Infant Behavior & Development 33 (2010) 136–148
Contents lists available at ScienceDirect
Infant Behavior and Development
Maternal anxiety, mother–infant interactions, and infants’ response to
challenge
Marsha Kaitz a,∗ , Hilla Rubin Maytal a , Noa Devor a , Liat Bergman a , David Mankuta b
a
b
Hebrew University, Jerusalem, Israel
Hadassah Hospital-Hebrew University Medical School, Jerusalem, Israel
a r t i c l e
i n f o
Article history:
Received 9 September 2009
Received in revised form 4 December 2009
Accepted 28 December 2009
Keywords:
Anxiety
Maternal behavior
Mother–infant interactions
Emotion regulation
a b s t r a c t
Children of anxious mothers are at risk for social–emotional difficulties and disturbed, early
interactions with their mother may account for some of the risk. This study evaluated the
association between maternal anxiety, features of mother–infant interactions, and infants’
emotion regulation during stressful situations (still-face, play with a stranger). Thirty-four
anxiety-disordered mothers of 6-month-old infants and 59 typical dyads comprised the
sample. Dyads were filmed during free play, teaching, care giving, and face-to-face play;
and monadic (e.g., maternal sensitivity, infant affect) and dyadic measures (e.g., synchrony)
were derived by global or time-event coding of the films. Results indicate that, compared to
controls, more anxious mothers showed exaggerated behavior with their infant during free
play and teaching, and infants of anxious mothers were less likely to show negative affect
during the still-face and stranger challenges. We conclude that anxious maternal behavior
reflects the hyperarousal that is characteristic of most anxiety disorders; and infants of
anxious mothers and controls show differences in the manner in which they cope with
social challenges.
© 2010 Elsevier Inc. All rights reserved.
1. Introduction
Anxiety disorders affect millions of adults world wide, causing them significant distress and difficulties in daily functioning
(Barlow, 2002). Anxiety disorders can last for years and can get worse if they are not treated. Anxiety disorders commonly
occur along with other mental health disorders such as depression, which may mask anxiety symptoms or make them worse.
Of especial concern, anxiety seems to run in families so that children of parents with anxiety disorders are at higher risk for
developing anxiety disorders and other developmental disorders than are children of healthy parents (Schreier, Wittchen,
Höfler, & Lieb, 2008). Research on the processes by which anxiety can be transmitted to offspring are needed in order to
identify potential routes of transmission and to discern early signs of perturbed development in children of anxious parents
(Shonkoff & Phillips, 2000).
Considering this, we carried out a study in order to identify distinctive features of interactions between anxious mothers and their infants and to look for early effects that maternal anxiety might have on the young. The research follows a
number of studies on depressed mothers that have shown that their interactions with their infants are marked by mothers’
more prevalent negative affect, less sensitive responsiveness, and less frequent shared behavioral states with their infants,
particularly in samples with multiple adversities (e.g., Field, Healy, Goldstein, & Guthertz, 1990; reviews in: Goodman,
∗ Corresponding author at: Department of Psychology, Hebrew University, Jerusalem 91905, Israel. Tel.: +972 2 5883372; fax: +972 2 5881159.
E-mail address: msmarsha@mscc.huji.ac.il (M. Kaitz).
0163-6383/$ – see front matter © 2010 Elsevier Inc. All rights reserved.
doi:10.1016/j.infbeh.2009.12.003
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
137
2007; Lovejoy, Graczyk, O’Hare, & Neuman, 2000; Reck et al., 2004). Research also provides strong evidence that these kind
of interactions can forecast developmental problems beginning at a very young age (reviews in Field, Hernandez-Reif, &
Diego, 2006; Weinberg & Tronick, 1998a). More generally, these studies are part of a larger literature that demonstrates
that mother–infant interactions are important social experiences for infants and, in atypical form, can lead to problems in
important developmental domains (Feldman, Greenbaum, & Yirmiya, 1999; Isabella & Belsky, 1991; Lyons-Ruth, Bronfman,
& Parsons, 1999; reviews in Schore, 2001; Swain, Lorberbaum, Kose, & Strathearn, 2007).
1.1. Maternal anxiety and mother–infant interactions
There are only a few studies in which highly anxious mothers have been observed with their infants, and findings regarding
distinctive features have been variable and in some studies, difficult to interpret. For example, Weinberg and Tronick (1998b),
using a mixed sample of women with panic disorder, depression, and obsessive compulsive disorder, reported pervasive
difficulties in aspects of mother–infant interplay, though as noted by the authors, the effects of anxiety cannot be discerned
because of the makeup of the sample. In a second study, Warren et al. (2003) compared panic-disordered (PD) mothers of
4 or 14-month-old infants to control dyads and reported significant group differences in maternal sensitivity and in some
parenting techniques. The infants of the probands had more sleep problems and higher levels of cortisol than did infants
of controls, although the groups did not differ on other measures (high reactivity, behavioral inhibition, or ambivalent
attachment). As in Weinberg and Tronick (1998b), it is difficult to ascribe these differences to anxiety per se because the PD
women had other disorders, including depression.
Using a more diagnostically homogenous sample, Murray, Cooper, Creswell, Schofield, & Sack (2007) found less pervasive,
but still significant differences between the interactions of anxious dyads and healthy ones. In that study, mothers with social
phobia (SOP) were described as no less sensitive to their 10-week-old infants than were control mothers; but they engaged
their infant less and looked more anxious than controls. Further, in the context of a social challenge (stranger–mother–child
interaction), the mothers with SOP looked more fearful and were less encouraging of their infants’ engagement. Interestingly,
mothers with generalized anxiety disorder (GAD) were also less engaged with their infant during dyadic play, but showed
no differences from controls during the stranger challenge. For their part, infants of mothers with SOP were less positively
engaged with the stranger than were infants of controls; this was not the case for infants of mothers with GAD. Notably,
the exclusion of women with depression from the sample did not change the pattern of results, thus demonstrating that
depression was not a confounding factor. Finally, in the most recent study; Weinberg, Beeghly, Olson, & Tronick (2008)
observed anxious (PD, without depression) and control mothers with their 3-month-old infants and found no distinctive
markers of anxiety among a large array of monadic and dyadic measures, though this may be due to the small size of the
sample (n = 13). Besides these studies, there are others that have reported a relation between mothers’ anxiety symptoms
(not diagnoses) and deficits in maternal and/or infant behavior (e.g., Blissett, Meyer, & Haycraft, 2007; Feldman, Greenbaum,
Mayes, & Erhlich, 1997; Field et al., 2005; Nicol-Harper, Harvery, & Stein, 2007; Nover, Shore, Timberlake, & Greenspan, 1984;
Stifter, Coulehan, & Fish, 1993; also see Wijnroks, 1999), however, the women in these samples usually were not anxious
(according to their symptom scores), so the results may not be generalizable to clinical samples.
In summary, the findings so far do not provide a coherent picture of anxious mother–infant interactions. More data are
needed to discern markers of anxious maternal behavior and developmental difficulties among children of highly anxious
mothers.
1.2. The present study
In the present study, we filmed clinically anxious mothers and their 6-month-old infants and compared their behavior to
that of healthy dyads. We also looked for group differences in the infants’ responses to challenge. Probands were diagnosed
for current anxiety so that we could relate their mental health to their concurrent behavior. In Warren et al. (2003), women
were diagnosed for lifetime (not necessarily current) disorders; in Weinberg et al. (2008) and in Murray et al. (2007), women
were diagnosed during pregnancy, though in the latter study, symptomology was confirmed by short symptom inventories
at the time of testing.
To derive a comprehensive picture, we filmed anxious and control dyads in varied episodes that simulated interactions
that mothers and infants have together on a routine basis (floor play, teaching, care giving). In addition, mothers and infants
were filmed during the still-face paradigm (SFP, Tronick, Als, Adamson, Wise, & Brazelton, 1978), in which mothers play
face-to-face with their infant, then adopt a “still-face”, and then resume face-to-face play. Infants also were filmed during an
interaction with a playful stranger. Using data derived from the still-phase phase of the SFP and from the stranger episode,
we looked for signs of atypical (infant) emotion regulation, succinctly defined as the “. . . extrinsic and intrinsic processes
responsible for monitoring, evaluating, and modifying emotional reactions” (Thompson, 1994, pp. 27–28). In many studies,
infants’ emotion regulation has been assessed by examining infants’ responses to mild challenges (e.g., Haley & Stansbury,
2003; Moore & Calkins, 2004; Moore, Cohn, & Campbell, 2001), and this was the tact taken in the present study. Importantly,
early difficulties in emotion regulation can predict later developmental difficulties, including fearfulness and anxiety, in
some children (Degnan & Fox, 2007; Park, Belsky, Putnam, & Crnic, 1997).
We addressed three research questions:
138
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
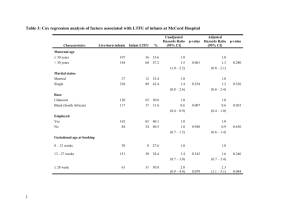
Table 1
Characteristics of the control (N = 59) and anxious (N = 34) groups.
Controls
M
Anxious
SD
Girl infants
Native Israeli
Seculara
Employedb
%
54.2
83.1
28.8
56.1
n
32
49
17
32
%
52.9
76.5
41.2
67.6
n
18
26
14
23
Education
High-school
Prof. train.
BAc
MAc
PhDc
8.5
16.9
62.7
10.2
1.7
5
10
30
6
3
11.8
11.8
35.3
38.2
2.9
4
4
12
13
1
Treatment
Therapy now
Past therapy
Meds nowd
1.7
13.6
.0
1
8
0
11.8
29.4
5.9
4
10
1
a
c
d
26.06
15.66
SD
25.11
15.19
b
4.07
2.39
M
Age
Education (year)
3.99
1.71
Secular vs. conservative, religious, or orthodox (all women were Jewish).
Employed outside of the home.
Completed or in progress.
Psychotropic medication.
(1) Do clinically anxious mothers and their infants show atypical features in their behavior during (non challenging) mutual
interactions? Without a clear direction from previous studies, we refrained from hypothesizing which behaviors distinguish anxious dyads from controls during non-stressful play.
(2) Do anxious dyads have a particularly hard time in realigning their social interplay after the still-face challenge? Tentatively, we predicted that they do (despite the null findings of Weinberg et al., 2008), assuming that the stress of the
still-face condition would exacerbate the anxiety symptoms of anxious mothers and, as a result, it would take anxious
dyads longer to recover from the still-face challenge than it would, control dyads (Ham & Tronick, 2006).
(3) Do infants of anxious mothers show atypical emotional responses to challenges? We considered this likely, but did not
predict whether infants of anxious mothers would show more distress or less distress than infants of controls. This is
because, on one hand, infants of anxious mothers may be vulnerable to distress if indeed they have been routinely stressed
by anxious maternal behavior (Kopp, 1989) or other factors associated with having a highly anxious mother (Rutter,
2005). On the other hand, a history of unresponsive or overzealous care by anxious mothers could interfere with their
infants’ natural tendency to call out to their caregiver (i.e., signal distress) for comfort (Bowlby, 1980, 1988). Significantly,
either outcome would constitute evidence of atypical development among infants of highly anxious mothers.
2. Method
2.1. Participants
The sample was comprised of first-time mothers and their 6-month-old infants. The anxious group was comprised of
34 women diagnosed with a current anxiety disorder (13 with panic, 8 with social phobia, and 13 with PTSD) without
(lifetime) depression. The control group was comprised of 59 controls who did not meet (DSM-IV, American Psychological
Association, 1994) criteria for (lifetime) clinical or sub clinical anxiety or depression (see Table 1 for demographics and
background information). As stipulated by inclusion criteria, the women in both groups were 20–40 years old, married,
primiparae, conceived naturally, had completed high-school, and had no serious physical conditions. Inclusion criteria also
required that the infants were born at full-term without complications, and had no serious health problems.
2.2. Recruitment and attrition
This study received ethic committee approval from the urban hospitals in which women were recruited. Women also were
recruited government-subsidized well-baby clinics up to 2 weeks after childbirth. On recruitment days, all first-time mothers
with healthy infants were asked for (written) permission to contact them when their infant was 1-month-old in order to tell
them more about a study on mothers’ feelings and infant development. Most of the women (920/980) agreed to be contacted
at one month postpartum; the 60 women who refused cited reasons including their unwillingness to participate in research
or their plans to move away. Of those who agreed to be contacted, 78 women could not be reached after trying on four
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
139
consecutive days at different hours of the day. Of the 842 women who were contacted at one month, 780 were interviewed
by phone at 5-months postpartum in order to screen them for anxiety and depression, evaluate anxiety symptomology, and
procure their agreement to come to the lab when their infant was 6-months old. The other women (n = 62) could not be
reached after four attempts at contact or were no longer interested in participating in the study.
The women who were interviewed at 5-months postpartum and answered yes to an anxiety screening question but no to
the depression screening question, and agreed to continue in the study were targeted for the anxiety group (82); those who
screened negative for depression and anxiety were targeted for the control group (178). Of these 260 women, 30 women
(18 targeted for control group and 12 targeted for the anxious group after screening, X2 , p > .05) could not be scheduled for
the lab session because of the mothers’ working hours (5), infants were more than 6.5 months old when contact was made
with their mothers (2), mothers could not be reached by phone (12), or mothers refused to come to the lab (11). The other
230 came to the lab where they were diagnosed and filmed; and of these, 59 met final criteria (see below) for the control
group and 34 met criteria for the anxious group. In sum, the total refusal and attrition rate of this study was 23.5% (230/980).
2.3. Diagnosis assessment
Current and lifetime diagnoses were based on the background interview and the anxiety and depression modules of
the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID), supplemented with Beck symptom inventories for
assessment of the severity of depression and anxiety symptoms (Beck Anxiety Inventory, BAI; Beck Depression Inventory,
BDI). Women who did not meet diagnostic criteria for threshold or subthreshold, current or lifetime disorders and scored
less than 9 on the BAI and BDI were eligible for the control group. Inclusion in the anxious group required a diagnosis of
one or more current (threshold) anxiety disorders; but excluding women diagnosed with “only” a specific phobia (n = 7) and
those diagnosed with an anxiety disorder plus depression at any time in their lives (n = 8). Women with “just” a specific
phobia were excluded (from the control and anxious groups) because phobias are highly specific to certain stimuli (e.g.,
animals, blood); and we presumed that, by themselves, they would not interfere with mothers’ behavior toward their infant.
Women with depression were excluded from the sample so it would not obscure effects of anxiety on mothers or infants.
Diagnostic interviews were conducted by psychologists or advanced psychology students after intensive training that
involved a review of DSM disorders, memorizing the SCID interview, review of training tapes, and structured role playing
over the course of several months. All interviewers reached agreement on at least 9/10 (anxiety disorder) training tapes
prior to interviewing subjects for this study. Diagnoses made during the study were reviewed in weekly staff meetings with
a psychologist in order to ascertain the reliability of diagnoses and maintain standards. Reliability between interviewers
was estimated on the basis of 10 taped interviews, and all of the classifications (anxious, control, depression) matched the
original ones ( = 1.00).
2.4. Diagnostic and assessment tools
2.4.1. Anxiety Screening Questionnaire (ASQ-15, Wittchen & Boyer, 1998)
The ASQ-15 is a diagnostic-specific, self-report screening measure for anxiety syndromes and depression. Each item
represents the primary criteria for a DSM-IV anxiety or depression disorder and is answered as yes or no. Test–retest
reliability and validity, when compared to DSM-IV diagnoses, has been shown to be good when the tool is administered by
telephone, as in this study.1
2.4.2. Structured Clinical Interview for DSM-IV Axis I Disorders (SCID IV, research version; First, Gibbon, Spitzer, & Williams,
1996)
This modular, semi-structured interview for the diagnosis of psychiatric disorders has become the general standard and
provides lifetime and current diagnoses.
2.4.3. Beck Depression and Anxiety Inventories (BDI, Beck, Ward, Mendelson, Mock, & Erbaugh, 1961; BAI, Beck, Epstein,
Brown, & Steer, 1988)
Both the BDI and BAI consist of 21 disorder-related symptoms (rated in severity, 0–3) and are frequently used self-report
measures. The inventories have good psychometric properties and are among the best self-rating tools for discriminating
anxiety from depression (Clark & Watson, 1991).
2.5. Observations
Observations were made in a play room in our laboratory, designed to be welcoming and comfortable for mothers and
infants. One standing camera was used to film the free play, teaching, and care giving episodes; and two wall-mounted
1
In addition to these assessment tools, mothers were administered the Infant Characteristics Questionnaire (fussy-difficult dimension only) (Bates,
Freeland, & Lounsbury, 1979). Results showed no group differences in infant temperament (M (SD): infants of controls 20.92 (4.90), infants of anxious
mothers 22.67 (6.59), with higher scores reflecting more difficult temperament). Results were not altered by the addition of temperament as a covariate.
140
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
cameras (one focused on the mother and the other on the baby) were used to film the face-to-face interactions. The signals
from these two cameras were transmitted through a digital timer and a split-screen generator into a video recorder to
produce a single image with a simultaneous front view of mother’s face, hands, and torso and the infant, in full view. This
configuration allowed for separate coding of mothers’ and infants’ behavior during the face-to-face interactions.
The order of the episodes was as follows: free play, teaching, still-face paradigm (SFP), face-to-face play with a stranger,
and care giving. Episodes began when the infants were alert and showed no signs of impending distress. If an infant became
very distressed (cried strongly for 10-s) during the still-face phase of the SFP, the reunion episode was initiated immediately
unless the infant was too distressed to continue. In these cases, the SFP was suspended and the infant was calmed prior to
beginning the stranger episode. If the infant could not be calmed, the SFP was terminated and the dyad did not partake in
the reunion phase. The episodes are described below.
2.5.1. Free play, teaching, care giving (floor episodes)
During these episodes, mother and infant were seated on the floor of the play room on a padded rug with a colorful sheet
over it. For the free play episode (5-min), several standard toys were placed on the sheet, and mothers were asked to play
with their infant. For the teaching episode (5-min), mothers were given a set of stackable, plastic boxes and asked to “teach
their infant the game”. For this episode, we purposely chose a game that was more appropriate for older infants because
we thought that teaching it to a young infant could elicit frustration and intrusive behavior on the part of parents who are
prone to such behavior. For the care giving episode (unlimited time), we asked mothers to dress the child in pajamas that
had “feet”, long sleeves, and snaps up both legs. Care giving was chosen as a task because it is a routine activity for mothers
and infants and may require some degree of negotiation if mothers’ and infants’ agendas are not the same.
2.5.2. Face-to-face still-face paradigm (with mother, SFP; Tronick et al., 1978)
During this episode, which is comprised of three phases, infants were seated in a baby-seat on a table facing their mother.
In the first phase, mothers and infants played freely without toys or use of a pacifier (face-to-face play, 2-min); in the second
phase, mothers gazed at their infant but did not respond to him/her (still-face, 2-min); in the third phase, mothers resumed
play with their infant (reunion, 2-min).
2.5.3. Stranger–infant face-to-face play
In this episode, infants and a stranger (one of six female research assistants) played face-to-face for 2-min. This episode
provided information on infants’ regulation of affect when faced with an unfamiliar person (without mother in sight).
2.6. Coding
Two types of coding were employed: global ratings on Likert scales reflecting important features of social interactions,
and time-event (continuous) coding that affords details about the timing of targeted responses (i.e., when they occurred
and for how long). In this study, free play, teaching, and care giving episodes (floor episodes) were coded by global ratings;
face-to-face interactions and infants’ affective behavior during the still-face phase and stranger episode were coded by
time-event coding.
2.6.1. Free play and teaching
Films were coded on 14 scales, adapted from the Rating Scale of Interactional Style (RSIS; Clark & Seifer, 1983) The RSIS
is a validated scoring system based on a 5-point Likert scale, with low scores reflecting no or infrequent shows of targeted
behavior and high scores reflecting frequent and clear shows. Behaviors coded for mother were: Overriding (parent disrupts
child’s ongoing behavior), Forcing (mother manipulates child physically), Imitation, Acknowledging (mother’s responsiveness to infant’s signals), Gaze (mothers’ focus on child or object of joint attention), Positive affect, Range of affect (range of
emotional expression accords with infant’s emotions, state, and activity), Vocalization (“motherese”), Sensitivity (supportive
presence), and Reciprocity (“give-and-take”). Infant scales included: Positive affect, Fussy, Initiation of play bids, and Positive
vocalization. These scales are similar to those used in previous mother–infant observation studies (Lyons-Ruth, Connell, Zoll,
& Stahl, 1987), including ones on maternal anxiety (Feldman et al., 1997).
For more detail and because hyperarousal is a common symptom of anxiety disorders (Grillon, 2008), coders entered
an “E” next to ratings of mother’s vocalization, acknowledgements, (positive) affect, and gaze if the observed behavior
was “exaggerated” (e.g., overly intense, too frequent; as in Bohlin & Hagekull, 1987). Together, the numerical rating (1–5)
reflected the degree of mothers’ sensitivity, and the E noted whether their behavior was exaggerated or not. For example, if
a mother spoke to her infant in a generally adult tone, but with some intonation and did so near-incessantly or very loudly,
Vocalization would be rated as a 3 (i.e., moderately sensitive), with an E. If a mother spoke with moderate sensitivity to her
infant, but the frequency and loudness of her vocalizations were considered “normal”, Vocalization would be coded as a
3, without an E. A previous study reported a negative relation between the number of Es and scores of infant’s “adequate”
interactive behavior (Bohlin & Hagekull, 1987).
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
141
2.6.2. Care giving
The coding protocol for the care giving episode was taken from the NICHD Study of Early Child Care Mother–Infant
Interactions (NICHD Early Child Care Research Network, 1997; Owen, unpublished). This protocol includes the following
scales: for mother – Negative Regard (shown in voice, touch, affect to infant), Sensitivity (appropriate, responsiveness,
warmth, and reciprocity), Positive Regard; for infant – Positive Affect, Negative Mood (negative expressions or vocalizations),
Sociability (bids for engagement). All of these behaviors were rated 1–4, generally reflecting “none” to “a great deal”. This
protocol was selected for coding the care giving episode, instead of the more detailed one used for free play and teaching,
because the care giving episode was often shorter than the other floor episodes; and infants’ responses during care giving
were somewhat limited due to the nature of the task. Previous studies have found a relation between maternal sensitivity
assessed by the NICHD scales at 6-months postpartum and infants’ attachment security at 15-months of age (McElwain &
Booth-LaForce, 2006).
2.6.3. Face-to-face interactions
Mothers’ and infants’ behavior was coded continuously according to the Infant and Caregiver Engagement Manual
(Weinberg & Tronick, 1999), which is based on the Monadic Phases Scoring System (Als, Tronick, & Brazelton, 1979). Monadic
phases are independent response categories created for the coding of second-by-second changes of affective engagement
during face-to-face interactions and represent a continuum from negative to positive engagement. Monadic phases were
defined as: (1) protest/negative; (2) withdrawn; (3) object/environment engagement; (4) social monitor; (5) play. Coding of
mothers’ and infants’ behavior was carried out separately, off-line using a computerized coding system (Noldus Observer,
version 5.031, Noldus Information Technology, Wageningen, Netherlands). Each coder used the exact same time for starting
the coding of each episode. During coding, each film was run at normal speed until a phase change was noted, then reversed
and played back at slow speed to enter the exact time of change.
2.6.4. Infant emotion regulation
Infants’ affective responses to the still-face and stranger were coded continuously for positive affect (smiles) and negative
affect/distress (e.g., looks sad, whimpers, cry).
2.7. Controls and reliability
Coders were trained extensively to at least K = .70 and 80% reliability on all measures; and all of the coders were blind as
to the mothers’ group-placement. To eliminate a potential source of bias in coding, coders were charged with coding one
episode only and, for the SFP, assistants coded either mother or infant, in one phase of the paradigm.
To assess interobserver reliability, 20% of each floor episode and each phase of the SFP and stranger episodes were selected
randomly and coded independently by two coders. For the floor episodes, mean intra-class correlations were: .82 (range
.76–.88) for maternal behavior and M = .92 (range .80–.96) for infant behavior.
For tests of inter observer reliability of time-series codings, percent agreement (defined as the proportion of time
that the two coders made identical ratings in the same 1-s interval) was evaluated by using the formula: agreements/agreements + disagreements. The number of times both coders agreed that a score did not occur was not considered
in this calculation to avoid inflating agreement. So calculated, mean agreement for mothers’ affect during face-to-face play
was .83 (range .76–.87), for infants’ affect during face-to-face play, .82 (range .72–.88), and for infants’ affect during challenge
(still-face and interaction with a stranger), .85 (range .78–.89). Reliability kappas also were conducted in 1-s time windows
and were M = .84 for mothers’ time-series (range .75–.89), M = .76 for infants’ time-series (range .74–.84) during face-to-face
play, and .79 (.77–.86) for infants’ affect during the challenging episodes.
2.8. Data reduction and final measures
2.8.1. Free play and teaching
Following previous studies on maternal anxiety and depression (Feldman et al., 1997), ratings on the RSIS scales were
averaged into three composites (per episode): Mother Sensitivity, Mother Intrusiveness, and Infant Involvement (see Table 2
for components of composite measures and estimates of coherence, Cronbach alpha). As defined here, Maternal Sensitivity represents the same sensitive–responsive construct, with minor variations, described in many longitudinal studies of
mother–infant interactions (e.g., Ainsworth, Blehar, Waters, & Wall, 1978; Crockenberg & McClusky, 1986; Kogan & Carter,
1996). Maternal Intrusiveness was included as a measure because it or similar constructs (overprotection, control) have
been related to anxiety in mothers of infants (Feldman et al., 1997) and theoretically (Chorpita & Barlow, 1998) and empirically to the development of anxiety in children in some studies (review in Wood, McLeod, Sigman, Hwang, & Chu, 2003;
meta-analysis in McLeod, Wood, & Weisz, 2007). Infant Involvement assessed the infant’s active participation in play and
the level of expressed positive affect. The final measures of exaggerated behavior reflected whether or not the mother had
shown exaggerated behavior in the free play or teaching episode.
142
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
Table 2
Composite measures of mother–infant interaction and scale coherence (Apha Cronbach, ˛).
Composite measure
Individual scales
Free play and teaching (global coding, 1–5)
Maternal sensitivity
Sensitivity, acknowledgement of infants’ signals + vocalization in the infant register + reciprocity + range of
affect + gaze + positive affect + imitation (free play ˛ = .85; teaching ˛ = .88)
Maternal intrusiveness
Over-riding (nonphysical coercion) + forcing (physical intrusiveness) (free play ˛ = .63; teaching ˛ = .78)
Infant involvement
Positive affect + positive vocalization + fussy (rev) + initiation of play bids (free play ˛ = .72; teaching ˛ = .74)
Care (global coding, 1–4, measure defined as mean rating)
Maternal sensitivity
Sensitivity + positive regard + negative regard (rev) (˛ = .84)
Infant affect
Positive affect + sociability + negative mood (rev) (˛ = .76)
Face-to-face (play and reunion, time-event coding)
Protest or sad expressions (rating 1 or 2)
Negative affecta
Show of social monitor or social play (rating 4 or 5)
Positive affectb
Infant regulation: stranger and still-face challenge (time-event coding)
Infant negative affect
Infants’ negative expression
Infant positive affect
Infants’ smile
a
b
Infants only.
Mother and infants, separately.
2.8.2. Care giving
Ratings of behavior during the care giving episode were reduced to two composite measures (Maternal Sensitivity and
Infant Affect), which reflected mothers’ sensitivity while dressing their infants and infants’ emotional state during the
episode.
2.8.3. Face-to-face play and reunion
Monadic and dyadic measures were obtained from the face-to-face play and reunion episodes. The monadic measures
were based on the proportions of the interaction (total seconds/total duration of episode) that mother and infant (separately)
were in a positive (social monitor or social play) or negative (anger/protest or withdrawn) state.
Proportions of mothers’ positive affect and infants’ positive affect during face-to-face play were arc-sine transformed
prior to analysis to correct for skewness of their distributions. Mothers’ proportions of negative affect were not analyzed
because so few mothers (<20%) showed negative affect during face-to-face play. Infants’ negative affect during face-to-face
play was highly skewed and recoded as dichotomous, as in Forbes, Cohn, Allen, and Lewinsohn (2004) among others. In sum,
final monadic measures included: (transformed) percent time in positive state for mother and infant and dichotomized
negative state for infant.
To derive the dyadic measures, we followed previous studies (Cohn & Tronick, 1988; Weinberg, Tronick, Cohn, & Olson,
1999) and averaged ratings within each 1-s period, resulting in one time-series for mothers’ behavior and one time-series
for infants’ behavior for each face-to-face interaction. From these data, four measures of dyadic coordination were derived.
(1) Matching: This measure is defined as the extent to which mothers and infants shared joint affective states at the same
moment in time (i.e., within the same 1-s interval). A measure of matched affect has been used by Weinberg et al. (1999)
and others (e.g., Field et al., 1990; Tronick & Cohn, 1989). As in these studies, matching was calculated as the proportion
of total interaction time that mothers and infants were in the monadic phase of social monitor or social engagement in
the same 1-s interval (social match). This measure was arc-sine transformed prior to analysis to correct for skewness
of its distribution. Proportion of time in negative matches was not subjected to analysis because there were few such
matches during mother–infant face-to-face interactions.
(2) Degree of synchrony: Whereas matching focuses on temporal contiguity and content of behavior (i.e., valence of expressions), synchrony focuses on the extent to which mothers and infants change their affective states together over time,
regardless of the content of their behavior. Thus some dyads may seldom be in matching states but may have high
synchrony scores because infant and mother tend to change in the same affective direction over the course of the
interaction.
As elsewhere, synchrony was computed separately for each dyad using time-series analysis of the two time lines
(one for mother and one for infant) describing the second-by-second changes in monadic states across each face-to-face
interaction. Derivation of synchrony involved the following steps: First, we “removed” the auto-correlated component
of the time-series that reflects the natural tendency to cycle between states of engagement and disengagement, The
auto-correlated component was estimated using separate Autoregressive Integrated Moving Average (ARIMA) models
for each series, and the best model was estimated, according to autocorrelation and partial autocorrelation plots (i.e.,
visual representations of the time-series and its autocorrelation matrix at different lags). Residuals of the “best model”
were then checked for lack of autocorrelation. Second, cross correlation functions (CCF) for each dyad were computed
with the two series of residuals, and the largest cross correlation coefficient on the CFF plot was taken as degree of
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
143
synchrony, which ranges from zero, implying no association between the two time-series to one, describing a perfect
match between the two time-series.
(3) Lead–lag relations: Lead–lag relations reflect the direction of dominance in the interaction and identify that partner
who is leading the changes in affective states across the interaction. Lead–lags are derived only when the interaction
is synchronous and when significant relations are found between the partners’ behavior, meaning that the CFF was
significant and at least one significant peak appeared on the CFF plot. A dyad received a score of one, if there was a
positive peak (parent follows infant), 0 if there was a negative peak (infant follows parent), and 2 if there was a negative
and positive peak (mutual synchrony).
(4) Time-lag-to-synchrony: The time-lag-to-synchrony variable indicates the time in seconds between change in one partner’s behavior and corresponding change in the other’s or as described elsewhere, “the time required for the dyadic
system to settle into a coregulated exchange” (Feldman, 2003, p. 11). Similar to the lead–lag relation variable, the
time-lag-to-synchrony variable assumed a positive value only when at least one significant peak appeared on the CCF.
The time-lag to the first significant peak, whether positive or negative, was used to index time-lag-to-synchrony. The
time-lag-to-synchrony variables were within the range of 1 (implying one second to the partner’s responsiveness) and
7.
2.8.4. Infants’ emotion regulation
The proportion of time that infants’ showed positive affect or distress to stranger and to mothers’ still-face was sharply
skewed and dichotomized prior to analyses. Accordingly, the two measures reflected whether or not the infants expressed
distress or positive affect during the each of the challenging episodes.
2.9. Data analysis
Preliminary analyses tested the normality of measures; and if kurtosis or skewness was unacceptable (see Tabachnick &
Fidell, 1996), variables were transformed as described in Sections 2.8.3–2.8.4. Additionally, we tested for group differences
on background measures. To examine the reliability and validity of final measures, correlations and regression models
evaluated the stability of measures across episodes and tested for relations between mothers’ and infants’ behavior within
episodes.
To address question 1, multivariate and univariate analyses (general linear models, GLMs) were used to compare anxious
and control groups on continuous behavioral measures (maternal sensitivity, maternal intrusiveness, infant involvement)
derived from the floor episodes and the 1st face-to-face interaction; chi square was used to test for group differences on the
dichotomous variable (infants’ negative affect). Log-linear analysis tested for group differences in lead–lag relations.
To address question 2, (transformed) continuous measures (social play and social monitor, positive match, degrees of
synchrony, time-lag-to-synchrony) derived from the 1st face-to-face interaction and the reunion episode were compared
by univariate repeated measure GLMs, with episode as the repeated measure. A multivariate analysis across measures was
not employed because final measures were derived from the same raw data and therefore were not strictly independent.
To test for group differences in categorical measures (infants’ negative affect, lead–lag relations) during the 1st and reunion
face-to-face interaction, data were subjected to separate conditional logistic regression analyses (for repeated measures;
Agresti, 1996).
To address question 3, we compared the proportion of infants in each group who showed positive affect and negative
affect in each of the two challenging by chi square analyses.
3. Results
3.1. Preliminary analyses
3.1.1. Missing data
Data on free play are missing on one dyad due to technical (camera) problems; no data are missing from teaching or the
1st face-to-face interaction. No data are missing from the stranger episode or the still-face phase of the SFP, although for two
infants, the latter was terminated early because they became very distressed. The data from four controls and two anxious
dyads are missing from the 2nd face-to-face interaction because the infants were too distressed after the still-face challenge
to continue onto the reunion. Two dyads did not partake in the care giving episode because the infants were too tired.
3.1.2. Demographics and background
There were no group differences in mothers’ age, religiosity (secular vs. religious), working status (employed, not
employed), or education (Table 1). The anxious group scored significantly higher than the control group on both the
BAI (M = 5.80, SD = 4.11 vs. M = 1.49, SD = 1.84, t (91) = 6.86, p < .0001) and BDI (M = 5.68, SD = 4.45 vs. M = 2.46, SD = 2.53, t
(91) = 4.30, p < .0001). As noted in Table 1, very few women in the anxious group and control group were in therapy or taking
psychotropic medication at the time of the observation.
144
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
Table 3
Mean scores of behavioral measures obtained from free play, teaching, and care giving episodes, by group.
Controls
*
Anxious
M
SD
M
SD
Free play
M. Sensitivity
M. Intrusive
I. Involve
3.56
1.76
4.34
.63
.77
.48
3.73
1.72
4.27
.66
.73
.63
Teaching
M. Sensitivity
M. Intrusive
I. Involve
3.76
1.95
3.97
.68
.79
.76
3.60
1.80
3.78
.68
.76
.85
Care
M. Sensitivity
I. Affect
3.15
2.78
.59
.82
3.23
2.89
.43
.79
p < .05.
3.1.3. Measures of maternal and infant behavior: reliability and validity
(1) Correlations across episodes: Significant correlations were found between measures of maternal sensitivity (free
play–teaching, r = .43, p = .0001; teaching–care, r = .21, p = .04, but not between care giving-free play), maternal intrusiveness (free play-teaching r = .31, p < .0001), and mothers’ affect during face-to-face interactions (r = .32, p = .0001). Measures
of infants’ behavior were also correlated across episodes (Infant Involvement: free play–teaching, r = .48, p = .0001; Infant
Affect: 1st phase—reunion phase of the SFP, r = .43, p < .0001; Infant Affect: care giving—1st phase of SFP, r = 2.0, p = .05;
care–reunion phase of the SFP, r = .26, p = .015). In addition, infants who showed negative affect during the 1st phase of
the SFP were more likely to show negative affect during the reunion phase (McNemar test for related samples, X2 (1,
N = 87) = 8.04, p < .005); infants who showed negative affect to mothers’ still-face phase were more likely to show negative affect to the stranger (McNemar, X2 (1, N = 93) = 25.41, p < .0001); and infants who showed positive affect to their
mothers’ still-face were more likely to show positive affect to the stranger (McNemar, X2 (1, N = 93) = 33.97, p < .0001).
(2) Intercorrelations between maternal behavior and infant behavior within episodes: Findings show that: (1) Maternal Sensitivity and Maternal Intrusiveness during free play were correlated with Infant Involvement during the same episode
(r = .33, p < .001; r = −.30, p = .004, respectively) and, together, Sensitivity and Intrusiveness accounted for 12.9% of the
variance in Infant Involvement (F(2, 89) = 6.57, p = .002), (2) Maternal Sensitivity and Intrusiveness during the teaching
episode predicted Infant Involvement (r = .54, p < .0001, r = −.22, p = .016, respectively) and jointly explained 30% of the
variance in Infant Affect (F(2, 90) = 19.10, p < .0001), (3) the correlation between mothers’ sensitivity during care giving
and Infant Affect during the care giving episode approached significance (r = .20, p = .057), and (4) there was a significant
relation between mothers’ positive affect and infants’ positive affect during the 1st phase (r = .24, p = .019) and during
the reunion phase of the SFP (r = .25, p = .017).
3.2. Primary analyses
3.2.1. Hypothesis 1: Anxious vs. control dyads during floor episodes and 1st face-to-face play
Tables 3 and 4 show the means and standard deviations of the behavioral composites derived from each floor episode and
the 1st face-to-face interaction by group. Separate multivariate GLM analyses tested for group differences in Maternal Sensitivity across all three floor time-episodes and for group differences in Maternal Intrusiveness and Infant Involvement across
free play and teaching episodes. Results were consistently negative, as were results of exploratory analyses in which Episode
was entered as a between-group factor based on findings of Ginsburg, Grover, Cord, & Ialongo (2006). Exploratory univariate
tests applied to each floor measure, taken separately, also yielded null results. Adding to these negative findings, univariate tests revealed no group differences in infants’ positive affect, matched positive affect, or time-lag-to-synchrony during
the 1st face-to-face interaction; nor did infants’ negative affect during the 1st interaction or lead–lag relations distinguish
between groups.
In fact, the only behavioral measure that discriminated the anxious mothers and controls were related to the notation
“E”, reflecting mothers’ exaggerated responsiveness (during the teaching and free play episodes). Specifically, 61.8% (n = 21)
of the anxious mothers acknowledged, gazed, expressed positive affect, and/or talked in an exaggerated fashion in the free
play and/or teaching episode(s) compared to 37.3% (n = 22) of the control mothers (X2 (1, N = 93) = 5.20, p = .023).
3.2.2. Hypothesis 2: Group differences in affect and coordination before and after the still-face phase
Repeated measures GLMs, with episode as the repeated measure, examined main effects of Episode (across control
and anxious groups), Group, and Episode × Group on measures derived from the 1st face-to-face interaction and reunion
phase of the SFP. Significant main effects of Episode were shown for mothers’ positive affect (1st interaction > reunion,
F(1, 85) = 12.14, p = .001, 2p = .13); infants’ positive affect (1st interaction > reunion, F(1, 85) = 3.90, p = 05, 2p = .03), infants’
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
145
Table 4
Measures based on microanalytic coding of face-to-face interactions, by group.
Play 1
Reunion
Control
Anxious
Control
Anxious
M
SD
M
SD
M
SD
M
SD
Mother affect
Positive
66.66
21.51
67.00
19.53
59.23
23.44
65.53
21.57
Infant affect
Positive
Negative (% infants)
29.85
32.2
18.36
26.48
26.5
20.12
24.23
54.5
18.26
25.48
40.6
19.12
Positive match
Degree of synchrony
Time-lag to synch (s)
18.67
.14
2.33
7.36
.07
1.43
18.90
.12
2.54
9.77
.08
2.01
15.82
.13
2.63
11.82
.05
2.62
17.35
.13
2.56
10.35
.07
2.03
Lead–lag (% dyads)
No peak
Baby leads
Mother leads
Mutual
10.2
11.9
22.0
55.9
8.8
14.7
26.5
50.0
7.3
16.4
20.0
56.4
9.4
21.9
12.5
56.3
Table 5
Percentage of infants who showed positive and negative affect during still-face and
stranger challenges.
% Control
% Anxious
Still-face
Positive
Negative
52.5
45.8
50.0
23.5*
Stranger
Positive
Negative
64.4
30.5
64.7
5.9**
*
**
p < .05.
p < .005.
negative affect (1st interaction < reunion, conditional logit: Wald = 11.30, p < .0001, 97% CI, .12–.54), and Matched Positive
Affect (1st interaction > reunion, F(1, 85) = 4.54, p = .04, 2p = .015). In contrast, none of the variables showed significant Group
and/or Group × Episode interactions, though there were two trends that are worthy of note: (1) a Group × Episode interaction
on Matched Positive Affect (F(1, 85) = 3.33, p = .071, 2p = .04), reflecting a somewhat more robust decline from the 1st faceto-face interaction to the reunion among control dyads compared to anxious dyads, and (2) a parallel Group × Episode
interaction on Infant Positive Affect (F(1, 85) = 3.38, p = .07, 2p = .04) reflecting a more robust decline in smiling among
infants of controls than infants of anxious mothers.
3.2.3. Hypothesis 3: Infants’ affect during still-face and interaction with a stranger
Table 5 displays the percentages of infants that showed positive and negative affect during the still-face phase of the SFP
and stranger episode. As shown, a larger proportion of control infants showed negative affect during the still-face (X2 (1,
N = 93) = 4.54, p = .03) and stranger challenges: (X2 (1, N = 93) = 7.75, p = .005) compared to the infants of anxious mothers.
There were no group differences in the proportion of infants who showed positive affect during either challenge.
4. Discussion
The present study aimed at discerning atypical features of interactions between anxious mothers and their infants.
We also looked for differences in infants’ emotional response to mild challenges. To address these issues, we recruited a
community sample of women and selected those with current, clinical anxiety and excluded women with depression so
to provide a “clean” picture of social interactions between anxious mothers and their infants. To provide a comprehensive
view, we observed different types of mother–infant interactions and examined infants’ responses to two challenges. For
analysis, we derived a broad set of measures from each participant, using time-event coding and global rating scales.
A number of results are worthy of mention. First, we found no evidence for deficits in general maternal sensitivity or intrusiveness, although more anxious mothers than controls behaved in an exaggerated manner during the free play and teaching
episodes. We presume that this distinction reflects the hyperarousal that characterizes most anxiety disorders, although the
finding seems somewhat at odds with previous descriptions of anxious mothers as less engaged with their infants during play
(Murray et al., 2007; also Turner, Beidel, Roberson-Nay, & Tervo, 2003; Woodruff-Borden, Morrow, Bourland, & Cambron,
2002). These differences may reflect variations in the composition of the proband groups or in procedures. Alternatively,
146
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
we might consider mothers’ over- or under-responding as reflecting a common difficulty in emotion regulation (Kaitz &
Maytal, 2005), which is a core feature of affective disorders including anxiety (Rodebaugh & Heimberg, 2008). In any case, as
noted by Murray et al. (2007), the discerning features of dyadic interactions between (low risk) anxious mothers and infants
seem more subtle than those described in many observation studies of depressed mothers and their infants (e.g., review in
Goodman, 2007).
Of particular note, infants in our sample and the infants of mothers with social phobia described by Murray et al. (2007)
seemed less communicative and less emotional during social challenges. In the present study, this was seen in the smaller
proportion of “anxious infants” who showed distress to strangers and to mothers’ still-face, and in Murray et al. (2007),
this was seen in infants’ less positive engagement with a stranger. Interestingly, infants of depressed, high-risk mothers
also have been described as less interactive and less upset when their mothers were inattentive to them (Field et al., 2007;
Hart, Field, Letourneau, & Del Valle, 1998; also see Kiser, Bates, Malsin, & Bayles, 1986) or absent for a short period of time
(Dawson, Klinger, Panagiotides, Hill, & Spieker, 1992; Pelàez-Nogueras, Field, Hossain, & Pickens, 1996). As suggested by
Field et al. (2007), this kind of behavior could reflect flattened affect, inhibition, or avoidance on the part of infants who may
be stressed and stressors related to having an affectively disordered mother. These stressors may include routine exposure
to their mothers’ anxiety-related behavior (Murray et al., 2007) or other stressors like abnormal family functioning (Bögels
& Brechman-Toussaint, 2006) that may be related to having a highly anxious mother.
Before ending, we mention several limitations of the present study. First, the sample size was relatively small, and we
may not have had the power to detect small effect sizes, although medium to large effects should have been detected.2 A
second caveat was that inclusion criteria stipulated that the women in the sample were first-time mothers and married,
and this may limit the generalizability of our findings. Also, the sample was well educated, by the women’s reports. Third,
our episodes may have been too brief or our coding protocols may not have captured behaviors that are related to anxiety,
although we used a broad range and ones that seemed to be good candidates. Fourth, our anxious group was comprised of
women with panic, PTSD, or social phobia, and though these disorders share a component of hyperarousal, it is possible that
variations within the anxious group obscured differences between the anxious group and controls.
Certainly more research is needed in order to understand the social environment of infants of anxious mothers and how
it contributes to the transmission of anxiety from parent to child. For this, it will be important to identify profiles of maternal
behaviors related to specific anxiety disorders, as well as features of behavior that seem to be common to anxiety, in general.
For both these purposes, it seems important to consider new measures and paradigms that are tailor-made for the study of
maternal anxiety as shown by the usefulness of our E notation and of the novel paradigm used by Murray et al. (2007) to pick
up signs of mothers’ social phobia (also see Hock, McBride, & Gnezda, 1989). Best would be if these efforts were embedded
in longitudinal designs that incorporate environmental variables (e.g., review in Rutter, Moffitt, & Caspi, 2006), which may
explain variance in children’s outcome. Finally, certain genes (e.g., short allele variant of the 5 HTT) need to be considered as
significant moderators of the relation between maternal anxiety and children’s behavior/developmental problems, given the
risk associated with some genotypes (Fox et al., 2005; review in Rutter et al., 2006). In short, there is much to be done before
strong conclusions can be made regarding the links between maternal anxiety, maternal behavior, and child development;
and the studies available should be regarded as just the beginning.
As part of these efforts, the present study offers data on the interactive behavior of infants and their anxiety-disordered
mothers, who like many women in this category, were not in treatment or medicated (Tam, Newton, Dern, & Parry, 2002).
In all, the data add to the few available on the behavior of anxiety-disordered mothers and perhaps most important, they
demonstrate again that some children of anxious mothers can be distinguished from children of healthy mothers during
infancy.
Acknowledgements
Marsha Kaitz, Department of Psychology; Hilla Rubin Maytal, Department of Psychology (now at the Department of
Psychology, Bar Ilan University, Ramat Gan, Israel); Liat Bergman, Department of Psychology (now at Department of Psychology, The Academic College of Tel-Aviv-Yaffo, Tel-Aviv, Israel); Noa Devor, Department of Sociology and Anthropology;
David Mankuta, Department of Obstetrics & Gynecology.
This study was supported by the Israel Science Foundation (900/02-34) to the first author. We thank the many students
who recruited, interviewed the mothers, and painstakingly coded the films. We also thank the nurses in the well-baby clinics
who helped us recruit mothers and Dr. Ronit Nirel, Department of Statistics, Hebrew University, who provided statistical
advice. We are indebted to the mothers and infants who participated in the study.
References
Agresti, A. (1996). An introduction to categorical data analysis. New York, NY: John Wiley.
Ainsworth, M. D. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of attachment: A psychological study of the strange situation. Hillsdale, NJ: Erlbaum.
2
The results of post hoc power analyses suggest that for detecting medium size effects, chi-square tests in hypotheses 1 and 3 had a power estimate of
.82, GLM design in hypothesis 1 had a power estimate of .63, and repeated-measures GLM in hypothesis 2 had a .99 power estimate (G*Power; Erdfelder,
Faul, & Buchner, 1996).
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
147
Als, H., Tronick, E., & Brazelton, T. B. (1979). Analysis of face-to-face interactions in infant–adult dyads. In M. E. Lamb, S. J. Suomi, & G. R. Stephenson (Eds.),
Social interaction analysis: Methodological issues. Madison: University of Wisconsin Press.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
Barlow, D. H. (2002). Origins of apprehension, anxiety disorders, and related disorders. In D. H. Barlow (Ed.), Anxiety and its disorders: The nature and
treatment of anxiety and panic (pp. 252–291). New York: Guildford Press.
Bates, J. E., Freeland, C. A. B., & Lounsbury, M. L. (1979). Measurement of infant difficultness. Child Development, 50, 794–803.
Beck, A. T., Epstein, N., Brown, G., & Steer, R. A. (1988). An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and
Clinical Psychology, 56, 893–897.
Beck, A. T., Ward, C. H., Mendelson, M., Mock, J. E., & Erbaugh, J. K. (1961). An inventory for measuring depression. Archives of General Psychiatry, 4, 561–571.
Blissett, J., Meyer, C., & Haycraft, E. (2007). Maternal mental health and child feeding problems in a non-clinical group. Eating Behaviors, 8, 311–318.
Bögels, S. M., & Brechman-Toussaint, M. L. (2006). Family issues in child anxiety: Attachment, family functioning, parental rearing, and beliefs. Clinical
Psychology Review, 26, 834–856.
Bohlin, G., & Hagekull, B. (1987). “Good mothering”: Maternal attitudes and mother–infant interaction. Infant Mental Health Journal, 8, 352–363.
Bowlby, J. (1980). Attachment and Loss New York: Basic Books.
Bowlby, J. (1988). Developmental psychiatry comes of age. American Journal of Psychiatry, 145, 1–10.
Chorpita, B. F., & Barlow, D. H. (1998). The development of anxiety: The role of control in the early environment. Psychological Bulletin, 124, 3–21.
Clark, G. N., & Seifer, R. (1983). Facilitating mother–infant communication: A treatment model for high risk and developmentally delayed infants. Infant
Mental Health Journal, 4, 67–82.
Clark, L. A., & Watson, D. (1991). Tripartite model of anxiety and depression: Psychometric evidence and taxonomic implications. Journal of Abnormal
Psychology, 100, 316–336.
Cohn, J. F., & Tronick, E. Z. (1988). Mother–infant face-to-face interaction: Influence is bidirectional and unrelated to periodic cycle in either partner’s
behavior. Developmental Psychology, 24, 386–392.
Crockenberg, S. B., & McClusky, K. (1986). Change in maternal behavior during the baby’s first year of life. Child Development, 57, 746–753.
Dawson, G., Klinger, L. G., Panagiotides, H., Hill, D., & Spieker, S. (1992). Frontal lobe activity and affective behavior of infants of mothers with depressive
symptoms. Child Development, 63, 725–737.
Degnan, K. A., & Fox, N. A. (2007). Behavioral inhibition and anxiety disorders: Multiple levels of a resilience process. Development and Psychopathology, 19,
729–746.
Erdfelder, E., Faul, F., & Buchner, A. (1996). GPower: A general power analysis program. Behavior Research Methods, Instruments, & Computers, 28, 1–11.
Feldman, R. (2003). Infant–mother and infant–father synchrony: The coregulation of positive arousal. Infant Mental Health Journal, 24, 1–23.
Feldman, R., Greenbaum, C. W., Mayes, L. C., & Erhlich, S. H. (1997). Change in mother–infant interactive behavior: Relations to change in the mother, the
infant, and the social context. Infant Behavior and Development, 20, 151–163.
Feldman, R., Greenbaum, C. W., & Yirmiya, N. (1999). Mother–infant affect synchrony as an antecedent of the emergence of self-control. Developmental
Psychology, 35, 223–231.
Field, T., Healy, B. T., Goldstein, S., & Guthertz, M. (1990). Behavior-state matching and synchrony in mother–infant interactions of nondepressed versus
depressed dyads. Developmental Psychology, 26, 7–14.
Field, T., Hernandez-Reif, M., & Diego, M. (2006). Intrusive and withdrawn depressed mothers and their infants. Developmental Review, 26, 15–30.
Field, T., Hernandez-Reif, M., Diego, M., Feijo, L., Yanexy, V., Gil, K., et al. (2007). Still-face and separation effects nondepressed mother–infant interactions.
Infant Mental Health Journal, 28, 314–323.
Field, T., Hernandez-Reif, M., Vera, Y., Gil, K., Diego, M., Bendall, D., et al. (2005). Anxiety and anger effects on depressed mother–infant spontaneous and
imitative interactions. Infant Behavior and Development, 28, 1–9.
First, M. B., Gibbon, M., Spitzer, R. L., & Williams, J. B. W. (1996). Structured Clinical Interview for DSM-IV Axis (research version). New York, NY: Biometric
Research.
Forbes, E. E., Cohn, J. F., Allen, N., & Lewinsohn, P. (2004). Infant affect during parent–infant interaction at 3 and 6 months: Differences between mothers
and fathers and influence of parent history of depression. Infancy, 5, 61–84.
Fox, N. A., Nichols, K. E., Henderson, H. A., Rubin, K., Schmidt, L., Hamer, D., et al. (2005). Evidence for a gene–environment interaction in predicting behavioral
inhibition in middle childhood. Psychological Science, 16, 921–926.
Ginsburg, G. S., Grover, R. L., Cord, J. J., & Ialongo, N. (2006). Observational measures of parenting in anxious and nonanxious mothers: Does type of task
matter? Journal of Clinical Child and Adolescent Psychology, 35, 323–328.
Goodman, S. H. (2007). Depression in mothers. Annual Review of Clinical Psychology, 3, 107–135.
Grillon, C. (2008). Models and mechanisms of anxiety: Evidence from startle studies. Psychopharmacology, 199, 421–437.
Haley, D. W., & Stansbury, K. (2003). Infant stress and parent responsiveness: Regulation of physiology and behavior during still-face and reunion. Child
Development, 74, 534–1546.
Ham, J., & Tronick, E. (2006). Infant resilience to the stress of the still-face. Annals of New York Academy of Science, 1094, 297–302.
Hart, S., Field, T., Letourneau, M., & Del Valle, C. (1998). Jealousy protests in infants of depressed mothers. Infant Behavior and Development, 21, 137–148.
Hock, E., McBride, S., & Gnezda, M. T. (1989). Maternal separation anxiety: Mother–infant separation from the maternal perspective. Child Development, 60,
793–802.
Isabella, R. A., & Belsky, J. (1991). Interactional synchrony and the origins of infant–mother attachment: A replication study. Child Development, 62, 373–384.
Kaitz, M., & Maytal, H. (2005). Interactions between anxious mothers and infants: An integration of theory and research findings. Infant Mental Health
Journal, 26, 570–597.
Kiser, L. J., Bates, J. W., Malsin, C. A., & Bayles, K. (1986). Mother–infant play at six months as a predictor of attachment security at thirteen months. Journal
of the American Academy of Child Psychiatry, 25, 68–75.
Kogan, N., & Carter, A. S. (1996). Mother–infant reengagement following the still-face: The role of maternal emotional availability in infant affect regulation.
Infant Behavior and Development, 19, 359–370.
Kopp, C. B. (1989). Regulation of distress and negative emotions: A developmental view. Developmental Psychology, 25, 343–354.
Lovejoy, M. C., Graczyk, P. S., O’Hare, E., & Neuman, G. (2000). Maternal depression and parenting behavior: A meta-analytic review. Clinical Psychology
Review, 20, 561–592.
Lyons-Ruth, K., Bronfman, E., & Parsons, E. (1999). Maternal frightened, frightening, or atypical behavior and disorganized infant attachment patterns.
Monographs of the Society for Research in Child Development, 64(3), 67–96.
Lyons-Ruth, K., Connell, D. B., Zoll, D., & Stahl, J. (1987). Infants at social risk: Relations among infant maltreatment, maternal behavior, and infant attachment
behavior. Developmental Psychology, 23, 223–232.
McElwain, N. L., & Booth-LaForce, C. (2006). Maternal sensitivity to infant distress and nondistress as predictors of infant–mother attachment security.
Journal of Family Psychology, 20, 247–255.
McLeod, B. D., Wood, J. J., & Weisz, R. J. (2007). Examining the association between parenting and childhood anxiety: A meta-analysis. Clinical Psychology
Review, 27, 55–172.
Moore, G. A., & Calkins, S. D. (2004). Infants’ vagal regulation in the still-face paradigm is related to dyadic coordination of mother–infant interaction.
Developmental Psychology, 40, 1068–1080.
Moore, G. A., Cohn, J. F., & Campbell, S. B. (2001). Infant affective responses to mothers’ still-face at 6 months differentially predict externalizing and
internalizing behaviors at 18 months. Developmental Psychology, 37, 706–714.
Murray, L., Cooper, P., Creswell, C., Schofield, E., & Sack, C. (2007). The effects of maternal social phobia on mother–infant interactions and infant social
responsiveness. Journal of Child Psychology and Psychiatry, 48, 45–52.
148
M. Kaitz et al. / Infant Behavior & Development 33 (2010) 136–148
NICHD Early Child Care Research Network. (1997). The effects of infant child care on infant–mother attachment security: Results of the NICHD study of
early child care. Child Development, 68, 860–879.
Nicol-Harper, R., Harvery, A. G., & Stein, A. (2007). Interactions between mothers and infants: Impact of maternal anxiety. Infant Behavior and Development,
30, 161–167.
Nover, A., Shore, M. F., Timberlake, E. M., & Greenspan, S. I. (1984). The relationship of maternal perception and maternal behavior: A study of normal
mothers and their infants. American Journal of Orthopsychiatry, 54, 210–222.
Owen, M. T. (unpublished). The NICHD study of early child care mother–infant interaction scales.
Park, S.-Y., Belsky, J., Putnam, S., & Crnic, K. (1997). Infant emotionality, parenting, and 3-year inhibition: Exploring stability and lawful discontinuity in a
male sample. Developmental Psychology, 33, 218–227.
Pelàez-Nogueras, M., Field, T. M., Hossain, Z., & Pickens, J. (1996). Depressed mothers’ touching increases infants’ positive affect and attention in still-face
interactions. Child Development, 67, 1780–1792.
Reck, C., Hunt, A., Fuchs, T., Weiss, R., Noon, A., Moehler, E., et al. (2004). Interactive regulation of affect in postpartum depressed mothers and their infants:
An overview. Psychopathology, 37, 272–280.
Rodebaugh, T. L., & Heimberg, R. G. (2008). Emotion regulation and the regulation and the anxiety disorders: Adopting a self-regulation perspective. In A.
Vingerhoets, & J. Denollet (Eds.), Emotion regulation: Conceptual and clinical issues (pp. 140–149). New York, NY: Springer Science + Business Media.
Rutter, M. (2005). Environmentally mediated risks for psychopathology: Research strategies and findings. Journal of the American Academy of Child Adolescent
Psychiatry, 44, 3–18.
Rutter, M., Moffitt, T. E., & Caspi, A. (2006). Gene–environment interplay and psychopathology: Multiple varieties but real effects. Journal of Child Psychology
and Psychiatry, 47(3/4), 226–261.
Schore, A. N. (2001). The effects of early relational trauma on right brain development, affect regulation, and infant mental health. Infant Mental Health
Journal, 22, 201–269.
Schreier, A., Wittchen, H.-U., Höfler, M., & Lieb, R. (2008). Anxiety disorders in mothers and their children: Prospective longitudinal community study. The
British Journal of Psychiatry, 192, 308–309.
Shonkoff, J. P., & Phillips, D. A. (Eds.). (2000). From neurons to neighborhoods. Washington, DC: National Academy Press.
Stifter, C. A., Coulehan, C. M., & Fish, M. (1993). Linking employment to attachment: The mediating effects of maternal separation anxiety and interactive
behavior. Child Development, 64, 1451–1460.
Swain, J. E., Lorberbaum, J. P., Kose, S., & Strathearn, L. (2007). Brain basis of early parent–infant interactions: Psychology, physiology, and in vivo functional
neuroimaging studies. Journal of Child Psychology and Psychiatry, 48, 262–287.
Tabachnick, B. G., & Fidell, L. S. (1996). Using multivariate statistics (3rd Ed.). New York: Harper Collins.
Tam, L. W., Newton, R. P., Dern, M., & Parry, B. L. (2002). Screening women for postpartum depression at well baby visits: Resistance encountered and
recommendation. Archives of Women’s Mental Health, 5, 79–82.
Thompson, R. A. (1994). Emotion regulation: A theme in search of definition. Monographs of the Society for Research in Child Development, 59(2–3), 25–52.
Tronick, E. Z., Als, H., Adamson, L., Wise, S., & Brazelton, T. B. (1978). The infant’s response to entrapment between contradictory messages in face-to-face
interaction. Journal of Child Psychiatry, 17, 1–13.
Tronick, E. Z., & Cohn, J. F. (1989). Infant–mother face-to-face interaction: Age and gender differences in coordination and the occurrences of miscoordination.
Child Development, 60, 85–92.
Turner, S. M., Beidel, D. C., Roberson-Nay, R., & Tervo, K. (2003). Parenting behaviors in parents with anxiety disorders. Behaviour Research and Therapy, 41,
541–554.
Warren, S. L., Gunnar, M. R., Kagan, J., Anders, T. F., Simmens, S. J., Rones, M., et al. (2003). Maternal panic disorder: Infant temperament, neurophysiology,
and parenting behaviors. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 814–825.
Weinberg, M. K., Beeghly, M., Olson, K. L., & Tronick, E. (2008). Effects of maternal depression and panic disorder on mother–infant interactive behavior in
the face-to-face still-face paradigm. Infant Mental Health Journal, 29, 472–491.
Weinberg, M. K., & Tronick, E. Z. (1998a). Emotional characteristics of infants associated with maternal depression and anxiety. Pediatrics, 102, 1298–1304.
Weinberg, M. K., & Tronick, E. Z. (1998b). The impact of maternal psychiatric illness on infant development. Journal of Clinical Psychiatry, 59, 53–61.
Weinberg, M. K. & Tronick, E. Z. (1999). Infant and caregiver engagement phases (ICEP). Unpublished manuscript. Boston, MA: Children’s Hospital and
Harvard Medical School.
Weinberg, M. K., Tronick, E. Z., Cohn, J. F., & Olson, K. L. (1999). Gender differences in emotional expressivity and self-regulation during early infancy.
Developmental Psychology, 35, 175–188.
Wijnroks, L. (1999). Maternal recollected anxiety and mother–infant interaction in preterm infants. Infant Mental Health Journal, 20, 393–409.
Wittchen, H.-U., & Boyer, P. (1998). Screening for anxiety disorders. Sensitivity and specificity of the Anxiety Screening Questionnaire (ASQ-15). British
Journal of Psychiatry, 173(Suppl. 14), 10–17.
Wood, J., McLeod, B. D., Sigman, M., Hwang, W.-C., & Chu, B. C. (2003). Parenting and childhood anxiety: Theory, empirical findings, and future directions.
Journal of Child Psychology and Psychiatry, 44, 134–151.
Woodruff-Borden, J., Morrow, C., Bourland, S., & Cambron, S. (2002). The behavior of anxious parents: Examining mechanism of transmission. Journal of
Clinical Child and Adolescent Psychology, 31, 364–374.