PDF file
advertisement

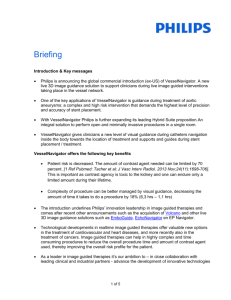
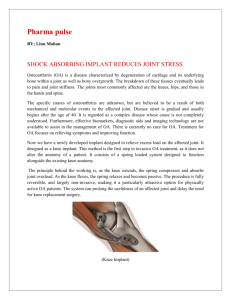
recovering after a week and after three weeks she was able to sit, stand and walk. Body righting reflexes are complex and these are five separate types of reflexes (i) Labyrinthine righting reflexes acting upon the neck muscle, (ii) Neck righting reflexes acting upon the body (iii) Body righting reflexes acting upon the head (iv) Body righting reflexes acting upon the body (v) Optical righting reflexes. Center for (i) to (iv) types of righting reflexes is in brain stem and for optical righting reflexes is cortical. Sensory impulses from proprioceptors of muscles, tendons and joints are conveyed to the spinal cord by medial division of the posterior roots and connects with the cells of Clarke’s column and further continued upwards in the dorsal (posterior) and ventral (anterior) spinocerebellar tracts of the same side. Dorsal spinocerebellar tract through inferior cerebellar peduncle and ventral through superior cerebellar peduncle reaches to the cerebellum. Impulses from floculonodular lobe of cerebellum passes to reticular formation in brain stem via fastigiobulbar tract (center for body righting reflexes) and further through reticulospinal tract to anterior horn cells message is conveyed regarding regulation of tone of skeletal musculature of extremities, trunk and neck to maintain the posture of body (vegetative nervous system).2,3 Fig. 1 : MRI brain showing ring lesion. Fig. 2 : Contrast MRI brain showing ring-enhancing lesion. temperature, viberation, position and cortical sensations) bilateral normal. Rhomberg sign positive (both open and closed eyes), Cerebeller functions were normal. Position of head in relation to trunk and body was normal and she was able to lift the head. On investigation: Urinalysis, Haemogram, Blood biochemistry, X-ray Chest, E.K.G. were normal. M.R.I. Brain (Plain and contrast) revealed a 6 X 5 X 5 mm. ringenhancing lesion with peri-lesional oedema (hypertense on T2 weighted images) involving right side of caudal brain stem in the paramedical area of dorsal medulla sparing right restiform body (Figs. 1 and 2 ). Elisa for cysticercosis was positive i.e. 0.55 OD (> 0.35 OD is positive). Patient was treated with Albendazole 400 mg twice a day for three weeks and Prednisolone 20 mg per day for two weeks and thereafter tapered. Patient started 668 In this reported case, inflammatory lesion with perilesional oedema in the right side of caudal brain stem with normal sense of position and vibration and cerebellar functions i.e. sparing right restiform body may have involved the center for body righting reflexes acting upon the right side of the body. Peri-lesional oedema must have subsided with prednisolone and relieved pressure on the center in caudal part of right side of brain stem, may explain the full recovery i.e. she was able to sit, stand and walk properly. Available literature was reviewed, such type of unilateral neurological involvement i.e. unable to maintain upright posture with normal motor and sensory system is not reported so far. AK Gupta Medical Specialist, Regional Hospital, Nahan, Himachal Pradesh 173 001. Received : 13.12.2005; Revised : 4.3.2006; Accepted : 7.7.2006 REFERENCES 1. Magnus R. Studies on the physiology of posture. Lancet 1926;2:531-6. 2. Magoun HW. The ascending reticular activating system. Res Publ Ass Ner Ment Dis 1952;30:480-8. 3. Best CH, Taylor NB. Spinal cord and brain stem. A Text Book of Applied Physiology, 8 th ed (II nd Indian Reprint) Calcutta, 1967;116-43. Aortic Aneurysm : An Unusual Presentation Sir, Nowadays, superior vena cava syndrome (SVCS) is www.japi.org © JAPI • VOL. 54 • AUGUST 2006 believed to result almost entirely from malignancy, and at presentation other causes of SVCS1 are overlooked or underreported. Aneurysms and pseudoaneurysms of the ascending aorta have been reported to cause SVCS. Atherosclerosis is not commonly associated with aneurysms of the ascending aorta2 even though it is the usual cause of aneurysm of the descending aorta.3 Atherosclerosis as the cause of aneurysm of the entire aorta is also unusual. We report a case of atherosclerotic aneurysm involving the entire aorta presented with SVCS, a rare clinical presentation. A 52 years man with a history of heavy smoking was admitted for evaluation of exertional breathlessness of 3 months duration. Physical examination revealed features of obstruction of the superior vena cava (SVC) and pleural effusion on the left side. His pulse rate, blood pressure and temperature were normal. There were no signs suggestive of any connective tissue disease. The fasting lipids were: total cholesterol –282mg/dl, LDL cholesterol –202mg/dl, HDL cholesterol –35mg/dl VLDL –62mg/dl and the triglycerides –146mg/dl. Chest radiograph revealed pleural effusion on the left side, cardiac enlargement with a widened aortic shadow and prominence of the superior vena cava (Fig. 1). Electrocardiogram showed left ventricular hypertrophy and transthoracic echocardiography showed dilated aortic root, moderate aortic regurgitation and a left ventricular ejection fraction of 70%. A computed tomogram of the chest and abdomen showed fusiform aneurysm involving the ascending, the arch and the descending portions of the thoracic and the abdominal aorta up to the common iliac arteries with multiple small areas of calcification consistent with diffuse atherosclerosis. Dilated ascending aorta was compressing the superior vena cava causing the SVCS (Fig. 2). There was no intra-thoracic or intra-abdominal lymphadenitis and the lungs and the abdominal viscera were normal. Other laboratory parameters (including syphilitic serology) were normal. The patient was advised aortic valve replacement and aortic surgery with engraftment of the whole thoracic aorta in a two-step procedure but he opted for medical therapy. He was advised smoking cessation and avoidance of strenuous activities and was prescribed ramipril 5mg OD, aspirin 150mg OD, clopidogrel 75mg OD and atorvastatin 20mg HS. After two months of treatment, he reported some improvement in his exertional dyspnoea and his lipid abnormalities showed significant improvement. Other than malignancy benign intrathoracic tumors, inflammatory or infective processes, and a group of cardiovascular diseases can cause SVCS. 1 Cardiovascular causes for SVCS are aneurysm of the ascending aorta, dissection of the proximal aorta, thrombosis of the SVC and rarely pseudoaneurysm of the ascending aorta complicating aortic root surgery. © JAPI • VOL. 54 • AUGUST 2006 Fig. 1 : Prominent SVC (arrow) Fig. 2 : Arrow shows the compressed SVC Ascending aortic aneurysms are seen in association with familial disorders of collagen (Marphan syndrome, Ehlers-Danlos syndrome and osteogenesis imperfecta), syphilis, ankylosing spondylitis, mycotic aneurysms caused by infections, trauma and coarctation of aorta. This patient had extensive aneurysm involving ascending and descending aorta and the etiology was most likely atherosclerotic as supported by vascular risk factors (cigarette smoking and dyslipidemia) and CT scan findings. More so, there was no evidence of connective tissue disorder and syphilis. Even though SVCS and atherosclerotic aortic aneurysms are common entities in clinical practice, atherosclerotic aneurysm of the entire aorta presenting as SVCS is rare. www.japi.org 669 Asha G Pillai*, J Thomas*, J Antony*, MJ Pappachan**, G George***, P Sujathan+ diagnosis and treatment. Am J Crit Care 1992;1:54-64. 2. Agmon Y, Khandheria BK, Meissner, et al. Is aortic dilatation an atherosclerosis-related process? Clinical, laboratory, and transesophageal echocardiographic correlates of thoracic aortic dimensions in the population with implications for thoracic aortic aneurysm formation. J Am Coll Cardiol 2003;42:1076-83. 3. Reynolds HR, Tunick PA, Kort S, et al. Abdominal aortic aneurysms and thoracic aortic atheromas. J Am Soc Echocardiogr 2001;14:1127-31. *Resident; **Senior lecturer; ***Associate professor; +Professor, Department of Internal Medicine, Kottayam Medical College. Kerala- 686 008. Received : 16.3.2006; Revised : 5.6.2006; Accepted : 7.7.2006 REFERENCES 1. Baker GL, Barnes HJ. Superior vena cava syndrome: etiology, Announcement 36TH Annual Conference of Endocrine Society of India ESICON 2006, Jaipur 17th – 19th November, 2006 will be held at B.M. Birla Science and Technology Centre, Jaipur. For further details please contact : Dr. R Patni (Chairman) or Dr. Prakash Keswani (Organising Secretary) Secretariat : 399, Near Geeta Bhawan, Adarsh Nagar, Jaipur – 302 004. E-mail : esicon2006@yahoo.com Website : www.esicon2006.com; Phone : 0141-2602342, 2612049 Announcement XIIIth Annual Conference of API WB Branch at Hyatt Regency, Kolkata on 23rd and 24th September 2006. Contact API WB Branch for registration Prof. Samar Banerjee - Chairman, Dr. Surendra Daga - Hon. Secretary. Tel: 033 2227 6024 / 6048 670 www.japi.org © JAPI • VOL. 54 • AUGUST 2006