CMS Limitations Guide
advertisement

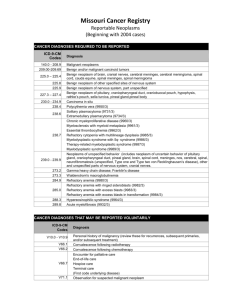
CMS Limitations Guide – Mammograms and Bone Density Radiology Services Starting July 1, 2008, CMS has placed numerous medical necessity limits on tests and procedures. This reference guide provides you with all of the latest changes. This guide is not an all-inclusive list of National Coverage Documents (NCD) and Local Coverage Documents (LCD). Please consult the CMS website for additional information at cms.hhs.gov/mcd/search.asp?clickon=search. You can search by LCD or NCD or keyword and region. CMS will deny payment if the correct diagnosis codes are not entered on the order form, and your patient’s test or procedure will not be covered. We compiled this information in one location to make it easier for you to find the proper codes for medically necessary diagnoses. It is the responsibility of the provider to code to the highest level specified in the ICD-9-CM (e.g. to the fourth or fifth digit). The correct use of an ICD-9-CM code listed below does not assure coverage of a service. The service must be reasonable and necessary in the specific case and must meet the criteria specified in this determination. We will continue to update this list as new CMS limitations are announced. You can always find the most current list on mymunson.org. If you have any questions, please contact Kari Smith, Office Coordinator, at (231) 935-2296, or Karen Fouch, Manager, Patient Access Services, at (231) 935-6164. Screening Mammograms (L26890)....................................................................................................2 Diagnostic Mammograms (L26890) ...................................................................................................3 US Breast & MRI Breast (L26890) ......................................................................................................6 Bone Densities (L26385).....................................................................................................................8 -1- Screening Mammograms (L26890) V76.11 SCREENING MAMMOGRAM FOR HIGH-RISK PATIENT V76.12 OTHER SCREENING MAMMOGRAM -2- Diagnostic Mammograms (L26890) 174.0 MALIGNANT NEOPLASM OF NIPPLE AND AREOLA OF FEMALE BREAST 174.1 MALIGNANT NEOPLASM OF CENTRAL PORTION OF FEMALE BREAST 174.2 MALIGNANT NEOPLASM OF UPPER-INNER QUADRANT OF FEMALE BREAST 174.3 MALIGNANT NEOPLASM OF LOWER-INNER QUADRANT OF FEMALE BREAST 174.4 MALIGNANT NEOPLASM OF UPPER-OUTER QUADRANT OF FEMALE BREAST 174.5 MALIGNANT NEOPLASM OF LOWER-OUTER QUADRANT OF FEMALE BREAST 174.6 MALIGNANT NEOPLASM OF AXILLARY TAIL OF FEMALE BREAST 174.8 MALIGNANT NEOPLASM OF OTHER SPECIFIED SITES OF FEMALE BREAST 174.9 MALIGNANT NEOPLASM OF BREAST (FEMALE) UNSPECIFIED SITE 175.0 MALIGNANT NEOPLASM OF NIPPLE AND AREOLA OF MALE BREAST 175.9 MALIGNANT NEOPLASM OF OTHER AND UNSPECIFIED SITES OF MALE BREAST 183.0 MALIGNANT NEOPLASM OF OVARY 196.3 SECONDARY AND UNSPECIFIED MALIGNANT NEOPLASM OF LYMPH NODES OF AXILLA AND UPPER LIMB 197.0 SECONDARY MALIGNANT NEOPLASM OF LUNG 197.1 SECONDARY MALIGNANT NEOPLASM OF MEDIASTINUM 197.2 SECONDARY MALIGNANT NEOPLASM OF PLEURA 197.7 MALIGNANT NEOPLASM OF LIVER SECONDARY 198.2 SECONDARY MALIGNANT NEOPLASM OF SKIN 198.3 SECONDARY MALIGNANT NEOPLASM OF BRAIN AND SPINAL CORD 198.5 SECONDARY MALIGNANT NEOPLASM OF BONE AND BONE MARROW 198.81 SECONDARY MALIGNANT NEOPLASM OF BREAST 199.0 DISSEMINATED MALIGNANT NEOPLASM 199.1 OTHER MALIGNANT NEOPLASM OF UNSPECIFIED SITE 217 BENIGN NEOPLASM OF BREAST 232.5 CARCINOMA IN SITU OF SKIN OF TRUNK EXCEPT SCROTUM 233.0 CARCINOMA IN SITU OF BREAST 238.2 NEOPLASM OF UNCERTAIN BEHAVIOR OF SKIN 238.3 NEOPLASM OF UNCERTAIN BEHAVIOR OF BREAST 239.2 NEOPLASM OF UNSPECIFIED NATURE OF BONE SOFT TISSUE AND SKIN 239.3 NEOPLASM OF UNSPECIFIED NATURE OF BREAST 451.89 PHLEBITIS AND THROMBOPHLEBITIS OF OTHER SITES 610.0 SOLITARY CYST OF BREAST -3- 610.1 DIFFUSE CYSTIC MASTOPATHY 610.2 FIBROADENOSIS OF BREAST 610.3 FIBROSCLEROSIS OF BREAST 610.4 MAMMARY DUCT ECTASIA 610.8 OTHER SPECIFIED BENIGN MAMMARY DYSPLASIAS 610.9 BENIGN MAMMARY DYSPLASIA UNSPECIFIED 611.0 INFLAMMATORY DISEASE OF BREAST 611.1 HYPERTROPHY OF BREAST 611.2 FISSURE OF NIPPLE 611.3 FAT NECROSIS OF BREAST 611.4 ATROPHY OF BREAST 611.5 GALACTOCELE 611.6 GALACTORRHEA NOT ASSOCIATED WITH CHILDBIRTH 611.71 MASTODYNIA 611.72 LUMP OR MASS IN BREAST 611.79 OTHER SIGNS AND SYMPTOMS IN BREAST 611.83 CAPSULAR CONTRACTURE OF BREAST IMPLANT 611.89* OTHER SPECIFIED DISORDERS OF BREAST 611.9 UNSPECIFIED BREAST DISORDER 612.0 DEFORMITY OF RECONSTRUCTED BREAST 612.1 DISPROPORTION OF RECONSTRUCTED BREAST 785.6 ENLARGEMENT OF LYMPH NODES 793.80 UNSPECIFIED ABNORMAL MAMMOGRAM 793.81 MAMMOGRAPHIC MICROCALCIFICATION 793.82 INCONCLUSIVE MAMMOGRAM 793.89 OTHER (ABNORMAL) FINDINGS ON RADIOLOGICAL EXAMINATION OF BREAST 879.0 OPEN WOUND OF BREAST WITHOUT COMPLICATION 879.1 OPEN WOUND OF BREAST COMPLICATED 922.0 CONTUSION OF BREAST 996.54 MECHANICAL COMPLICATION OF BREAST PROSTHESIS 996.69 INFECTION AND INFLAMMATORY REACTION DUE TO OTHER INTERNAL PROSTHETIC DEVICE IMPLANT AND GRAFT V10.3 PERSONAL HISTORY OF MALIGNANT NEOPLASM OF BREAST V10.89* PERSONAL HISTORY OF MALIGNANT NEOPLASM OF OTHER SITES V15.89 -4- OTHER SPECIFIED PERSONAL HISTORY PRESENTING HAZARDS TO HEALTH V45.83* BREAST IMPLANT REMOVAL STATUS V67.1 FOLLOW-UP EXAMINATION FOLLOWING RADIOTHERAPY V67.2 FOLLOW-UP EXAMINATION FOLLOWING CHEMOTHERAPY V71.1 OBSERVATION FOR SUSPECTED MALIGNANT NEOPLASM *Use ICD-9-CM code 611.89 for hematoma *ICD-9-CM codes V10.89 and V45.83 may be reported only until clinical stability has been established. -5- US Breast & MRI Breast (L26890) 174.0 MALIGNANT NEOPLASM OF NIPPLE AND AREOLA OF FEMALE BREAST 174.1 MALIGNANT NEOPLASM OF CENTRAL PORTION OF FEMALE BREAST 174.2 MALIGNANT NEOPLASM OF UPPER-INNER QUADRANT OF FEMALE BREAST 174.3 MALIGNANT NEOPLASM OF LOWER-INNER QUADRANT OF FEMALE BREAST 174.4 MALIGNANT NEOPLASM OF UPPER-OUTER QUADRANT OF FEMALE BREAST 174.5 MALIGNANT NEOPLASM OF LOWER-OUTER QUADRANT OF FEMALE BREAST 174.6 MALIGNANT NEOPLASM OF AXILLARY TAIL OF FEMALE BREAST 174.8 MALIGNANT NEOPLASM OF OTHER SPECIFIED SITES OF FEMALE BREAST 174.9 MALIGNANT NEOPLASM OF BREAST (FEMALE) UNSPECIFIED SITE 175.0 MALIGNANT NEOPLASM OF NIPPLE AND AREOLA OF MALE BREAST 175.9 MALIGNANT NEOPLASM OF OTHER AND UNSPECIFIED SITES OF MALE BREAST 196.3 SECONDARY AND UNSPECIFIED MALIGNANT NEOPLASM OF LYMPH NODES OF AXILLA AND UPPER LIMB 198.2 SECONDARY MALIGNANT NEOPLASM OF SKIN 198.81 SECONDARY MALIGNANT NEOPLASM OF BREAST 199.1 OTHER MALIGNANT NEOPLASM OF UNSPECIFIED SITE 217 BENIGN NEOPLASM OF BREAST 233.0 CARCINOMA IN SITU OF BREAST 238.3 NEOPLASM OF UNCERTAIN BEHAVIOR OF BREAST 239.2 NEOPLASM OF UNSPECIFIED NATURE OF BONE SOFT TISSUE AND SKIN 239.3 NEOPLASM OF UNSPECIFIED NATURE OF BREAST 610.0 SOLITARY CYST OF BREAST 610.1* DIFFUSE CYSTIC MASTOPATHY 610.2* FIBROADENOSIS OF BREAST 610.3* FIBROSCLEROSIS OF BREAST 610.4* MAMMARY DUCT ECTASIA 610.8* OTHER SPECIFIED BENIGN MAMMARY DYSPLASIAS 610.9* BENIGN MAMMARY DYSPLASIA UNSPECIFIED 611.0 INFLAMMATORY DISEASE OF BREAST 611.1 HYPERTROPHY OF BREAST 611.2* FISSURE OF NIPPLE 611.3* FAT NECROSIS OF BREAST 611.4* ATROPHY OF BREAST -6- 611.5* GALACTOCELE 611.6* GALACTORRHEA NOT ASSOCIATED WITH CHILDBIRTH 611.71 MASTODYNIA 611.72 LUMP OR MASS IN BREAST 611.79 OTHER SIGNS AND SYMPTOMS IN BREAST 611.89* OTHER SPECIFIED DISORDERS OF BREAST 611.9* UNSPECIFIED BREAST DISORDER 612.0 DEFORMITY OF RECONSTRUCTED BREAST 612.1 DISPROPORTION OF RECONSTRUCTED BREAST 793.80 UNSPECIFIED ABNORMAL MAMMOGRAM 793.81 MAMMOGRAPHIC MICROCALCIFICATION 793.82 INCONCLUSIVE MAMMOGRAM 793.89 OTHER (ABNORMAL) FINDINGS ON RADIOLOGICAL EXAMINATION OF BREAST 996.54 MECHANICAL COMPLICATION OF BREAST PROSTHESIS 996.69 INFECTION AND INFLAMMATORY REACTION DUE TO OTHER INTERNAL PROSTHETIC DEVICE IMPLANT AND GRAFT V10.3 PERSONAL HISTORY OF MALIGNANT NEOPLASM OF BREAST -7- Bone Densities (L26385) ICD-9-CM code 733.13 should be reported for collapse of vertebrae NOS. ICD-9-CM code 793.7 should be reported as a secondary diagnosis when DXA is performed for subsequent monitoring following a BMM performed by another modality. ICD-9-CM code V45.77 should be reported for women s/p oophorectomy. ICD-9-CM code V58.65 should be reported for an individual on glucocorticoid therapy. ICD-9-CM code V58.69 should be reported for DXA testing while taking medicines for osteoporosis/osteopenia. ICD-9-CM code V67.51 should be reported for an individual who has COMPLETED drug therapy for osteoporosis and is being monitored for response to therapy. ICD-9-CM code 733.90 should be reported to indicate osteopenia, (only when billing 77080-DXA), when used to follow treatment with FDA approved osteoporosis medications. For Bone Density CPT 77080 Only: 255.0 CUSHING'S SYNDROME 733.00 OSTEOPOROSIS UNSPECIFIED 733.01 SENILE OSTEOPOROSIS 733.02 IDIOPATHIC OSTEOPOROSIS 733.03 DISUSE OSTEOPOROSIS 733.09 OTHER OSTEOPOROSIS 733.90 DISORDER OF BONE AND CARTILAGE UNSPECIFIED V58.65 LONG-TERM (CURRENT) USE OF STEROIDS V58.69 LONG-TERM (CURRENT) USE OF OTHER MEDICATIONS V67.51 FOLLOW-UP EXAMINATION FOLLOWING COMPLETED TREATMENT WITH HIGH-RISK MEDICATION NOT ELSEWHERE CLASSIFIED These following diagnoses may support medical necessity for CPT codes 77078, 77079, 77080, 77081, 77083, 76977 and G0130, when these tests are performed for bone mass density screening for potential osteopenia/osteoporosis in qualified beneficiaries with estrogen deficiency, vertebral abnormalities/fractures, primary hyperparathyroidism or glucocorticoid administration 252.01 PRIMARY HYPERPARATHYROIDISM 256.2 POSTABLATIVE OVARIAN FAILURE 256.31 PREMATURE MENOPAUSE 256.39 OTHER OVARIAN FAILURE 259.3 ECTOPIC HORMONE SECRETION NOT ELSEWHERE CLASSIFIED 627.0 PREMENOPAUSAL MENORRHAGIA 627.1 POSTMENOPAUSAL BLEEDING 627.2 SYMPTOMATIC MENOPAUSAL OR FEMALE CLIMACTERIC STATES 627.3 POSTMENOPAUSAL ATROPHIC VAGINITIS 627.4 SYMPTOMATIC STATES ASSOCIATED WITH ARTIFICIAL MENOPAUSE -8- 627.8 OTHER SPECIFIED MENOPAUSAL AND POSTMENOPAUSAL DISORDERS 627.9 UNSPECIFIED MENOPAUSAL AND POSTMENOPAUSAL DISORDER 733.13 PATHOLOGICAL FRACTURE OF VERTEBRAE 756.51 OSTEOGENESIS IMPERFECTA 758.6 GONADAL DYSGENESIS 793.7 NONSPECIFIC (ABNORMAL) FINDINGS ON RADIOLOGICAL AND OTHER EXAMINATION OF MUSCULOSKELETAL SYSTEM 805.00 CLOSED FRACTURE OF CERVICAL VERTEBRA UNSPECIFIED LEVEL 805.01 CLOSED FRACTURE OF FIRST CERVICAL VERTEBRA 805.02 CLOSED FRACTURE OF SECOND CERVICAL VERTEBRA 805.03 CLOSED FRACTURE OF THIRD CERVICAL VERTEBRA 805.04 CLOSED FRACTURE OF FOURTH CERVICAL VERTEBRA 805.05 CLOSED FRACTURE OF FIFTH CERVICAL VERTEBRA 805.06 CLOSED FRACTURE OF SIXTH CERVICAL VERTEBRA 805.07 CLOSED FRACTURE OF SEVENTH CERVICAL VERTEBRA 805.08 CLOSED FRACTURE OF MULTIPLE CERVICAL VERTEBRAE 805.10 OPEN FRACTURE OF CERVICAL VERTEBRA UNSPECIFIED LEVEL 805.11 OPEN FRACTURE OF FIRST CERVICAL VERTEBRA 805.12 OPEN FRACTURE OF SECOND CERVICAL VERTEBRA 805.13 OPEN FRACTURE OF THIRD CERVICAL VERTEBRA 805.14 OPEN FRACTURE OF FOURTH CERVICAL VERTEBRA 805.15 OPEN FRACTURE OF FIFTH CERVICAL VERTEBRA 805.16 OPEN FRACTURE OF SIXTH CERVICAL VERTEBRA 805.17 OPEN FRACTURE OF SEVENTH CERVICAL VERTEBRA 805.18 OPEN FRACTURE OF MULTIPLE CERVICAL VERTEBRAE 805.2 CLOSED FRACTURE OF DORSAL (THORACIC) VERTEBRA WITHOUT SPINAL CORD INJURY 805.3 OPEN FRACTURE OF DORSAL (THORACIC) VERTEBRA WITHOUT SPINAL CORD INJURY 805.4 CLOSED FRACTURE OF LUMBAR VERTEBRA WITHOUT SPINAL CORD INJURY 805.5 OPEN FRACTURE OF LUMBAR VERTEBRA WITHOUT SPINAL CORD INJURY 805.6 CLOSED FRACTURE OF SACRUM AND COCCYX WITHOUT SPINAL CORD INJURY 805.7 OPEN FRACTURE OF SACRUM AND COCCYX WITHOUT SPINAL CORD INJURY 805.8 CLOSED FRACTURE OF UNSPECIFIED PART OF VERTEBRAL COLUMN WITHOUT SPINAL CORD INJURY 805.9 OPEN FRACTURE OF UNSPECIFIED PART OF VERTEBRAL COLUMN WITHOUT SPINAL CORD INJURY 806.00 CLOSED FRACTURE OF C1-C4 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY 806.01 CLOSED FRACTURE OF C1-C4 LEVEL WITH COMPLETE LESION OF CORD -9- 806.02 CLOSED FRACTURE OF C1-C4 LEVEL WITH ANTERIOR CORD SYNDROME 806.03 CLOSED FRACTURE OF C1-C4 LEVEL WITH CENTRAL CORD SYNDROME 806.04 CLOSED FRACTURE OF C1-C4 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY 806.05 CLOSED FRACTURE OF C5-C7 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY 806.06 CLOSED FRACTURE OF C5-C7 LEVEL WITH COMPLETE LESION OF CORD 806.07 CLOSED FRACTURE OF C5-C7 LEVEL WITH ANTERIOR CORD SYNDROME 806.08 CLOSED FRACTURE OF C5-C7 LEVEL WITH CENTRAL CORD SYNDROME 806.09 CLOSED FRACTURE OF C5-C7 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY 806.10 OPEN FRACTURE OF C1-C4 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY 806.11 OPEN FRACTURE OF C1-C4 LEVEL WITH COMPLETE LESION OF CORD 806.12 OPEN FRACTURE OF C1-C4 LEVEL WITH ANTERIOR CORD SYNDROME 806.13 OPEN FRACTURE OF C1-C4 LEVEL WITH CENTRAL CORD SYNDROME 806.14 OPEN FRACTURE OF C1-C4 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY 806.15 OPEN FRACTURE OF C5-C7 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY 806.16 OPEN FRACTURE OF C5-C7 LEVEL WITH COMPLETE LESION OF CORD 806.17 OPEN FRACTURE OF C5-C7 LEVEL WITH ANTERIOR CORD SYNDROME 806.18 OPEN FRACTURE OF C5-C7 LEVEL WITH CENTRAL CORD SYNDROME 806.19 OPEN FRACTURE OF C5-C7 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY 806.20 CLOSED FRACTURE OF T1-T6 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY 806.21 CLOSED FRACTURE OF T1-T6 LEVEL WITH COMPLETE LESION OF CORD 806.22 CLOSED FRACTURE OF T1-T6 LEVEL WITH ANTERIOR CORD SYNDROME 806.23 CLOSED FRACTURE OF T1-T6 LEVEL WITH CENTRAL CORD SYNDROME 806.24 CLOSED FRACTURE OF T1-T6 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY 806.25 CLOSED FRACTURE OF T7-T12 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY 806.26 CLOSED FRACTURE OF T7-T12 LEVEL WITH COMPLETE LESION OF CORD 806.27 CLOSED FRACTURE OF T7-T12 LEVEL WITH ANTERIOR CORD SYNDROME 806.28 CLOSED FRACTURE OF T7-T12 LEVEL WITH CENTRAL CORD SYNDROME 806.29 CLOSED FRACTURE OF T7-T12 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY 806.30 OPEN FRACTURE OF T1-T6 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY 806.31 OPEN FRACTURE OF T1-T6 LEVEL WITH COMPLETE LESION OF CORD 806.32 OPEN FRACTURE OF T1-T6 LEVEL WITH ANTERIOR CORD SYNDROME 806.33 OPEN FRACTURE OF T1-T6 LEVEL WITH CENTRAL CORD SYNDROME 806.34 OPEN FRACTURE OF T1-T6 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY 806.35 OPEN FRACTURE OF T7-T12 LEVEL WITH UNSPECIFIED SPINAL CORD INJURY 806.36 OPEN FRACTURE OF T7-T12 LEVEL WITH COMPLETE LESION OF CORD - 10 - 806.37 OPEN FRACTURE OF T7-T12 LEVEL WITH ANTERIOR CORD SYNDROME 806.38 OPEN FRACTURE OF T7-T12 LEVEL WITH CENTRAL CORD SYNDROME 806.39 OPEN FRACTURE OF T7-T12 LEVEL WITH OTHER SPECIFIED SPINAL CORD INJURY 806.4 CLOSED FRACTURE OF LUMBAR SPINE WITH SPINAL CORD INJURY 806.5 OPEN FRACTURE OF LUMBAR SPINE WITH SPINAL CORD INJURY 806.60 CLOSED FRACTURE OF SACRUM AND COCCYX WITH UNSPECIFIED SPINAL CORD INJURY 806.61 CLOSED FRACTURE OF SACRUM AND COCCYX WITH COMPLETE CAUDA EQUINA LESION 806.62 CLOSED FRACTURE OF SACRUM AND COCCYX WITH OTHER CAUDA EQUINA INJURY 806.69 CLOSED FRACTURE OF SACRUM AND COCCYX WITH OTHER SPINAL CORD INJURY 806.70 OPEN FRACTURE OF SACRUM AND COCCYX WITH UNSPECIFIED SPINAL CORD INJURY 806.71 OPEN FRACTURE OF SACRUM AND COCCYX WITH COMPLETE CAUDA EQUINA LESION 806.72 OPEN FRACTURE OF SACRUM AND COCCYX WITH OTHER CAUDA EQUINA INJURY 806.79 OPEN FRACTURE OF SACRUM AND COCCYX WITH OTHER SPINAL CORD INJURY 806.8 CLOSED FRACTURE OF UNSPECIFIED VERTEBRA WITH SPINAL CORD INJURY 806.9 OPEN FRACTURE OF UNSPECIFIED VERTEBRA WITH SPINAL CORD INJURY E932.0 ADRENAL CORTICAL STEROIDS CAUSING ADVERSE EFFECTS IN THERAPEUTIC USE V45.77 ACQUIRED ABSENCE OF ORGAN GENITAL ORGANS V49.81 ASYMPTOMATIC POSTMENOPAUSAL STATUS (AGE-RELATED) (NATURAL) V58.65 LONG-TERM (CURRENT) USE OF STEROIDS - 11 -