REVIEW ARTICLE
Prevention of Relapse After Quitting Smoking
A Systematic Review of Trials
Tim Lancaster, MSc, MB, BS; Peter Hajek, PhD; Lindsay F. Stead, MSc;
Robert West, PhD; Martin J. Jarvis, DSc
Background: After initially successful quit attempts,
many people return to smoking within a year, reducing
the public health benefits of investment in smoking cessation. We aimed to assess whether interventions designed to prevent relapse after a successful quit attempt
reduce the proportion of recent quitters who return to
smoking.
Methods: We searched the Cochrane Tobacco Addiction Review Group trials’ register. We selected randomized or quasi-randomized controlled trials of relapse prevention interventions with a minimum follow-up of 6
months. We included people who quit on their own, underwent enforced abstinence, or were in treatment programs. We included trials comparing relapse prevention interventions with no intervention or cessation plus
relapse prevention with cessation intervention alone. Two
of us independently extracted data from each report, with
disagreements referred to a third author.
N
Author Affiliations:
Department of Primary Health
Care, University of Oxford,
Oxford, England (Dr Lancaster
and Ms Stead); Clinical
Psychology, The Royal London
Hospital, and Tobacco
Dependence Research Centre,
Barts and The London, Queen
Mary’s School of Medicine and
Dentistry, London, England
(Dr Hajek); and Department of
Epidemiology and Public
Health (Drs West and Jarvis)
and Tobacco Studies (Dr West),
Cancer Research UK Health
Behaviour Unit, University
College London, London.
Results: Forty-two studies met the inclusion criteria.
The most common interventions were skills training
to identify and resolve tempting situations and
extended treatment contact. A few studies tested pharmacotherapy. We separately analyzed studies that randomized abstainers and those that randomized participants before their quit date. Within subgroups of
trials, pooled odds ratios ranged from 0.86 to 1.30,
and in most analyses, 95% confidence intervals
included 1. Most studies had limited power to detect
moderate differences between interventions.
Conclusion: The evidence to date does not support the
adoption of skills training or other specific interventions to help individuals who have successfully quit smoking to avoid relapse, but this is an important area for future study.
Arch Intern Med. 2006;166:828-835
ICOTINE REPLACEMENT,1
some antidepressants,2
and behavioral support3,4 for smoking cessation increase longterm quit rates compared with control, but
a proportion of initially successful participants return to smoking over time. Several strategies for improving public health
by reducing this proportion have been
studied. These strategies include behavioral techniques, such as skills training,5
extended treatment contact, imaginary cue
exposure, aversive smoking and social support, drug treatments, and other interventions primarily used for supporting quit
attempts. In planning tobacco treatment
programs, it is important to be informed
about the relative effectiveness of different strategies, particularly in determining how much resource to allocate to helping quit attempts vs supporting abstinence.
The objective of this review is to provide
information to assist this decision. An extended version of this review has been published and will be regularly updated in the
Cochrane Database of Systematic Reviews.6
(REPRINTED) ARCH INTERN MED/ VOL 166, APR 24, 2006
828
METHODS
SEARCH STRATEGY
We searched the Cochrane Tobacco Addiction Review Group register of trials, which includes the results of systematic searches, updated quarterly, of MEDLINE, PsycINFO, and
conference abstracts. We identified studies
mentioning relapse prevention or maintenance in the title, abstract, or keywords. The
most recent search was in August 2005.
INCLUSION CRITERIA
We included randomized or quasi-randomized
controlled trials with at least 6 months of follow-up after quitting. We included participants
who had quit smoking on their own, were in enforced abstinence, or were in cessation programs. There is no clear distinction between a
relapse prevention intervention and an extended cessation treatment. Thus, we included
interventions identified by study investigators as
intended to prevent relapse, compared with no
intervention, a shorter intervention, or an intervention not oriented toward relapse prevention. The outcome was abstinence at follow-up
of at least 6 months from randomization.
WWW.ARCHINTERNMED.COM
Downloaded from www.archinternmed.com at TEXAS TECH HLTH SCI CTR, on November 8, 2006
©2006 American Medical Association. All rights reserved.
DATA EXTRACTION
We extracted data on study setting,
population, method of randomization,
and allocation concealment; age, sex,
baseline cigarette consumption, and period of quitting of participants; interventions and control condition; outcome, including length of follow-up;
definition of cessation; and validation of
self-reported smoking status.
DATA SYNTHESIS
The primary outcome was the number
of quitters at the longest follow-up. We
used biochemically validated cessation
in preference to self-report where available, preferring continuous or prolonged abstinence to point prevalence
abstinence where possible. We classified randomized participants who withdrew, were lost to follow-up, or failed
to provide validation samples as continuing smokers. When studies reported strict and more lenient outcomes, we extracted both and conducted
a sensitivity analysis on the pooled results. We expressed individual study results as an odds ratio (OR) with a 95%
confidence interval (CI) and pooled
study outcomes using a fixed-effect
(Mantel-Haenszel) model, unless there
was significant statistical or clinical heterogeneity between trials. We separately analyzed trials that randomized abstainers from those that randomized
smokers. We also separated studies in
which contact time was matched and
those in which the relapse prevention included longer contact.
We performed subgroup analyses for
longer (⬎4 weeks) and shorter durations of intervention, in trials randomizing smokers to matched-duration interventions, and between more (⬎4 sessions)
and fewer intervention sessions for unmatched intervention and control programs. We also considered subgroup
analyses for “skills” and social support
studies, and for spontaneous quitters such
as pregnant women and individuals seeking smoking cessation treatment.
DESCRIPTION OF STUDIES
We identified 42 studies for inclusion.
One article7 reported 2 trials each with
multiple arms relevant to different comparisons, and 48-11 included subgroups
or factorial designs contributing to different comparisons. Two (5%) of the
studies did not specifically describe the
intervention as involving relapse prevention. One12 was a replication of an included study, and one13 randomized abstainers.
Studies Randomizing People
Who Had Stopped Smoking
Twenty-six studies randomized people
who had stopped smoking (Table 1). The
interventions for preventing relapse
included behavioral strategies and pharmacotherapy. Intensive behavioral interventions involved repeated face-to-face
contact usually aiming at teaching clients
to identify tempting situations and to apply a range of coping and cognitive strategies to resist relapse. Less intensive interventionsincludedwrittenmaterialsand
brief face-to-face or telephone contacts.
Amongthestudiesrandomizingpeople
who had stopped smoking, 9 randomized
pregnant14-19 or postpostpartum20-22 abstainers. Two studies9,13 randomized hospital inpatients with cardiovascular illness
who had not smoked during hospital admission, and one23 randomized hospital
patients who were abstinent on the day
of discharge. Two studies24,25 randomized
military recruits undergoing enforced
abstinence. Five studies10,11,26-28 randomized participants recruited from local
communities.
Five studies29-33 randomized abstainers who had taken part in a cessation
program to behavioral interventions.
Four studies randomized abstainers to
pharmacological interventions, including nicotine chewing gum10,11 and bupropion hydrochloride.34,35
Studies Randomizing Current
Smokers Before Their Quit Date
Seventeen studies (including 1 also contributing to the first category9) randomized smokers who then attempted to quit
with or without relapse prevention components (Table 2).
Intervention and Control Groups
Matched for Contact Time. In 9 studies,
intervention and control conditions were
matched for the amount of contact. Seven
studies (1 with 2 components)7,8,36-39 used
a group behavioral format, and 29,40 used
individual counseling. Three provided
pharmacotherapy to all treatment participants (the studies by Emmons et al38 and
Buchkremer et al [with 2 components]7).
A factorial design tested nicotine gum
against no gum.40
Intervention and Control Groups Not
Matched for Contact Time or Duration.
Most smoking cessation studies comparing more with less intensive treatments
include some intervention to prevent relapse. We only included trials that specified relapse prevention as an explicit focus of the intervention. We did not
include studies offering treatment proac-
(REPRINTED) ARCH INTERN MED/ VOL 166, APR 24, 2006
829
tively to special populations, such as pregnant or hospitalized smokers, because all
trials using these groups provide some relapse prevention input within the active
treatment arm, and they are covered in
separate Cochrane reviews. Where studies had 3 or more treatment conditions,
we compared the most with the least intensive interventions. Seven studies7,12,41-45 compared longer with shorter
programs, all involving face-to-face contact. The relative intensity of the cessation and the relapse prevention components varied. One study46 compared
group-based behavior therapy for 8 weeks
plus proactive calls 1, 8, and 11 months
later with group therapy alone. We excluded other studies that tested the use
of telephone counseling as an adjunct to
nicotine replacement therapy, because
most of the behavioral support was provided during the cessation period.
METHODOLOGICAL QUALITY
OF INCLUDED STUDIES
Sample Size and Study Design
Many trials were small and had limited
power to detect realistic differences in quit
rates, especially in the group that randomized smokers before the quit date.
Studies randomizing successful endof-treatment quitters provide the most
straightforward test of relapse prevention
interventions designed for clinical practice. All 4 studies10,11,34,35 of pharmacologicaltreatmentsusedthisapproach,butonly
2 studies31,33 of behavioral treatments randomized participants who were abstinent
for more than 1 week of treatment.
Definition of Smoking Cessation
We required a report of smoking status a
minimum of 6 months from the start of
the intervention. In the case of studies that
randomized smokers before quitting, this
could have been from the quit date. Some
studies timed follow-up from the end of
treatment. Three trials9,22,38 reported
6 months of follow-up; all others had a
longer follow-up. Some studies did not
provide a definition of abstinence, and
most others reported point prevalence
rather than sustained abstinence.
Validation of
Self-reported Abstinence
All but 6 studies20,22,24,25,28,29 used some
form of biochemical validation of selfreported smoking status, but in some
other cases, samples were not collected
from all participants, were not collected at long-term follow-up, or were
not used to correct self-reports.
WWW.ARCHINTERNMED.COM
Downloaded from www.archinternmed.com at TEXAS TECH HLTH SCI CTR, on November 8, 2006
©2006 American Medical Association. All rights reserved.
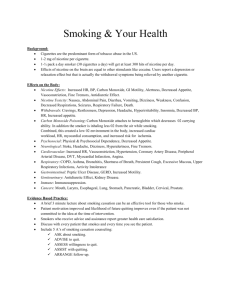
Table 1. Details of Studies Randomizing Abstainers
Country/No.
of Participants
Source
Common
Components
and Control
RP
Interventions
Ershoff et al,14
1995
United States/
171 females
(early pregnancy)
Self-help booklets, 4 on cessation at
the baseline visit and 4 RP-focused
booklets mailed
Secker-Walker
et al,15 1995
United States/
165 females
(early pregnancy)
Counseling, skills rehearsal, 10-15 min
at the first, second, and third prenatal
visit and 6 and 36 wk postpartum
Lowe et al,16
1997
United States/
78 females
(early pregnancy)
Control: usual care,
including nurse advice
Secker-Walker
et al,17 1998
United States/
125 females
(early pregnancy)
McBride et al,18
1999
United States/
897 females
(44% already
quit in early
pregnancy and RP
postpartum for
end-of-pregnancy
quitters)
Hajek et al,19
2001
England/249
cluster-randomized
females (early
pregnancy)†
United States/1026
cluster-randomized
females
(postpartum)†
Counseling, 10-min RP materials at
the fifth-grade reading level enhance
social support with materials, and
choose a “buddy”; reinforcement
at routine visits by clinic staff
Structured intervention from a
physician, counseling by nurse
counselor, first, second, third, fifth,
and 36-wk prenatal visits
1. Prepartum intervention: tailored letter,
S-H book; after 28 wk, sent RP kit;
3 telephone counseling calls,
approximately 2 wk after S-H mailing
and 1 and 2 mo later (average,
8.5 min). 2. Prepartum/postpartum
intervention: as done in 1, plus 3 calls
within the first 4 mo postpartum
(average, 7.7 min). 3. Newsletters
Advice from a midwife with an
explanation of CO reading, a
pamphlet, and a prompt placed
in notes for reinforcement
Counseling plus follow-up at 2-, 4-,
and 5-mo visits, plus materials
Counseling session in the hospital,
plus 8 telephone calls (weekly for
1 mo and biweekly for 2 mo);
skills training, S-H pamphlets,
and no smoking materials
Counseling from a visiting nurse,
15-30 min, after baseline interview;
reinforcement by pediatric care
provider at 2-wk and 2- and 4-mo
well-baby clinics; written materials;
chart sticker used to prompt
intervention
RP intervention with focus on coping
skills and stress management
(6 sessions that were 1 h long)
Usual care
Severson et al,20
1997
Ratner et al,21
2000
Canada/215 females
(postpartum)
Van’t Hof et al,22
2000
United States/
277 females
(postpartum)
Schmitz et al,9
1999 (part)
United States/
53 females
(hospitalized for
coronary artery
disease)‡
Hajek et al,13
2002
England/540 males
and females
(hospitalized for
myocardial
infarction or
coronary artery
bypass grafting)
Japan/106 males
and females
(hospitalized,
quit on day of
discharge)
United States/
18 010 Air Force
recruits (smokers
before training)
Hasuo et al,23
2004
Klesges et al,24
1999
Conway et al,25
2004
United States/
1682 female
naval recruits
(661 reached
at follow-up)
OR (95% CI)
for Abstinence at
Longest Follow-up
Late in third trimester
(PPA)/cotinine
1.32 (0.61-2.89)
36 wk of pregnancy,
8-54 mo postpartum/
cotinine-creatinine ratio
prepartum only
End of pregnancy,
sustained/saliva
thiocyanate
Prepartum,
0.88 (0.46-1.68);
and postpartum,
1.02 (0.53-1.96)
1.24 (0.42-3.64)
Sustained abstinence at
36-wk pregnancy, 1 y
postpartum, CO for 36
wk (urine cotinine)*
28-wk pregnancy, 12 mo
postpartum
(PPA)/saliva cotinine*
Prepartum,
0.64 (0.31-1.32);
and postpartum,
0.65 (0.32-1.33)
Prepartum,
interventions 1 and 2,
1.62 (0.93-2.82);
and postpartum,
intervention 1,
0.99 (0.63-1.55),
and intervention 2,
1.04 (0.66-1.63)
Usual midwife care
Birth (12 wk SA) and
12 mo (SA)/CO
Birth, 1.35 (0.82-2.24);
and postpartum,
0.88 (0.49-1.58)
All: information pack,
including letter from
pediatrician on risks
of passive smoking
12-mo postpartum (SA);
no validation
(losses to follow-up
[25%] assumed to
have relapsed)
12-mo postpartum
(SA)/CO
1.38 (1.05-1.82);
and corrected
for clustering,
1.25 (0.93-1.68)
Usual care, baseline
assessment from
a visiting nurse
6-mo postpartum/no
validation
0.83 (0.51-1.34)
Intervention based on
Health Belief model;
smoking-related health
information related to
disease; focus on
benefits of stopping
All: verbal advice and
“Smoking and Your
Heart” booklet
6 mo (PPA)/CO and
urine cotinine*
0.81 (0.15-4.42)
12 mo (SA)/saliva cotinine
0.86 (0.60-1.23)
Additional telephone contact (5 min at 7,
21, and 42 d postdischarge)
All: intervention from
public health nurse
during hospitalization
(3 times, for 20 min)
12 mo/urine nicotine
1.20 (0.57-2.64)
Single 50-min intervention during the
final week of training, 50 per group
(including nonsmokers); discussed
health effects, costs, social impact,
and role play
6 S-H mailings over 12 mo, 1-page
flyers, cognitive-behavioral RP, stress
management, weight, and fitness,
tailored for naval women
All: 6-wk smoking ban and
2 videos. Control:
general health video
12 mo/no validation
OR not estimable,
no significant benefit
All: 2-mo smoking ban.
Control: no intervention
12 mo/no validation (PPA)
OR not estimable,
no significant
benefit)
Intervention from cardiac nurses during
routine work (20 min); CO reading,
booklet on smoking, and cardiac
recovery, written quiz, offer to find
support “buddy,” commitment, and
reminder in notes
All: 2-min discussion on
smoking and pregnancy
with health educator.
Control: 1-page tip
sheet
Control: usual care
Longest Follow-up
(Type of Abstinence)/
Validation
Control: usual care from
physician, prompted
at first visit
Self-help booklet only
1.17 (0.62-2.22)
(continued )
Randomization
Four studies used cluster-randomized
designs. In the 2 among military re-
cruits,24,25 allocation was by training
group and selection bias was unlikely.
In the others, allocation was by midwife19 or pediatric practice,20 and selec-
(REPRINTED) ARCH INTERN MED/ VOL 166, APR 24, 2006
830
tion bias in the subsequent enrollment
of participants might have been possible. Two of the cluster-randomized
trials reported that correlation between
WWW.ARCHINTERNMED.COM
Downloaded from www.archinternmed.com at TEXAS TECH HLTH SCI CTR, on November 8, 2006
©2006 American Medical Association. All rights reserved.
Table 1. Details of Studies Randomizing Abstainers (cont)
Country/No.
of Participants
RP
Interventions
Killen et al,10
1990
United States/
1218 community
volunteer smokers
who quit unaided
for 48 h
Fortmann and
Killen,11 1995
United States/
1044 proactively
recruited smokers,
who quit unaided
for 24 h
Brandon et al,26
2000
United States/
584 unaided
ex-smokers
(median
abstinence,
6.5 mo)
Brandon et al,27
2004
United States/
431 unaided
ex-smokers
(mean abstinence,
75 d)
Borland et al,28
2004
Australia/215 quitters
(calling quitline;
63% had quit in the
previous week)†
Powell and
McCann,29
1981
United States/
51 assisted
abstainers
Stevens and
Hollis,30 1989
United States/
587 assisted
abstainers
(confirmed
abstinent 4 d
after CP)
Factorial trial, contributes to 2
comparisons: behavioral
intervention, RP-focused S-H
materials, 16 modules prepared
(either 7 self-selected modules in
weekly mailings or 7 random
modules); and pharmacotherapy
intervention, 2-mg nicotine gum,
fixed or ad libitum schedule
Factorial trial, contributes to 2
comparisons: behavioral
intervention, RP-focused S-H
materials; and pharmacotherapy
intervention, 2 mg of nicotine
gum
2 ⫻ 2 factorial design testing
mail and hotline interventions.
1. Mailings condition: 8 Stay Quit
booklets mailed at 1, 2, 3, 5, 7,
9, and 12 mo. 2. Stay Quit
hotline. Participants called if not
registered within 2 wk and at 3
mo if no call made. 3. Combined
mailing and hotline
2 ⫻ 2 factorial design testing
the effects of high vs low
content and high vs low contact.
1. Repeated mailings; 8 booklets
at enrollment and 1, 2, 3, 5, 7, 8,
and 12 mo. 2. Mass mailings.
Same 8 booklets all at
enrollment. 3. Repeated letters,
single booklet, 7 supportive
letters, same schedule as in 1
S-H: tailored advice letters based
on standardized telephone
assessment; 2-3 pages, tailored
in part by stage of change,
timing varied
1. 4-wk support group.
2. Telephone contact system
allowing participants to
telephone each other
Three 2-h weekly meetings
covering skills development
and active rehearsal of
coping strategies
Razavi et al,31
1999
Belgium/344
abstainers
(3 mo after CP)
Smith et al,32
2001
United States/
677 abstainers
(1 wk after
quit day)
Mermelstein et
al,33 2003
United States/
341 abstainers
Hays et al,34 2001
United States/429
abstainers after
7 wk of bupropion
hydrochloride
therapy
United States/176
abstainers after an
8-wk tailored-dose
nicotine patch
Source
Hurt et al,35 2003
1. Ten monthly sessions, including
group discussion and role play
led by a professional counselor.
2. Ten sessions of group
discussion led by former
smokers
1. Cognitive-behavioral skills
training (6 times, from 1 wk
post-TQD), including managing
negative effect, homework, and
manual. 2. Motivational
interviewing, supportive group
counseling (6 times from
1-wk post-TQD). No homework
or manual
Tailored proactive telephone
counseling: 3 weekly sessions,
and then 3-6 alternate weekly
sessions (15 min each)
Bupropion, 300 mg/d, for 45 wk
Bupropion, 300 mg/d, for 6 mo
Common
Components
and Control
Longest Follow-up
(Type of Abstinence)/
Validation
OR (95% CI)
for Abstinence at
Longest Follow-up
All: S-H booklet, “How to
Cope With the Urge to
Smoke Without
Smoking.” Behavioral
control: no further
contact.
Pharmacotherapy
control: placebo gum or
no gum
All: $100 incentive for
6-mo quit. Behavioral
control: no S-H
materials.
Pharmacotherapy
control: no gum
No true control; minimal
contact condition
received first Stay Quit
booklet
12 mo (PPA)/saliva
cotinine*
Effect of S-H materials:
1.19 (0.88-1.61);
and effect of
nicotine gum,
1.23 (0.93-1.64)
12 mo (PPA)/CO and
saliva cotinine
S-H, 1.00 (0.73-1.37);
and nicotine gum,
1.39 (1.02-1.91)
12 mo (PPA)/CO*
Interventions vs
minimal contact,
0.99 (0.66-1.50);
S-H mailings vs not,
1.05 (0.74-1.48)
(includes dropouts
as relapsed)
No true control; minimal
contact condition
received 1 booklet
at enrollment
24 mo (SA, since
18 mo)/CO (local
volunteers only)*
Interventions vs
minimal contact,
1.20 (0.77-1.85);
S-H mailings vs not,
1.74 (1.09-2.97)
(including dropouts
as relapsed)
All: quit pack after contact
with the quitline, 1-2 d
before recruitment.
Control: no further
intervention
All: cessation program
before randomization.
Control: no further
contact
All: cessation program
before randomization.
Active control:
discussion condition;
three 2-h social support
meetings. Control:
no further contact
All: CP before
randomization. Control:
no further intervention
12 mo (SA)/no validation
1.65 (0.98-2.80)
12 mo/no validation
1.00 (0.24-4.08)
12 mo (SA)/saliva
thiocyanate
1.44 (0.95-2.19)
9 mo (SA)/CO and
urine cotinine
1.41 (0.85-2.33)
All: 3 brief individual
counseling sessions,
nicotine patches, and
S-H materials. Control:
no further intervention
12 mo (PPA)/CO
0.67 (0.43-1.06)
All: 7-wk group CP.
Control: supportive
but nonspecific
proactive counseling
(same schedule)
All: physician advice, S-H,
and brief counseling
during cessation phase.
Control: placebo
15 mo (PPA)/no validation
0.76 (0.49-1.16)
2 y, 1 y after EOT (SA)/CO
validation
1.16 (0.76-1.77)
All: brief advice and S-H
during the cessation
phase. Control: placebo
12 mo, 6 mo after EOT
(PPA)/CO validation
1.59 (0.73-3.46)
Abbreviations: CI, confidence interval; CO, carbon monoxide; CP, cessation program; EOT, end of treatment; OR, odds ratio; PPA, point prevalence abstinence;
RP, relapse prevention; SA, continuous, multiple point prevalence, or sustained abstinence; S-H, self-help; TQD, target quit date.
*Incomplete validation or validated rates not reported.
†Trial also recruited smokers, not included herein.
‡Excludes postrandomization dropouts.
(REPRINTED) ARCH INTERN MED/ VOL 166, APR 24, 2006
831
WWW.ARCHINTERNMED.COM
Downloaded from www.archinternmed.com at TEXAS TECH HLTH SCI CTR, on November 8, 2006
©2006 American Medical Association. All rights reserved.
Table 2. Studies Randomizing Participants Before Their Quit Attempt
Source
Country/No. of
Participants
RP
Interventions
Longest Follow-up
(Type of
Abstinence)/
Validation
Common Components
and Control
Intervention and Control Matched for Contact Time
Skills training, 14 (75-min) sessions
Discussion control, same schedule
included aversive smoking therapy,
relaxation, commitment, cost
benefits, and RP skills with role play
of risk situations. (Aversive
smoking condition arms collapsed.)
United States/
1. Active cognitive-behavioral skills
All: 6 (1.5- to 2-h) weekly sessions of a
45 smokers
training focusing on 11 problem
broad-spectrum cessation package,
situations. 2. “Enhanced control”
with a TQD of wk 5. Control: no
with discussion of same problems
additional components
United States/
RP focusing on smoking as a learned All groups: 8 (2-h) weekly sessions,
48 smokers in
behavior; quit day in group format
including relaxation training, social
group format
at third session. Additional
support, and practicing alternative
and 91 in
elements included identifying
behaviors. All S-H: same components
S-H format
high-risk situations, cognitive
in 8 weekly workbooks. Control:
restructuring, and role playing
“Absolute abstinence” approach.
Focused on addictive component of
smoking. Quit day in group format at
fifth session. Additional elements
included focused smoking, health
education, and contingency contract
United States/
RP-focused cessation program,
“Broad-spectrum” cessation program.
49 smokers
8 (1.5-h) weekly sessions,
There were 12 (1-h) sessions over
TQD between weeks 3 and 4;
8 wk. TQD between weeks 3 and 4.
prequit self-monitoring. Choice of
Included nicotine fading
“cold turkey” or gradual reduction.
Relaxation, role play, and
cognitive coping
Study 1:
Relapse coping training included
All: nicotine patch, dose individualized,
Germany/
within sessions
9 weekly sessions, including reduction,
94 smokers*
self-monitoring, contract management,
and risk avoidance. TQD after 6 wk.
Control: no further RP component
Study 2:
1. Relapse coping training using role
All: nicotine patch, dose individualized,
Germany/
play and TQD at 6 wk. 2. Modified
9 weekly sessions, including reduction,
124
relapse coping. Rapid abstinence,
self-monitoring, contract management,
smokers*
TQD at session 4, covert
and risk avoidance. TQD after 6 wk.
sensitization, and thought stopping
Control: no further RP component
Spain/
Program included problem-solving
All: 8 weekly group sessions, including a
76 smokers
skills training
motivational contract, nicotine fading,
stimulus control, and TQD at wk 4.
Control: no further RP component
United States/
1. CBT with imagined cue exposure
All: 1 brief individual counseling session
120 smokers
(75-min sessions). 2. CBT with
1 wk before TQD, plus S-H; 5 individual
cue exposure and nicotine gum
sessions over 2 wk post-TQD. Control:
(90 min)
brief CBT (15-min sessions) or CBT
(60 min) plus nicotine gum
United States/
Coping skills RP, including stress
All: 6 (1-h) group sessions. Control:
107 female
management and homework
Health Belief model; smoking-related
smokers with
health information–related CAD profile.
CAD risk
Focus on quit benefits
factors‡
OR (95% CI)
for Abstinence
at Longest
Follow-up
Hall et al,36 1984 United States/
135 smokers
12 mo (PPA)/CO
and plasma
thiocyanate
1.67 (0.81-3.42)
Davis and
Glaros,37
1986
12 mo (PPA)/CO
1.08 (0.13-8.80)
12 mo (SA)/saliva
thiocyanate and
2 collateral
verifiers
Group format,
0.56
(0.16-1.92);
S-H format,
1.71
(0.61-4.78)
6 mo (PPA)/saliva
thiocyanate
0.52 (0.15-1.88)
12 mo post-EOT
(PPA)/urine
nicotine†
1.33 (0.58-3.05)
12 mo post-EOT
(PPA)/urine
nicotine†
0.52 (0.23-1.19)
12 mo CO during
treatment/
informants at
follow-up
12 mo (SA)/CO
1.32 (0.51-3.44)
6 mo (PPA)/urine
cotinine and CO†
0.75 (0.26-2.17)
Curry et al,8
1988
Emmons et al,38
1988
Buchkremer
et al,7 1991
Becona and
Vazquez,39
1998
Niaura et al,40
1999
Schmitz et al,9
1999
0.38 (0.09-1.48)
(continued )
outcomes in individuals in the same cluster was small so that reporting individual outcomes was acceptable. These
2 trials also had high loss to follow-up,
although there was no evidence of differential loss between arms.
In the absence of significant findings in meta-analysis subgroups, we did
not attempt to explore the influence of
study quality on outcomes.
RESULTS
TRIALS IN ABSTAINERS
Specific Populations
Pregnant and Postpartum
Ex-smokers. We did not detect a significant benefit at the end of preg-
(REPRINTED) ARCH INTERN MED/ VOL 166, APR 24, 2006
832
nancy from 6 trials14-19 (n=1183; OR,
1.17; 95% CI, 0.90-1.53). We also
failed to detect an effect in the studies15,17-22 that included postpartum
follow-up (n=2695; OR, 1.08; 95%
CI, 0.92-1.27).
Hospital Inpatients. We failed to detect an effect of intervention in hos-
WWW.ARCHINTERNMED.COM
Downloaded from www.archinternmed.com at TEXAS TECH HLTH SCI CTR, on November 8, 2006
©2006 American Medical Association. All rights reserved.
Table 2. Studies Randomizing Participants Before Their Quit Attempt (cont)
Source
Killen et al,41
1984
Hall et al,42
1985
Brandon et al,43
1987
Hall et al,12
1987
Buchkremer et
al,7 1991
Lifrak et al,44
1997
Shoptaw et al,45
2002
Lando et al,46
1996
Country/No. of
Participants
RP
Interventions
Common Components
and Control
Intervention and Control Had Different Numbers of Contacts
RP skills training: 2 sessions in 2 wk, All: CP, 4 (1.5-h) sessions over 4 d,
then 4 weekly drop-in sessions,
including CBT, skills training, and
including identification of high-risk
nicotine gum. Control: no further
situations and coping strategies;
intervention
homework
United States/
Intensive BT, 14 (75-min) sessions
Control: 4 sessions in 3 wk,
84 smokers*
over 8 wk, including RP skills
educational materials, written
training, relaxation, and 2 mg of
exercises, group discussion, and
nicotine gum
nicotine gum
United States/
Additional 4 (1.5-h) sessions at
All: group CP, 6 (2-h) sessions over
39 smokers‡
2, 4, 8, and 12 wk postcessation:
2 wk. Control: no maintenance
self-monitoring, advice,
sessions
assignment of exposure, and
coping exercises
United States/
Group behavioral treatment,
Factorial trial; nicotine gum conditions
139 smokers
14 (75-min) sessions, including
collapsed. Control: “low contact,”
6-second aversive smoking,
5 (60-min) sessions, including
RP skills training, and written
exercises, materials, group
exercises, with or without
discussions, and quit techniques
nicotine gum
Study 1: Germany/ Additional 3 booster sessions 6 mo
All: nicotine patch, dose individualized,
149 smokers*
after TQD, with or without RP
9 weekly sessions, including
component CP
reduction, self-monitoring, contract
management, and risk avoidance.
TQD after 6 wk. Control: no further
RP component
United States/
Extended support; 16 weekly 45-min All: 4 individual sessions with a nurse
69 smokers
cognitive-behavioral RP therapy
to review S-H materials and use of
sessions
NRT. Nicotine patch for 10 wk.
Control: no further intervention
United States/
Group BT, 12 (1-h) weekly sessions, All: 12-wk nicotine patch. Control:
175 smokers
including mood management
no counseling, factorial study, and
undergoing
contingency management arms
methadone
collapsed
maintenance
therapy
United States/
Telephone counseling at 3, 9, and
All: 15-session 8-wk group CP.
1083 smokers
21 mo. At each point, up to 3 calls
Control: no further intervention
could be made if requested
United States/
44 smokers*
Longest Follow-up
(Type of
Abstinence)/
Validation
OR (95% CI)
for Abstinence
at Longest
Follow-up
10.5 mo (4-wk
prevalence)/CO
(serum thiocyanate
at 6 wk only)
3.40 (0.93-12.49)
1 y (PPA)/CO and
serum thiocyanate
1.32 (0.55-3.16)
1 y/CO during
treatment,
2 informants
1.14 (0.31-4.16)
1 y/thiocyanate, CO,
significant other
0.68 (0.33-1.40)
1 y post-EOT
0.78 (0.38-1.58)
(PPA)/urine nicotine
1y (PPA)/urine
cotinine
1.49 (0.54-4.11)
1 y (PPA)/CO and
urine cotinine
0.57 (0.13-2.44)
34 mo (12 mo after
EOT, PPA)/saliva
cotinine at 12 mo†
1.11 (0.86-1.43)
Abbreviations: BT, behavioral therapy; CAD, coronary artery disease; CBT, cognitive-behavioral therapy; CO, carbon monoxide; CP, cessation program; EOT, end of
treatment; NRT, nicotine replacement therapy; PPA, point prevalence abstinence; RP, relapse prevention; SA, continuous, multiple point prevalence, or sustained
abstinence; S-H, self-help; TQD, target quit date.
*In relevant arms.
†Incomplete validation or validated rates not reported.
‡Excludes postrandomization dropouts.
pitalized patients who had not
smoked in the hospital, based on 2
studies9,13 (n=558; OR, 0.86; 95% CI,
0.60-1.22). One further study46 offering 3 telephone calls for relapse
prevention among patients abstinent at discharge failed to detect evidence of benefit (n = 106; OR, 1.20;
95% CI, 0.57-2.64).
pected in these populations of young
smokers, but no effect was detected from the additional interventions. Less than 3% of participants
used the telephone support offered
in one trial.25
Military Personnel. Neither trial24,25
detected a benefit of intervention. In
both trials, the period of enforced abstinence gave rise to a higher quit
rate than the spontaneous rate ex-
We detected no evidence of a benefit of interventions to prevent relapse in people who had quit unaided10,11,26-28 (n=3561; OR, 1.14; 95%
CI, 0.96-1.34). All 5 studies used self-
Behavioral Interventions
for Unaided Abstainers
(REPRINTED) ARCH INTERN MED/ VOL 166, APR 24, 2006
833
help interventions, although in one,28
the materials were individually tailored based on information collected via telephone questionnaires.
Using different comparator groups in
the 2 factorial studies27,28 of different types of self-help did not substantially alter the pooled effect.
Behavioral Interventions
for Assisted Abstainers
We detected no long-term effect of
skills-based interventions to prevent
relapse in 5 studies29-33 in which ab-
WWW.ARCHINTERNMED.COM
Downloaded from www.archinternmed.com at TEXAS TECH HLTH SCI CTR, on November 8, 2006
©2006 American Medical Association. All rights reserved.
staining smokers were randomized after participation in a formal treatment
program (n=1121; OR, 1.00; 95% CI,
0.80-1.25). This meta-analysis compared the most intensive intervention
with the least intensive control in the
trials with more than 2 arms. Using a
different comparison did not change
the conclusion.
Pharmacotherapies
for Abstainers
Two trials10,11 detected a small effect
of nicotine gum (n=2261; OR, 1.30;
95% CI, 1.06-1.61). We failed to detect a significant benefit of bupropion when we pooled data from 2
trials34,35 (n=605; OR, 1.25; 95% CI,
0.86-1.81).
STUDIES RANDOMIZING
SMOKERS BEFORE
THEIR QUIT DATE
Behavioral Interventions
Matched for Contact Time
We found no benefit from the use
of specific relapse prevention components in group or individual format interventions, based on 9 trials
(with 1 trial that included 2 components)7-9,36-40 (n = 793; OR, 0.91;
95% CI, 0.65-1.27). There was no evidence of heterogeneity. Because all
but 140 of the studies involved treatment contact for more than 4 weeks,
we did not conduct a subgroup analysis by treatment duration. Most trials
used a skills training approach.
One study8 comparing different
versions of a self-help program did
not detect a difference in quit rates
(OR, 1.71; 95% CI, 0.61-4.78).
Behavioral Intervention
Not Matched for Contact Time
or Duration
We detected no effect of relapse prevention in 7 trials7,12,41-45 involving extended face-to-face contact (n=699;
OR, 1.01; 95% CI, 0.71-1.44). We detected no significant heterogeneity.
Extended Contact Using
Proactive Telephone Calls
One trial46 failed to detect a benefit
of providing extended contact by
telephone after an intensive 8-week
group program (OR, 1.11; 95% CI,
0.86-1.43).
COMMENT
Through meta-analysis of randomized trials, we failed to detect a clinically significant effect of existing relapse prevention interventions in
sustaining successful attempts to stop
smoking. Because most studies concerned only 1 particular type of intervention (skills training), the volume of work is modest (to our
knowledge, there exists only 1 study
randomizing smokers at the end of a
formal treatment period), and because many of the studies have serious limitations, there is a strong need
for continuing research in this area.
Most studies included in this review evaluated low-intensity interventions, such as brief face-to-face
encounters, written materials, mailings, and telephone contact. Although only a few included studies
had adequate sample sizes to detect
the expected effects, the CIs around
the pooled estimates suggest that it
is unlikely that the analysis failed to
detect a significant benefit of lowintensity interventions. However, it
is more difficult to exclude a clinically useful effect of more intensive
interventions, because these have
been less extensively studied.
Any negative verdict is limited to
the only treatment approach studied
extensively so far, the skills training
approach. Other approaches, which
have not been studied well or at all,
have been proposed; these include opportunistic use of nicotine replacement, contingency contracting, social support, cue exposure (only
imaginary exposure has been studied so far), and interventions aimed
at maintaining abstainers’ morale.
We included all studies that randomized abstainers, because these
provide the best test of interventions
aimed at maintaining abstinence. We
also included studies randomizing
smokers before quitting, which were
described as tests of relapse prevention treatments, although there is not
a clear-cut distinction between those
interventions and others tested as
pure cessation interventions.
There are 2 arguments in favor of
randomizing smokers before stop-
(REPRINTED) ARCH INTERN MED/ VOL 166, APR 24, 2006
834
ping smoking. From a theoretical perspective, it may be difficult to separate cessation and relapse prevention
advice; and from a practical perspective, sample sizes are usually much
higher at the start than at the end of
treatment. The methodological disadvantage of integrating cessation and
relapse prevention is that it reduces
power to detect specific relapse prevention effects. The primary outcome variable is normally the abstinence rate at follow-up. It is difficult
to differentiate effects of the intervention on the initial smoking cessation from effects on preventing relapse in smokers who were initially
successful. One solution to this problem is to provide a separate analysis
of those achieving initial success.
However, none of the existing studies used this approach, and it also
poses problems with randomization
if the initial cessation rate is unequal in the 2 groups.
Randomizing only those smokers who have made a successful quit
attempt provides a stronger design
for isolating the effects of relapse prevention, because true effects are not
masked by other factors related to
the initial success or skewed by uneven initial cessation rates. Of the existing studies using this approach,
most recruited spontaneous abstainers, such as pregnant women. Of the
studies of behavioral methods for relapse prevention, only 131 randomized smokers abstinent at the end of
an initial treatment episode and
329,30,32 randomized smokers abstinent 5 to 8 days after their quit day.
The studies randomizing abstainers varied considerably in the periods for which participants had already abstained from smoking, from
24 hours to 16 months. This reflects the lack of a consistent definition of a successful quit attempt.
Futurestudiesshouldconsiderrandomizingsmokerswhowereabstinent
continuously and completely for at
least 4 weeks, and use as the primary
outcome measure continuous lapsefree abstinence of at least 6 months if
the intervention was aimed at avoiding lapses. Where the intervention
aimed at helping patients to cope with
lapses should these occur, a period of
grace (eg, 6 months) should be included, followed by another 6 months
of lapse-free abstinence.
WWW.ARCHINTERNMED.COM
Downloaded from www.archinternmed.com at TEXAS TECH HLTH SCI CTR, on November 8, 2006
©2006 American Medical Association. All rights reserved.
In summary, this review does not
exclude a small effect of some relapse prevention interventions, but
neither does it provide evidence to
support inclusion of relapse prevention interventions in smoking treatment programs.
Accepted for Publication: September 16, 2005.
Correspondence: Tim Lancaster,
MSc, MB, BS, Department of Primary Health Care, University of Oxford, Old Road Campus, Headington, Oxford OX3 7LF, England (tim
.lancaster@dphpc.ox.ac.uk).
Author Contributions: Dr Lancaster had full access to all the data
in the study and takes responsibility for the integrity of the data and
the accuracy of the data analysis.
Financial Disclosure: None.
Funding/Support: The Cochrane
Tobacco Addiction Review Group is
supported by the National Health
Service of the United Kingdom.
Role of the Sponsor: The funding
body had no role in data extraction
and analyses, in the writing of the
manuscript, or in the decision to submit the manuscript for publication.
11.
12.
13.
14.
15.
16.
17.
18.
19.
REFERENCES
1. Silagy C, Lancaster T, Stead L, Mant D, Fowler G.
Nicotine replacement therapy for smoking
cessation. Cochrane Database Syst Rev. 2004;
(3):CD000146.
2. Hughes J, Stead L, Lancaster T. Antidepressants
for smoking cessation. Cochrane Database Syst
Rev. 2004;(4):CD000031.
3. Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst Rev. 2002;(3):CD001292.
4. Stead LF, Lancaster T. Group behaviour therapy
programmes for smoking cessation. Cochrane Database Syst Rev. 2002;(3):CD001007.
5. Marlatt A, Gordon J. Relapse Prevention. New York,
NY: Guilford Publications; 1985.
6. Hajek P, Stead LF, West R, Jarvis M. Relapse prevention interventions for smoking cessation. Cochrane Database Syst Rev. 2005;(1):CD003999.
7. Buchkremer G, Minneker E, Block M. Smokingcessation treatment combining transdermal nicotine substitution with behavioral therapy.
Pharmacopsychiatry. 1991;24:96-102.
8. Curry SJ, Marlatt GA, Gordon J, Baer JS. A comparison of alternative theoretical approaches to
smoking cessation and relapse. Health Psychol.
1988;7:545-556.
9. Schmitz JM, Spiga R, Rhoades HM, Fuentes F.
Smoking cessation in women with cardiac risk: a
comparative study of two theoretically based
therapies. Nicotine Tob Res. 1999;1:87-94.
10. Killen JD, Fortmann SP, Newman B, Varady A.
Evaluation of a treatment approach combining
nicotine gum with self-guided behavioral treat-
20.
21.
22.
23.
24.
25.
26.
27.
ments for smoking relapse prevention. J Consult
Clin Psychol. 1990;58:85-92.
Fortmann SP, Killen JD. Nicotine gum and selfhelp behavioral treatment for smoking relapse prevention: results from a trial using populationbased recruitment. J Consult Clin Psychol. 1995;
63:460-468.
Hall SM, Tunstall CD, Ginsberg D, Benowitz NL,
Jones RT. Nicotine gum and behavioral treatment: a placebo controlled trial. J Consult Clin
Psychol. 1987;55:603-605.
Hajek P, Taylor TZ, Mills P. Brief intervention during hospital admission to help patients to give up
smoking after myocardial infarction and bypass
surgery: randomised controlled trial. BMJ. 2002;
324:87-89.
Ershoff DH, Quinn VP, Mullen PD. Relapse prevention among women who stop smoking early
in pregnancy: a randomized clinical trial of a selfhelp intervention. Am J Prev Med. 1995;11:
178-184.
Secker-Walker RH, Solomon LJ, Flynn BS, et al.
Smoking relapse prevention counseling during prenatal and early postnatal care. Am J Prev Med.
1995;11:86-93.
Lowe JB, Windsor R, Balanda KP, Woodby L.
Smoking relapse prevention methods for pregnant women: a formative evaluation. Am J Health
Promot. 1997;11:244-246.
Secker-Walker RH, Solomon LJ, Flynn BS, Skelly
JM, Mead PB. Smoking relapse prevention during pregnancy: a trial of coordinated advice from
physicians and individual counseling. Am J Prev
Med. 1998;15:25-31.
McBride CM, Curry SJ, Lando HA, Pirie PL, Grothaus LC, Nelson JC. Prevention of relapse in women
who quit smoking during pregnancy. Am J Public Health. 1999;89:706-711.
Hajek P, West R, Lee A, et al. Randomized controlled trial of a midwife-delivered brief smoking
cessation intervention in pregnancy. Addiction.
2001;96:485-494.
Severson HH, Andrews JA, Lichtenstein E, Wall
M, Akers L. Reducing maternal smoking and relapse: long-term evaluation of a pediatric
intervention. Prev Med. 1997;26:120-130.
Ratner PA, Johnson JL, Bottorff JL, Dahinten S,
Hall W. Twelve-month follow-up of a smoking relapse prevention intervention for postpartum
women. Addict Behav. 2000;25:81-92.
Van’t Hof SM, Wall MA, Dowler DW, Stark MJ.
Randomised controlled trial of a postpartum relapse prevention intervention. Tob Control. 2000;
9(suppl 3):III64-III66.
Hasuo S, Tanaka H, Oshima A. Efficacy of a smoking relapse prevention program by postdischarge telephone contacts: a randomized trial [in
Japanese]. Nippon Koshu Eisei Zasshi. 2004;
51:403-412.
Klesges RC, Haddock CK, Lando H, Talcott GW.
Efficacy of forced smoking cessation and an adjunctivebehavioraltreatmentonlong-termsmokingrates.
J Consult Clin Psychol. 1999;67:952-958.
Conway TL, Woodruff SI, Edwards CC, Elder JP,
Hurtado SL, Hervig LK. Operation Stay Quit: evaluation of two smoking relapse prevention strategies for women after involuntary cessation during US Navy recruit training. Mil Med. 2004;
169:236-242.
Brandon TH, Collins BN, Juliano LM, Lazev AB.
Preventing relapse among former smokers: a comparison of minimal interventions through telephone and mail. J Consult Clin Psychol. 2000;
68:103-113.
Brandon TH, Meade CD, Herzog TA, Chirikos TN,
(REPRINTED) ARCH INTERN MED/ VOL 166, APR 24, 2006
835
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
Webb MS, Cantor AB. Efficacy and costeffectiveness of a minimal intervention to prevent smoking relapse: dismantling the effects of
amount of content versus contact. J Consult Clin
Psychol. 2004;72:797-808.
Borland R, Balmford J, Hunt D. The effectiveness of personally tailored computer-generated
advice letters for smoking cessation. Addiction.
2004;99:369-377.
Powell DR, McCann BS. The effects of a multiple
treatment program and maintenance procedures on
smoking cessation. Prev Med. 1981;10:94-104.
Stevens VJ, Hollis JF. Preventing smoking relapse, using an individually tailored skillstraining technique. J Consult Clin Psychol. 1989;
57:420-424.
Razavi D, Vandecasteele H, Primo C, et al. Maintaining abstinence from cigarette smoking: effectiveness of group counselling and factors predicting outcome. Eur J Cancer. 1999;35:1238-1247.
Smith SS, Jorenby DE, Fiore MC, et al. Strike while
the iron is hot: can stepped-care treatments resurrect relapsing smokers? J Consult Clin Psychol.
2001;69:429-439.
Mermelstein R, Hedeker D, Wong SC. Extended
telephone counseling for smoking cessation: does
content matter? J Consult Clin Psychol. 2003;
71:565-574.
Hays JT, Hurt RD, Rigotti NA, et al. Sustainedrelease bupropion for pharmacologic relapse prevention after smoking cessation: a randomized, controlled trial. Ann Intern Med. 2001;135:423-433.
Hurt RD, Krook JE, Croghan IT, et al. Nicotine patch
therapy based on smoking rate followed by bupropion for prevention of relapse to smoking.
J Clin Oncol. 2003;21:914-920.
Hall SM, Rugg D, Tunstall C, Jones RT. Preventing relapse to cigarette smoking by behavioral skill
training. J Consult Clin Psychol. 1984;52:372382.
Davis JR, Glaros AG. Relapse prevention and smoking cessation. Addict Behav. 1986;11:105-114.
Emmons KM, Emont SL, Collins RL, Weidner G.
Relapse prevention versus broad spectrum treatment for smoking cessation: a comparison of
efficacy. J Subst Abuse. 1988;1:79-89.
Becona E, Vazquez FL. The course of relapse across
36 months for smokers from a smoking-cessation
program. Psychol Rep. 1998;82:143-146.
Niaura R, Abrams DB, Shadel WG, Rohsenow DJ,
Monti PM, Sirota AD. Cue exposure treatment for
smoking relapse prevention: a controlled clinical
trial. Addiction. 1999;94:685-696.
Killen JD, Maccoby N, Taylor CB. Nicotine gum
and self-regulation training in smoking relapse
prevention. Behav Ther. 1984;15:234-248.
Hall SM, Tunstall C, Rugg D, Jones R, Benowitz
N. Nicotine gum and behavioral treatment in smoking cessation. J Consult Clin Psychol. 1985;
53:256-258.
Brandon TH, Zelman DC, Baker TB. Effects of maintenance sessions on smoking relapse: delaying the
inevitable? J Consult Clin Psychol. 1987;55:
780-782.
Lifrak P, Gariti P, Alterman AI, et al. Results of two
levels of adjunctive treatment used with the nicotine patch. Am J Addict. 1997;6:93-98.
Shoptaw S, Rotheram-Fuller E, Yang X, et al.
Smoking cessation in methadone maintenance.
Addiction. 2002;97:1317-1328.
Lando HA, Pirie PL, Roski J, McGovern PG, Schmid
LA. Promoting abstinence among relapsed chronic
smokers: the effect of telephone support. Am J
Public Health. 1996;86:1786-1790.
WWW.ARCHINTERNMED.COM
Downloaded from www.archinternmed.com at TEXAS TECH HLTH SCI CTR, on November 8, 2006
©2006 American Medical Association. All rights reserved.