug regimes was common, people took fewer and smaller doses than prescribed and discontinued the medication of their own volition. Addiction and dependency were major concerns of people taking medication; they would take reduced or less frequent doses because of this. Discontinuation occurred when people felt worse when taking the drugs than without them. There was also a tendency for people to stop their medication too early, when their symptoms began to improve. Some participants felt that they would be unable to return to work while they were taking medication; they felt that a prolonged period of treatment would necessitate a long absence from work and tried to manage without the medication. Side effects were often severe in the first few weeks during which time the medication was changed or discontinued by the General Practitioner (GP). One person had his medication monitored by a Community Psychiatric Nurse (CPN). Some participants felt that prescribing medication was a process of trial and error to find the right drugs for each person. 3.4 Effects on Work Respondents felt that it took them longer to do their work and that their medical condition caused them to have lower performance levels. Many felt unable to cope with their workload even though it may not have changed. Safety issues concerned them with regard to their responsibilities to others e.g. teacher, car mechanic. Employees with many years experience were finding that their job had changed radically and they were not trained or supported to manage the changes. 3.5 Organisational Issues Most organisations did not deal with mental health issues any differently to physical health issues and rehabilitation periods were often limited to one month, this could be extended when occupational health staff supported the employee and manger during the rehabilitation period. However occupational health services were not available in all organisations, and those who did have this service were not always willing to implement the recommendations made for work adaptations and rehabilitation. Support and rehabilitation of employees experiencing anxiety and depression included: reduced workload, reduced hours or a change of job on a temporary or permanent basis. Work was often target driven and some tasks were not flexible enough to allow modification of working hours or output to enable employees to remain at work. Feedback from organisational representatives suggested that high levels of pressure were simply a part of present day lifestyles. Managers were thought to be under pressure themselves making them less tolerant of staff with problems they don’t fully 80 37th Annual Conference Ergonomics Society of Australia Inc. understand such as anxiety and depression. Part of the role of human resources was seen to be enabling a manager to deal appropriately with those problems. 3.6 Management Issues Management methods were identified as contributory factors in work related anxiety and depression. It was felt that some managers had not been trained in management skills when their work responsibilities had changed. Employees who struggled with their workload were often given time management training as the problem was seen to be with the individual rather than the organisation. Managers questioned the competence of long standing employees who started to make uncharacteristic errors without exploring the possible causes of the change in their standard of work. It was thought that training should be available to improve the understanding of mental health issues by managers and colleagues. 3.7 Support in the Workplace When asked what kind of support they would want at work, respondents highlighted the need for practical help with the volume of work at difficult times. Many people suggested that simple but time-consuming tasks caused them unnecessary stress. It was also suggested that in-house support services such as occupational health or a counselling service should be available, or simply the opportunity for a confidential talk. Respondents felt that if anxiety and depression were better understood, managers and colleagues would be more able to give appropriate support. 4. DISCUSSION AND CONCLUSIONS Workers felt that they were not well informed about the side effects of drug treatment or how long they should expect to continue medication. The effects of anxiety and depression made it difficult for people to act on the information they were given. Monitoring by a CPN gave reassurance if side effects became a problem and alerted doctors to the need for a review of medication. Non-compliance was common, side effects from the medication and concerns about dependency were major issues, however discontinuation was also the result of individuals ‘feeling better’ or wanting to get back to work. Many participants did not begin to take medication until they were absent from work due to anxiety and depression and they found it difficult to differentiate between the effect of the condition and the effect of the medication on their work performance, although it was thought to be due to both. Participants were often reluctant to tell their employer that they had anxiety and depression due to the stigma and the negative consequences it might have on their career. Support at work was most beneficial when colleagues were able to help with the workload or offer the opportunity for a confidential talk. Support services such as human resources and counselling services felt themselves to be in a difficult position if they identified potential problems in the organisation such as bullying or harassment but were bound by confidentiality. This study is providing detailed information regarding the impact of mental health problems and their treatment on performance at work. The results will inform future guidelines for employers and employees. 81 Better Integration 27-30 November 2001 5. ACKNOWLEDGMENTS We wish to acknowledge the support of the Health and Safety Executive (HSE) who are funding this research. The views expressed, however are those of the authors and do not necessarily represent those of the HSE. We would also like to thank our focus group participants for their support and the time they gave so generously to this study. 6. REFERENCES Cohen, A. F., Posner, J., Ashby, L., Smith, R. and Peck, A.W., 1984, A comparison of methods for assessing the sedative effects of diphenhydramine on skills related to car driving. European Journal of Clinical Pharmacology; 27: 477-482. Cox, T., 1993, Stress research and Stress management: Putting Theory to Work (HSE). Dunne, M., Hartley, L., and Fahey, M., 1986, Stress, anti-anxiety drugs and work performance. In: Trends in Ergonomics of Work, 23rd annual conference of the Ergonomics Society of Australia and New Zealand, pp 170-177. Health and Safety Executive, 1999. Health and Safety Statistics 1998/99. HSE, 1999, ISBN 0 7176 1716 5. Maguire, K., 1997, Mental health: A major dimension of occupational health. Workshops at IOSH 1997, pp1-8. Morgan, D.L., 1997, Focus groups as qualitative research. 2nd Ed, (Sage Publications, California). Nicholson, A.N., 1990, Medication and skilled work. In: Human factors and Hazardous Situations, Proceedings of the Royal Society Discussion Meeting, 28 & 29 June. (Edited by Broadbent, D.E., Reason, J. and Baddeley, A.), (Clarendon press: Oxford), pp 65-70. Potter, W.Z., 1990, Psychotropic medications and work performance. Journal of Occupational Medicine; 32: 355-361. Tilson, H.H., 1990, Medication monitoring in the workplace: toward improving our system of epidemiologic intelligence. Journal of Occupational Medicine; 32: 313-319. 82 37th Annual Conference Ergonomics Society of Australia Inc. Project Update: Evaluation of an Ergonomics Program Intervention to Prevent Injuries due to Manual Tasks – PerforM Robin Burgess-Limerick School of Human Movement Studies, The University of Queensland Roxanne Egeskov Division of Workplace Health & Safety, DIR (Queensland) Leon Straker School of Physiotherapy, Curtin University of Technology Clare Pollock School of Psychology, Curtin University of Technology Wendy Brown School of Human Movement Studies, The University of Queensland Keywords: Manual tasks, program evaluation, participative ergonomics, RCT ABSTRACT This paper provides an update on the progress of a randomised controlled trial of a participative ergonomics program which aims to reduce the risk of injury due to manual tasks. The project is being undertaken with funding from QComp (Workcover Queensland) and the National Health and Medical Research Council. An audit tool was developed which assesses manual task risk management systems, and provides an assessment of the risk of injury due to manual tasks within each workplace through an assessment of a sample of tasks within each workplace. Training was provided to 45 inspectors in the use of tool. Audits of 120 south east Queensland workplaces employing between 30-100 people in construction related manufacturing and wholesaling, food processing other than meat, nursing homes and accommodation for the aged, were undertaken in October – December, 2000. These workplaces were invited to participate in the trial of the Participative Ergonomics for Manual tasks (PErforM) program. 48 workplaces accepted the invitation, and 31 were randomly assigned to participate in the period February – August, 2001. All workplaces will be audited again in April – June 2002, and the second group of workplaces will then receive the program. Workers compensation data for each workplace (provided by QStats) and the audit results will allow an evaluation of the short term outcome of the program. Interviews are being undertaken with staff and management of participating workplaces to obtain an understanding of the intervention process and the factors which influence the success (or otherwise) of the intervention. 83 Better Integration 27-30 November 2001 1. INTRODUCTION The direct health costs of occupational injuries exceed $1,360 Million each year (SRDC, 1999) and the total annual economic cost of these injuries is estimated at $27,000 Million (NOHSC, 1998). Approximately 40% of all occupational injuries are musculoskeletal injuries associated with manual tasks. There is widespread recognition of the magnitude of the problem, but little evidence for the effectiveness of any of the interventions attempted to date (such as selection, training, or protective equipment). Most occupational health experts and authorities believe that implementation of a comprehensive ergonomics program is likely to be the most effective means of reducing exposure to musculoskeletal injury risks associated with manual tasks. In 1996 the United States General Accounting Office was requested by the US congress to identify the core elements of effective ergonomics programs and determine the benefits, or otherwise, of such programs. While not a controlled trial, the resulting report (GAO/HEHS, 1997) documents the experiences of five large companies across a range of industries. The core elements of a successful ergonomics program were identified as management commitment, employee involvement, hazard identification, risk control, employee training and education, and appropriate medical management. The benefits were found to include a reduction of injury rates and compensation costs at all companies. Importantly, the report also identified the need of employers, and especially small to medium sized employers, for assistance in implementing an ergonomics program. This report, in part at least, provided the impetus for the US Occupational Health and Safety Authority to propose a an “Ergonomics” Standard which would have made the implementation of an ergonomics program mandatory for about one third of US workplaces. Support for this proposal was not unanimous, however, and the standard was repealed after two months. Some authors have questioned the likely effectiveness of such programs (eg., Hart et al., 1998) and the lack of a firm empirical basis (see eg., Dempsey, 1998) is seen as an impediment to its implementation. Evidence regarding the effectiveness of such a program is required to justify the significant expenditure required, but this evidence is not available. Indeed, randomised controlled trials of occupational injury prevention interventions are rare, and typically only the weakest quasi-experimental designs have been employed (see Zwerling et al, 1997 for a review). This interdisciplinary project brings together researchers from Schools of Human Movement Studies, Physiotherapy and Psychology at The University of Queensland and Curtin University of Technology to collaborate with Queensland Division of Workplace Health & Safety in a randomised controlled trial of an ergonomics program intervention. The project is being conducted in consultation with a reference group comprised of stakeholder representatives from government, professional associations, and industry bodies. The project was initially funded by Q-Comp, the regulatory services division of Workcover Queensland. Additional funding has been provided to the research project by the National Health and Medical Research Council in the form of a “Translational Grant in Injury”, of which four were awarded nationally in 2000 from NHMRC strategic funds. This funding is to undertake an evaluation of the intervention process in addition to the outcome measures. 84 37th Annual Conference Ergonomics Society of Australia Inc. 2. RESEARCH DESIGN A schematic description of the research design is presented in Figure 1. Following the random selection of 150 small to medium workplaces (30-100 employees) across three high risk industry sectors (nursing homes and accommodation for the aged, food processing excluding meat, construction related manufacturing and wholesaling), 10 workplaces from each industry were randomly assigned to a single audit group (group 1) while the remaining 120 will receive two audits throughout the project. An audit tool was developed by the investigators, and trialed and revised in conjunction with a small group of DWHS inspectors. The tool assesses management systems related to manual tasks, and provides an assessment of the risk of injury due to manual tasks within each workplace through an assessment of a sample of tasks within each workplace. Training in the use of the tool was provided to 45 inspectors, and the 120 workplaces were audited in October – December, 2000, as part of the Division of Workplace Health and Safety audit of a total of 204 workplaces across the whole state. The audits involved an assessment of 1046 tasks, and resulted in 246 improvement notices, and 3 prohibition notices. Formal advice relating to a further 625 tasks was provided. Forty-eight of the 120 eligible workplaces volunteered to participate in the trial of the PErforM program. Thirty-one were randomly assigned to receive the program between February and July 2001 (group 2), with the remainder scheduled to participate July-November 2002 (group 3) following the second round of audits in April – June 2002. The remaining workplaces which did not volunteer constitute group 4. A description of the intervention follows in the next section. The study design allows for the impact of critical confounding variables such as time of program implementation and number of audits to be assessed. If these factors are significant they will be used as covariates in subsequent analysis. A mixed model multivariate analysis of variance approach will be used to evaluate the effectiveness of the intervention using data from groups 2 and 3. Analysis will be conducted initially at an industry level, with additional analysis at an organisation level. The relationships between quantitative dependent variables (risk exposure, legislative compliance, and claims experience) will be assessed via calculation of Pearson product moment correlation coefficients, and 95% confidence interval of these correlations calculated utilising a Fisher-Z transformation. Calculation of Cohen’s effect sizes (d), and odds ratios, and the 95% confidence interval of these effect size statistics will also be assessed in a series of pair-wise planned comparisons. The impact of the ergonomics program intervention on risk exposure, legislative compliance and compensation claims experienced will be assessed by a comparison of pre and post intervention data obtained from the experimental and control groups (Groups 2 and 3). The changes in these measures over a 12 month period in the absence of audit or intervention will be assessed by comparing the single audits group (group 1) results, with the data obtained in the first audit of the remaining groups (2, 3 and 4). The influence of a single audit alone will be assessed by comparing the data obtained from the single audit group (group 1) with the data obtained in the contemporaneous second audit of control and non-volunteer groups (Groups 3 and 4). Variation in the results between the industry sectors will be explored by repeating these comparisons on data obtained from workplaces within each industry sector and utilising multiple logistic regression. 85 Better Integration 27-30 November 2001 Interviews will be undertaken with staff and management in each workplace participating in the program. Following transcription, analysis of the data obtained via interview and focus group will take the form of iterative thematic analysis, case summaries, and workshopping to create a grounded understanding of the intervention process. Combination of the audit and claims experience data with that obtained via interview and focus groups will allow variability in intervention effectiveness across workplaces to be explored and an improved understanding regarding the factors contributing to the degree of success of the intervention to be gained. Random s election o f 150 small to mediu m wo rkplaces acros s 3 high ris k indu stries. Ran dom ass ignment of 120 to dual audit grou p Sing le audit group Dual audit g roup Aud it 1 o f 120 wo rkplaces acros s 3 indus tries 50 Vo lunteers 70 Non-v olun teers Randomly as signed to exp erimental an d control grou ps 30 Experimental workplaces 20 Contro l workplaces Intervention (Interviews & fo cus g ro ups) (group 1 ) Contemporaneous Au dits 30 workplaces (group 2 ) Aud it 2 , 6 mon ths after interv ention (group 3 ) Aud it 2 (group 4 ) Aud it 2 Intervention for control grou p Lo ng term follow up Figure 1: Schematic representation of research design 3. THE “PErforM” PROGRAM The program involves four visits to each workplace by a PErforM consultant. The exact content of each contact is modified to suit the requirements of the individual workplaces, but the following constitutes a typical arrangement. 86 37th Annual Conference Ergonomics Society of Australia Inc. Visit 1: Management briefing and workplace familiarisation. The consultant provided the manager with a thorough briefing regarding the training to be provided to staff; negotiated how the training may be delivered with minimum disruption to the workplace; and discussed the most appropriate way of assessing workplace performance (1 hour). The consultant was then escorted through the workplace to gain an appreciation of the details of the workplace (1 hour). The consultant also provided the manager with information explaining the program which was suitable for distribution to staff. Visit 2: Management systems, supervisor and WHSO briefing, videotaping tasks. The consultant assisted the manager, or delegate, in the development/improvement of OH&S management systems (2 hours). This incorporated discussion of the results of the DWHS manual tasks audit. The consultant then provided a briefing to supervisors of the work teams which were to be involved in the training, and to the Workplace Health and Safety Officer. This briefing provided the supervisors with information regarding the management systems and content of the training (1 hour). The consultant requested assistance from the supervisors in identifying relevant manual tasks suitable for videotaping (1 hour). The objective was to obtain workplace specific illustrations to utilise in subsequent training. Visit 3: Risk management training. The core of the PErforM program was training of 1-3 intact work teams in manual tasks risk management. The training focused on enabling staff to meet the requirements of the Queensland Manual Tasks Advisory Standard and incorporated video clips of specific workplace tasks (1-3 work teams x 90 minutes). Between visits 3 & 4 each work team was asked to conduct and document manual tasks risk assessment of selected tasks within their workplace and to suggest control measures. Visit 4: Work team debriefing. The final visit involved a review of the risk assessments conducted by each work team to provide feedback regarding the assessments and control measures suggested (1-3 teams x 90 minutes). Questionnaires assessing group cohesion, work group characteristics and safety climate were also distributed to each worker at this session. Workplace follow up: The PErforM consultants were available for further assistance for a limited time following the program delivery. Evaluation Interviews: The evaluation process also involves interviews with management, supervisors and staff on (at most) three occasions at 3 monthly intervals in the nine months following the implementation of the program. The purpose of these interviews is to evaluate the program and determine how the process might be improved. 4. WHAT WE HAVE LEARNED (OR CONFIRMED) SO FAR… While the outcome of the program in quantitative terms will not be known for some time, a number of comments can be made. It was remarkably difficult to interest many workplaces in participating in the (free) trial. Some workplaces were undergoing changes in location, ownership etc which precluded participation. Others, particularly in the construction related industries, cited severe economic hardship resulting in significant loss of staff and/or preoccupation with obtaining work. Other reasons given involved either a belief that the workplace did not have any manual tasks risks or, more commonly, an unwillingness to 87 Better Integration 27-30 November 2001 commit staff time to the training required. Given that the requirement for staff training was kept to an absolute minimum (a total of 3 hours over two days plus time to undertake risk assessments), and that the program was being offered at no cost, this may indicate that even if the intervention proves to be effective, a problem will still exist to ensure that such training is provided in many workplaces. From our experiences of implementing the program in the 30 small to medium sized workplaces who have participated in the trial, the following were observed: The program was generally very well received by the staff and management. The use of workplace specific video clips was very effective means of increasing the perceived relevance of the training and understanding of manual tasks risk factors. Following the 90 minute training session, staff with a large range of educational backgrounds were capable of undertaking a manual tasks risk assessment. It may be possible to reduce the time of each session to 60 minutes (as was necessary on some occasions). It may be better to combine visits 3 and 4 if rostering makes it difficult to get the same group together for a second session. Staff from non-english speaking backgrounds or low literacy were able to perform the risk assessment with assistance from other staff (working in pairs). Staff who perceived (rightly or wrongly) that the management of the workplace were unlikely to implement controls were much less enthusiastic and less likely to generate solutions to risks identified. Lack of confidence in any link in the chain of responsibility may have this effect. Staff who were not replaced during the training (and thus had to “catch up” later) were less motivated to participate. There is likely to be considerable variation between workplaces in the benefits gained. Although assistance was provided with management systems were required, workplaces with established reporting systems are likely to gain greater benefit from the training. Those workplaces with a prior history of implementing controls and consultative management practices are likely to experience greater participation by staff with consequently better results. Low staff turnover is also likely to be a positive factor. 5. ACKNOWLEDGMENTS This project is funded by Q-Comp (Workcover Queensland) and the National Medical Research Council. Donna Lee, Karen O’Rourke, and Sue Price provided the interventions to the workplaces. Excellent assistance has also been provided by Division of Workplace Health & Safety inspectors and other staff. 6. REFERENCES Dempsey, P.G, 1998, A critical review of biomechanical, epidemiological, physiological and psychophysical criteria for designing manual materials handling tasks. Ergonomics 41, 73-88. Hart, D.L., Isernhagen, S.J. and Matheson, L.N, 1998, Impact of the Dayton Tire case. Work 11: 119-121. 88 37th Annual Conference Ergonomics Society of Australia Inc. Government Accounting Office, 1997, Worker protection – Private sector ergonomics programs yield positive reports. GAO/HEHS-97-163. National Occupational Health and Safety Commission, 1998, Compendium of workers’ compensation statistics, Australia, 1996-97. NOHSC. Strategic Research Development Committee, 1999, Paradigm shift. Injury: from problem to prevention. New research direction. NHMRC. Zwerling, C., Daltroy, L.H., Fine, L.J., Johnstone, J.J., Melius, J., Silverstein, B.A, 1997, Design and conduct of occupational injury intervention studies: A review of evaluation strategies. American Journal of Industrial Medicine 23: 164-179. 89 Better Integration 27-30 November 2001 90 37th Annual Conference Ergonomics Society of Australia Inc. Ergonomic Review of Rest Breaks in Call Centres David Caple, David Caple & Associates Pty Ltd Melbourne, Australia Keywords: Call centres, rest breaks, RSI, VDU work. ABSTRACT During the 1980s, formal rest breaks were introduced into injury prevention strategies for RSI in a number of Australian organisations. Since that time, computer work has evolved and call centre activity has increased across Australia. Call centre work provides a broad range of job design and application areas using the head set and computer technologies together. This study has reviewed the task analysis in 3 different call centre applications and compared the ergonomic factors with the research in relation to rest breaks. Specifically, the research has focussed on the visual, cognitive and musculo skeletal demands on the operators to determine the justification for continuing formal rest breaks in the call centres under review. It was found that the discontinuance of formal rest breaks could be justified in those calls centres providing greater flexibility in the workload demands and informal break opportunities for the operators. 1. INTRODUCTION Call centres have grown in their size and variety since the 1980s with a common feature of an operator using a telephone head set whilst interfacing with a computer terminal. Extensive research has been published in relation to the incidents of RSI claims amongst call centre operators, both in Australia and internationally since the 1980s. As part of Industrial Relation agreements during this period, the introduction of formalised rest breaks every hour were agreed between some employers and their unions. These breaks were in addition to operators’ normal tea and lunch breaks during a shift. This entitlement has continued to occur within a number of industrial agreements in 2001. Since the 1980s, a wide variety of call centre applications have been introduced without any industrial agreement for compulsory additional rest breaks. For the purposes of this study, a product information/sales call centre was used as a control work site as it did not have compulsory additional rest breaks. The two assessment sites were call centres that were taking compulsory 10 minute breaks. These centres involved a customer information centre with a high volume of short duration calls and a faults processing centre, involving problem solving activities between the operator and the client. All these call centres were operated by the same management and the operators were assessed using similar key performance indicators. This study was a review of the task demands within the call centres and literature review to ascertain the relationship between the task design and the recommendations for compulsory rest breaks. 91 Better Integration 27-30 November 2001 2. OBJECTIVES 1. To conduct an ergonomics task analysis for each of 3 call centres and to identify the work practices and risk factors associated with the potential for work related injuries. 2. To determine the appropriateness for continuing formal rest breaks in each of the call centre environments. 3. METHODOLOGY 3.1 Task Analysis Within three different call centres, individual task analysis were documented in consultation with a cross section of operators. These call centres were :3.1.1 Sales/Product Information 3.1.2 Customer Information 3.1.3 Faults Processing 3.2 Key Performance Indicators For each of the three types of call centres, details of the key performance indicators used by management to assess the quality and productivity of the operators were obtained and compared. All three call centres were operated by the same company and were primarily assessed using the same KPIs. 3.3 Posture and Movement Analysis A range of photographs and video were taken of the operators whilst they performed their call centre duties. This enabled comparison of the static postures and the dynamic movements involved in performing their call centre activities. Operators were randomly selected to illustrate the variety of working postures. 3.4 Task Analysis 3.4.1 Primary task demands. It was evident in all applications that the primary input demands on the operator were (a) Visual – the operators in Customer Information and Sales call centres, would be watching their computer monitor virtually constantly throughout the interactions. The exception would be when they were awaiting the next call or were waiting for the client to find additional information, when they would look away from the screen. This ability to frequently look away from the screen was more common in the faults/problem solving call centres. (b) Auditory input – in all instances, the operators wore a headset and were receiving input from their client via the headset using their auditory processing system. The operator would then speak through the headset to their client to clarify details as they interfaced with the computer software. 92 37th Annual Conference Ergonomics Society of Australia Inc. 3.4.2 Secondary demands (a) Keyboard location. With each of the applications assessed, the technical staff reported a significant reduction in required keyboard input or mouse work due to the advances in software design. As a result, the Customer Information operators would use less than 10 keystrokes per call i.e. between 1,000-2,000 keystrokes per hour. This was compared with data entry operators averaging 10,000-13,000 keystrokes per hour assumed in much of the musculo-skeletal research projects (Oxenburgh et al, 1985; Kamwendo et al 1991) Hence, call centre operators , covered in this study, could not be classified as data entry staff in terms of their keyboard entry demands. (b) Mouse location. It was found that the operators did not use the mouse for any significant part of their call centre activities as the majority of interface was conducted through the keyboard. 3.4.3 Telephone location The Customer Information applications required the calls automatically drop into the headset of the operator. Hence, there is little tactile contact with the telephone handset. However for Faults and Sales, the operator could accept the next call, place it on hold, and transfer it as required. 3.4.4 Pen and Paper Sales and Faults operators utilised a note pad to record information which will be required by them to process the call. This avoids committing such data to memory. The location of the pen and paper was found to be in front of the operator with their keyboard pushed back towards the monitor. 3.5 Task Profile The duration of the calls vary significantly depending on the type of call centre. Customer Information. The average duration of the call is 15-20 seconds. With the introduction of new technologies, there has been a progressive reduction in the time take by the operator interacting directly with the customer. 3.5.2 Sales and Faults. For both these call centre applications, the durations of the call vary significantly, depending on the nature of the enquiry. The calls range from 4-9 minutes. For Faults, up to 50% of this time could be taken by the customer in finding information requested by the call centre operator. At the end of each Sales or Faults call, the operator has an allocation of time for finalising the service required by the customer. This enables them some discretionary time to complete any paper work or contact any third parties to process the implementation of necessary actions. 3.6 Working Postures A range of working postures was seen amongst the operators who were provided with fully height adjustable work tops and seating. It was found that the operators, who “hot desk” do adjust the height of their workstation generally to locate the computer monitor into the preferred visual angle position. It was noted that many of the operators had adjusted the monitor so that the centre of the screen was at approximately eye height. This is in contravention to the ergonomic recommendation, with the top of the monitor at eye height to 93 Better Integration 27-30 November 2001 facilitate the reduction of static posture with the neck. The posture analysis indicated that the operators preferred to sit back in their chair and look slightly up at the screen, rather than to sit in a vertical posture and look in a horizontal and slightly downward direction. It was also noted that the operators do communicate with each other and that the preferred seated posture facilitated eye contact and conversation between the operators at adjacent workstations. 3.7 Stressors Within Job Design 3.7.1 It was noted in the Customer Information call centres that operators reported angry and stressful comments from their customers. This generally related to their perceived service from the call centre company and the products being marketed. Further, restructuring of the call centre management and staff, including the introduction of outsourced and casual labour, was an additional element of stress for the permanent call centre operators. 3.7.2 In contrast the Sales and Fault processing operators appeared to have a more relaxed communication with their customers as they explored the relevant issues to be resolved. The stressors associated with these tasks tended to result from call back from disgruntled customers who had not received the services that they had previously been promised by the provider. 4. DISCUSSION 1. This project has identified that there is a range of job design parameters covered by the generic title of “call centre operators”. It appears that those call centres which have highly repetitious calls which automatically drop into the headset of the operator for which they have limited control continue to provide the greatest level of stress and potential for musculoskeletal discomfort. As a consequence, it would still be recommended that a program of scheduled breaks would be maintained to provide the opportunity for the operators to move away from the auditory input and the information processing demands of the cognitive tasks being performed. It is also evident in these call centres that the operators have minimal ranges of postural variation due to the constant visual demands in retrieving information from the computer monitor. It is noted that the primary justification for these breaks are not related to data entry on the keyboard or mouse, but are primarily related to the cognitive demands of the task as well as the visual demands of viewing the computer screen and the associated static postures. 2. In contrast to the highly repetitious and cognitive demanding calls of Customer Information call centres, the Sales and Faults service call centres have longer duration calls with a higher level of informal interaction between the operator and the customer. There is flexibility in how the operator is dependent on the customer to provide them with information and to find details to enable processing of their calls. There is also flexibility at the end of each call when the operator is off line and completes the necessary paperwork and follow-up activities. It was found that operators may take a brief break, such as visiting the toilet, or making a coffee at the completion of a long call during this follow-up period before taking their next call. The passive and active exercise taken during these breaks provide additional benefits (Thompson, 1990). 94 37th Annual Conference Ergonomics Society of Australia Inc. This work practice was part of a regime of informal breaks which were separate from the formalised tea and lunch breaks. Rest breaks with short duration, are consistent with Sauter and Swanston (1992) recommendations for mini breaks (3 minutes) and micro-breaks (30 seconds) throughout the work period. 3. The key performance indicators relating to call centres, primarily focus on the adherence time, where the operators are monitored that they are on the telephones processing the calls waiting in the queues. It was found that the different types of call centres were able to achieve over 90% of adherence time both with the formal rest breaks and also the informal rest breaks such as in the Sales function. 4. Where the system of work is regimented and repetitive, formal rest breaks in the call centre have the advantage from the organisational perspective that monitoring of call centre traffic can be scheduled knowing the exact number of operators who should be available to process the calls in any call centre across the network. If unstructured breaks were to be available to the staff, then a lack of accuracy in the prediction of available operators to process calls would then effect the performance indicators in monitoring traffic flows from a management perspective. Hence, there are organisational reasons why the maintenance of formalised rest breaks are seen as an advantage to the management of call centres regardless of the health and safety implications to the operators. 5. The stressors associated with work processes undergoing change, and those applications where operators are working on paced systems of work, or subjected to abuse from customers on a frequent basis, have a justifiable reason for taking regular breaks away from their system of work. In contrast, where there is more autonomy and control over the calls, such as in the Sales and Faults processing without the same predictable levels of stress, then there are different assumptions associated with requirements for rest breaks. 5. CONCLUSION It could be concluded from this study that the cognitive information processing tasks, together with the visual demands in highly repetitive call centre activities, particularly those involving aggressive and frequent abuse from customers, would justify the maintenance of formal rest breaks. However, it could be concluded that the flexibility of less formal breaks within the Faults and Sales reporting areas could be adopted. These provide the operators with greater flexibility in taking short, frequent breaks such as micro and mini breaks as outlined in the literature after the completion of prolonged calls. The operators would also be entitled to the formal morning and afternoon tea breaks, as well as their lunch. As long as the central control of traffic monitoring of the calls into the centres can be managed, greater flexibility in rest breaks should be provided for the operators to suit their individual needs. 95 Better Integration 27-30 November 2001 6. REFERENCES Kamwendo K, Linton S. and Moritz U, 1991, Neck and shoulder disorders in medical secretaries Part 11. Ergonomical work environment and symptom profile. Scandinavian Journal of Rehabilitation Medicine, 23, 135-142. Oxenburgh M, Rowe S. and Douglas D, 1985, Repetitive strain injury in keyboard operators. Successful management over a two year period. The Journal of Occupational Health and Safety – Australia and New Zealand, 1 (2): 106-112. Sauter S.L. and Swanston N.G, 1992, The effects of frequent rest breaks on performance and well-being in repetitive computer work., Paper presented at Work with Display Units ’92, Berlin, September. 96 37th Annual Conference Ergonomics Society of Australia Inc. The Role Of Legislation To Impact Proactive Ergonomics Programs David Caple, David Caple & Associates Pty Ltd Melbourne, Australia Keywords: OH & S legislation, MSD, manual handling, ergonomics ABSTRACT Governments around Australia, and internationally, have been introducing legislation to address ergonomics issues in the workplace, specifically manual handling, over the last 15 years. A review of evaluative studies has verified the role and effect of legislation to bring about proactive improvements in workplace injury reduction. The PREMUS conference in Amsterdam, October 2001 provides an opportunity for international researchers to review the outcomes of studies relating to the role of legislation to address MSD risks in industry. These sessions will incorporate their findings into these evaluations. It is evident that proactive programs are initiated by a range of factors such as workers compensation costs; quality assurance programs; corporate initiatives in large companies; capital investments to address productivity and quality problems. A revision of Australia’s National Standard for Manual Handling is required to address the body of prevention research conducted since 1990. 1. INTRODUCTION The majority of Western Governments have OH & S legislation which places the responsibility for injury prevention upon the employer within specified workplaces. Breaches of the general duty to provide “a safe place of work” can result in prosecution and fines against the companies. To provide more specific responsibilities on hazards known to be a major source for workers compensation claims, governments have introduced regulations, rules, ordinances, and other legislative instruments to provide specific responsibilities on the prevention of these workplace hazards. In Victoria, there are 3.5 million residents over 15 years of age. Approximately 31,500 workers compensation claims were made in 1999/2000 of which 17,700 (56%) were for musculoskeletal disorders (Victorian WorkCover Authority, 2001). The direct cost for all injuries was $1,100M for 1999/2000. This included $700M (54%) for the musculoskeletal claims. Prior to 1988, the Victorian laws provided a prescriptive limit of 16kg prohibiting all women or men under the age of 18 to be requested to handle such objects by their employer. It was also the responsibility that workers performing manual labour, be trained on the principles of safe lifting techniques. In 1988, the Victorian State Government, and subsequently the Australian Government in 1990, adopted a performance based approach to the prevention of sprain and strain injuries. This was primarily modelled on the Nordic ordinance of that time. This approach required the employer to :97 Better Integration 27-30 November 2001 a) Identify those tasks involving manual handling with the potential of back injury to the workers b) For those tasks identified, to conduct a risk assessment based on a series of descriptive risk factors derived from research that were relating to musculoskeletal disorders c) To implement risk control strategies relating to eliminating the hazard or reducing the risk through the use of engineering changes to the workplace If these were not practical, they were then required, to implement administrative controls relating to the organisation of work duties to minimise the exposure on individual workers. Further, they were required to provide appropriate training for workers performing the manual tasks based on the competencies required in using the risk control strategies. This process or performance based model, has remained the generic approach in legislation since that time and has been adopted in a wide range of countries as the primary strategy of Governments to approach injury prevention of sprain and strain injuries. Subsequent guidance was introduced to cover upper limb disorders or overuse injuries beyond the initial approach on back injuries. During 2000, the Washington State Government introduced their Ergonomics Rule and the USA Congress proclaimed, and subsequently repealed, their Ergonomics Standard. The role of Government to determine legal obligations for employers to accept responsibility for preventing musculoskeletal disorders remains a current and contentious issue. 2. METHODOLOGY 1. The awareness of MSD prevention legislation amongst employers in Australia was initially determined by a telephone survey of 2,000 workplaces stratified for industry type and size. 2. A study of 50 case studies was conducted to determine what employers had undertaken for legislative compliance. 3. A comparative analysis was undertaken with the Washington State legislation in reviewing an equivalent case study analysis. 3. RESULTS The awareness of the Australian Manual Handling Standard, Regulations and Codes of Practice was conducted in 1996 and reported at ESA 1999 (Caple, et al, 1999). This study found that:Less than 23% of the small employers were aware of the existence of the performance based regulations or demonstrated any understanding of the processes that were necessary for compliance. Similarly, approximately 43% of medium sized employers were aware of the regulations and the conformance requirements. Although over 80% of the larger employers appeared to be aware of the regulations and the conformance requirements, it was found that they had actually implemented 98 37th Annual Conference Ergonomics Society of Australia Inc. less than 50% of the risk control recommendations arising from the risk assessment processes which had been undertaken. Of those controls which had been undertaken, nearly 60% would have been classified as the “quick fix” or short term control strategies. Whilst the general principles behind the performance based requirement of the regulations were understood, the employers and workers frequently requested specific guidance on each of the risk factors. The particular risk factors associated with upper limb musculoskeletal disorders were found to be inadequately covered in the initial regulations that were primarily focussed on the prevention of back injuries. The review of 50 case studies relating to implementation of Manual Handling Regulations indicated that:Interventions were observed in a wide cross section of industry sectors and sizes of workplaces. Risk assessment consultative teams were formed in all of the large workplaces (over 100 employees) to conduct the assessments. The majority of assessments were conducted within 2 years of the release of the regulation; on incident involving injury or a visit by Government Inspector. Justification for capital expenditure, deemed significant by the workplace, was more likely to reflect anticipated quality and/or productivity improvements rather than just to reduce injury risks. The multi-factorial nature to risk assessment was seen to be too complex and vague to assist workers in the teams. Simple local checklists were frequently observed. The comparison between the Australian National Standard for Manual Handling (1990) and the Washington State Ergonomics Rule (2000) indicates that the limited scope and technical assistance to risk assessment teams of the Australian Standard make it of narrow use in addressing MSD risks. 4. DISCUSSION In the early 1990’s Australia was seen as a leading country in legislative reform to address MSD risks in industry. Whilst individual States have continued to develop more comprehensive legislation, the National Standard has not been reformed (Victoria, 1999, Queensland, 2000). The research community involved in MSD have developed a position on key risk factors including quantitative recommendations on biomechanical risk factors, (PREMUS, 2001 proceedings). In the USA, a “Threshold Limited” option has been drafted for Upper Limb risk factors. In Europe, the EU has also developed a position on MSD risk factors during their consultative forums. The Australian workplaces covered during these studies indicate that, with a simple risk assessment model, they are capable of understanding and implementing an MSD injury prevention program. Quantitative data from the case studies indicate that reductions in injury severity have been reported, with associated reductions in workers compensation costs. However, for sustained performance, it is evident that additional issues are required. These include:99 Better Integration 27-30 November 2001 (a) leadership and commitment from senior management (b) theoretical understanding of biomechanical risk factors (c) incorporation of work organisational risk factors with the biomechanical factors as equally relevant (d) risk controls integrated into continuous improvement programs 5. CONCLUSION It is evident that Australian workplaces are capable of effective implementation of MSD risk control programs. The models outlined in legislation vary between jurisdictions. The primary focus of risk factors relates to biomechanical factors derived from research however, the National Standard for Manual Handling does not reflect contemporary findings. The injury prevention approach covered by the legislation is limited by the employer accountabilities outlined in OH & S Law. Hence, the full spectrum of psychological or work organisational factors have been limited in Regulations by the scope of the OH & S Laws. It is timely for the National Standard for Manual Handling to be comprehensively revised and the comprehensive approach incorporate all the risk factors found in ergonomics research and not just the biomechanical issues. 6. REFERENCES Caple, D.C. et al, 1999, Evaluation of Manual Handling legislation, 35th Annual conference of the Ergonomics Society of Australia. Division of Workplace Health & Safety, 2000, Manual Tasks Advisory Standard, Queensland, Australia. Victorian WorkCover Authority, 1999, Manual Handling Regulation, Melbourne, Australia. Washington State Department of Labour, 2000, Ergonomics Rule, Washington State, USA. Worksafe Australia, 1990, National Standard for Manual Handling, National Occupational Health & Safety Commission, Canberra, Australia. 100 37th Annual Conference Ergonomics Society of Australia Inc. Forearm Support and Computer Keyboard Use. Catherine Cook School of Exercise and Health Sciences, University of Western Sydney Robin Burgess-Limerick School of Human Movement Studies, The University of Queensland. Keywords : Musculoskeletal symptoms, computer keyboard, forearm support ABSTRACT Forearm support during keyboard use has been reported to reduce neck and shoulder muscle activity and discomfort. However, the effect of forearm support on wrist posture has not been examined. The aim of this study was to determine the effect of forearm support on posture, muscle activity and discomfort of the forearm/hand and neck/shoulder during keyboard use. In a laboratory study of 13 subjects, forearm support resulted in significantly less ulnar deviation, more time spent in a neutral wrist posture and less reports of discomfort than the traditional “floating” posture. The findings for the neck and shoulder were consistent with previous findings. These positive findings indicate that forearm support may be preferable to the traditional “floating” posture adopted by keyboard users. 1. INTRODUCTION The relationship between computer use and musculoskeletal disorders of the neck and upper extremity has been well documented, with the prevalence of musculoskeletal symptoms among keyboard users reported to be as high as 76% (Aaras, Fostervold, Ro, Thoresen, & Larsen, 1997). Many risk factors have been associated with computer use. These include physical ergonomic factors, working postures, (Grandjean et al., 1984; Aaras et al., 1997), the use of input devices such as the computer mouse (Cook, Burgess-Limerick, & Chang, 2000; Burgess-Limerick et al., 1999) organisational factors such as the duration of computer use per day and psychosocial factors such as stress (Smith & Carayon, 1996). Symptoms of the neck, proximal and distal upper extremities have been associated with keyboard use. The continuous activation of muscles of the arms, shoulder girdle, neck and trunk during keyboard use has been proposed as one of the causal factors of neck and shoulder and arm hand diagnoses (Bergqvist, Wolgast, Nilsson, & Voss, 1995). Despite this, the traditional recommendation for typists to ‘hover or float’ over the keyboard whilst keying, maintaining a neutral wrist posture without supporting the arms is still advocated (OSHA, 2001). Upper extremity support has been reported to reduce muscular load in work tasks and has been proposed as a way of reducing static shoulder and neck muscle load during keyboard use (Aaras et al., 1998; Aaras, Ro, & Horgen, 2000). Aaras et al, (1998) reported a significant decrease in static trapezius load, neck and shoulder pain in a group of participants who were able to support their whole forearm and hand on the table top. No change was found for forearm or hand pain. While these results suggest that forearm support may be beneficial for 101 Better Integration 27-30 November 2001 the proximal upper extremity and neck, the effect of forearm support on wrist posture during keyboard use was not reported. An alternate means of supporting the arm is to support the wrists by the work surface, or by wrist or palm rests. Some authors report that the use of wrist rests reduced wrist flexion/extension resulting in more neutral wrist postures (Albin, 1997), while others report that the use of wrist support (desktop or when a wrist rest is used) resulted in an increase intracarpal tunnel pressure (Horie, Hargens, & Rempel, 1993), which is considered a risk factor for wrist disorders. Supporting the forearm on the work surface may increase comfort and decrease muscular load of the neck and shoulders. However, the effect of forearm support on wrist postures has not been examined. The aim of this research is to determine the effect of arm support on posture and muscle activity of the forearm/hand and neck/shoulder during keyboard use. 2. METHODS 2.1 Participants Thirteen volunteers (10 F, 3 M; median age 24 years) participated in this laboratory based, experimental design study. Participants completed a 20 minute copy typing task in each of 3 conditions: a) forearms fully supported on worksurface; b) wrists supported on worksurface; c) no arm support (‘floating’ posture). An adjustable desk and chair and a conventional keyboard were used during the study. 2.2 Data Collection The Peak Motion analysis system was used to record bilateral wrist, shoulder and elbow extension/ flexion and wrist ulnar/radial deviation using three video cameras (overhead, left and right lateral). Electromyographic (EMG) activity of the extensor digitorum communis, extensor carpi ulnaris, upper trapezius and anterior deltoid was recorded bilaterally via a FlexComp/DSP system (Thought Technology Ltd, Montreal). Participants were asked to report the location of discomfort using a Body Map and severity scale prior to task commencement and at 5 minute intervals during each position (Corlett & Bishop, 1976). 2.3 Data analysis Maximum and mean angles were calculated for each participant for each trial for each angle. The percentage of time spent in extreme angles i.e. more than 15 degrees ulnar deviation was determined for each test position. One way Analysis of Variance was used to assess the probability of obtaining effects of the observed magnitude given a null hypothesis of zero effect. Mean RMS values were calculated for each posture for each participant. Repeated measures ANOVA was applied to mean EMG values for each task. Chi square was used to determine differences in proportions of reported discomfort for each work position. 102 37th Annual Conference Ergonomics Society of Australia Inc. 3. RESULTS 3.1 Postural analysis Forearm support resulted in significantly greater shoulder flexion and elbow extension bilaterally due to the placement of the keyboard at a greater distance from the edge of the worksurface (Table 1). Use of the wrist rest was associated with a typical increase in wrist extension of between 6 and 9 degrees over the forearm support and floating conditions. Forearm support resulted in a lower mean ulnar deviation than either the wrist support or floating positions for both the left and right hands. The use of forearm support resulted in significantly less time in an extreme ulnar posture of >15degrees for the right hand than either the wrist support or the floating positions. Similar results were found for the left hand, with forearm support resulting in less mean ulnar deviation than the wrist or floating positions. The proportion of time spent in extreme ulnar deviation of the left hand was also significantly less for the forearm support position than either the wrist support or the floating positions. Table 1: Summary statistics of angles from lateral and overhead cameras. Posture Right wrist extension Left wrist extension Right ulnar deviation Left ulnar deviation Right shoulder flexion Left shoulder flexion Right elbow extension Left elbow extension Forearm Mean(SD) -1.4(5.8) -0.7(9) 14.8(5.6) 13.6(5.3) 17.9(5.9) 17.2(7.8) 77.8(7.6) 79.9(7.9) Wrist Mean(SD) 4.1(5.7) 4.2(10.6) 17.6(6.7) 17.6(4.7) 5.8(8.6) 3.5(9.4) 84.6(12.7) 85.8(13.8) Floating Mean(SD) -2.5 (5.4) -5.3(10.6) 18.1(5.3) 16.3(5.9) 4.8(9.6) 4.6(9.4) 87.7(14.9) 92.9(12.1) F 6.1 38.6 5.2 11.8 39.5 32.5 6.9 18.3 p 0.008 <0.001 0.014 <0.001 <0.001 <0.001 0.005 <0.001 3.2 Muscular activity The wrist support position resulted in significantly less muscular activity in the trapezius and the anterior deltoid bilaterally. Both the forearm and wrist support positions resulted in significantly lower right trapezius muscle activity than the floating position (Figure 1). There were no significant differences or consistent patterns for extensor digitorum or extensor carpi ulnaris. 103 Better Integration 27-30 November 2001 50 40 Forearm Wrist Floating 30 % RVC 20 10 0 R Trap L Trap R Delt L Delt Muscle Figure 1: Mean group RMS (% reference voluntary contractions) for the neck and shoulder muscles. 3.3 Discomfort All participants reported discomfort in one or more body parts during the experiment. Significantly more participants (p=0.002) reported discomfort in the floating position than the wrist support position or the forearm support position. The frequency and severity of discomfort was lowest for the forearm position. These reports were consistent with the postural and EMG data. 4. DISCUSSION The results of decreased neck and shoulder muscle activity and decreased discomfort with forearm support the findings of Aaras et al, (1998). In this study, forearm support was found to lead to a reduction in extreme ulnar deviation. Reports of discomfort were highest for the floating position. The reports of discomfort in the neck and back are consistent with previous literature which reports an association between lack of forearm support and shoulder and arm hand diagnoses (Bergqvist et al., 1995). Although a number of participants reported that the forearm support position felt 'different' on commencement of the task, the overall frequency of discomfort reports for this posture was lowest. Forearm support also resulted in significantly less ulnar deviation, and significantly less time spent in extreme ulnar deviation during keyboard use. This decrease in ulnar deviation appears be a consequence of a combination of factors. Shoulder flexion increases when the forearms are supported and the hands are further away from the body. In the wrist support or floating positions, the arms appeared to be more constrained by the proximity of the arms to the body, resulting in more ulnar deviation. When the forearms were supported, the forearms 104 37th Annual Conference Ergonomics Society of Australia Inc. were observed to pivot on the worksurface, rather than deviating the hand to reach the keys. This influence of forearm support on ulnar deviation has not previously been reported. Deviated wrist postures have been demonstrated to increase carpal tunnel pressure (Weiss, Gordon, Bloom, So, & Rempel, 1995) with the lowest pressures recorded when the wrist is ulnarly deviated in the range of 10 to 15 degrees. In the current study, forearm support resulted in mean deviation within the extreme range for a little less than half the study time for the right hand, whereas the other positions resulted in two thirds to three quarters to of the time spent in the extreme range. The conclusions are restricted to the conventional keyboard which is still very much the predominant keyboard in use at present. While alternate keyboard designs may reduce ulnar deviation, the current evidence is not clear. 5. CONCLUSIONS The results of this study indicate that typing with forearm support may be preferable to the traditional floating posture due to a reduction in upper extremity load, a decrease in discomfort and a reduction in extreme wrist postures. Guidelines for keyboard workstations should recommend forearm support during keyboard use rather than a floating posture. 7. REFERENCES Aaras, A., Fostervold, K., Ro, O., Thoresen, M., & Larsen, S. ,1997,. Postural load during VDU work: a comparison between various work postures. Ergonomics, 40(11), 1255-1268. Aaras, A., Horgen, G., Bjorset, H.-H., Ro, O., & Thoresen, M. ,1998,. Musculoskeletal, visual and psychosocial stress in VDU operators before and after multidisciplinary ergonomic interventions. Applied Ergonomics, 29(5), 335-360. Aaras, A., Ro, O., & Horgen, G. ,2000,. Supporting the forearms in a neutral position when doing VDU work. Primary prevention of musculoskeletal pain. Paper presented at the IEA 2000/HFES 2000 Congress, San Diego. Albin, T. ,1997,. Effect of wrist rest use and keyboard tilt on wrist angle while keying. Paper presented at the 13th Triennial conference of the International Ergonomics Association. Bergqvist, U., Wolgast, E., Nilsson, B., & Voss, M. ,1995,. Musculoskeletal disorders among visual display terminal workers: individual, ergonomic and work organisational factors. Ergonomics, 38(4), 763-776. Burgess-Limerick, R., Shemmell, J., Scadden, R., & Plooy, A. ,1999.. Wrist position during pointing device use. Clinical Biomechanics, 14, 280-286. Cook, C., Burgess-Limerick, R., & Chang, S. ,2000,. The prevalence of neck and upper extremity musculoskeletal symptoms in computer mouse users. International Journal of Industrial Ergonomics, 26(3), 347-356. 105 Better Integration 27-30 November 2001 Corlett, E. N., & Bishop, R. P., 1976, A Technique for assessing postural discomfort. Ergonomics, 19(2), 175-182. Grandjean, E., Hunting, W., & Nishiyama, K, 1984, Preferred VDT workstation settings, body posture and physical impairments. Applied Ergonomics, 15(2), 99-104. Horie, S., Hargens, A., & Rempel, D, 1993, The effect of keyboard wrist rest in preventing carpal tunnel syndrome. Paper presented at the Proceedings of American Public Health Association Annual meeting, San Francisco. OSHA, 2001, Keyboard workstation setup, [website]. Available: www.osha [2001, May]. Smith, M., & Carayon, P, 1996, Work organisation, stress and cumulative trauma disorders. In S. D. Moon & S. L. Sauter (Eds.), Beyond biomechanics. Psychological aspects of musculoskeletal disorders in office work. (pp. 23-42). (London: Taylor & Francis). Weiss, N. D., Gordon, L., Bloom, T., So, Y., & Rempel, D, 1995, Position of the wrist associated with the lowest carpal tunnel pressure: Implications for splint design. The Journal of Bone and Joint Surgery, 77A(11), 1695-1699. 106 37th Annual Conference Ergonomics Society of Australia Inc. Ergonomic Improvements Increase Productivity in a Heavy Engineering Workplace Roger Fairfax WorkCover NSW Keywords: Audit, safe work procedures, ergonomics, continuous improvement ABSTRACT A heavy engineering company servicing railway stock including City Rail trains and freight rolling stock sought help to improve occupational health and safety. They were a newly formed company with little knowledge of safety and ergonomics. The consulting group chosen conducted a workplace OHS audit that highlighted more than 300 discrepancies where improvements were needed. Some of these were ergonomic improvements. The company took the report seriously and contracted one of the consultants to provide guidance with ergonomic and OHS improvements. Within eight months the company had corrected all but a few that were high cost items that needed capital approval and were awaiting budget approval. A number of antiquated work practices were carefully examined. Over time major ergonomic improvements emerged with introduction of roll-over work stands. The first one of these was developed and built in house. It housed the large bogie frames and changed the welding repair procedures to such an extent that in its first year of operation it more than paid for itself in the first few months of operation. The company saw the benefits of this and justified the building of large roll over stands for a number of tasks. Some previous tasks had been performed with brute strength and crowbars. This paper indicates these and other related improvements increased productivity through a continuous improvement approach. 1. INTRODUCTION 1.1 Commitment to Occupational Health, Safety and Injury Management The company referred to in this paper is known as Maintrain. They took over the servicing of State Rail’s trains and freight bogie equipment at the Clyde workshops in 1993 when private industry tendered for this work. They elected to operate a teams based approach. Initially there were 17 teams. There are now 18. Most employees had limited experience in working on rolling stock and this presented a huge challenge. In their first year of operations lost time injuries were high for the employees. In late 1994 Maintrain asked WorkCover Techsource to conduct a workplace OH&S and ergonomic audit. Over 300 discrepancies were noted in the audit report. The company quickly 107 Better Integration 27-30 November 2001 addressed every discrepancy. They then asked one of the Techsource consultants to do an ergonomic assessment of the freight wheel line. This then led to development of numerous safe work procedures (SWPs), a noise management programme, various ergonomic assessments and general OH&S activities by the consultant over a five year period on an average of one day a fortnight. The company paid for this service. A consultant from Technical and Further Education (TAFE) also worked with the company’s training manager on skills development of individual employees. Nearly 80% responded to the challenge and attended TAFE courses that were selected with guidance from the TAFE consultant to help improve the skills of each participant. Employee skills were recognized which provided them with a wider scope of work and increased their earning potential. The company also dedicates a half an hour each week for each team to actively discuss ways to improve OH&S and production within their work environment. Teams are encouraged to introduce safety improvements that they can initiate. They minute their weekly meetings. Some OHS issues are referred to the OHS Committee and when needing management approval they are referred to the company’s weekly Steering Committee chaired by the General Manager and attended by OHS Chairperson, Union Delegates and operations Managers. Teams are encouraged through their direct involvement to improve their work processes and environment. Other initiatives in addition to SWPs are major ergonomic improvements and injury management improvements, introduction of regular workplace inspections, manual handling training called “No Strain No Pain” and introduction of an OHS representative within each team. The company pays particular attention in managing OHS&IM integrally with every other aspect of the company’s operation providing a continuous improvement approach and gaining long-term savings with improved productivity and lower workers compensation costs. In 1998 WorkCover closed its Techsource consulting service. 2. EXAMPLES OF IMPROVEMENTS 2.1 Development of Safe Work Procedures (SWPs) One of the WorkCover auditors whom from here on is referred to as the OHS consultant was asked to provide an ergonomic assessment of the Freight Wheel Line where manual handling injuries were high. He worked in close liaison with the team leader and members responsible for this process and his report highlighted areas where significant improvements in manual handling could be made. This led to development of SWPs for that and other work processes. To ensure continuity in the development of SWPs the company’s Organisational Development Manager provided a checklist of parameters. It was agreed that the OHS consultant would provide the OH&S and ergonomic expertise to this program working directly with the team members and liaising regularly with management. The company was mindful that “among all waste that organizations generate, the greatest are the wastes of intellect, the waste of abilities and the waste of unrealised potential for participants to find satisfaction and productive lives” (p7, Scott and Harker, 1998). As various SWPs developed the particular team leader responsible assigned two team members to work with the OHS consultant. Every aspect of the job being performed was considered and the 108 37th Annual Conference Ergonomics Society of Australia Inc. team member’s words were written on a white board and became the foundation for the SWP. Reference was made to the SWPs checklist when needed. Regular workshop visits to view the work task ensured specific points were captured in the SWP. They were written in plain English, typed and given a reference number and then checked by the team who performs that specific work task. Corrections were made as agreed. SWPs were kept specific to the task. Technical and environmental comments for each specific SWP was provided by company engineers and the environmental officer. All SWP comments were referenced to their specific job instruction. Photographs and sketches were used to explain particular points of reference. Comments specific to manual handling and ergonomics were written into each SWP. The continuous improvement approach in production and OH&S by teams brought about changes to work processes and the subsequent re-writing of the specific SWP including engineering and environmental approval and recording of changes introduced. Generic SWPs were developed for general work tasks such as hand grinding, welding, use of pneumatic tools etc. that are used throughout all workshops. Generic SWPs were referenced where necessary in specific SWPs. All team members whether involved or not in the development of an SWP were given training with the task that a SWP covers. Training is then signed off. 2.2 Ergonomics Improvements The WorkCover Workplace audit of 1994 found some bogie repair work activities were performed with antiquated equipment. Crowbars were being used to manipulate heavy bogie parts into position for hand grinding and weld repairs. In one location team members were sitting, squatting or lying on the floor on mats to perform welding tasks to bogie frames. Suggestions were made that rollover fixtures might be introduced to improve ergonomics of tasks and eliminate some of these antiquated practices. The company took their responsibility seriously and seeking some guidance from the OHS consultant, they developed over a period of time rollover work stands for many varied operations. Bogie welding improvements One roll-over stand built by and later improved by team members allowed a CityRail bogie frame measuring roughly 2.3 metres wide by 3 metres long by 0.6 metres deep and weighing nearly 5 tons to be held on its side and rolled in the stand. Team members performing welding operations were then able to weld in a standing position. The result in productivity was dramatic. Welders were no longer getting back pains and burns, there were virtually no reject welds and the process was sped up nearly five fold. The rollover stand was built mainly from unused equipment within the workshop with some items purchased and initially cost about $15,000. It has been upgraded and continuously improved. A cost analysis of the work output improvements created by use of this fixture revealed that it saved the company over $100,000 in its first year of operations taking into consideration the faster turn around time and virtual elimination of weld rejections. Reduction of injuries and associated costs are not included in the above figure. Bogie pre-stripping improvements CityRail bogies were pre-stripped on a raised rail about 15 metres long and 1 metre above the floor. The logistics of getting from one side of this rail to the other, access to compressed air outlets located inside the structure and difficulty retrieving bogie items that dropped into the raised structure was identified by team members as a huge manual handling problem. The team 109 Better Integration 27-30 November 2001 performing this job initiated improvements. With engineering approval they had the raised rail cut into two smaller sections, raised for easier access to bogie parts during disassembly and the two raised rails placed side by side and parallel to each other. The ends of each structure were left open with pneumatic services and lighting contained inside the structure. These modifications reduced manual handling risks and sped up the stripping process. Adjustable height trolleys were introduced to slide large springs and brake gear parts onto during disassembly. Tangara brake disc pin removal and replacement Another example was the development of a hydraulic pusher puller for removal and replacement of Tangara brake disc pins. Initially the complaint received by the OHS consultant was of a sore shoulder by a team member from an estimated 700 to 800 hammer blows per shift when removing steel pins about 3cm diameter. Team members and the OHS Consultant discussed ideas for a hydraulic pusher /puller tool for removing and inserting these pins. The tool was then manufactured in the company’s machine shop. It eliminated the use of a hammer altogether and eliminated high noise levels (about 120dB linear) and sped the process up nearly fourfold. The team responsible for this modification in early 1999 had processed their 100th productivity improvement from ideas emanating from within the team. Freight wheel line The freight wheel line section of the workshop has been virtually re-designed to improve ergonomics. Heavy manual handling tasks have been eliminated and dangerous cross-over points that could cause serious injury have been removed which has lead to increased production with less manual effort. Over five years this area has undergone many changes, each one improving productivity and reducing manual effort. Before any improvements, the area where axle boxes were removed from freight wheel axles assemblies had a number of manual handling injuries. To remove the axle boxes containing wheel bearings a large hydraulic puller mounted on a carriage guided on rails was manually pushed into position and the puller lowered over the axle box before being energized hydraulically. Dirty grease that oozed out of the axle box being removed would sometimes spill onto the steel tread plate floor. A floor grit like kitty litter was spread around to try and reduce slipping on the greasy floor. This grit jammed the wheels of the bearing puller carriage being pushed or pulled along the guide rails causing it to be difficult to move. The team along with the OHS consultant changed the work process that eliminated grease spills and the hydraulic puller carriage was removed and the puller suspended from a jib crane. All pushing and pulling was therefore eliminated along with manual handling injuries. Further productivity improvements in this area have since been implemented to allow removal of axle boxes from each side of the axle simultaneously and eliminate mechanical rotation the wheel assembly on the wheel line. This reduced maintenance costs. Bogie wheel jig The method of re-wheeling a CityRail ‘J’ type bogie frame took five people. Four positioned the large coil spring assemblies while the fifth person carefully lowered the 5 tonne bogie frame onto the springs and wheel axle assemblies. This was a dangerous process with high probability for injury to fingers, hand and back of any of the four people fitting the spring assemblies. CityRail Bogie Team members put their thoughts together and designed a jig which located wheel axle assemblies. The spring assemblies (approximate total weight 45kg) could then be slid into position on the axle boxes using an adjustable height hydraulic trolley. One person could do all this and 110 37th Annual Conference Ergonomics Society of Australia Inc. when all springs were in position he could then lower the bogie frame over the springs and axle boxes. This improvement eliminated the necessity to lift spring assemblies which presented pinch points for possible hand injuries during the lift process. There are three coil springs to a spring assembly. They locate within each other. Spring Calibration CityRail bogie springs are visually checked and as an assembly of three as noted above are calibrated for compressibility. During assembly, hand and back injuries were a problem due to pinch points and weight. This was highlighted in the initial WorkCover audit. Improvements initiated the use of a disused jib crane and hoist and a lever action magnet. Assembly of springs using the magnet allowed the innerspring to be placed inside the middle spring and the two to then be placed inside the outer spring without even touching the springs by hand. The hoist eliminated any need to physically lift the spring assembly onto a small jig for sliding the spring assembly under the calibration tester and back out. When calibrated, serviceable spring sets are placed onto a pallet using the magnet and hoist for transportation to the bogie assembly area. The frequency of heavy manual handling work has been removed from the spring testing process. (2) Jiang and Smith 1985. Bolster and side frame rotating jigs The WorkCover audit highlighted a manual-handling problem when fitting freight bogie bolster and side frames into their respective rough rework jigs. These heavy parts weighing 500kg and more were maneuvered into position for grinding and welding with the aid of a gantry crane and heavy steel crowbars. This was usually a two-person operation. These components were then wedged in place with steel wedges. After the success of the CityRail bogie frame rollover-welding jig, the company quickly built rollover stands with gearboxes for the bolsters and side frames for freight bogies. This removed the need for workers to use crowbars to move these items. This paper only presents a small number of improvements that have been brought about by the company with direct input and suggestions from individual team members. “Others (Yu et al 1984. (3) Tak-sun Yu, Lewis H Roht, Robert A Wise, D J Kilian and F W Weir, have also found the teams approach is successful in improving both the occupational health and safety for workers and the productivity of the company.” 3. GENERAL BENEFITS Since the commencement of developing SWPs and serious attention to ergonomics and manual handling, many job tasks have been improved with direct input from the team members. This has resulted in increased productivity and safety awareness. Lost time injury frequencies (LTIFs) declined dramatically from the 34 in 1994. In June1999 LTIFs were down to 2.7 with 268 employees. The cost benefit of building the first roll-over stand for the CityRail bogie frame with a saving of $100,000 in the first twelve months enabled management to see the tangible benefits of improving the ergonomics of other work activities of which only a few have been mentioned in this paper. 111 Better Integration 27-30 November 2001 In 1998 Maintrain entered the Western Sydney Industry Award and won first place. There were four sections to this award two of which were OHS improvements and productivity improvement. 4. CONCLUSION Managing OHS and Injury Management integrally with other management operations of the workplace, and involving the employees where ever possible so that they share in the development of the OHS management system, brings about productivity improvement. The selection of a suitable OHS consultant who worked with all levels of the company in an advisory, nurturing capacity, drew out hidden talents of employees, won their trust and helped to focus attention on OHS&IM. The detailed process that involved workers in their development of safe work procedures including training helped them gain knowledge of good OHS practice in their daily work activities. All ergonomic improvements involved the team members and provided not only improved ergonomics and improved manual handling but increased productivity. The other initiatives mentioned in the introduction such as the value of regular workplace inspections and OHS awareness generated through the weekly team meetings has helped provide team members with initiative to continuously improve OHS and productivity. 5. ACKNOWLEDGMENTS I acknowledge the cooperation and friendship of managers and all people within Maintrain with particular mention of Ken Myles, Colin Edwards and Geoff Damon and Production Managers for their valued assistance over the years and for allowing me to present this paper about the company’s OHS and ergonomic improvements. 6. REFERENCES Bernard C Jiang and James L Smith, 1985, The comparison of stressfulness of manual materials handling activities, in R.E. Eberts and C.G. Eberts (Eds), Trends in Ergonomics/Human Factors II, (Elsvier Science Publishers B. V., North Holland), page 583. Scott, T. & Harker, P., 1998, The importance of the individual, Humanity at Work, Phil Harker and Associates Pty Ltd, Queensland, page 7. Tak-sun Yu, Lewis H Roht, Robert A Wise, D J Kilian and F W Weir, 1984, Low-back pain in industry an old problem revisited, Journal of Occupational Medicine, 26, 518. 112 Ergonomics Society of Australia Inc. 37th Annual Conference