Wound dressings - Surgery journal
advertisement

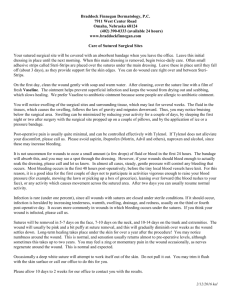
BASIC SKILLS The local environment of the wound Wounds can be divided into four categories (Figure 1) based on their appearance and stage of healing. Each wound type has slightly different characteristics and a wound healing by secondary intention will progress through these different stages over time. There is no ‘one size fits all’ dressing, hence wounds must be re-evaluated regularly in order to identify and respond to any changes. Wound dressings Nicholas F S Watson Wendy Hodgkin Necrotic wounds (Figure 1a) are usually black or dark green and contain devitalized tissue. Infected necrotic wounds require sharp surgical debridement back to viable tissue in order to prevent systemic sepsis. In the absence of infection, necrotic tissue will eventually separate from the wound bed by autolysis. Necrotic wounds are particularly susceptible to dehydration, and autolysis is inhibited if the wound is allowed to dry out; the main priority of a dressing is to maintain sufficient moisture in the local environment of the wound. The rational use of dressings for wound healing by secondary intention is the focus of this contribution, which should be read with ‘Classification and management of acute wounds’, page 47. Practical selection of dressing There is a lack of high-quality research data regarding the relative efficacy of the various dressings, so the choice of dressings used in everyday practice in the UK is often based on familiarity, personal preference and cost. Wound care and dressing selection should be a holistic, structured process involving close cooperation between medical and nursing staff. Three factors must be considered when assessing the requirement for a wound dressing: • general health of the patient • local environment of the wound • specific properties of the dressing. Sloughing wounds (Figure 1b) contain a mixture of leukocytes, wound exudate, dead bacteria and fibrin, typically forming a glutinous yellow layer of tissue over the wound. The presence of slough predisposes to wound infection because it provides a nutrient-rich environment for bacterial proliferation. The formation of granulation tissue is delayed in a sloughing wound compared with a clean wound, and hence the optimal dressing will contribute towards wound debridement and maintenance of a clean wound bed. Granulating wounds (Figure 1c) are highly vascularized and are a rich pink or red colour. The amount of exudate produced is often substantial, and a dressing with the capacity to absorb excess exudate is desirable. Significant heat loss may occur with wounds covering large areas, requiring a dressing with insulating properties. Overgranulating wounds have the following properties, they: • contain excessive friable granulation tissue • are prone to recurrent episodes of bleeding • suffer from delayed epithelialization. In this situation, caustic pencils containing silver nitrate or topical corticosteroid can be applied directly to the affected areas in order to control the excess tissue. Patient factors Patients should undergo systematic assessment to address the underlying cause of their wound. Factors that may delay the healing process must be addressed, and may include ensuring that: • nutritional intake is sufficient • anaemia and electrolyte imbalances are corrected • diabetic control is optimized • appropriate pressure-relieving equipment is provided • systemic infection is treated • foreign bodies are removed • peripheral oedema is reduced • smoking is stopped. Some factors may not be easily resolved (e.g. advanced malignancy, previous radiotherapy), and this should be considered when monitoring progress of the wound. If the patient has to manage the wound himself, assessment should also include factors such as co-ordination, continence and general cognitive function, any of which may alter the final selection of the dressing. Epithelializing wounds (Figure 1d) contain new epithelial tissue (formed by migration of keratinocytes from the wound margins) or contain islands of tissue (formed from skin appendages in the wound bed). The main priorities for dressing are the maintenance of a warm, moist environment around the wound, and the use of low-adherence dressings (see below) to minimize the trauma of dressing changes. In addition to the type of wound, the location, size and depth of the wound may vary considerably. Along with the condition of the surrounding skin, these should also be considered when deciding the most suitable dressing. Dressing factors The ‘ideal’ properties of a dressing for optimal wound healing are listed in Figure 2. No product fits this profile exactly, so dressing selection should address the most important factors identified in a particular clinical scenario. Dressings can be grouped into broad categories because many have similar actions and characteristics (Figure 3). Nicholas F S Watson is a Research Fellow in Colorectal Surgery in the Department of Surgery, Queen’s Medical Centre, Nottingham, UK. Wendy Hodgkin is a Clinical Nurse Specialist in tissue viability for Nottingham Primary Care Trusts and Queen’s Medical Centre, Nottingham, UK. SURGERY 23:2 52 © 2005 The Medicine Publishing Company Ltd BASIC SKILLS Wound appearances in different stages of healing by secondary intention a Necrotic wound. b Sloughy wound. c Granulating wound. d Epithelializing wound. 1 Tulle dressings (e.g. Paratulle™, Bactigras™, Jelonet™) are cotton or viscose gauze dressings impregnated with paraffin (antiseptic or antibiotic may also be incorporated). Paraffin lowers the dressing adherence, but this property is lost if the dressing dries out. The hydrophobic nature of paraffin prevents absorption of moisture from the wound, and frequent dressing changes are usually needed. Skin sensitization is also common in medicated types. Tulle dressings are mainly indicated for superficial clean wounds, and a secondary dressing is usually needed. Properties of the ‘ideal’ wound dressing • Maintains a moist environment around the wound • Removes excess exudate, but prevents saturation of the dressing to its outer surface (‘strike through’) • Permits diffusion of gases • Protects wound from micro-organisms • Provides mechanical protection • Controls local temperature and pH • Is easy and comfortable to remove/change • Minimizes pain from the wound • Controls wound odour • Is cosmetically acceptable • Is non-allergenic • Does not contaminate the wound with foreign particles • Is cost effective Low-adherence dressings (e.g. Melolin™, Mepore™, Mepitel™) are manufactured from materials ranging from knitted viscose to polyester fabric. Built-in perforations reduce adherence between the dressing and the wound surface. Removal is easy with little or no trauma, but they have minimal absorptive capacity and are unsuited for all but lightly exudating and superficial wounds. Hydrocolloids (e.g. Granuflex™, Comfeel™, Tegasorb™) contain a hydrocolloid matrix of gelatin, pectin and cellulose mixed together to form a waterproof adhesive dressing that interacts with the 2 SURGERY 23:2 53 © 2005 The Medicine Publishing Company Ltd BASIC SKILLS alginates change from a soft fibrous texture into a gel, facilitating easy removal and preventing dressing fibres from contaminating the wound. Alginates are manufactured as flat sheets or as rope, and are suitable for packing cavities. Main types of wound dressings • • • • • • • • • • Tulle dressings Low-adherence dressings Hydrocolloids Hydrofibres Hydrogels Films Foams Alginates Mechanical devices Bioactive/biological dressings Odour-reducing dressings (e.g. Clinisorb™, Actisorb™) are used primarily for fungating, infected and gangrenous wounds where malodour is a particular problem. They usually contain charcoal and should not be cut into because the charcoal fibres may shed into the wound. Dressings containing iodine(e.g. Inadine™, Iodosorb™, Iodoflex™) come in two forms, as povodine–iodine impregnated into a low-adherent dressing or dressings containing concentrated cadexomer iodine paste. They possess broad antibacterial activity and are indicated for infected or heavily colonized wounds. Iodinated dressings should be removed when they change colour from brown to white (indicates uptake of available iodine). Systemic absorption of iodine can be significant with prolonged use, especially if used in wounds with a large surface area. Hence, these dressings should be avoided in patients with a history of thyroid disorders. 3 wound bed. Exudates produced by the wound absorb into the dressing, which dissolves and forms a gel. The moisture from this gel enhances autolytic debridement of necrotic and sloughing tissues and promotes the formation of granulation tissue. Hydrocolloid dressings absorb light-to-moderate levels of exudate, do not require a secondary dressing, and are shower-proof. Dressings containing silver exist in many different formulations, and exhibit a broad antibacterial spectrum. They are often used in burn wounds, and are also indicated for infected and heavily colonized wounds. Their use is occasionally limited by hypersensitivity. A summary of the most commonly used primary wound dressings for different wound types is shown in Figure 4. Hydrofibres (e.g. Aquacel™) are produced from similar materials to hydrocolloids and also form a gel on contact with the wound, but are softer and more fibrous in appearance, with a greater capacity to absorb exudate. Moisture from the gel assists in debridement and facilitates non-traumatic removal. Mechanical devices In the UK, the most commonly used mechanical device in wound care is the vacuum-assisted closure device, which applies topical negative pressure (50–125 mmHg) spread evenly over the wound bed. A specialized open-pore foam dressing is cut to fit the wound dimensions and is then attached to a vacuum pump unit via tubing placed under an occlusive secondary dressing. Vacuum-assisted closure is extremely effective in removing exudate and reducing oedema in the surrounding tissue, while leaving the surface of the wound moist. Local blood flow to the wound is improved, with a subsequent increase in vascularity of the wound bed and formation of granulation tissue. The wound is completely sealed to the external environment and, because exudate is removed, bacteria are drawn away, and the risk of wound sepsis is reduced. Vacuum-assisted closure is used in the management of large or deep wounds where very high levels of exudate are produced which would quickly overwhelm conventional dressings. Necrotic wounds or those with thick, dry slough require adequate debridement before vacuum-assisted closure can be applied. Vacuum-assisted closure is contraindicated in: • wounds with exposed blood vessels or organs • unexplored fistulas • untreated osteomyelitis • local malignancy. Hydrogels (e.g. Intrasite™, Nu-gel™, Aquaform™) consist of starch polymers with a very high intrinsic content of water. They conform to wounds with unusual shapes due to their gel-like nature. In contrast to hydrofibres, hydrogels are used primarily to donate fluid to dry necrotic and sloughing wounds, and their absorbency is limited. A secondary dressing is usually needed. Films (e.g. Opsite™, Tegaderm™, Bioclusive™) are made from a thin polyurethane film coated with adhesive. Film dressings are highly comfortable, shower-proof and their transparency allows for wound monitoring without dressing removal. Vapour-permeable films allow diffusion of gases and water vapour, but are minimally absorbent. Problems can arise if these dressings are applied to heavily exudating wounds because fluid tends to accumulate underneath the film, leading to maceration of the wound and the surrounding skin. Films are thus suited to superficial, lightly exudating or epithelializing wounds. Foam dressings (e.g. Lyofoam™, Allevyn™, Tielle™) are constructed from polyurethane and absorb exudate without interacting with the wound bed. They absorb low-to-moderate amounts of fluid and usually have a semi-permeable backing to allow the escape of moisture. Foams do not require a secondary dressing and are often used as an outer dressing with other products (e.g. hydrogels). Alginates (e.g. Sorbsan™, Kaltostat™, Algisite™) are derived from a calcium salt of alginic acid, producing highly absorbent dressings suitable for heavily exudating wounds; some alginates also possess haemostatic properties. As they absorb exudate, SURGERY 23:2 Biological dressings Larvae (LarvE™) of the common greenbottle fly (Lucilia sericata) are bred in sterile conditions. These larvae are necrophagous 54 © 2005 The Medicine Publishing Company Ltd BASIC SKILLS Dressings for different wound types • Hydrogel* • Hydrocolloid • Saline-soaked hydrofibre* Dry necrosis Dry slough • Dry hydrofibre* • Larvae (seek specialist advice) Wet, loose slough Superficial wound • Foam • Hydrocolloid Granulating Cavity wound Sinus cavity • Hydrofibre • Alginate • Low adherent* dressing • Hydrocolloid* • Film Epithelializing Infected Treat with systemic antobiotics Malodorous Check for signs of infection and treat if appropriate with systemic antibiotics Dressing containing silver or iodine No infection Deodorizing dressing* (consider debridement if appropriate) Bleeding Haemostat (i.e. alginate)* Fungating Not bleeding Treat as above, but consider non-adherent primary layer to reduce risk of bleeding *Requires secondary dressing 4 (avoiding healthy, viable tissues) and are very effective in treating sloughing and necrotic wounds. The number of larvae applied is relative to the size of the wound, and they are usually left in situ for three days. The larvae feed by a process of extracorporeal digestion, secreting various enzymes that break down the dead tissue to an ingestible consistency. Larvae also possess direct antibacterial activity, although the exact mechanism for this is unknown. Side-effects (physical discomfort, transient pyrexia, bleeding) are rare. Larvae therapy is contraindicated in wounds that connect with body cavities. UK guidelines Current guidance from the UK National Institute for Clinical Excellence on the use of debriding agents and specialist wound care clinics for difficult-to-heal surgical wounds states that ‘although there is no randomized controlled trial evidence to support any particular method, both modern dressings which promote autolytic debridement and larvae therapy may reduce pain and be more acceptable to patients when compared with traditional dressings’. They also advise that the individual choice of dressing should consider aspects related to patient acceptability, type and location of wound, and total costs. u ‘Skin-substitute’ dressings (e.g. Integra™, Alloderm™) are increasingly finding clinical application in the UK, but their use is restricted to the specialist setting. SURGERY 23:2 55 © 2005 The Medicine Publishing Company Ltd