Brucellosis - TMA Department Sites

MINISTRY OF HEALTH OFTHE REPUBLIC OF UZBEKISTAN
CENTER OF DEVELOPMENT OF MEDICAL EDUCATION
TASHKENT MEDICAL ACADEMY
Department of Infectious and Pediatric Infectious Diseases
SUBJECT: INFECTIOUS DISEASES
THEME: BRUCELLOSIS
Educational-
methodical guideline
for teachers and students of
Treatment Faculty
MINISTRY OF HEALTH OFTHE REPUBLIC OF UZBEKISTAN
CENTER OF DEVELOPMENT OF MEDICAL EDUCATION
TASHKENT MEDICAL ACADEMY
"A F F I R M"
Pro-rector of educational work
Professor Teshaev O.R.
__________________________
«____»____________2012
Department of Infectious and Pediatric Infectious Diseases
SUBJECT: INFECTIOUS DISEASES
THEME: Brucellosis
Educational-methodical guideline for teachers and students of Treatment
Faculty
"
A F F I R M E D"
at a DNC meeting of Therapeutic Faculty
Protocol № ___from_________2012
Chairman of DNC
, Professor
Karimov M.Sh.___________
1.
Theme: Brucellosis
Place of the lessons, equipping
- The auditorium;
- The emergency room;
- Department of brucellosis;
- Diagnostic department;
- The laboratory.
- Technical sources of teaching: patients with brucellosis; TV and video, teachingsupervising program, methods of work scenarios in small groups, situational tasks.
2. The duration of the study
Number of hours– 4
3. The purpose of classes
- to acquaint students with the basic clinical and laboratory signs of brucellosis;
-Methods of diagnosis, treatment and prophylaxis the principles of disease;
-Bring a sense of interest to the problem of brucellosis;
-Bring a sense of responsibility for the lives of patients with brucellosis;
-Develop scientific, logical thinking at the bedside;
- A creative approach to the diagnosis and treatment of patients with brucellosis.
Objectives
The student should know:
-Statement of the clinical diagnosis of brucellosis;
-the therapeutic tactics for brucellosis;
-Complications of brucellosis;
-Prevention of brucellosis.
The student should be able to:
- To collect patient complaints with brucellosis;
- To collect epidemic anamnesis and medical history;
- To examine the patient by organs and systems;
- Identify the typical symptoms of brucellosis;
- To formulate a preliminary clinical diagnosis;
- Assess the severity of condition of the patient;
- Interpretation of the results of laboratory tests;
- To write history of a patient with brucellosis;
- Statement of provocative tests to the patient with brucellosis;
-Draw up a plan of patient with brucellosis.
As a result of lessons the student should learn practical skills:
- To take blood for serology;
- Result of auto – and izo-therapy for diagnosis of brucellosis.
4. The motivation
Brucellosis is a anthroponouse disease flowing in both animals and humans. Brucellosis – the most common disease among the group of zoonotic infections, particularly affects farm animals.
Caused great economic damage to Animal Production and the implementation of the food
program. The study of the major issues of brucellosis is an important problem for the development and implementation of diagnostic, therapeutic and preventive measures for infectious diseases and veterinary services.
5. Inter-subject and intra-subject connection
Teaching this topic is based on the knowledge bases of students of biochemistry metabolism, microbiology, immunology, pathological anatomy, pathological physiology, physiology of the muscular-skeletal system. The findings of the lessons of knowledge will be used during the passage of medicine, surgery, obstetrics, gynecology, hematology and other clinical disciplines.
6. The content oflessons
6.1. The theoretical part
Brucellosis – zoonotic, infectious and allergic disease, with fever, lesions of the reticuloendothelial, vascular, nervous and other systems and most often the musculoskeletal system.
Etiology.
The disease in humans and animals caused by bacteria that are combined into one group called "brucellosis."
It is now known six species of brucellosis:
1.
2.
3.
4.
5.
6.
Causative agent of brucellosis in cattle.
The causative agent of brucellosis in cattle.
Causative agent of brucellosis in pigs.
The causative agent of brucellosis bush rats.
The causative agent of brucellosis in sheep, are not pathogenic to humans, but it does have antibodies in relation to this type.
Causative agent of brucellosis in dogs can cause disease in children.
In artificial media they grow slowly and the first generation appear in a period of 10-14 days to 3 months and form a small transparent colonies. The best breeding ground or them is the liver and liver broth agar. Brucella is high lyresistant to external influences and vitality.
Epidemiology . Brucellosis is a zoonosis group . The maincarriers ofbrucellosis infectionarefarm animals : sheep, goats, cows, pigs, camels, etc., as well as wildanimals -deer, elk , wolves, rodents, etc.
The most important epidemiological significance belongs to the cattle.
Sick animals brucellosis pathogen isolated from urine, feces , milk. Therefore, hair, litter, cut, water, soil contaminated with their droppings can be a source of infection for humans.
Infection occurs through the alimentary enough when using heat-treated meat and dairy products , or through casual contact and through damaged skin and mucous membranes in the care of animals or the processing of raw materials from them. Possible and aurogenic route of infection , which is due to microbial penetration through the upper airway of dust particles, hair, manure, litter the ground. Microbes suspended in the dust particles can enter the body through the mucous membrane of the conjunctiva.
Pathogenesis
Phases of infection
Phase compensated infection
Phases sepsis without local ever lesions decompensation
Phase of formation local lesions sub acute and chronic recurrent disease regulating the
( metastasis) of
Phase recovery from the residual effects of compensation , without or them, compensati on
Phase metabrutse lo sion and para gic allerphenomena of post-
Brucella
Clinical forms of brucellos is
Latent form of primary
The
(acute) form sharp-septic of The form septic metastatic
(subacute) of The form of the secondary latent
Residual symptoms after suffering a brucellosis
The form of secondary chronic
Metastatic form of primary chronic
Metastatic
Clinically significant
Clinic
The incubation period for brucellosis ranges from 2 to 5 weeks , while those of professional groups from 8 to 12 weeks or longer.
In the prodromal period, you can detect the presence of general malaise , feelings of irritability , weakness, anxiety, loss of appetite; muscle aches in the limbs, chilliness in the evening , a slight increase in temperature to sub febrile figures and other symptoms in patients that do not pay attention and continue their usual job.
At the expiration of the period of prodromal patients developed clinical brucellosis , while in some cases it starts badly , with chills , fever, sweating increased sharply , ache all over, gain and increases symptoms of intoxication , and in others
– with the gradual development of the symptomology of the disease in a chilling, feeling hot, dry mouth, a gradual increase in temperature , which then becomes the leading symptom of the disease, or against subfebrile develop other symptoms of the disease.
Primary latent brucellosis observed in the case of brucellosis , but because of good resistance of the patient did not manifest clinical symptoms . Individuals with positive serological reactions ( Wright, Hedelson ) for brucellosis without clinical manifestations are registered for the observation of a person with latent .
Sharpseptic (acute ) form at the end of the incubation period lasts from 1 week to1-2 months . Sometimes several months ( latency), begin to show clinical signs . The acute stage of the disease accompanied by fever , lasting from a few days , weeks to 1-3 months , sometimes longer.
The temperature curves are of tenundulating character . Characteristic chills are of ten stunning , as in malaria , and during the day repeated several times , as well as sweating, especially at night, profuse that the patient during the day several times compelled to change the linen. Disturbed sleep and appetite slightly , even at high temperature and general condition remains satisfactory.
There is an increase in axillary inguinal , submandibular, less often than other nodes .
Patients appear volatile pain in large joints , increased liver, spleen, less frequently in violation of the functional activity of the liver , as well as the autonomic nervous system
(irritability , sweating, etc.). Sex organs are affected .
Cardiovascular system is marked dullness of heart tones , hypotension. Violation of other organs most often less pronounced . From the peripheral blood changes are minor , often marked leucopenia , neutropenia and relative lymphocytosis, ESR accelerated.
With timely proper treatment of acute illness may complete recovery. If treatment is not carried out , the acute stage can last up to three months with the transition , and sub-acuteor chronic form of the disease.
Septic metastatic (sub-acute ) form is a continuation of the pathological process. It is characterized by a greater severity of clinical manifestations and diverse, persistent lesions in various organs and systems , often excruciating pain.
There are local affections of the loco-motor system in the form of arthritis, bursitis , sacroiliitis , and sometimes swelling of joints ( especially large ones), accompanied by severe pain and limitation of active movement . The defeat of the spine is observed as spondylarthrosis
(usually the lower part ). Develop myositis, myalgia, tendovaginitis , fibrositis , cellulitis .
The most common lesion of the nervous system is mainly peripheral plexitis, radiculitis .
The men are possible orchitis , epididymitis, orho-epidilemitis ; female menstrual disorders, inflammatory changes of the genital organs , miscarriages, up to infertility.
Sub-acute form of the disease occurs with high fever , often wave-like type, with damage to various organs and systems, and may continue for several months.
Absence of proper treatment promotes the progression of the process with the transition to secondary chronic stage.
Characteristic clinical re-infection brucellosis is that the disease is symptomatic , clinically relevant form of the disease . With the defeat of re-infection with the systems of internal organs is more pronounced , and the performance of serological reactions is higher than in primary disease brucellosis, which should be considered in the diagnosis of brucellosis multiplicity . Also , it is proved that the clinic of acute , sub-acute, primary and secondary forms of chronic brucellosis rein centers, deprived of brucellosis of small ruminants , occurs with a short incubation period , more seriously , with the defeat of the reticulo-endothelial system and reproductive organs, as well as more prolonged course of disease compared with primary disease.
Brucellosis in vaccinated . The clinical picture is different. There are various clinical forms of the disease.
Clinic of brucellosis in children. The clinical picture in children is the same as in adults , but along with these children revealed a number of peculiarities caused by age. At an early age- severe acute infection with brucellosis symptoms severe enough , with age, the clinic is complicated , there is a tendency toa prolonged duration.
Mixed brucellosis. The course of brucellosis, with concomitant acute intestinal infections
(typhoid and paratyphoid diseases, dysentery and viral hepatitis) and chronic diseases
(tuberculosis, chronic hepatitis and colitis) is persistent. At the clinic symptoms of brucellosis accumulate concomitant acute or chronic disease that can lead to a complicated course.
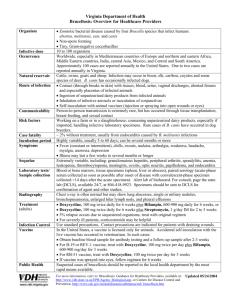
Diagnosis
Established on the basis of epidemiological history , the development of the disease, objective data and the results of laboratory studies . Laboratory diagnosis of brucellosis includes bacteriological, serological method and an allergy test .
Bacteriological method is blood culture , bone marrow, cavity fluids , urine, bile, milk , cerebrospinal and amniotic fluid, genital secretions .
Serological method is based on the development of the organism Brucella-patients with specific antibodies. Recommended for the diagnosis of reaction Wright Heddelson , Coombs , complement fixation , passive hemagglutination .
Wright's reaction is specific and is considered positive in dilutions of 1:100 -1:200 ; rapid method agglutination test Heddelson very sensitive but less specific .
Antiglabulin test of Coombs best price for chronic and residual brucellosis , especially when the reaction Wright and Heddelson , RSK negative. Complement fixation testis specific and is more sensitive in protracted and chronic forms of brucellosis.
Passive hem-agglutination reaction is highly sensitive and specific for brucellosis, a titer of 1:100 is considered as positive.
Allergic diagnosis of brucellosis by using the sample (atByurne ). Samples Byurne based on the ability of the organism , and specifically meet the local response to intra-dermal administration of brucellin . The response is evaluated positively swelling in size from 2 to 6 sm diameter.
Differentiated from the typhoid and paratyphoid diseases , malaria, typhus , Q fever , tuberculosis, rheumatic fever , sepsis, leishmaniasis, Hodgkin's disease , influenza, etc.
Are crucial epidemiological history, the history of the disease , the results of objective and laboratory studies.
Treatment
Treatment is prescribed in the light of clinical and laboratory data individually, which requires a careful examination of the patient . Treatment should be comprehensive , with etiotropic , special
(vaccination ), pathogenetic , symptomatic , and physical therapy techniques.
Antibiotic shave a bacteriostatic effect on the agents of brucellosis , remove intoxication and cropped the clinical symptoms . The treatment is effective, drugs were tetracycline group
( terramycin, tetracycline, biomycin ), gentamicin, rifampicin, rondomitsin , levomitsin , streptomycin and its analogues . The combination of streptomycin with one of the antibiotics has the best effect . It is also used erythromycin, oletotetrin ( tetraolean) oleandomitsin and other antibiotics . Degidrostreptomitsin and streptomycin injected i/m to 250,000 units.
Tetracycline drugs administered by 200000 - 300000 units every 6 hours , chloramphenicol by 0.5g every 6 hours later , rifampicin 0.15g every 6 hours , later to exchange the inside, gentamicin 40 mg . i/m , antibiotics are appointed within 7- 10days.
With little effect antibiotic substitute to other antibiotic , and a second course of antibiotic therapy . The interval between courses should be given 5-10 days in the peripheral blood and the condition of the patient .
Antibiotic treatment does not always prevent relapses of brucellosis. When latent , chronic forms , i.e., in the inactive phase, with a normal temperature, the phenomenon of residual antibiotics are not effective. In view of this antibiotic should be administered strictly justified.
Vaccine is a specific method of treatment. It stimulates the immune response, resulting in a temporary hypo-sensitization , promotes a more rapid effect of treatment.
In the appointment of vaccine therapy should be considered an allergic condition of the body
(sample of Byurne ), the activity of the infectious process ( serological reaction of Wright ), the cardiovascular system ( ECG).
Vaccine is indicated for chronic brucellosis , the activation process with the clinical manifestations of acute , sub-acute, and latent forms of vaccine therapy is not indicated.
In the course of treatment is necessary to change the dose of vaccine , depending on the reaction of the organism.
Intravenous method is effective , most used in practice in the treatment of patients with a two-step method by G.P. Rudnev ( a course of injections with an interval of 3-4 days ). With this method, the vaccine at the recommended dose in 2 divided doses with an interval of 1.5 - 2 hours postsmoothes the vaccine response ( a serving is called the primary, sets up the patient , and 2 the resolution is reworking serving of the daily dose). The positive therapeutic effect of the vaccine is considered when starting from 3-4 injections of fever .
Corticosteroids - with the defeat of the CNS, encephalitis , meningitis, poly-arthritis of rheumatoid type. The best effect has the use of hormones in the sub-acute stage and phase of relapse of chronic forms of brucellosis.
Contraindications to the use of corticosteroids are hypertension, peptic ulcer and 12 duodenal ulcers , marked osteoporosis , diabetes, mental illness, and menopause.
Rational corticosteroids in combination with antibiotics 250,000 units 3 times a day for 10 days , vitamins, blood transfusion and other bracing means single-group blood transfusion of 100- 150 ml.
When sharply pronounced neuralgia and neuritis shows novocaine blockade . Used method of creeping infiltration , enter 0.25% solution of Novocain/cof 25-100ml.
Radiculitis , persistent arthritis, bursitis and CNS has a good effect the introduction of a mixture of 1% novocaine solution (5-10ml), hydrocortisone (20-25mg) and penicillin ( 50,000 IU ) or just the novocaine ( 3-5 ml ) in the most painful point in the joint, along the roots.
At various pains of vegetative origin, as well as shown in polyneuritis introduction of novocaine as a 0.25% solution in increasing doses 05-10ml daily (a total of 10-15injections ).
In introduction of novocaine and novocaine blockade are effective in pain expressed in the sub-acute and chronic and residual brucellosis .
Physical methods of treatment currently hold a leading position in the complex treatment of patients with sub-acute , chronic and residual brucellosis . The choice of physical therapy depends on clinical form of the disease, the phase currents, and the duration of the disease process .
Clinical supervision for the ill with brucellosis carried out in order to prevent the progression of the infection process and the transition of their disability .
Prevention
For a sharp decline in the incidence of brucellosis people necessary to carry out complex epidemiological and preventive measures to eliminate hotbeds of infection.
Comprehensive Plan activities include measures to prevent disease , detect and eliminate the source of infection , early diagnosis and early treatment are brought to the sick, medical examinations react positively for brucellosis . In addition, a comprehensive plan takes into account the state of the epizootic among sheep , cattle, belonging to community and individual households . In identifying patients and positive lyre acting animals should taked rastic measures and of reacting negatively in the number of animals tested for brucellosis should be specific prophylaxis against this infection .
Of particular importance is the implementation of preventive measures on meat and
Leather processing plants, Karakul factory , where the manufacturing process should izladit basis of mechanization and automation, is prevented from hides of infected animals , as well as to implement safety measures aimed at preventing infection and disease brucellosis workers .
In prevention of brucellosis is important impact on the route of infection , including increased alertness to the infection of employees live stock and meat processing plants , conducting sanclearance work to wards at preventing infection with brucellosis as a result of direct contact with the source of infection ( animal raw materials and products ).
Of particular importance is the decontamination of milk ( pasteurization or boiling quality ), the strict control of milk on dairy farms , milk collection points , systematic laboratory testing of milk for brucellosis in dairy factories .
Used in this lesson, new educational technology " Brainstorm "
" Handle at the middle of the table ."
USING "BRAINSTORM"
The main provisions of the technique:
- Any comments and criticisms , which prevent the formation of ideas;
- Greet in soaring thought , given that the more unusual the idea , the better;
- Receiving the largest number of proposals;
- A combination of ideas and their development;
- short statement , without argument deployed ;
- The division of those who generate ideas and those of their processes .
This technique is taught to argue and defend their own point of view , to find the optimal solution in every situation , to build communication, to persuade opponents of loyalty to the position advocated .
USING " HANDLE AT THE MIDDLE OF THE TABLE "
It is proposed the task to the whole group (for example, to list the symptoms of brucellosis , drugs used for brucellosis , etc). Each student write son a piece of an answer and sends it to a neighbor , and his hand moves to the middle of the table .
The teacher monitors the work of the group and the involvement of everyone, a generic version is written in the notebook.
While working on this method can be adapted to use the OCP setting
Options for abstracts:
1.
Definition of Brucellosis : Brucellosis – Infectious and allergic disease , which has a tendency to chronicity . It is characterized by prolonged fever, lesions of musculoskeletal , neurological, cardiovascular, genitourinary and other systems .
2.
Which group is brucellosis ? Zoonotic infections .
3.
List the causative agent of brucellosis : Br. melitensis, Br. Abortus bovis, Br. Abortus suis, Br. neotomae, Br. canis, Br. ovis.
4.
Source of infection : small and large cattle, pigs.
5.
The mechanism of infection and transmission : The mechanism of infection or nutritional pin path, however, also possible aerogenic . In the transmission from animals to humans are the value of raw meat and dairy products. Secretions of infected animals containing
Brucella , dirty hair, food, litter in the stalls , soil and water. All the se objects can be infected by factors of transmission .
6.
Clinical classification : The duration of the course : acute (up to 3 months). Sub-acute (up to 6 months). Chronic (more than 6 months.) . Residual ( clinical implications ). Severity
( mild, moderate, severe). The phases of (compensation, subcompensation , decompensation ).
7.
Complications of brucellosis : Organic changes musculoskeletal deformity of the joints due to proliferation of periarticulartissues.
8.
Laboratory diagnosis of brucellosis : bacteriological , biological, serological and allergic .
Serological methods : the reaction Wright and Heddelson , RAC , Phragmites , Coomb's reaction . Allergic method – reaction of Byurne .
9.
What re-infection and super-infection ? Re-infection- redeveloping the disease as a result of new infection with the same agent. Super-infection – connection to the primary disease the second, caused by another agent.
10.
What is cellulite and fibrosis ? Cellulite – is education in the subcutaneous tissue of dense , painful nodules. Fibrositis – is the formation of tendons and muscles tight , painful knots.
11.
The main clinical symptoms of residual forms of brucellosis : increased sweating, irritability, changes in the neuropsychiatric, arthralgia . Pain in joints intermittent, aggravated by physical work and the weather . Body temperature is normal, at least lowgrade .
12.
What medications are used for specific prevention of brucellosis ? Live brucellosis vaccine (Br.bovis).
6.2. The analytical part of
Situational problems :
Objective number one .
Patient L.
, 19 years old, works on the farm milkmaid . Vaccination has not been . With a planned survey found positive serological reaction Hedelson + + ; Wright1:200.
Does not hurt. On examination, no complaints. As authorities showed no abnormality . Complete blood count was normal.
1. Your preliminary diagnosis ?
2. Your tactics of the patient ?
№
The answer
1. Brucellosis, primary latent form.
2. Monitoring , decontamination of chronic foci of infection .
Protective mode.
Increased food (protein , vitamins ).
Objective number two .
Patient Yu , 32 years old, works as an accountant , became ill acute. In the evening the temperature rose up to 38,5 ºC. Happy condition remained satisfactory , the
patient continued to work. For the first time turned to the doctor on the third week of illness.
When viewed from t = 37,8 ºC, normal skin color and moist. Axillary lymph nodes with beans, mobile and painless. Heart and liver were normal. The liver is 1.5cm,0.5cm Chair spleen , urine output was normal. Bones and joints without the disease. Previously, no hurt. In the individual farm has a cow, which had a miscarriage.
1.
Your preliminary diagnosis ?
2.
Plan examination ?
3.
Make a plan of treatment for diagnosis.
№ The answer
1. Acutely septicaemic form of brucellosis.
2. Blood on thesterility,blood cultures .
Blood on thereactionWrightHedelsona .
3. a)a combination ofbroad-spectrum antibioticswith athree-course5day break; b)restorative therapy , vitamin therapy ; c)desensitizationtherapy; d)detoxificationtherapy.
The practical part
Forserologicalstudies , if obtainedminimumtitresfor the diagnosisof brucellosisis appliedautoisohematherapy-a provocativemethod.To do this:/ in15 mlof bloodis takenand put into/ mnumber 3in a day.After twodaystakesa bloodserology , if after the autoisohemotherapybloodtiterrisesthanon the basisof the primaryepid.anamneza
, clinical andphysical examinationcandiagnosebrucellosis.
The formof knowledge andskills
- Interpreting ;
- Solutionof situationalproblems;
- Demonstration ofskills .
7.Test questions
1. Determination ofbrucellosis.
2. The etiology ofbrucellosis.
3.
The epidemiology ofbrucellosis.
4. The pathogenesis ofbrucellosis.
5. Clinical classification ofbrucellosis.
6.Clinic ofacutesepticforms ofbrucellosis.
7.Clinicsepticmetastaticforms ofbrucellosis.
8. Clinic forprimarychronic form ofbrucellosis.
9.Clinicsecondarychronic form ofbrucellosis.
10.Laboratory diagnosis ofbrucellosis.
11.Differential diagnosis ofbrucellosis.
12.Outcomesand complications ofbrucellosis.
13.Treatment ofbrucellosis.
14.Prevention ofbrucellosis.
15.Whatskillsare used forbrucellosis ?
7. Recommended reading
Main books:
Madzhidov V.M. infectious diseases , T., 1992.
Makhmudov O.S. childhood infectious diseases , T., 1995.
Uchaikin V.R. Guide to Infectious Diseases in Children , M., 1999.
Shuvalov E.P. Infectious Diseases , Moscow, 1999.
Additional
Musabayev I.K
. "Guide to intestinal infections ", T.
, 1982.
Pokrovsky V.I. Pak S. G . et al, " Infectious disease and epidemiology ."
– Moscow, 2003
Yushchuk N.D., Vengerov Y.Y. "Lectures on infectious diseases ." – M.
, 1999.
Uchaikin V.F. "Guidelines for Infectious Diseases in Children" , - M., 1998.
Online Resources (www.medlinks.ru, www.cdc.gov).