- The King's Fund
advertisement

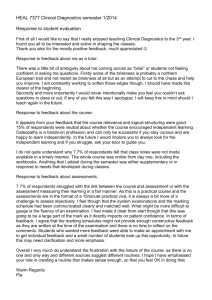
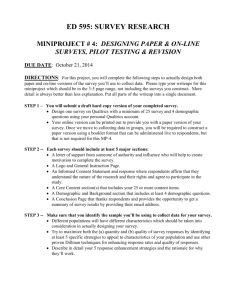
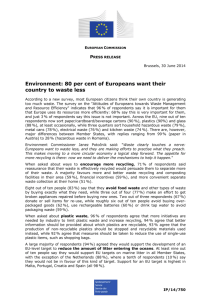
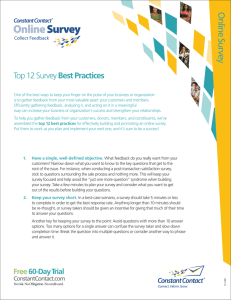
Authors Nick Goodwin Shilpa Ross Alex Smith October 2010 The quality of care in general practice Capturing opinions from the front line Introduction The Inquiry into the Quality of General Practice in England, commissioned by The King’s Fund, has collected and examined evidence on the quality of care and services provided by GPs and other health professionals working in general practice. The work has focused on key aspects (‘dimensions’) of general practice, selected by the inquiry panel as representing core areas for quality improvement. This paper examines the key findings of an online survey designed by The King’s Fund to complement the GP inquiry, in order to gain the views of those working in general practice. The survey sought to gain the opinions of GPs and other primary care professionals on the extent to which general practice is currently providing ‘high-quality’ patient care and their reaction to current approaches to ‘quality improvement’ in general practice. The survey was an informal one, carried out through the online tool Survey Monkey. As such, it did not set out to achieve scientific rigour – but instead to offer a snapshot of health professionals’ views and to indicate areas that might warrant further investigation. How was the survey conducted? The King’s Fund posted the open-access survey on the GP Inquiry website between mid-December 2009 and the end of March 2010. We recruited respondents by contacting individuals who had previously signed up for updates from the Inquiry and through communications targeted at members of the Royal College of General Practitioners, the NHS Alliance and the Royal College of Nursing. Due to the nature of the survey, it would not be appropriate to take the findings as representative of those working in general practice. However, in capturing a range of views from the front line, the survey has raised a number of key issues for further exploration and debate. 1 © The King’s Fund 2010 The quality of care in general practice What questions did the survey ask? The survey was divided into two parts: n The first part of the survey asked for opinions about the current quality of care in general practice, both generally and across the care dimensions selected by the Inquiry. Specifically, it asked respondents what they thought were the key priorities for quality improvement in the future. n The second part asked about the impact (whether real or potential) of different methods for quality improvement, and for respondents’ views on how quality could best be improved in the future. In particular, it asked respondents which approaches they felt were the most likely, and which the least likely, to improve quality. How many people completed the survey? The survey was completed by 843 GPs and other practice-based professionals. Their roles are shown in Table 1. (Percentages are rounded to one decimal place.) Table 1 Number and types of respondents from general practice completing the survey* Role Number Per cent GP partner 569 67 Salaried GP 63 7 GP registrar 16 2 GP locum or sessional GP 29 3 Practice manager 79 9 Nurse employed in general practice 74 9 Other staff member in a GP practice 13 2 *N=843 Results The quality of care in general practice For the purposes of the survey, we defined high-quality care in general practice as ‘the delivery of services that improve health outcomes for patients and reflect current professional knowledge and best practice’. It asked respondents to rate the current level of quality across different dimensions of care on a 10-point scale, with 10 being the highest rating of quality. It asked them to do this in terms of the quality provided both in their own practice and in general practice as a whole. Figure 1 shows the distribution of findings by each dimension for the whole sample. This shows that survey respondents rated the performance of their own general practice across a range of scores, between a low average of 7.9 (out of 10), for tackling inequalities in care, to a high of 8.6, for the quality of diagnosis and patient engagement during consultations. Respondents tended to hold slightly more positive views about the quality of care provided in their own practice than about that of general practice as a whole. In assessing general practice as a whole, average scores ranged from a low of 7.2, for access to care, to a high of 7.9, for the quality of diagnosis. 2 © The King’s Fund 2010 The quality of care in general practice Figure 1 The quality of various dimensions of care in general practice, as rated by those in general practice osis ment ons hips Diagnosis t of ons Patient engagement during consultations erral Therapeutic relationships tion tion Management of long-term conditions care Referral Dimension and ment care Health promotion and ill health prevention End-of-life care care Prescribing and medicines management ties care 6.5 7.0 7.5 Co-ordination8.5 of care 8.0 9.0 Average score Access to care Tackling inequalities in care 6.5 My practice 7.0 7.5 8.0 8.5 9.0 Average score General practice as a whole A key objective of the survey was to test views about which dimensions of care should be prioritised for improvement. Respondents were asked to tick their top three choices. Figure 2 shows which dimensions of care respondents felt should be prioritised. As the figure shows, the two dimensions of care most often chosen as a priority for improvement were continuity of care (which almost 60 per cent of respondents identified as a priority) and the management of long-term conditions. Despite the focus on access to care in recent public debate, this issue came fairly low down the list of priorities and was My practice identified by only around 20General per cent of respondents. Referral was at bottom of the list, practice as a whole with only 10 per cent identifying it as a priority. The survey also asked respondents to identify the dimensions that should not be prioritised for improvement, again by indicating their top three choices. As Figure 3 shows, access to care was most often chosen as the dimension of care that did not need to be prioritised, even though this dimension received the lowest quality rating of all the dimensions considered. In contrast, fewer than 1 in 10 respondents identified continuity of care and 3 © The King’s Fund 2010 The quality of care in general practice management of long-term conditions as dimensions that should not be prioritised. End-of-life care was the dimension chosen least often in this part of the survey. The results of this survey should not be seen as representative, but they do suggest that those working in general practice would seek to prioritise improvements in continuity of care over improvements in access to care. This does not mean that access is not an important consideration, but the findings are consistent with recent indications that patients, when given a choice, would generally opt for better continuity of care over speed of access (Gerard et al 2008; Turner et al 2007). The Inquiry’s report on continuity of care also concluded that continuity of care had been taken for granted for many years, despite being an important determinant of satisfaction among staff and patients alike (Freeman and Hughes 2010). Figure 2 Which dimensions of care should be prioritised?* 60 Percentage 40 20 Co nt in ui ty of lo ca ng M re -t an er ag m e He co me nd n ill alt iti t o -h h o f ea pr lth om ns o pr ti e o En ven n an d- tio d of n -li fe ca re Di P ag no du atie si rin nt s m g co an ns ag m ul em ed ta e ici tio n ne Pr ns t s esc m r an ib ag ing e Ac me and ce nt ss to ca re In eq ua lit ie s re The la ra tio p ns eu hi tic ps Re fe rra l 0 * Respondents (n=672) could indicate up to three dimensions 4 © The King’s Fund 2010 The quality of care in general practice Figure 3 Which dimensions of care should not be prioritised?* 60 Percentage 40 20 lit ie s T re he la ra Pa t io pe du tie ns u rin nt hi tic m g ps co an ns ag m ul em ed ta e ici tio n ne Pr ns t s esc m r an ib ag ing em a en nd Di t He ag no ill alt -h h si ea pr s lth om pr oti e o lo ng M ven n an a t -t n er ag ion d m e co me Co nd nt nt itio o f in ui ns ty of ca En re dof -li fe ca re ua ra l Re fe r eq In Ac ce ss to ca re 0 * Respondents (n=562) could indicate up to three dimensions The survey also gave GP respondents the opportunity to provide some ‘free-text’ responses to the question, asking ‘Are there any other aspects of patient care provided by general practices that you believe require improvements in quality?’. As Figure 4 shows, recurrent themes cited by GPs fell into two main areas: more time spent with patients, and better care co-ordination. The most cited area in which quality gains could be made was more time with patients. This was consistent with other non-GP responses – particularly the need for greater investment in numbers of staff and practice infrastructure to enable this to happen. The GPs also cited better co-ordination of care as an important area where quality gains could be made – especially if barriers in the system could be removed to ensure better coordination of care between professionals and organisations responsible for patient care. 5 © The King’s Fund 2010 The quality of care in general practice Figure 4 GP partner responses* on aspects of patient care requiring improvement in quality More time for patient care 53 Themes (top 5) More investment in resources and/or more GPs 30 Continuity of care (in all locations and out of hours) 22 Better co-ordination with other professionals 22 Removal of barriers within the health care system 22 0 10 20 30 40 50 60 Number of times theme cited * N=245 Approaches to support quality improvement in general practice The second part of the survey asked respondents about the impact of different methods of quality improvement. These included their assessment of the value of: n clinical or best practice guidance designed to inform and support those working in general practice to provide high-quality care n pay-for-performance schemes such as the Quality Outcomes Framework (QOF), QOF+ and local enhanced services n the Quality Practice Award an award given to general practices by the Royal College of General Practitioners in recognition of high-quality patient care provided by all members of staff in the practice based on a formal assessment n revalidation an initiative that assesses whether GPs meet current professional standards and are fit to practise n accreditation a quality improvement process to support the organisational development of general practice, to demonstrate compliance with the registration requirements of the Care Quality Commission n patient experience surveys that enable information to be gathered about patients and their experiences of care after they access services n balanced scorecards an approach that brings together a basket of performance measures, in order to assess and monitor performance over time. The survey also sought views on how quality could best be improved in the future, and on which of these approaches were the most likely to improve quality, and which the least likely. As Figure 5 shows, more than 70 per cent of respondents thought that best practice guidelines and pay-for-performance mechanisms would have a positive or highly positive impact. In comparison, only 32 per cent thought this to be the case for practice accreditation and revalidation schemes, and respondents rated balanced scorecards and patient experience surveys even lower. 6 © The King’s Fund 2010 The quality of care in general practice Cl in nt ex pe su rie rv nc Ba ey e la s nc ed sc or ec ar ds n at io Pa tie Re va lid ac cr ed at io n QP A st gu pra id cti an ce ce Pr ac tic e ica la nd be F+ LE S Figure 5 What impact do various approaches to quality improvement have? Approaches to quality improvement Don’t know Highly negative impact Negative impact Little or no difference Positive impact Highly positive impact The survey also asked respondents to indicate which approaches they thought were the most, and which the least, effective in improving quality in general practice (see figures 6 and 7), selecting up to three options. Again, the respondents felt that clinical or best practice guidelines and pay-for-performance mechanisms were likely to have the highest impact in improving quality, with patient experience surveys, revalidation and balance scorecards having the least. It is not clear whether respondents’ views about the impact and effectiveness of patient experience surveys suggest that those working in general practice do not value the views of patients, or whether they reflect concerns about the way the surveys are carried out and the data presented. Either way, if these findings do reflect their views, it gives some cause for concern. 7 © The King’s Fund 2010 The quality of care in general practice Figure 6 What approaches to quality improvement are most effective?* 80 Percentage 60 40 20 n nt ex pe su rie rv nc Ba ey e la s nc ed sc or ec ar ds Pa tie ita tio cr ed Ac QO be st - pr ac tic e Clin gu ic id al an o F+ ce r an d LE S sc he m Qu es al ity Fr a am nd ew O or utc k om (Q e OF s ) Qu al i t Aw y ar Pra d ct (Q ic PA e ) Re va lid at io n 0 * N=642 The survey offered respondents the opportunity to comment more generally on approaches to quality improvement through a free-text question. Most responses to this question were provided by GP partners. Figure 8 shows the top five themes that they raised. The responses to the questions about what impact different approaches to quality improvement might have (see Figures 6 and 7) appeared to put least value on systems of audit, accreditation and benchmarking. However, in contrast, the free-text responses from GP partners suggested that practitioners valued these approaches when they were undertaken by the professionals themselves. The GP partners who completed the free-text option most commonly cited the need for: n learning opportunities n continuing professional development n the time and ability to use data to undertake internal peer review and local audit. These themes also emerged strongly in the free-text responses provided by other GPs and practice nurses. A final key theme to emerge was the plea for protected time to value and undertake such activities, enabling professionals to take stock and reflect on the quality of care they provide. 8 © The King’s Fund 2010 The quality of care in general practice Figure 7 What approaches to quality improvement are least effective?* 60 Percentage 40 20 al Aw ity ar Pra QO d ct (Q ic F+ PA e an ) d LE S sc he m be es st -p ra ct ice C gu linic id al Qu an o al ce r ity Fr a am nd ew O or utc k om (Q e OF s ) n Qu Ac cr ed ita tio ar ds sc or ec ed Ba la nc Pa tie nt ex pe su rie rv nc ey e s Re va lid at io n 0 * N=647 Figure 8 GP partner responses* on other effective approaches to quality improvement in general practice Learning and continuing professional development 51 36 Themes (top 5) Auditing Peer review and feedback 15 Collaboration across boundaries 14 13 Practice-based commissioning 0 10 20 30 40 Number of times theme cited * N=242 9 © The King’s Fund 2010 50 60 The quality of care in general practice Discussion This survey was conducted to engage frontline professionals in general practice in order to gain a snapshot of their views about the quality of care that they provide. It captured the opinions of some 843 individuals working in general practice. Although it cannot claim to be representative of the views of general practice as a whole, it does indicate some interesting findings and raise important questions for debate. 10 © The King’s Fund 2010 n When asked how many GP practices in England provided high-quality care overall, the average score was 82.5 per cent. Is this rating something that the profession as a whole should be proud of, or does it suggest complacency? To what extent does this suggest that a significant minority of practices are failing to achieve the minimum standards that one would expect? n The survey suggested that when it comes to quality improvement, continuity of care (in the sense of involving patients in decision-making and helping them to navigate access to other health services) may be a more important priority than access to care (in terms of ease of access to practices and convenience of appointment times). Is this really the case – and, if so, is the current political debate focusing on the wrong issue by emphasising the issue of access? n The majority of GPs who responded to the survey felt that quality would be most improved through being able to devote more time to patient care, linked to greater investment in practice infrastructure. To what extent should the focus on investment be linked to developing and extending the staff, skill-mix and infrastructure within GP practices, compared with developing better co-ordinated networks of care provision between GP practices and other providers of primary, community, secondary and social care? n Does the reported view that patient experience surveys lack impact and effectiveness suggest that those working in general practice do not value the views of patients, or does it indicate that they distrust the way the data on patient experience is collected? Either way, should these findings give cause for concern? n What is the right balance of levers and incentives to support general practice in providing the best possible care? Is the Quality Outcomes Framework really the most important tool for quality improvement, or do the findings suggest a general unwillingness to embrace or trust other forms of quality improvement initiatives, such as revalidation and accreditation? n The findings indicate that those working in general practice have an appetite for being proactive in quality improvement – for example, through education, professional development and peer review. How can the system provide the time and headspace to enable this? The quality of care in general practice References Freeman G, Hughes J (2010). Continuity of Care and the Patient Experience [online]. The King’s Fund website. Available at: www.kingsfund.org.uk/current_projects/gp_ inquiry/dimensions_of_care/continuity_of_care.html (accessed on 22 June 2010). Gerard K, Salisbury C, Street D, Pope C, Baxter H (2008). ‘Is fast access to general practice all that should matter?: a discrete choice experiment of patients’ preferences’. Journal of Health Services Research and Policy, vol 13 (2), pp 3–10. Turner D, Tarrant C, Windridge K, Bryan S, Boulton M, Freeman G, Baker R (2007). ‘Do patients value continuity of care in general practice?: an investigation using stated preference discrete choice experiments’. Journal of Health Services Research and Policy, vol 12 (3), pp 132–37. 11 © The King’s Fund 2010 Barcode here? The King’s Fund 11–13 Cavendish Square London W1G OAN Tel 020 7307 2400 Registered charity: 207401 www.kingsfund.org.uk 12 © The King’s Fund 2010 The King’s Fund is a charity that seeks to understand how the health system in England can be improved. Using that insight, we help to shape policy, transform services and bring about behaviour change. Our work includes research, analysis, leadership development and service improvement. We also offer a wide range of resources to help everyone working in health to share knowledge, learning and ideas.