Thymosin Alpha 1 - Wiley Online Library
advertisement

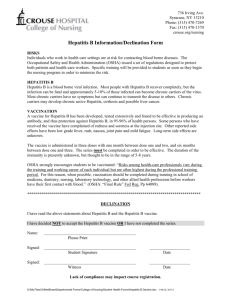
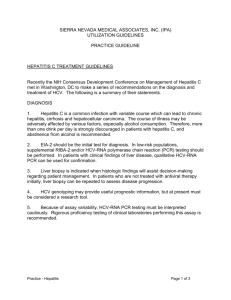
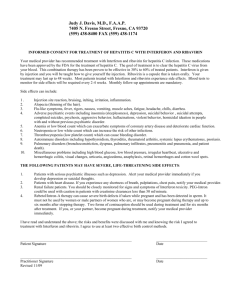
Thymosin Alpha 1 From Bench to Bedside ENRICO GARACI,a CARTESIO FAVALLI,a FRANCESCA PICA,a PAOLA SINIBALDI VALLEBONA,a ANNA TERESA PALAMARA,b CLAUDIA MATTEUCCI,c PASQUALE PIERIMARCHI,c ANNALUCIA SERAFINO,c ANTONIO MASTINO,d FRANCESCO BISTONI,e LUIGINA ROMANI,e AND GUIDO RASIc a University of Rome Tor Vergata, Rome, Italy b University of Rome La Sapienza, Rome, Italy c CNR, Rome, Institute of Neurobiology and Molecular Medicine, Rome, Italy d University of Messina, Messina, Italy e University of Perugia, Perugia, Italy ABSTRACT: After the initial dramatic effects, observed in a Lewis lung carcinoma animal model, using a combination of thymosin alpha 1 (T1) and interferon (IFN) after cyclophosphamide, a number of other preclinical models in mice (Friend erythroleukemia and B16 melanoma) and in rats (DHD/K12 colorectal cancer liver metastasis) have confirmed the efficacy of the combination therapy with T1 and either IFN or IL-2 plus chemotherapy. These results provided the scientific foundation for the first clinical trials using T1 in combination with BRMs and/or chemotherapy. Pivotal trials in advanced non-small cell lung cancer (NSCLC) and melanoma with T1 and IFN- low doses after cis-platinum or dacarbazine produced the first evidence of the high potentiality of this approach in the treatment of human cancer. The combination of T1 and IFN- was also used in patients affected by chronic B and C hepatitis including IFN-nonresponders and infected by precore mutants or genotype 1b. Further studies demonstrated additional biological activities clarifying the mechanism of action of T1, partially explaining the synergism with IFN. It has been shown the capacity of activating infected dendritic cells through Toll-like receptor signaling, thus influencing the inflammation balance, and of increasing the expression of tumor, viral, and major histocompatibility complex (MHC) I antigens. Dose–response studies suggested the possibility of improving the efficacy of this molecule reducing the overall toxic. Based on these information Address for correspondence: Guido Rasi, M.D., CNR, Institute of Neurobiology and Molecular Medicine, Via Fosso del Cavaliere, 100, 00133, Rome, Italy. Voice: + 39-06-49934486; fax: + 39-06233249504. guido.rasi@artov.inmm.cnr.it C 2007 New York Academy of Sciences. Ann. N.Y. Acad. Sci. 1112: 225–234 (2007). doi: 10.1196/annals.1415.044 225 226 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES two clinical trials are ongoing: a large phase II on advanced melanoma patients treated with T1 at different doses after dacarbazine and a phase III one, on IFN-resistant hepatitis C virus (HCV) patients treated with a triple combination (IFN, ribavirin, and T1). KEYWORDS: thymosin alpha 1; preclinical models; clinical trials INTRODUCTION After 1985,1 when thymosin alpha 1 (T1) was first used in a clinical trial, an impressive number of data has been produced supporting the potential clinical benefits of this molecule. Since then a number of pivotal clinical trials have been carried out for the treatment of cancer and chronic viral hepatitis using T1 in combination with chemotherapeutic agents or with interferon (IFN). The results, although partial, have always been encouraging and warranted the actual ongoing phase II and phase III large trial on advanced melanoma and on chronic C hepatitis for IFN-resistant patients. The continuous progress of the knowledge about both, the mechanisms of T1 action on one side, and the mechanisms of tumor progression and viral persistence on the other, further supported the potentiality of this molecule, also suggesting better treatment schedules and new possible indications. The effects described in many papers indicate T1 as a powerful molecule able to activate or boost the immune system by many different ways. The most relevant in vitro effects are listed in TABLE 1. These findings encouraged the use of T1 as an adjuvant for cancer and infectious disease. USE OF T1 IN CANCER MODELS In 1990, our group2 demonstrated the possibility to completely eradicate Lewis lung carcinoma in mice using T1, followed by murine IFN-/ after cyclophosphamide. The schedule was to insert a cycle of immunotherapy consisting of 4 days T1 treatment followed by 1 day of IFN- (or / in mice according to the availability) between two cycles of “standard” chemotherapy, according to the scheme illustrated in FIGURE 1. This schedule of combination treatment proved to be highly active in curing established tumors, whereas single treatments were not effective. The concept of combining a sequence of immunotherapy (T1 plus a cytokine) after chemotherapy was further developed on the assumption that chemotherapy on the one hand was advantageous in reducing the tumor mass but on the other induced a marked depression of the immune response. Moreover, the potential positive effects of powerful cytokines, such as IFN and GARACI et al. 227 TABLE 1. List of the most relevant in vitro effects of T1 Cytokines and receptors –IL-12, IL-2 increase –IFN- increase –Expression of high-affinity IL-2R (CD25) –IL-4 inhibition T cell proliferation/differentiation –Stimulates CD34+ stem cells into CD3 + 4+ cells –Stimulates CD4+ and CD8+ cell proliferation –Increases of CD4+ and CD45RO+ (memory T cells) –Stimulates NK-cell activity Effect on tumor/infected cells –Increases MHC I –Increases tumor antigen expression –Increases GSH levels FIGURE 1. Treatment schedule of combination therapies in cancer. interleukin-2 (IL-2), could not fully be exploited because of the toxicity shown at the effective doses. The combination therapy was aimed at obtaining a synergistic effect by combining T1 with immunoactive molecules at low doses, thus reducing the overall toxicity of the treatment. The results went beyond the expectation and encouraged further experiments. Similar results were obtained in other experimental models: Friend erythroleukemia3 and B16 melanoma4 in mice and DHD/K12 colorectal carcinoma liver metastases in rats,5 as summarized in TABLE 2. Many of the effects listed in the introduction may explain these results, including the boosting of cellular immune responses. However, the increased expression of major histocompatibility complex (MHC) I antigens6 along with the increased tumor antigen expression7 might be the key point for this successful approach as shown in FIGURE 2. In fact, many strategies able to induce or enhance a cytotoxic T-lymphocyte (CTL) response frequently fail to correlate with the expected antitumor effect. The experience in preclinical models was translated into the clinics, performing two clinical trials exactly reproducing the experimental model. Pivotal trials in advanced non-small cell lung cancer (NSCLC)8,9 and in melanoma10 with T1 and low doses IFN- after cis-platinum and dacarbazine, respectively, produced the first evidence of the possibility to enhance the clinical response rate and the survival time by this approach (TABLE 3). 228 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES TABLE 2. Combination therapies in cancer preclinical models Author/Ref Year Tumor Garaci et al.2 1990 Lewis lung carcinoma Garaci et al.3 Rasi et al.5 Pica et al.4 Treatment Responses Cy+T1+ IFN-/ Cure/complete regression NK and CTL increase 1993 Friend Cy+ T1+ Increased survival erythroleukemia IL-2/ IFN-/ NK and CTL increase 1994 DHD/K12 CRC 5-FU + T1+ Increased survival liver metastases IL-2 reduced metastatic spread NK and CTL increase 1998 B16 melanoma Cy + T1 + Increased survival IFN- T1 dose– response effect Animal model Mice Mice Rats Mice Cy = cyclophosphamide; 5-FU = 5 fluorouracil; CRC = colorectal cancer. FIGURE 2. Effect of T1 on CEA antigen expression in WiDr colorectal cancer cell lines. T1 is able to induce CEA overexpression making tumors more visible to lymphocytes. (A) Untreated WiDr cells; (B) WiDr cells treated with T1 (50 ng/mL) for 48 h. USE OF T1 IN INFECTIOUS DISEASES Cancer models demonstrated the powerful action of T1 on the immune system and the synergy between T1 and IFN suggesting a possible use in infections. T1, besides being a potent immune modulator itself, showed a synergistic action with many cytokines (IFN-, IL-2, IFN- ). The abovementioned possibility to upregulate MHC class I antigen expression, by a different pathway from the IFN, provided the first molecular explanation for the synergy. This also disclosed a new action of T1, that is, the ability to act on cells other than the lymphoblastoid cells. Further experiments, in fact demonstrated the possibility to upregulate viral antigens expression both in vitro and in vivo (Palamara, personal data). Furthermore, a direct antiviral GARACI et al. 229 TABLE 3. Clinical experiences with T1 combination therapy in cancer patients Author/ref Garaci et al.8 Year Tumor Treatment Responses (range) 1995 NSCLC DDP/VP-16 + T1+IFN 43% RR 15.7 MST IFO + T1+ IFN 10% RR – TP 9 (6/18) 33% RR – TP 18 (9/53)∗ 25% CR – 50% Expected ∼25% RR 11.5 MST for matching population Salvati et al.9 1996 NSCLC Rasi et al.10 2000 Melanoma DTIC + T1+ IFN Note Reduced toxicity for combination Expected ∼20% for matching population CR = complete response; TP = time to progression (weeks); DDP = cisplatinum; VP-16 = etoposide; RR = response rate; IFO = ifosfamide; MST = median survival time (months); DTIC = decarbazine. ∗ P = 0.0059. action was demonstrated in a model of influenza virus infection and woodchuck hepatitis.11 Based on these data, and with the experience of a preclinical cancer models, a pivotal phase II trial was performed using T1 in combination with low dose of lymphoblastoid interferon- (L-IFN-) in chronic hepatitis B patients. The overall sustained response rate, normal enzyme (ALT) and negative HBV-DNA 6 months after the end of treatment, was greater than expected with IFN alone (46% versus 30%). However, the most important finding was the number of responses observed after the end of treatment whereas a significant number of relapses are what generally takes place. The response raised up to 55% after 18 months and a sustained response12 was also observed in “difficultto-treat patients,” such as previous IFN failures and/or precore mutants. CTL and NK enhancement surely play a role in these results, but, once again, the hypothesis of the increased expression of MHC I antigens could be particularly relevant, given the specific lack of MHC class I antigens expression in HBV-infected hepatocytes. This trial provided the first evidence of the effectiveness of the combined approach and was followed by many other trials13–15 (TABLE 4) that confirmed the initial observations and gave some important indication: evidence of the “late response,” unique of T1 and opposite to IFN, the response also in “IFN nonresponders patients” and in precore mutants, and the dose–response effect (TABLE 5).16–19 After the positive experience on hepatitis B, a pivotal trial with recombinant IFN- and T1 was performed in patients affected by chronic C hepatitis.20 In this trial were included IFN failures and genotype 1b patients. The results gave an encouraging 40% sustained response compared to an expected 15–29% with IFN alone; opening new hope for these diseases also confirmed from other trials (TABLE 6).21–23 230 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES TABLE 4. Clinical experiences with T1 combination therapy in chronic hepatitis B Treatment and duration Author/ref Year Rasi et al.12 1996 T1+L-IFN- (26 weeks) End of treatment Follow- up % Pts n % of responses 52/78 w End points 15 40 (a) 53/60 ALT/DNA HBsAg Saruc et al.13 2002 T1+IFN (c) (52 weeks) 21 87.7 (b) 76 ALT/DNA Saruc et al.14 2003 T1+IFN (c) IFN + 3TC (d) IFN (52 weeks) 27 15 10 74 53 40 70/71 26/20 20/10 ALT/DNA T1 + 3TC 20 Not reported 70 ALT/DNA Chan et al.15 2001 Pts = patients. (a) including IFN failures; HBeAg+; (b) Anti HBe+ patients/naı̈ves; (c) IFN for 52 weeks; (d) Lamivudine 3TC for 78 weeks. TABLE 5. Further clinic experiences in HBV difficult-to-treat patients Author/ref. Andreone et al.16 Zhuang et al.17 You et al.18 Iino et al.19 Year ∗ Treatment (6 months/ 1.6 BW) 1996 T1 vs. IFN 2001 T1 vs. IFN∗ 2006 T1 vs. IFN 2005 T1 0.8 vs. 1.6∗∗ End of treatment % Pts. n of responses Follow up % End points 33 29 vs. 44 48 33 vs. 46 62 31 vs. 45 316 Not reported 41 vs. 25 55 vs. 23.3 48 vs. 27 25 vs. 30 ALT/DNA ALT/DNA ALT/DNA ALT/DNA Pts = patients ∗ Anti HBe+ patients; ∗∗ including IFN failures. A number of hypotheses have been raised about the possible mechanism of action and the most recent findings indicate the dendritic cells and TNF- as two major players in promoting liver injury. Recent works demonstrated the ability of T1 to activate macrophage Th1 responses, through Toll-like receptor signaling, and to promote a regulatory environment for balance of inflammation and tolerance,24,25 and to downregulate macrophages TNF- release (Serafino 2006, personal data; FIG. 3). Taken together these findings better explain the possible role of thymosin in hepatitis C virus (HCV) chronic infection. The pleiotropic function of T1 is well documented by recent studies on transcriptional response to this molecule, performed in human peripheral blood mononuclear cells (PBMCs) using the gene-array technology. By means of this experimental approach T1 has been actually shown to GARACI et al. 231 TABLE 6. Clinical experiences with T1 combination therapy in chronic hepatitis C Author Year Rasi et al.20 1996 Sherman et al.21 Andreone et al.22 Poo et al.23 Treatment and duration T1+ L-IFN 52 weeks 1998 T1+IFN2b vs. IFN2b 26 weeks 2003 T1+IFN2b vs. IFN2b 26 weeks 2004 T1+IFN2b+Ribavirin 24 weeks Pts n Responses (%) E.T. F.U. End points 15 73 40 ALT/RNA 35 37 22 19 23 37 19 64 32 39 14 8 32 21 ALT/RNA ALT/RNA RNA Pts = patients; E.T. = end of treatment response; F.U. = follow-up. End points: normal ALT; RNA nondetectable by PCR. FIGURE 3. Effect of T1 on TNF- release from human macrophages. T1 induces a downregulation of TNF- release from human macrophages. TNF- production after 24 h T1 in vitro treatment (ELISA). upregulate the expression of a plethora of genes related to innate response and to growth factors, cytokines, and chemokines.26 Part of these results is reported in FIGURE 4. The clinical experience is now going to receive a significant contribution by two ongoing major clinical trials. The first is related to the treatment of HCV chronic patients which resulted nonresponders to IFN treatment. Those patients for whom there is no hope of cure, IFN retreatment is the only option with a disappointing response rate of about 5–10%. This study is a phase III trial using a triple combination of T1 plus ribavirin plus pegylated IFN, on the basis of all the knowledge achieved in terms of mechanism and combinations of those molecules. The second is a first-line phase II study on 500 patients with advanced melanoma using dacarbazine followed by T1 plus low dose of IFN. Different arms using high-doses of T1 are included to comply with the overall 232 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES FIGURE 4. Genes regulated by T1 in human lymphocytes. Human PBMCs from healthy donors were cultured in the presence of T1 at 1 g/mL for 48 h and transcriptional response was assayed by gene-array technology. Results for some upregulated genes are reported and expressed as fold change compared to the untreated sample. clinical and experimental experience in melanoma, where a dose effect was documented. In the future it is reasonable to expect further use of this molecule, due to the continuous improvement in the knowledge of different mechanisms and interactions. REFERENCES 1. SCHULOF, R.S., M.J. LLOYD, J. STALLINGS, et al. 1985. Recombinant leukocyte A interferon in B-cell chronic lymphocytic leukemia: in vivo effects on autologous antitumor immunity. J. Biol. Response Mod. 4: 310–323. 2. GARACI, E., A. MASTINO, F. PICA, et al. 1990. Combination treatment using thymosin alpha 1 and interferon after cyclophosphamide is able to cure Lewis lung carcinoma in mice. Cancer Immunol. Immunother. 32: 154–160. 3. GARACI, E., F. PICA, A. MASTINO, et al. 1993. Antitumor effect of thymosin alpha 1/interleukin-2 or thymosin alpha 1/interferon alpha,beta following cyclophosphamide in mice injected with highly metastatic Friend erythroleukemia cells. J. Immunother. Emphasis Tumor Immunol. 13: 7–17. 4. PICA, F., M. FRASCHETTI, C. MATTEUCCI, et al. 1998. High doses of Thymosin alpha 1 enhance the anti-tumor efficacy of combination chemo-immunotherapy for murine B16 melanoma. Anticancer Res. 18(5A): 3571–3578. 5. RASI, G., G. SILECCHIA, P. SINIBALDI-VALLEBONA, et al. 1994. Anti-tumor effect of combined treatment with thymosin alpha 1 and interleukin-2 after 5-fluorouracil in liver metastases from colorectal cancer in rats. Int. J. Cancer 57: 701–705. GARACI et al. 233 6. GIULIANI, C., G. NAPOLITANO, A. MASTINO, et al. 2000. Thymosin-alpha1 regulates MHC class I expression in FRTL-5 cells at transcriptional level. Eur. J. Immunol. 30: 778–786. 7. SINIBALDI VALLEBONA, P., P. PIERIMARCHI, G. MORONI, et al. 2002. Thymalfasin upregulates tumor antigen expression in colorectal cancer cells. ISOBM 23/S1/02 0–55. 8. GARACI, E., M. LOPEZ, G. BONSIGNORE, et al. 1995. Sequential chemoimmunotherapy for advanced non-small cell lung cancer using cisplatin, etoposide, thymosinalpha 1 and interferon-alpha 2a. Eur. J. Cancer 13/14: 2403–2405. 9. SALVATI, F., G. RASI, L. PORTALONE, et al. 1996. Combined treatment with thymosin alpha 1 and low dose interferon alpha after ifosfamide in non-small cell lung cancer: a phase II controlled trial. Anticancer Res. 16: 1001–1004. 10. RASI, G., E. TERZOLI, F. IZZO, et al. 2000. Combined treatment with thymosinalpha1 and low dose interferon-alpha after dacarbazine in advanced melanoma. Melanoma Res. 10: 189–192. 11. GERIN, J.L., B.E. KORBA, P.J. COTE & B.C. TENNANT 1992. A preliminary report of a controlled study of thymosin alpha-1 in the woodchuck model of hepadnavirus infection. Adv. Exp. Med. Biol. 312: 121–123. 12. RASI, G., M.G. MUTCHNICK, D. DI VIRGILIO, et al. 1996. Combination of lowdose lymphoblastoid interferon and thymosin alpha-1 therapy in the treatment of chronic hepatitis B. J. Viral Hepat. 3: 191–196. 13. SARUC, M., H. YUCEYAR, N. KUCUKMETIN, et al. 2002. Combination thymosinalpha 1 and interferon-alpha 2b in the treatment of anti-HBe positive chronic hepatitis B in Turkey. Hepatogastroenterology 49: 798–802. 14. SARUC, M., N. OZDEN, S. AYHAN, et al. 2003. Long-term outcomes of thymosinalpha 1 and interferon alpha-2b combination therapy in patients with hepatitis B. 2003. J. Pharm. Sci. 92: 1386–1395. 15. CHAN, H.L., J.L. TANG, W. TAM & J.J. SUNG. 2001. The efficacy of thymosin in the treatment of chronic hepatitis B virus infection: a meta-analysis. Aliment Pharmacol. Ther. 15: 1899–1905. 16. ANDREONE, P., C. CURSARO, A. GRAMENZI, et al. 1996. A randomized controlled trial of thymosin-alpha 1 versus interferon alfa treatment in patients with hepatitis B e antigen antibody—and hepatitis B virus DNA—positive chronic hepatitis B. Hepatology 24: 774–777. 17. ZHUANG, L., J. YOU, B.Z. TANG, et al. 2001. Preliminary results of hymosin-a1 versus interferon-alpha-treatment in patients with HBeAg negative and serum HBV DNA positive chronic hepatitis B. Word J. Gastroenterol. 7: 407–410. 18. YOU, J., L. ZHUANG, H.Y. CHENG, et al. 2006. Efficacy of thymosin alpha-1 and interferon alpha in treatment of chronic viral hepatitis B: a randomized controlled study. World J. Gastroenterol. 12: 6715–6721. 19. IINO, S., J. TOYOTA, H. KUMADA, et al. 2005. The efficacy and safety of thymosin alpha-1 in Japanese patients with chronic hepatitis B; results from a randomized clinical trial. J. Viral Hepat. 12: 300–306. 20. RASI, G., M.G. MUTCHNICK, D. DI VIRGILIO, et al. 1996. Combination low-dose lymphoblastoid interferon and thymosin alpha 1 therapy in the treatment of chronic hepatitis B. J. Viral Hepat. 3: 191–196. 21. SHERMAN, K.E., M. SJOGREN, R.L. CREAGER, et al. 1998. Combination therapy with thymosin alpha 1 and interferon for the treatment of chronic hepatitis C infection: a randomized, placebo-controlled double-blind trial. Hepatology 27: 1128–1135. 234 ANNALS OF THE NEW YORK ACADEMY OF SCIENCES 22. ANDREONE, P., A. GRAMENZI, C. CURSARO, et al. 2003. Interferon-alpha combined with ketoprofen as treatment of naive patients with chronic hepatitis C: a randomized controlled trial. J. Viral Hepat. 10: 306–309. 23. POO, J.L., F. SANCHEZ-AVILA, D. KERSHENOBICH, et al. 2004. Triple combination of thymalfasin, peginterferon alfa-2a and ribavirin in patients with chronic hepatitis C who have failed prior interferon and ribavirin treatment: 24-week interim results of a pilot study. J. Gestroenterol. Hepatol. 6: S79–S81. 24. ROMANI, L., F. BISTONI, R. GAZIANO, et al. 2004. Thymosin alpha 1 activates dendritic cells for antifungal Th1 resistance through toll-like receptor signaling. Blood 103: 4232–4239. 25. ROMANI, L., F. BISTONI, K. PERRUCCIO, et al. 2006. Thymosin alpha1 activates dendritic cell tryptophan catabolism and establishes a regulatory environment for balance of inflammation and tolerance. Blood 108: 2265–2274. 26. GARACI E., F. PICA, P. SINIBALDI-VALLEBONA, et al. 2003. Thymosin alpha 1 in combination with cytokines and chemotherapy for the treatment of cancer. Int. Immunopharmacol. 3: 1145–1150.