Objectives Stages of Hemostasis
advertisement

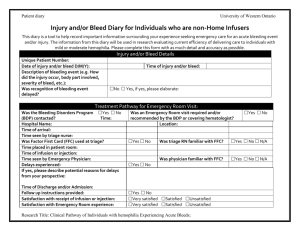
2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children Objectives Von Willebrand Disease and Other Bleeding Disorders in School Aged Children Jessie Pindilli,BSN, RN Program Coordinator UW Hospital & Clinics Comprehensive Program for Bleeding Disorders Describe normal hemostasis Describe Von Willebrand Disease and Hemophilia Identify signs and symptoms of bleeding disorders, particularly in female students Describe what to do in an emergency Recognize potential barriers that children with a bleeding disorder may face at school April 24, 2015 Comprehensive Care at Hemophilia Treatment Centers (HTC) Team members all have expertise and experience in treating bleeding disorders – Core members include hematologist, nursing, social work, and physical therapy – Comprehensive, interdisciplinary care model Access to clotting factor concentrates Over 130 HTCs throughout the U.S. & territories Rate of hospital stays for bleeding-related events among patients seen in HTC’s was 40% lower than the rates of patients seen in other care facilities (Soucie et al, 2000) Patients seen in HTCs are 40% less likely than those seen elsewhere to die of a hemophilia related complication. (Soucie et al, 200) Wisconsin: Milwaukee (Children’s Hospital of Wisconsin), Madison (University of WI Hospital and Clinics), Green Bay (Hemophilia Outreach Center), and La Crosse (Gundersen Clinic) Normal Hemostasis Stages of Hemostasis Three Distinct Phases: 1. Primary Hemostasis • Occurs after damage to the vessel wall • Involves vasoconstriction and adhesion of platelets on subendothelial vessel wall. • Further platelets aggregate to form a platelet plug 2. Secondary Hemostasis • Activation of the coagulation system, leading to the generation of fibrin strands, which are laid down between platelets and reinforce the platelet plug. • Clotting factor activation leading to fibrin formation 3. Fibrinolysis • Breakdown of clot Abnormal Hemostasis due to incomplete fibrin clot formation Measure of Hemostasis Clot Dissolution (Fibrinolysis) Clot Formation (Coagulation) PT aPTT Thrombin Time Fibrinogen Individual Clotting Factors FDP D-Dimer HMWK Prekallikrein 1 2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children “Simplified” Effects of Factor Deficiencies on aPTT and PT aPTT Prolonged, PT normal – Deficiency of intrinsic pathway – VIII, IX, XI, XII PT Prolonged, aPTT normal – Deficiency of extrinsic pathway factor - VII Both PT and aPTT prolonged – Deficiency of common pathway factors – Fibrinogen, II, V, X – Multiple factor deficiencies Inheritance of Hemophilia Hemophilia Hemophilia A – Factor VIII Deficiency – 1 in 5,000 live male births in US Hemophilia B – Factor IX Deficiency – 1 in 30,000 live male births in US Approximately 20,000 affected in the U.S. X-linked, recessive inheritance – Primarily affects males (very rarely females) 30% are spontaneous mutations If mother is a carrier of hemophilia… Daughter has 50% chance of becoming a carrier Son has 50% chance of having hemophilia If father has hemophilia … All daughters will be obligate carriers Sons will be unaffected National Hemophilia Foundation Steps for Living www.stepsforliving.hemophilia.org Internet encyclopedia of health and science Severity Severity of disease depends upon amount of circulating clotting factor (Normal = 50-150%) – Mild (5-50%) – Moderate (1-5%) – Severe (<1%) Amount of baseline circulating factor remains constant throughout life and is constant within families Treatment advances have dramatically improved life expectancy Life expectancy – 7.8 years in the 1930s – 74 years (if HIV-negative) from 1990 to 2001 15% of the total population of patients with hemophilia are 45+ years old Centers for Disease Control and Prevention. Summary Report of UDC Activity: National. 2 2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children Clotting Factor Infusion Almost all severe hemophiliacs, and many mild and moderate hemophiliacs, learn to infuse at home for convenience Parents of toddlers and boys as young as age 7 begin to learn home infusion Prefer morning infusions so factor is at “highest strength” during the day when most active Peripheral Vein vs. Infusaport – Infusaport often used to facilitate prophylaxis beginning in toddlers – Prefer not to leave accessed, especially while at school due to increased risk of serious infection – With any fever over 100.5 must rule out port infection with blood cultures Most Common Complication: Joint bleeding Pediatric patient with untreated bleed to the knee Special Considerations in Mild-Moderate Hemophilia Bleeding generally related to a procedure or significant injury Sometimes less familiar with signs of a bleed or how to treat – Reporting of injuries or procedures is often delayed Less likely to perform self infusion Frequently diagnosed later in life when they face bleeding challenges von Willebrand Disease (VWD) Deficiency of Von Willebrand Factor – Clotting protein that binds with Factor VIII – Prevents degradation of Factor VIII until it is needed during coagulation- known as “carrier protein” in plasma for Factor VIII. Most Common Bleeding Disorder – affects 1-2% of general population Affects Males and Females Equally – Most commonly autosomal dominant inheritance (only need to inherit one of the affected chromosomes to get the disease) – Rarely autosomal recessive inheritance People with hemophilia bleed LONGER NOT FASTER Types of von Willebrand Disease Type 1 = mild • Decreased amount of Von Willebrand Factor • VWF Activity 30-50% = very mild bleeding, <20%=moderately severe bleeding • Most common Type 2 = qualitative • VWF doesn’t work correctly • Subtypes 2A, 2B, 2M, 2N Type 3 = severe • Very low or No VWF • <5% of cases • Bleeding pattern very similar to hemophilia Acquired • Rare • Occurs late in life, r/t autoimmune complications 3 2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children Platelet Function Defects Desmopressin (DDAVP) Generally mucosal bleeding Treatments – Platelet transfusions – DDAVP, Antifibrinolytics – Estrogen for menorrhagia Platelet Storage Pool Disorders – Bleeding is typically mild, related to trauma and invasive procedure Bernard Soulier (very rare) – Large, abnormal platelets & low platelet count – Bleeding can be very severe Glanzmann’s Thrombasthenia – Decreased Platelet aggregation – Bleeding can be very severe (very rare) Synthetic Anti-diuretic Hormone – Common side effects include flushing & headache – Risk for water retention, hyponatremia – Limit fluid intake x24 hours after taking STIMATE – Intranasal Desmopressin – >50 kg =1 spray to each nostril <50 kg = 1 spray to 1 nostril – once q24 hrs for a max of 3 consecutive days – Not readily available through local pharmacies, usually need min 24 hrs notice IV DDAVP – 3 mcg/kg IV prior to a procedure or in response to a bleed Von Willebrand factor concentrate – Given intravenously. Contains factor VIII and von Willebrand factor. – If patient does not respond to Stimate or for certain type 2 and all of type 3 vWD. Bleeding with VWD Antifibrinolytics Prevent lysis of clots Aminocaproic Acid (Amicar) Tranexamic Acid (Lysteda) Prescription – Tablet, solution or IV Every 6-8 hours for minimum of 5 days after bleed Why does my nose bleed? The answer it not always simple. Reference: Berkowitz, C. (2008). Pediatrics: A Primary Care Approach. Los Angeles: Saunders Company. Images via google. Mucous membrane bleeding is most common, as vWF is essential for primary hemostasis – Nosebleeds – Mouth bleeds – Bruising – Prolonged oozing from superficial cuts – Bleeding after trauma or surgery – Prolonged/ heavy menstrual bleeding Joint and muscle bleeds are less common than in hemophilia except severe Type 3 and some Type 2 – Treat with RICE and von willebrand factor clotting factor concentrate as indicated How to treat mucosal bleeding Nosebleeds – Same as any other child with a nosebleed – Tilt head forward, pressure (full 10 minutes), ice – If bleeding has not stopped after 10 minutes, repeat the pressure. If persists, call your doctor or go to emergency room. Stimate may be used if school has permission. – Prevention: Cool mist humidifier in bedroom, Saline gel (AYR) – Urgent QR (OTC) powder – Afrin OTC (Oxymetazoline), soak cotton balls – Do not stuff tissues or things in the nose to stop the bleeding – May need evaluation for cauterization if frequent Mouth Bleeding – Soft, cool or lukewarm diet until area is fully healed – No straws, gum or smoking – Topical thrombin for frenulum or tongue laceration 4 2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children Soft Tissue/Superficial Bleed Soft Tissue – Easy bruising with or without hematomas – Generally do not require aggressive treatment other than rest and ice if they do not threaten function and mobility Superficial Cuts & Scrapes – Treatment is typical first aid Life & Limb Threatening Bleeds Intracranial Spinal Cord Oropharynx Gastrointestinal/Intra-abdominal Ocular Limb compartments/Iliopsoas Call 911, parent, HTC (follow school plan for emergency notification) Require IMMEDIATE treatment with factor concentrate Female Students Normal Periods Issues with menorrhagia Average age in US: 12 years – Too early: before 8 years – Too late: after 15 years Average cycle length: 21-35 days – Too often: under 21 days – Not often enough: greater than 35 days Average cycle duration: 7 days or less Hormones When is it too much? Menorrhagia – Greater than 80 ml/cycle (average 25-80 ml) – Greater than 7 days of menstruation 5 2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children How much is too much? Signs of menorrhagia Have a menstrual flow that soaks through one or more pads or tampons every hour for several hours in a row. (Hall passes!) Need to double up on pads to control your menstrual flow. Need to change pads or tampons during the night. Have menstrual periods lasting more than 7 days. Have a menstrual flow with blood clots the size of a quarter or larger. Have a heavy menstrual flow that keeps you from doing the things you would do normally. Have constant pain in the lower part of the stomach during your periods. Are tired, lack energy, or are short of breath Prevalence of Bleeding Disorders in Adolescents with Menorrhagia von Willebrand Disease Platelet Dysfunction Factor XI Deficiency Low Factor VIII Thrombocytopenia 5-36% 2-44% < 1-4% ~ 8% 13-20% Resources for Bleeding Disorders in Women http://www.fwgbd.org CDC – Screening Tool for Identifying Women with Menorrhagia for Testing for Underlying Bleeding Disorder Treatment for menorrhagia secondary to bleeding disorder Combined oral contraceptives used to treat Menorrhagia – usually monophasic – often require high doses or continuous cycling Other contraceptive methods known to reduce amount of menstrual – Mirena IUD, Implanon, Depo-Provera DDAVP (Stimate) – max of 3 consecutive days, consider treatment before bed to minimize side effects) Antifibrinolytic agents – Lysteda 1300 mg TID x5 days during menstruation Iron supplementation PRN Acute Illness, Injury and Invasive Procedure Conditions that wouldn’t normally cause a person to bleed may put a hemophiliac at risk for a bleed and require treatment – e.g. coughing and pharyngitis Invasive procedures including dental work other than a cleaning generally require pretreatment to prevent bleeding Increased metabolic states will increase factor requirements May have delayed wound healing with scaring 6 2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children Other Treatments RICE – Rest – Ice (15-20 minute intervals) – Compression (Pressure for 15 min) – Elevation Pain Management – Tylenol, Avoid NSAID’s & Aspirin – Celebrex & Opioids per MD discretion Typical first aid for cuts and scrapes and minor bruises Mild Hemophilia A - Stimate (Intranasal DDAVP) Exercise Students with a bleeding disorder are encouraged to be active and should participate in gym and activities Staying active improves joint strength and helps maintain normal weight Avoid high contact sports such as football, hockey, wrestling, boxing and power lifting Highly recommended activities are strength training, swimming, bicycling, jogging, golf, dancing, hiking, bowling and aerobic or cardiovascular training Sports & Activities A child with a bleeding disorder should : – Do warm up exercises before playing and cool down and stretching exercises after playing A child with a bleeding disorder should not: – Follow the “no pain, no gain” philosophy – Hide a bleed or injury – Exercise when in pain • The child should stop an exercise if it hurts a muscle or joint. – Exercise when healing from an injury • Injuries should have adequate time to heal. The HTC can help you to know when it’s safe to resume an activity Preventative Health Dental care – Twice yearly visits – Brush and Floss twice daily (continue flossing even with gum bleeding initially) Hepatitis A & B immunization Safety & injury prevention – Helmets, seat belts, etc. Physical activity & nutrition to maintain healthy weight – Being overweight will increase burden on joints Good source of iron in the diet and/or iron supplementation Medic Alert Emblem School Attendance Goal is for students to be at school with minimal absences related to their bleeding disorder For children aged 5-17 years, average annual school absenteeism due to hemophilia was 4.7 days Parents of affected children miss 3.2 days of work annually IEP Hemophilia Utilization Group Study (HUGS) 7 2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children School Awareness of Social/Emotional Needs Education from HTC available to overcome fear due to lack of knowledge Possible for student to have increased anxiety, frustration due to limitations with condition Avoid identification of disability- focus on what the student can do Key Points People with bleeding disorders bleed longer not faster Children with bleeding disorders should participate in all school activities except contact sports Female students are disproportionately affected by von Willebrand Disease and Platelet function defects Early treatment of bleeding episodes is critical Collaborate with Hemophilia Treatment Center Staff References Manco-Johnson, et. al. (2007). Prophylaxis vs Episodic Treatment to Prevent Joint Disease in Boys with Severe Hemophilia: New England Journal of Medicine National Hemophilia Foundation (2000), von Willebrand Disease Just the FAQs National Hemophilia Foundation. (2005) Playing It Safe: Bleeding Disorders, Sports and Exercise Ramot. (2007). Toxicol Pathol Drug Induced Thrombosis Ramot. Experimental , Clinical, and Mechanistic Conditions. Soucie JM, et al. Mortality among males with hemophilia: relations with source of medical care. Blood 2000;96:437-42 Secondary Education & Career Planning Most young people with a bleeding disorder will be able to pursue a normal education and career – In most states having Hemophilia alone will not qualify a person for disability Generally unable to pursue careers with physical performance testing – e.g. military, law enforcement, firefighting Physical, manual labor can present challenges for a person with a bleeding disorder Consider the potential benefits available – Health Insurance is a must, Good health insurance may take priority over salary – Best to be employed by a larger company (>100 employees) Many scholarships specific to students with bleeding disorders are available References Centers for Disease Control. Hemophilia. http://www.ced.gov/ncbddd/hemophilia/HTC.html Centers for Disease Control and Prevention. Summary Report of UDC Activity: National. Available at https://www2a.cdc.gov/ncbddd/htc/web/UDC_Report/ UDC_Report/asp April 1 2012 Dunn, A.L., Abshire, T.C. (2004) Recent advances in the management of the child who has hemophilia. Hematology Oncology Clinics of North America, (18) 1249-1276. Hemophilia in Pictures Presentation. World Federation of Hemophilia. www.wfh.org MASAC Document #205 MASAC Recommendations Concerning Products Licensed for the treatment of hemophilia and other bleeding disorders References Soucie JM, Symons J, Evatt B, Brettler D, Huszti H, Linden J and the Hemophilia Surveillance System Project Investigators. (2001). Home-based factor infusion therapy and hospitalization for bleeding complications among males with hemophila. Haemophilia 7:198-206. World Federation of Hemophilia. Hemophilia of Georgia. Protocols for the treatment of Hemophilia and Von Willebrand Disease 3rd edition World Federation of Hemophilia. (2009) What are Inhibitors? Wulff K, Zappa S, Womack, M and the Nursing Group of Hemophilia Region VI. (1999) Emergency Care for Patients with Hemophilia: An Instructional Manual for Medical Professionals. 8 2015 WASN Spring Conference 5C: Von Willebrand Disease and Other Bleeding Disorders in School Aged Children References White E, Menga Y, The Student with Hemophilia. www.hemophilia.org Accessed March 10 2012 Zappa S, Lacasse L, Jacobson R, Pucell S and Wulff K. Emergency Care for Patients with von Willebrand Disease: An Instructional Manual for Medical Professionals Please don’t hesitate to contact me with any questions jpindilli@uwhealth.org Resources National Hemophilia Foundation Steps for Living www.stepsforliving.hemophilia.org World Federation of Hemophilia “Hemophilia in Pictures” www.wfh.org 9