Uncomplicated Symptomatic Urinary Tract Infection (PDF 71KB)
advertisement
")
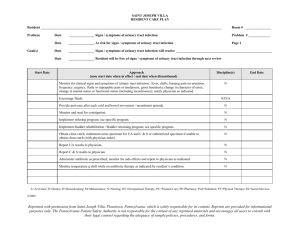
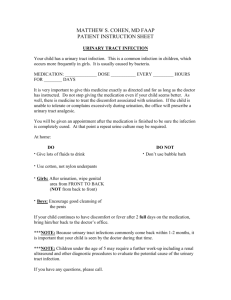
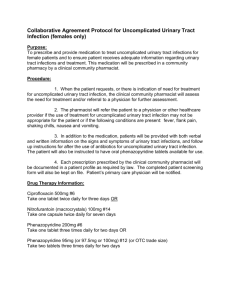
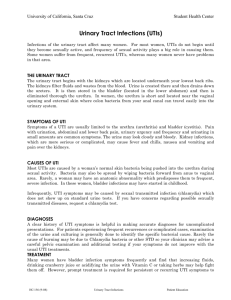
Uncomplicated Symptomatic Urinary Tract Infection Urinary Tract Infections – Urinary tract infections (UTI – also known as cystitis) are a bacterial infection of the lower urinary tract or bladder. Infections in the elderly can range from being asymptomatic to bactereamia. The most common organism isolated is gram-negative bacilli with E. coli infection in up to 20-50% of presentations. Other common organisms include Klebsiella, Enterococci, group B Streptococcus and Proteus mirabilis. UTIs are a common infection in the elderly and women have a higher prevalence. The expected outcome of use of this clinical guideline is rapid and effective relief from symptoms and eradication of bacteria from urinary tract, prevention of reoccurrence of infection, reduction in hospitalisation rates, improved morbidity and reduce the risk and rate of mortality. The diagnosis of UTI in the elderly can be difficult, treatment of a resident with cloudy or malodorous urine without symptoms does not require treatment. There is a worldwide emergence of multi-resistant E. Coli associated with UTIs. Uncomplicated Symptomatic Urinary tract Infection.doc Page 1 of 11 Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection SCOPE OF PRACTICE PRACTITIONER Nurse Practitioner – Aged Care Medical Practitioner ± Nurse Practitioner Uncomplicated Symptomatic Urinary tract Infection.doc SCOPE OUTOMES Resident showing signs and symptoms of uncomplicated UTI The NP will refer all Hall & Prior residents outside their scope of practice, to a medical practitioner. Page 2 of 11 • The expected outcome of use of this clinical guideline is rapid and effective relief from symptoms and eradication of bacteria from the urinary tract, prevention of reoccurrence of infection, reduction in hospitalisation rates, improved morbidity and reduce the risk and rate of mortality. • Upon failure of treatment, complications of infection or recurrence of infection, referral to an urologist is required.6 Nurse practitioners should consider referral to continence advisor if incontinence is a contributing factor. Referral to occupational therapist and/or physiotherapist should be considered if lack of mobility or hygiene aids are contributing factors. Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection RESIDENT’S ASSESSMENT RESIDENT’S HISTORY SCOPE Presenting symptoms Signs and symptoms of uncomplicated UTI in the elderly: dysuria, frequent urination with small volume, nocturia, urgency, haematuria,loin pain suprapubic discomfort, confusion, delirium, falls, immobility or anorexia, temperature may be elevated . • Relevant medical, surgical and obstetric history • Constructing and ruling out related differential diagnoses to specific pathophysiology identified. • Identify residents not suitable for treatment by NP with CPG and direct to GP . Previous medical history Medications Other relevant information PHYSICAL Ax Usual physical examination Indications for specific examinations Uncomplicated Symptomatic Urinary tract Infection.doc OUTCOMES • Current Medications Allergies, previous UTI history, continence, nutrition & hydration, skin integrity, mobility, cognition, behaviour SCOPE Gaining comprehensive and holistic data in order to prescribe appropriate diagnostics and interventions related to indicators identified in assessment. Identify resident suitable for treatment by NP with clinical practice guidelines (CPG) OUTCOMES Record findings: vital signs, genitourinary assessment, pain assessment, other symptoms may be present vaginal discharge or haematuria. Visual assessment of external genitalia, digital rectal examination (DRE) at NPs discretion Page 3 of 11 • • • • Correct diagnosis, provision of effective disease and symptomatic eradication/relief. Consideration of previous history of UTIs. Recent or present instrumentation. Pre-disposing and associated conditions detected and considered to determine UTI Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection SCOPE INDICATIONS INVESTIGATIONS Routine investigations Laboratory/diagnostics used for diagnosis and identification of organism: urinalysis (positive blood/protein/nitrites/leucocytes), clean or sterile mid stream urine specimen for microculture and sensitivity testing, FBC (if indicative of bacteraemia). Pathology To determine underlying organism, severity and sensitivity of organism. OUTCOMES • Results from all investigations will be used when determining future management of the resident’s urine which is positive for nitrates and leucocytes will be sent for MC and S. • Accurate diagnosis will be made in the presence of signs and symptoms. • Correct diagnosis will be determined • Correct pharmacotherapy will be prescribed based on sensitivity of organism. • A diagnosis of UTI will be considered in an elderly confused resident . • Treatment will be made with correct antibiotics Urine MCS Imaging Bladder Scan for detection of residual urine +/retention of urine . Haematology / Biochemistry If suspected pyelonephritis only. FBC, U&E Other Investigations nil Uncomplicated Symptomatic Urinary tract Infection.doc Page 4 of 11 Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection FOLLOW UP AND EDUCATION INTERVENTION Pharmacotherapeutics SCOPE OUTCOMES Asymptomatic UTIs do not require treatment. Symptomatic UTIs require a combination of pharmacological and non-pharmacological interventions. Upon diagnosis, identification of the organism and it’s sensitivities, antibiotic treatment is to be commenced. *see formulary for more detail. • • • • Eradication of infection Prevention of recurrence of infection Symptomatic relief Prevention of complications Prophylactic maintenance is recommended for resident’s with recurrent UTIs. Use of cranberry and/or prophylactic antibiotics and intravaginal oestrogen should be considered post treatment. Non-pharmacological Uncomplicated Symptomatic Urinary tract Infection.doc Non-pharmacological interventions that should be considered to help manage and prevent further infections include education of resident’s and nursing/care staff regarding effective toilet hygiene (wipe front to back), wash skin around genitalia and anus daily, shower rather than bathe, regular and complete emptying of bladder, voiding and hygiene post sexual intercourse and adequate hydration.1,8 Avoiding irritants - fragrance/feminine deodorisers, synthetic underwear, carbonated, caffeinated, alcoholic and acidic foods and fluids are also effective management strategies. Heat packs can be applied to lower abdomen to aid in relieving discomfort/pain. Page 5 of 11 Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection FOLLOW UP AND EDUCATION INTERVENTION SCOPE Follow up appointments Resident’s needs to be reviewed daily post commencing antibiotic therapy to reassess symptoms and monitor for any complications or adverse reactions to therapy. Follow up MSU is required at completion date of antibiotic therapy to validate eradication of infection and determine whether further antimicrobial treatment is required. An evidence base care plan should be developed. Nurse practitioners are required to follow up on all referrals to allied health/specialists and reinforce education and management strategies to prevent recurrent infections. Resident’s/staff education Letters Uncomplicated Symptomatic Urinary tract Infection.doc OUTCOMES • Underlying disease will be detected at follow up. • Upon failure of treatment, complications of infection or recurrence of infection, referral to a GP is required. • Nurse practitioners should consider referral to continence advisor if incontinence is a contributing factor. • Resident with complications outside the scope of practice of the NP are referred to appropriate providers. Nursing staff and resident’s need to be educated about the treatment plan, infection control, importance of medication intervention & compliance and follow up procedures (i.e. repeat diagnostics, follow up appointments). • Optimise independence, awareness and education Optimise compliance with treatment Optimise eradication of infection and prevent recurrence of infection Letter to residents GP • Page 6 of 11 • • Letters/progress reports are provided at the discretion of the NP Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection PHARMACOTHERAPY Uncomplicated UTIs should commence first line oral antibioticstrimethoprim or cephalexin for residents with penicillin hypersensitivity or amoxycillin/clavulanate Duration of treatment depends on severity of infection, aetiology of infection, antibiotic treatment, antibiotic resistance and gender of the resident’s. Female resident’s are recommended 3-7 days treatment, males 14 days. If symptomatic management of suprapubic discomfort and dysuria is required paracetamol 500mg Prophylactic maintenance is recommended for resident’s with recurrent UTIs. Use of cranberry and/or prophylactic antibioticsmay be ordered.3,5,6,7,9 Prophylactic treatment ascorbic acid; and/or oestriol 1 pessary PV 1-2 times weeklyrefer to GP for review and consultation Uncomplicated Symptomatic Urinary tract Infection.doc Page 7 of 11 Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection PHARMACOTHERAPY FORMULARY S4 st Cephalexin 1st line treatment Trimethoprim 1 line treatment Drug (generic name): trimethoprim Drug (generic name): cephalexin Poisons schedule: schedule 4 Poisons schedule: schedule 4 Therapeutic class: 8(g) other antibiotics Therapeutic class: 8(b) cephalosporins Dosage range: 300mg Dosage range: 500mg orally / 12 hourly Route: oral Route: oral Frequency of administration: daily (nocte) Frequency of administration: 6-12 hourly in uncomplicated UTI Duration of order: females 3 days, males 14 days Duration of order: 5 days Actions: competitively inhibits bacterial folate production, is Special Consideration : Renal impairment requires dose bacteriostatic reduction . Indications for use: empirical Rx of lower UTIs in men and non- Actions: intervenes in bacteria cell wall peptidoglycan synthesis pregnant women . Indications for use: staphylococcal & streptococcal infections Precautions : severe renal impairment, allergy to trimethoprim, (when mild-moderate allergy to penicillins), susceptible gram avoid use in particular blood dyscrasias and skin disorders negative bacterial UTIs, epididymo-orchitis Adverse drug reactions: nausea, vomiting, hyperkalaemia, fever, Contraindications for use: allergy to cephalosporins or rash, itch, folate deficiency (especially long term) carbapenems and penicillins (5%-10% cross reaction) Adverse drug reactions: nausea, diarrhoea, electrolyte imbalance, rash Uncomplicated Symptomatic Urinary tract Infection.doc Page 8 of 11 Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection PHARMACOTHERAPY amoxycillin trihydrate: potassium clavulanate treatment norfloxacin Drug (generic name): amoxycillin with clavulanic acid Drug (generic name): norfloxacin Poisons schedule: schedule 4 Poisons schedule: schedule 4 Therapeutic class: 8(a) penicillins Therapeutic class: 8(e) quinolones Dosage range: 500mg/125mg, 875/125mg Dosage range: 400mg Route: oral Route: oral 1hr before food or 2hrs after Frequency of administration:12 hourly Frequency of administration: 12 hourly Duration of order: 5 days (UTI) Duration of order: 3 days Actions: intervenes in bacteria cell wall peptidoglycan synthesis, Actions: blocks DNA gyrase & topoisomerase IV, thus inhibiting is bactericidal DNA synthesis, is bactericidal Indications for use: UTI, epididymo-orchitis, otitis media, Indications for use: UTI, shigellosis, traveller’s diarrhoea, sinusitis, hospital acquired pneumonia, bites & clenched fist campylobacter enteritis, prostatitis (when other AB options injuries, melioidosis ineffective or contraindicated) Contraindications for use: allergy to penicillins, cephalosporins Contraindications for use: allergy to quinolones or carbapenems, cholestatic jaundice, hepatic dysfunction r/t Adverse drug reactions: nausea, vomiting, diarrhoea, abdo. amoxycillin with clavulanate or ticarcillin with clavulanate pain, dyspepsia, rash, itch. Adverse drug reactions: allergy, diarrhoea, nausea, rash, superinfection, transient increase in liver enzymes & bilirubin Uncomplicated Symptomatic Urinary tract Infection.doc Page 9 of 11 Created on 7/11/2012 1:20:00 PM Uncomplicated Symptomatic Urinary Tract Infection PHARMACOTHERAPY paracetamol Oestriol (refer to GP) Drug (generic name): paracetamol Drug (generic name): oestriol Poisons schedule: unscheduled Poisons schedule: schedule 4 Therapeutic class: 4(b) simple analgesics and antipyretics Therapeutic class:7(d) topical vaginal medication Dosage range: 500mg-1g Dosage range: 0.5mg Route: oral Route: per vagina (pessary) Frequency of administration: 6 hourly ,max 4g daily Frequency of administration: daily/12 hourly Duration of order: as required Duration of order: long term Actions: inhibition of prostaglandin synthesis Actions: oestrogen replacement Indications for use: mild-moderate pain, migraine, headache, Indications for use: oestrogen deficiency, menopausal fever, muscular pain symptoms, UTI prophylaxis, adjunct to vaginal surgery Contraindications for use: nil Contraindications for use: undiagnosed vaginal bleeding, VTE, Adverse drug reactions: (rare) rash, drug fever, mucosal lesions, thrombophlebitis, porphyria, endometriosis, liver dysfunction, neutro/pancyto/thrombocytopenia. Acute overdose –hepatitis, disturbed lipid metabolism renal tubular necrosis, hypoglycaemia. Adverse drug reactions: local irritation, cystitis like symptoms, breast pain, thromboembolism, cervical/menstrual changes, dementia, increased size of uterine fibroids Uncomplicated Symptomatic Urinary tract Infection.doc Page 10 of 11 Created on 7/11/2012 1:20:00 PM REFERENCES 1. Clinical Practice Guidelines for Nurses in Primary Care [monograph online]. 2000 [cited 2006 Apr 12]. Available from: http://www.hc-sc.gc.ca/msb/fnihp. 2. Tal S, Guller V, Levi S, Bardenstein R, Berger D, Gurevich I, Gurevich A. Profile and prognosis of febrile elderly resident’s with bacteremic urinary tract infection. Journal of Infection [serial online]. 2005 [cited 2006 Oct 20]; 50:296-305. Available from: ScienceDirect. 3. The Royal Australian College of General Practitioners. Medical Care of Older Persons in Residential Aged Care Facilities. 4th ed. South Melbourne: The Royal Australian College of General Practitioners; 2005. 4. Wagenlehner FM, Naber KG. Treatment of bacterial urinary tract infections: presence and future. European Urology [serial online]. 2006 [cited 2006 Oct 20]; 49:235-244. Available from: ScienceDirect. 5. Dartnell JG, editor. Therapeutic guidelines: antibiotic. 12th ed. Victoria: Therapeutic Guidelines Limited; 2003. 6. Rossi S, editor. Australian medicines handbook. Adelaide SA: Australian Medicines Handbook Pty Ltd; 2011. 7. eMIMS MIMS. MIMS medicine information [standard online]. c2005 [cited 2006 Oct 20]. Available from: eMIMS MIMS Online. 8. Hughes J. Urinary tract infections. Proceedings from The Infectious Diseases Module Lectures; 2006 Oct 9-16; Bentley, Perth: Curtin University of Technology; n.d. 9. McMurdo M, Bissett L, Price R, Phillips G, Crombie I. Does ingestion of cranberry juice reduce symptomatic urinary tract infections in older people in hospital? A double-blind, placebo-controlled trial. Age and Ageing. 2005; 34: 256-261. 10. etg complete( internet ). Melbourne : Therapeutic Guidelines Limited; 2011 Nov Accessed 2001at http://etg.com.au/ref/ref 11. Grayson ML, McDonald M, Gibson K, Athan E, Munckhof WJ, Paull P, et al. Once-daily intravenous cefazolin plus oral probenecid is equivalent to once-daily intravenous ceftriaxone plus oral placebo for the treatment of moderate-to-severe cellulitis in adults. Clinical Infectious Diseases. 2002; 34(11): 1440-1448. 12. Ginsberg MB. Cellulitis: analysis of 101 cases and review of the literature. Southern Medical Journal. 1981; 74(5): 530-533. 13. Fleisher G, Ludwig S. Cellulitis: a prospective study. Annals of Emergency Medicine. 1980; 9(5): 246-249. 14. Kennedy M L, Fletcher KR, Plank LM. Management guidelines for nurse practitioners working with older adults. 2nd ed. Philadelphia: F. A. Davis; 2004. 15. Reuben DB, Herr KA, Pacala JT. Geriatrics at your fingertips. 6th ed. Malden, MA: Blackwell; 2004. 16. McKinnon PS, Paladino JA, Grayson ML, Gibbons GW, Karchmer AW. Cost-effectiveness of ampicillin/su;bactam versus imipenum/cilastatin in the treatment of limb-threatening foot infections in diabetic resident’s. Clinical Infection Diseases. 1997; 24(1): 57-63. 17. Friedlaender MH. A review of the causes and treatment of bacterial and allergic conjunctivitis. Clinical Therapeutics. 1995; 17(5): 800-810. 18. Wan W L, Farkas GC, May WN, Robin JB. The clinical characteristics and course of adult gonococcal conjunctivitis. American Journal of Ophthalmology. 1986; 102(5): 575-583. Uncomplicated Symptomatic Urinary tract Infection.doc Page 11 of 11 Created on 7/11/2012 1:20:00 PM