Association of Procalcitonin With Acute Pyelonephritis
and Renal Scars in Pediatric UTI
WHAT’S KNOWN ON THIS SUBJECT: Prompt, high-quality
diagnosis of acute pyelonephritis and later identification of
children with scarring are important to prevent future
complications. Examination by dimercaptosuccinic acid scan is
the current clinical gold standard but is not routinely performed.
WHAT THIS STUDY ADDS: Procalcitonin demonstrated a more
robust predictive ability, compared with C-reactive protein or
white blood cell count, to selectively identify both children who
had acute pyelonephritis during the early stage of urinary tract
infections, as well as those with late scarring.
abstract
BACKGROUND AND OBJECTIVE: Urinary tract infections (UTIs) are common childhood bacterial infections that may involve renal parenchymal
infection (acute pyelonephritis [APN]) followed by late scarring.
Prompt, high-quality diagnosis of APN and later identification of
children with scarring are important for preventing future complications.
Examination via dimercaptosuccinic acid scanning is the current clinical
gold standard but is not routinely performed. A more accessible assay
could therefore prove useful. Our goal was to study procalcitonin as
a predictor for both APN and scarring in children with UTI.
METHODS: A systematic review and meta-analysis of individual patient
data were performed; all data were gathered from children with UTIs who
had undergone both procalcitonin measurement and dimercaptosuccinic
acid scanning.
RESULTS: A total of 1011 patients (APN in 60.6%, late scarring in 25.7%)
were included from 18 studies. Procalcitonin as a continuous, class, and
binary variable was associated with APN and scarring (P , .001) and
demonstrated a significantly higher (P , .05) area under the receiver
operating characteristic curve than either C-reactive protein or white
blood cell count for both pathologies. Procalcitonin $0.5 ng/mL yielded
an adjusted odds ratio of 7.9 (95% confidence interval [CI]: 5.8–10.9)
with 71% sensitivity (95% CI: 67–74) and 72% specificity (95% CI: 67–76)
for APN. Procalcitonin $0.5 ng/mL was significantly associated with
late scarring (adjusted odds ratio: 3.4 [95% CI: 2.1–5.7]) with 79%
sensitivity (95% CI: 71–85) and 50% specificity (95% CI: 45–54).
AUTHORS: Sandrine Leroy, MD, PhD,a,b Anna FernandezLopez, MD,c Roya Nikfar, MD,d Carla Romanello, MD,e
François Bouissou, MD,f Alain Gervaix, MD,g Metin K.
Gurgoze, MD,h Silvia Bressan, MD,i Vladislav Smolkin, MD,j
David Tuerlinckx, MD,k Constantinos J. Stefanidis, MD,l
Georgos Vaos, MD,m Pierre Leblond, MD,n Firat Gungor,
MD,o Dominique Gendrel, MD,p and Martin Chalumeau, MD,
PhDp,q
aCentre for Statistics in Medicine, University of Oxford, Oxford,
United Kingdom; bEpidemiology of Emerging Disease Unit, Institut
Pasteur, Paris, France; cDepartment of Pediatrics, Joan de Deu
Hospital, Barcelona, Spain; dDepartment of Pediatrics, Abuzar
Children Medical Center Hospital, Ahvaz, Iran; eDepartment of
Pediatrics, University of Udine, Udine, Italy; fDepartment of
Pediatrics, Children’s Hospital, Paul Sabathier University, CHU
Purpan, Toulouse, France; gDepartment of Pediatrics, University
Hospital of Geneva, Geneva, Switzerland; hFirat University
Medicine Faculty, Department of Pediatrics, Division of Pediatric
Nephrology, Elazı
g , Turkey; iDepartment of Pediatrics, University
of Padova, Padova, Italy; jDepartment of Pediatrics, Medical
Center, Afula, Israel; kDepartment of Pediatrics, Cliniques
Universitaires de Mont-Godinne, Université Catholique de Louvain,
Yvoir, Belgium; lDepartment of Pediatrics, ‘‘P. and A. Kyriakou’’
Children’s Hospital, Athens, Greece; mDepartment of Pediatric
Surgery, Alexandroupolis University Hospital, Democritus
University of Thrace School of Medicine, Thrace, Greece;
nDepartment of Pediatrics, Jeanne de Flandre Hospital, Lille,
France; oAkdeniz University, School of Medicine, Department of
Nuclear Medicine, Antalya, Turkey; pDepartment of Pediatrics of
Necker Hospital, Paris-Descartes University, Paris, France; and
qInserm U953 Unit, Paris, France
KEY WORDS
acute pyelonephritis, children, procalcitonin, renal scarring,
urinary tract infection
ABBREVIATIONS
APN—acute pyelonephritis
AUC—area under the curve
CI—confidence interval
CRP—C-reactive protein
DCA—decision curve analysis
DMSA—dimercaptosuccinic acid
LR—likelihood ratio
OR—odds ratio
PCT—procalcitonin
ROC—receiver operating characteristic
UTI—urinary tract infection
VUR—vesicoureteral reflux
WBC—white blood cell
CONCLUSIONS: Procalcitonin was a more robust predictor compared
with C-reactive protein or white blood cell count for selectively
identifying children who had APN during the early stages of UTI, as
well as those with late scarring. Pediatrics 2013;131:870–879
870
LEROY et al
Downloaded from by guest on March 5, 2016
(Continued on last page)
ARTICLE
Urinary tract infections (UTIs) are the
most common invasive bacterial infections among young febrile children.1 UTIs can occur as simple
bladder infections (lower UTI; bacteriuria only) but can also involve the
kidneys (acute pyelonephritis [APN],
in which bacteriuria is associated
with infectious renal parenchymal involvement), leading to renal scarring.2
The belief that persisting APN effects
followed by late renal scarring, sometimes with recurrences, may lead to
future complications such as hypertension and/or end-stage renal failure has
been the major driving force behind the
aggressive investigation and treatment
of first-occurrence UTIs.3 The prompt
and high-quality diagnosis of APN and
differentiation from lower UTI is therefore of key importance. A dimercaptosuccinic acid (DMSA) scan is considered
the gold standard in imaging for both
renal parenchymal involvement during
acute infection and for late renal damage left by the infection.4 However, DMSA
scans are not performed in most
children with UTI due to the limited
availability of nuclear medicine departments compared with the high
number of children with UTIs. Thus,
a more practical and accessible tool
that could assist clinicians in determining the presence of renal parenchymal involvement and/or late
renal damage would be of great clinical value.
Procalcitonin (PCT), a 116–amino acid
propeptide of calcitonin without hormonal activity, is an early, sensitive,
and specific marker of bacterial infection.5,6 PCT is almost undetectable
under physiologic conditions or during viral infections but rises in response to bacterial endotoxins; the
extent of this increase seems to be
proportional to the severity of the infection.6 However, its exact role, if any,
in the inflammatory response and in
the cytokine cascade remains unknown.6
In febrile UTI, the predictive ability of high
PCT concentrations for both APN and late
renal scarring has been previously investigated by several teams. A review7
and a recent systematic review and
meta-analysis8 showed that a serum
PCT .0.5 ng/mL predicts early renal
parenchymal involvement reasonably
well (diagnostic odds ratio [OR]: 14.3
[95% confidence interval (CI): 4.7–
43.2]); however, heterogeneity made
these results inconclusive.8 Moreover,
results concerning late renal scarring
were controversial, with no pooled
measurements provided.7 Most of this
heterogeneity and these discrepancies
may be due to threshold effects because the initial studies chose different
PCT cutoff values due to population
variation; unfortunately, any effects
from the latter could not be fully explored with only pooled data from the
studies. Under these circumstances,
the only way to analyze PCT as a continuous biomarker without a priori
threshold choice, simultaneously control for potential individual-level confounders, and then provide robust
conclusions concerning PCT as a predictor of APN and/or scarring would be
to obtain individual data unaltered by
thresholds.9
We thus aimed to perform an updated
systematic review and meta-analysis on
individual patient data to investigate
PCT as a predictor for both APN and
renal scarring in children with a febrile
UTI. The most appropriate threshold
values of PCT were simultaneously
studied.
METHODS
We performed a systematic review and
meta-analysis on individual patient
data, in accordance with international
standards (Centre for Reviews and
Dissemination guidelines,10 PRISMA,11
and STARD12). We electronically and
manually searched for all cohort
studies of children with UTI, a PCT
PEDIATRICS Volume 131, Number 5, May 2013
measurement, and a renal DMSA scintigraphy published between January
1993 and September 2011. The search
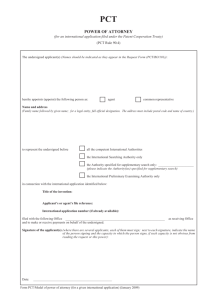
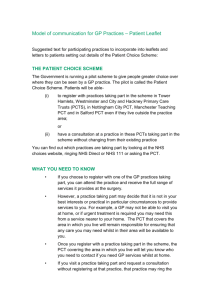
methods are detailed in Fig 1. Ethics
committees from each participating
center approved the protocol for each
initial study from which data were
collected.
All cohort studies of consecutively included children with a febrile UTI, a PCT
measurement, and an early (ie, within
14 days) and a late (ie, repeated at least
FIGURE 1
Flow chart of the systematic review. The electronic search was conducted in Medline for all
studies of UTI with a PCT measurement in children published from January 1993 (when PCT
was first described in relation to bacterial infection5) through November 2009, and updated
in September 2011. The search strategy used
medical subject heading terms and text words,
including “procalcitonin” and “children.” The
electronic search was enhanced by handsearching reference lists of all included articles,
obtaining any identified articles, and also supplemented by a manual review of abstracts from
the European Society of Pediatric Infectious
Diseases, the European Society for Pediatric
Nephrology, the International Pediatric Nephrology Association, the American Academy of
Pediatrics, and the American Society of Nephrology and by discussion with experts in the
field. The electronic search was then validated,
comparing the obtained list with the reference
list of previous reviews on PCT and UTI7,8 to
identify any potential systematic default. No
language restriction was used. The search
ended with 290 potentially eligible abstracts,
among which 19 were considered for inclusion.
One article was not included because of absence
of DMSA scan data. Finally, 18 articles were included, representing 13 centers as follows: Afula
(Israel),28 Ahvaz (Iran),33 Antalya (Turkey),22
Athens (Greece),27 Barcelona (Spain),19,20 Elazig
(Turkey),26 Geneva (Switzerland),17,21,31 Lille
(France),25 Padova (Italy),32 Thrace (Greece),29,30
Toulouse (France),16 Udine (Italy),23 and Yvoir
(Belgium).24
871
Downloaded from by guest on March 5, 2016
872
LEROY et al
Downloaded from by guest on March 5, 2016
62 (62)
21 (50)
52 (72)
68 (75)
,.001
613 (61)
64
33
61
174
76
80
57
100
61
100
42
72
91
1011
—
—
12 mo
6–24 moc
SB (105), CVM (105)
SB (105)
SB (105)
SB (105), CVM (105)
23 (36)
21 (64)
25 (41)
92 (53)
34 (45)
77 (96)
27 (47)
63 (63)
48 (79)
APN, n (%)
—
3–6 mo
6 mo
—
6 mo
3 mo
6 mo
6 mo
6 mo
Timing of Late
DMSA Scan
SA (any), UC (103)
UC (104), CVM (105)
SA (103), UC (104), CVM (105)
SA (any), UC (5.104), CVM (105)
UC (103), CVM (105)
SA (103), UC (103), CVM (105)
SA (any), UC (104), CVM (105)
UC (105), CVM (105)
SA (103), UC (5.104), CVM (105)
Urine Collection Techniques
(Threshold of the
Positive Bacteriuria)b
525
0
0
61
59
0
23
59
0
76
59
57
79
52
No. Included
(for LRS)
135 (26)
—
—
14 (23)
13 (22)
,.001
—
4 (17)
10 (17)
—
12 (16)
34 (58)
12 (21)
18 (23)
18 (35)
LRS, n (%)
332 (33)
19 (19)
12 (29)
31 (43)
19 (21)
.008
22 (35)
2 (6)
27 (44)
83 (48)
28 (37)
32 (40)
13 (23)
31 (31)
13 (21)
Male, n (%)
10.0 (4.0–30.0)
8.0 (17.5–57.0)
13.5 (6.0–48.0)
4.5 (1.1–9.8)
20.0 (8.8–64.9)
.001
14.0 (4.5–23.5)
48.0 (24.0–72.0)
0.6 (0.2–2.0)
4.8 (2.0–9.0)
30.0 (10.5–72)
8.9 (2.4–21.5)
16.0 (7.0–40.0)
8.0 (4.0–17.5)
37.2 (12.5–78.4)
Age (mo),
Median (IQR)
182 (23)
—
14 (58)
13 (18)
32 (36)
,.001
17 (27)
2 (33)
9 (15)
27 (23)
3 (4)
21 (28)
15 (29)
16 (18)
13 (22)
All-Grade
VUR, n (%)
80 (10)
—
3 (13)
3 (4)
12 (14)
,.001
9 (14)
2 (33)
7 (12)
9 (5)
0 (0)
9 (12)
11 (22)
9 (10)
6 (10)
Grade $3
VUR, n (%)
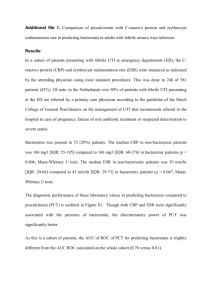
References for the articles corresponding to each center are presented in the Supplemental Appendix. CVM, clean-voided midstream; IQR, interquartile range; LRS, late renal scars; SA, suprapubic aspiration; SB, sterile bag; UC, urethral catheterization.
a Classified according to the urine collection technique in non–toilet-trained children.
b In colony-forming units per milliliter.
c Median of 9 months.
Centers using
SA or UC
Afula28
Antalya22
Athens27
Barcelona19,20
Elazig26
Geneva17,21,31
Thrace29,30
Udine23
Yvoir24
Centers using SB
Ahvaz33
Lille25
Padova18,32
Toulouse16
Between-center
variability (P)
Total
Centera
No. Included
(for APN)
We analyzed the relationships between
APN/renal damage and PCT, CRP, and
WBC count, respectively, using different,
backward, stepwise multilevel logisticregression models for each biomarker
(center was a group-level variable),
with fractional polynomial transformation for continuous variables if the
model assumption of linearity was violated. The discriminative ability of
each biomarker for APN and then late
renal damage was evaluated by drawing receiver operating characteristic
(ROC) curves, as well as by calculating
sensitivity, specificity, predictive values,
and likelihood ratios (LR) after dichotomization. In addition, we compared
biomarker models by using decision
curve analysis (DCA), a method for
evaluating the clinical net benefit of
prediction models in which the benefits
(true-positives) are added and the harms
(false-positives) are subtracted.15
Due to collinearity, no attempt was
made to combine biomarkers. Statistical methods are detailed in the
Appendix.
TABLE 1 Population Characteristics According to Each Center
3 months later if available) renal DMSA
scintigraphy were included. Febrile UTI
was defined as fever ($38°C) with
a positive result on bacterial urine
culture (thresholds for collection
techniques are given in Table 1). We
asked the authors to send us their
study data files (duplicates were discarded if any), from which we extracted clinical (gender, age), laboratory
(C-reactive protein [CRP], PCT, white
blood cell [WBC] count), and radiologic (DMSA scan results, vesicoureteral reflux [VUR] grade13 on
cystography) data. Information concerning the standard operating procedures used for urine collection, PCT
measurement, DMSA scanning (and
timing), and cystography at each
center was also collected. Methodologic study quality was assessed via
a checklist (Supplemental Appendix
Tables 1 and 2).14
ARTICLE
RESULTS
Study Characteristics
Following the aforementioned criteria,
we retrieved 227 abstracts by electronic
searching; 19 were potentially suitable
(Fig 1). After full text review, 1 study
was not included because of absence
of DMSA scan data, leaving 18 articles
to be included.16–33 The 13 corresponding study authors were contacted; all agreed to participate and
send data. A total of 1011 (97.9%)
patients fully met the inclusion criteria.
All studies had a high methodologic
quality (Supplemental Appendix Tables
1 and 2). Nine (69.2%) centers performed both early and late DMSA
scans. All centers performed the early
DMSA scan within 7 days; 5 of 9 centers
performed the late scan at 6 months,
and the other centers varied between 3
and 24 months (Table 1). Among the 9
centers performing late DMSA scans,
late scanning was systematically
conducted regardless of early-scan
results in only 1 (11.1%) center (Elazig,
Turkey). Nine (69.2%) centers collected urine samples following highquality standard operating procedures (suprapubic aspiration, urethral
catheterization for non–toilet-trained
children, and clean-voided midstream
for the other patients). All centers
measured PCT by using the LUMItest
PCT immunoluminometric assay or
the BRAHMS PCT-Q semiquantitative
rapid test (BRAHMS, Hennigsdorf,
Germany). All centers included hospitalized children with UTI. No adverse events had been reported
in performing PCT measurement,
DMSA scanning, or cystography.
Table 1 provides details on the
characteristics of each center’s
population.
Analysis of APN and late renal scars
involved 1011 and 525 patients, respectively. APN by grade was analyzed in
357 patients. PCT as a continuous variable involved only 883 (87.3%) patients,
as PCT was measured by the PCT-Q
semiquantitative test for 128 patients.
Analysis of CRP and WBC count involved
959 (94.9%) and 962 (95.2%) patients,
respectively. VUR was examined in 772
(76.4%) patients.
74) (Table 3). PCT remained strongly
associated with APN when assessed
by clinical grade, as did CRP and WBC
count (Supplemental Appendix Table 3).
Predicting Late Renal Scars
Predicting APN
APN was demonstrated in 613 children
(60.6%) of the 1011 patients included.
The mean 6 SD age of the children was
25.2 6 32.8 months (median: 10.5;
interquartile range: 4.3–32.3); 332
(32.8%) were boys. VUR was diagnosed in 182 (23.6%), and VUR $3
was found in 80 children (10.4%). PCT
as a continuous, class, or binary variable was significantly associated with
APN (Table 2, Fig 2). The strength of the
association increased when the PCT
category (when ordinal variable) increased (Table 2). PCT $0.5 ng/mL
(current threshold used in the literature) yielded an adjusted OR of 7.9
(95% CI: 5.8–10.9). CRP and WBC count
were also significantly related to APN,
with similar OR values for CRP as
previously described; however, lower
OR values were obtained for WBC
count (Table 2). PCT as a continuous
variable offered an area under the
ROC curve (AUC ROC) of 0.82 (95% CI:
0.79–0.84), after adjusting according
to the chosen model. The AUC ROCs for
CRP and WBC count were significantly
lower (P , .0001): 0.72 (95% CI: 0.69–
0.76) and 0.62 (95% CI: 0.57–0.65), respectively, once adjusted by using the
model (Fig 3). The DCA demonstrated
that PCT provided a more statistically
robust test than CRP, WBC count, or extreme systematic strategies (ie, DMSA
for all or no patients) for all threshold
probabilities. A PCT threshold $0.3 ng/
mL (median of nondiseased patient
distribution) demonstrated 88% sensitivity (95% CI: 85–90), with 47%
specificity (95% CI: 42–52) (Table 2);
interestingly, PCT $0.5 ng/mL offered
a higher specificity of 72% (95% CI: 67–
76) with a 71% sensitivity (95% CI: 67–
PEDIATRICS Volume 131, Number 5, May 2013
Late scars were demonstrated in 135
(25.7%) of the 525 children included.
The mean 6 SD patient age was 26.6 6
33.8 months (median: 11.0; interquartile range: 4–36); 162 (31%) were
male. VUR was present in 107 (22.0%)
of the 486 patients who underwent
cystography; VUR $3 was diagnosed in
51 (10.5%) children. PCT as a continuous and binary variable was significantly associated with renal scars
(Table 2, Fig 2). PCT $0.5 ng/mL yielded
an adjusted OR of 3.4 (95% CI: 2.1–5.7).
CRP and WBC count were also significantly related to renal scarring (Table 2, Fig 2). PCT as a continuous
variable resulted in an AUC ROC of 0.75
(95% CI: 0.70–0.80) once adjusted
according to the model built and was
significantly higher (P = .02) than those
values observed for CRP and WBC count
(0.70 [95% CI: 0.65–0.76] and 0.66 [95%
CI: 0.60–0.72], respectively) (Fig 3).
According to DCA, PCT was better than
CRP, WBC count, and both extreme
systematic strategies (ie, DMSA for
everyone or no one) (Fig 3). PCT $0.5
ng/mL had a 79% of sensitivity (95% CI:
71–85), with a 50% specificity (95% CI:
45–54) (Table 3).
DISCUSSION
We demonstrated that the measurement of serum PCT can provide considerable predictive value for the
development of APN and renal scars,
and that this predictive capacity is
better than that provided by either CRP
or WBC count regardless of considered
thresholds. Because the related medical decision process is binary (to perform or not to perform a DMSA scan),
our goal was to provide an alternative
873
Downloaded from by guest on March 5, 2016
TABLE 2 Relationship Between APN or Late Renal Scars and PCT, CRP, and WBC Count
Variables
APN
PCT (ng/mL)a
PCT as a continuous variable
PCT as a class variable
,0.13
0.13–0.3
0.3–0.6
.0.6
PCT as a class variable
,0.5
0.5–2
2–10
.10
PCT as a binary variable ($0.3)
PCT as a binary variable ($0.5)
CRP (mg/L)b
CRP as a continuous variable
CRP as a class VARIABLE
,10
10–20
20–60
.60
CRP as a binary variable ($20)
CRP as a binary variable ($30)
WBC count (cell/mm3)c
WBC count as a continuous variable
WBC count as a class variable
,10 000
10 000–15 000
15 000–20 000
.20 000
WBC count, binary variable ($15 000)
Late renal scars
PCT (ng/mL)d
PCT as a continuous variable
PCT as a binary variable ($0.5)
CRP (mg/L)e
CRP as a continuous variable
CRP as a binary variable ($20)
CRP as a binary variable ($30)
WBC count (cell/mm3)f
WBC count as a continuous variable
WBC count, binary variable ($15 000)
Crude OR (95% CI)
P
Adjusted OR (95% CI)
P
2.6 (2.2–3.1)
,.0001
2.7 (2.3–3.1)
,.0001
1
2.5 (1.3–4.9)
3.1 (1.6–5.8)
16.9 (9.3–30.6)
.006
.001
,.0001
1
2.3 (1.2–4.6)
3.0 (1.6–5.6)
17.0 (9.3–30.9)
.01
.001
,.0001
1
3.5 (2.5–5.0)
25.3 (14.8–43.2)
132.5 (17.9–979)
5.5 (3.8–7.8)
7.5 (5.5–10.3)
,.0001
,.0001
,.0001
,.0001
,.0001
1
3.7 (2.6–5.3)
26.3 (15.3–45.0)
146.3 (19.7–1085)
5.8 (4.0–8.3)
7.9 (5.8–10.9)
,.0001
,.0001
,.0001
,.0001
,.0001
2.7 (2.3–3.3)
,.0001
2.7 (2.3–3.3)
,.0001
1
2.7 (1.4–5.5)
8.0 (4.2–15.2)
26.0 (13.6–49.7)
8.6 (5.5–13.3)
6.3 (4.4–9.0)
.005
,.0001
,.0001
,.0001
,.0001
1
2.9 (1.4–5.9)
8.2 (4.3–15.5)
26.5 (13.8–50.8)
8.6 (5.5–13.3)
6.3 (4.4–9.1)
.003
,.0001
,.0001
,.0001
,.0001
1.0 (1.0–1.0)
,.0001
1.0 (1.0–1.0)
,.0001
1
1.8 (1.2–3.1)
3.1 (1.9–5.1)
4.9 (2.9–8.3)
2.4 (1.8–3.3)
.01
,.0001
,.0001
,.0001
1
1.8 (1.1–3.0)
3.0 (1.8–5.0)
4.9 (2.9–8.3)
2.4 (1.8–3.3)
.01
,.0001
,.0001
,.0001
1.8 (1.6–2.1)
3.8 (2.3–6.1)
,.0001
,.0001
1.7 (1.5–2.0)
3.4 (2.1–5.7)
,.0001
,.0001
2.3 (1.8–2.9)
4.8 (2.5–9.4)
4.6 (2.5–8.4)
,.0001
,.0001
,.0001
2.2 (1.7–2.9)
4.6 (2.3–9.4)
4.2 (2.3–7.9)
,.0001
,.0001
,.0001
1.0 (1.0–1.0)
2.1 (1.4–3.3)
,.0001
,.0001
1.0 (1.0–1.0)
2.1 (1.3–3.3)
,.0001
,.0001
A model was separately derived for each biomarker (PCT, CRP, or WBC count). Univariate and multivariate analysis used
a multilevel regression model. The final multivariate model was built by using a backward stepwise reduction procedure.
Each multivariate model for each biomarker was significantly better than the reduced model based on the maximum
likelihood test (P , .05).
a The analysis included 883 patients for PCTas a continuous or class variable, 937 patients for PCT dichotomized according to
the 0.3 ng/mL threshold, and 1011 patients for PCT dichotomized according to the 0.5 ng/mL threshold (because some
patients had a PCT-Q test [see text]). The final multivariate model was based on PCT and age (as a continuous variable, after
linear transformation); continuous PCT was transformed as follows to assess the model linearity assumption: ln(PCT/100) +
3.33732173.
b The analysis included 959 patients. The final multivariate model was based on CRP and age (as a continuous variable, after
linear transformation); CRP was transformed as follows to assess the model linearity assumption: ln(CRP/100) +
0.3965495066.
c The analysis included 962 patients. The final multivariate model was based on WBC count and gender.
d The analysis included 479 patients. The final multivariate model was based on PCTand high-grade VUR; PCTwas transformed
as follows to assess the model linearity assumption: ln(PCT/100) + 3.293186643.
e The analysis included 478 patients. The final multivariate model was based on CRP and high-grade VUR; CRP was transformed in the same purpose as above into: ln(CRP/100) + 0.439036841.
f The analysis included 478 patients. The final multivariate model was based on WBC count and high-grade VUR.
874
LEROY et al
Downloaded from by guest on March 5, 2016
assay that could contribute to diagnosis and investigate the optimal
threshold by which these clinical decisions could be made. PCT $0.5 ng/mL
seemed to offer the optimal compromise of sensitivity and specificity for
both APN and late renal scars: 71%
sensitivity (95% CI: 67–74) with a 72%
specificity (95% CI: 67–76) for APN;
79% sensitivity (95% CI: 71–85) with
a 50% of specificity (95% CI: 45–54)
for late scarring. Furthermore, DCA
showed that PCT offered the best
benefit/harm balance irrespective of
the chosen threshold, compared with
CRP, WBC count, or systematic strategies (DMSA for everyone or no one)
for the selective identification of
children who might benefit from
a DMSA scan.
Our findings add evidence to those of
Mantadakis et al.8 Together, they suggest a reasonably strong predictive
value based on PCT levels; however,
data from studies using pooled estimates lead to a more cautious interpretation due to the significant
heterogeneity found within these
study pools. We avoided these issues
by working with individual data,
adjusting for intercenter variability
modeling with multilevel regressions,
as well as accounting for all covariables of interest at the individual level.
Moreover, the study design (a metaanalysis of individual patient data)
allowed us to study the impact of different threshold levels, to perform
DCA, and to draw conclusions without
the usual threshold effect that often
affects diagnostic accuracy assessed
by meta-analysis, thus confounding
results. Our approach was complementary to that of Zaffanello et al,7
who performed a nonsystematic review of the potential of PCT to predict
late renal scarring, without computing pooled estimates, as they were
confronted with different studies and
cutoffs. With our systematic meta-analysis,
ARTICLE
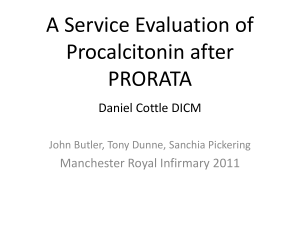
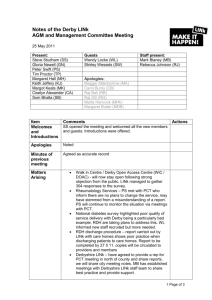
FIGURE 2
Distribution of PCT, CRP, and WBC count values according to the presence of APN or late renal scars. (A–C) Plots of PCT, CRP, and WBC count for APN. (D–F)
Plots of PCT, CRP, and WBC count for late renal scars. In each graphic, the horizontal line is the proposed threshold for dichotomizing classification via the
biomarker.
we offer further evidence to support
their results, updating the review in
a systematic manner and providing
pooled estimates of the predictive
ability of PCT, leading to a robust conclusion.
The use of imaging in this field has been
largely debated in the last decade.
However, the decision as to which tests,
if any, should be routinely conducted in
children with UTIs necessarily depends
on many factors. The “top-down” approach uses early DMSA scanning as
a screening test.34 Although children
with a negative acute-phase DMSA scan
are unlikely to develop scarring, DMSA
scans are expensive, invasive, and expose children to radiation. However,
the top-down strategy raises 2 concerns:
first, it requires DMSA scan availability
across countries and settings, which is
not currently the case, and second, the
identification of late renal scarring
results in only a more careful follow-up
of affected children. Therefore, PCT may
occupy an intermediate position useful
for identifying children at high risk for
APN and renal scarring, and for whom
a DMSA scan can be selectively proposed to confirm parenchymal involvement. The reported sensitivity and
specificity values may not appear very
convincing (∼70%). However, PCT is not
meant to replace DMSA scanning, which
remains the gold standard for assessing parenchymal involvement (APN or
scarring). PCT could be used as an intermediate strategy, based on a single
biomarker, easier to set up than a nuclear imaging process, which can help
discriminate between lower UTI and
APN, even in settings in which DMSA
scans are not available. Interestingly,
PCT offered the best benefit/harm
balance irrespective of the chosen
threshold, compared with systematic
PEDIATRICS Volume 131, Number 5, May 2013
strategies (DMSA for everyone or no
one) for the selective identification of
children who might benefit from
a DMSA scan. Later in the imaging
evaluation, a cystography could be
proposed for children with a proven
APN, to diagnose or rule out VUR, and
treat it if necessary. Moreover, PCT
may also be helpful when choosing
between oral or intravenous antibiotic treatments during the early infectious phase, depending on the
severity of the UTI (lower UTI or APN).
PCT could find a place in the debated
process of UTI imaging and treatment,
as a key point test in the decisional
flowchart.
There are several potential limitations
to our study that should be addressed.
First, despite the extensive electronic
and hand searches performed, a publication bias is possible, especially because test accuracy studies are more
875
Downloaded from by guest on March 5, 2016
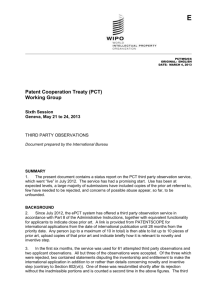
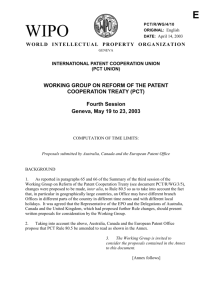
FIGURE 3
ROC curve and DCA for PCT, CRP, and WBC count. (A) ROC curves of PCT, CRP, and WBC count for APN. (B) ROC curves of PCT, CRP, and WBC count for late renal
scars. (C) The DCA of PCT, CRP, and WBC count for APN. One line represents 1 biomarker (PCT, CRP, and WBC count); the line “all” represents the benefit/harm
curve if everyone is investigated with a DMSA scan, whereas the line “none” represents the corresponding curve if no one undergoes examination.
(D) The DCA of PCT, CRP, and WBC count for late renal scars. One line represents 1 biomarker (PCT, CRP, and WBC count); the line “all” represents the
benefit/harm curve if everyone is investigated with a DMSA scan, whereas the line “none” represents the corresponding curve if no one undergoes
examination.
easily conducted and abandoned than
randomized controlled trials, and are
then particularly susceptible to publication bias.35 However, our current
knowledge about the precise effects of
publication bias on meta-analytic esti-
mates, as well as how to assess the
extents of these possible limitations,
are limited.36 Therefore, due to the
complexity of accurately assessing
this issue, we can provide no estimates of the effect of a probable
publication bias. Secondly, a participation bias related to the response
and voluntary participation of the
centers also might be possible but
seems unlikely because all authors
contacted responded positively to our
TABLE 3 Diagnostic Accuracy of PCT, CRP, and WBC Count for APN and Late Renal Scars
Variable
For APN
PCT $0.3 ng/mL
PCT $0.5 ng/mL
PCT $1 ng/mL
CRP $20 mg/L
CRP $30 mg/L
WBC count $15 000/mm3
For late renal scars
PCT $0.3 ng/mL
PCT $0.5 ng/mL
PCT $1.0 ng/mL
CRP $20 mg/L
CRP $30 mg/L
WBC count $15 000/mm3
Sensitivity
Specificity
Positive Predictive Value
88 (85–90)
71 (67–74)
65 (61–69)
87 (84–89)
74 (70–77)
63 (59–67)
47 (42–52)
72 (67–76)
87 (83–90)
41 (37–47)
54 (49–59)
55 (50–60)
74 (71–77)
79 (76–83)
90 (86–92)
70 (67–74)
72 (69–76)
71 (67–74)
91 (85–95)
88 (83–91)
74 (66–81)
85 (78–90)
78 (71–85)
68 (60–75)
30 (26–35)
50 (45–54)
67 (62–71)
36 (32–41)
47 (41–52)
51 (46–56)
31 (27–36)
51 (46–56)
43 (37–50)
32(27–37)
34 (29–39)
33 (27–38)
Negative Predictive Value
Positive LR
Negative LR
69 (63–74)
61 (57–66)
60 (55–64)
66 (59–71)
56 (51–61)
46 (42–51)
1.6 (1.5–1.8)
2.5 (2.1–3.0)
4.9 (3.7–6.5)
1.5 (1.3–1.6)
1.6 (1.4–1.8)
1.4 (1.2–1.6)
0.3 (0.2–0.3)
0.4 (0.4–0.5)
0.4 (0.4–0.5)
0.3 (0.3–0.4)
0.5 (0.4–0.6)
0.7 (0.6–0.8)
91 (84–95)
87 (82–91)
88 (84–92)
87 (81–92)
86 (81–90)
82 (77–86)
1.3 (1.2–1.4)
1.6 (1.4–1.8)
2.3 (1.9–2.6)
1.3 (1.2–1.5)
1.5 (1.3–1.7)
1.4 (1.2–1.6)
0.3(0.2–0.5)
0.4 (0.3–0.6)
0.4 (0.3–0.5)
0.4 (0.3–0.6)
0.5 (0.3–0.7)
0.6 (0.5–0.8)
Data are presented as % (95% CI).
876
LEROY et al
Downloaded from by guest on March 5, 2016
ARTICLE
requests for patient data sets. Thirdly,
the possibility of a classification bias
seems unlikely because PCT was
measured by using validated techniques (immunoluminometric assay or
semiquantitative PCT-Q assay), while
blinded to the outcome. Fourthly, we
assumed that patients who had a normal DMSA had no late lesions even if
late DMSA was not performed. However, this assumption is commonplace
in the literature,37 and we verified this
assumption in the only center (Elazig,
Turkey) in which all patients systematically underwent both late and early
DMSA: none of the negative early DMSA
cases were followed by a positive late
DMSA. This outcome gives an indication on the robustness of our
assumption. Fifth, we addressed heterogeneity issues due to data pooling
from different centers (including different time frames for the late DMSA
scan) by analyzing them as hierarchical data and using multilevel modeling. We chose to analyze the data set
as a meta-analysis of individual patient data because this method provides the least biased and most
reliable means of addressing the
questions at hand.9 Sixth, technical
concerns, such as the collection of
urine from non–toilet-trained children
in sterile bags at 4 of the selected
centers (not a recommended method)
could have led to selection bias.38,39
This procedure could have increased
the number of false-positive results
for UTI but without consequences to
the relationship between APN or late
scarring and PCT or other biomarkers.
In addition, the inclusion of only hospitalized children by the centers might
have led to another selection bias, due
to the inclusion of only the sickest
children. However, all children with
febrile UTI were systematically hospitalized in the included centers. Seventh, the absence of previous negative
DMSA scintigraphy results might also
have introduced a selection bias. Even
if all the centers confirmed having
included exclusively or mostly children with a first febrile UTI, it could
not guarantee that previous UTI with
persistent scarring had not occurred
in the included patients, as correct
diagnosis depends on the clinical
evaluation performed during previous febrile episodes. Moreover, not
all UTIs in children are accompanied
by fever, which is the main clinical
reason for obtaining urine cultures in
infants; therefore, previous UTIs
unaccompanied by fever may not have
been clearly identified. Lastly, the
delay between the first indications
of infection and PCT level measures
was not taken into account, and this
might have introduced a bias in the
results but only by underestimating
the relationship between APN or late
scarring and PCT, because this
marker increases as early as 6 hours
postinfection and also decreases just
as quickly at the end of infection.
stages of UTI and those that developed
later renal scarring. The use of serum
PCT measurements has the potential
to aid the clinical decision-making
process regarding the appropriate
acute management of children with
UTI. In particular, due to limited resources and technical availability, it
may be helpful to use such an assay to
selectively identify children who may
benefit from a DMSA scan at the early
and late stages of infection. The impact
of PCT measurements on the currently
debated practice of UTI examinations
needs to be evaluated by a welldesigned impact study and may lead
to possible refinement of the decisional process.
We demonstrated that PCT has a robust
predictive ability to selectively identify
children who had APN in the early
ACKNOWLEDGMENTS
The authors thank Dr Gardikis and
Dr Deftereos (Department of Pediatric
Surgery and Radiology, Alexandroupolous
University Hospital, Democritus University of Thrace School of Medicine,
Thrace, Greece), Dr Galetto-Lacour (Department of Pediatrics, University Hospital of Geneva, Geneva, Switzerland),
Dr Ellero (Department of Pediatrics,
University of Udine, Udine, Italy), Professor Da Dalt (Department of Pediatrics,
University of Padova, Italy) for participation in data collection/sharing,
Dr Bacchetta (Department of Pediatric
Nephrology–Reference Centre for Rare
Renal Diseases, Femme Mère Enfant
Hospital, University of Lyon, Lyon, France)
for helpful discussions, and Melissa
Laird (Inserm U818, Institut Pasteur,
Paris, France) for pertinent comments
and corrections.
normal scans with dimercaptosuccinic acid:
follow up study. BMJ. 1997;315(7113):905–908
3. Williams G, Fletcher JT, Alexander SI, Craig
JC. Vesicoureteral reflux. J Am Soc Nephrol. 2008;19(5):847–862
4. Rushton HG, Majd M. Dimercaptosuccinic
acid renal scintigraphy for the evaluation
of pyelonephritis and scarring: a review
of experimental and clinical studies.
J Urol. 1992;148(5 pt 2):1726–1732
5. Assicot M, Gendrel D, Carsin H, Raymond J,
Guilbaud J, Bohuon C. High serum procalcitonin concentrations in patients with sepsis
and infection. Lancet. 1993;341(8844):515–518
CONCLUSIONS
REFERENCES
1. Mårild S, Jodal U. Incidence rate of first-time
symptomatic urinary tract infection in children under 6 years of age. Acta Paediatr.
1998;87(5):549–552
2. Vernon SJ, Coulthard MG, Lambert HJ, Keir
MJ, Matthews JN. New renal scarring in
children who at age 3 and 4 years had had
PEDIATRICS Volume 131, Number 5, May 2013
877
Downloaded from by guest on March 5, 2016
6. Simon L, Gauvin F, Amre DK, Saint-Louis P,
Lacroix J. Serum procalcitonin and
C-reactive protein levels as markers of
bacterial infection: a systematic review and
meta-analysis. Clin Infect Dis. 2004;39(2):
206–217
7. Zaffanello M, Brugnara M, Franchini M,
Fanos V. Is serum procalcitonin able to
predict long-term kidney morbidity
from urinary tract infections in children? Clin Chem Lab Med. 2008;46(10):
1358–1363
8. Mantadakis E, Plessa E, Vouloumanou EK,
Karageorgopoulos DE, Chatzimichael A,
Falagas ME. Serum procalcitonin for
prediction of renal parenchymal involvement in children with urinary tract
infections: a meta-analysis of prospective
clinical studies. J Pediatr. 2009;155(6):
875–881, e1
9. Stewart LA, Parmar MK. Meta-analysis of
the literature or of individual patient data:
is there a difference? Lancet. 1993;341
(8842):418–422
10. Centre for Review Dissemination. Systematic reviews: CRD’s guidance for undertaking reviews in health care. Available at:
www.yorkacuk/inst/crd/SysRev/!SSL!/WebHelp/
SysRev3htm. Accessed December 1, 2012
11. Moher D, Liberati A, Tetzlaff J, Altman DG;
PRISMA Group. Preferred reporting items
for systematic reviews and meta-analyses:
the PRISMA statement. BMJ. 2009;339:
b2535
12. Bossuyt PM, Reitsma JB, Bruns DE, et al;
Standards for Reporting of Diagnostic Accuracy. Towards complete and accurate
reporting of studies of diagnostic accuracy:
the STARD initiative. BMJ. 2003;326(7379):
41–44
13. Lebowitz RL, Olbing H, Parkkulainen KV,
Smellie JM, Tamminen-Möbius TE; International Reflux Study in Children. International system of radiographic grading of
vesicoureteric reflux. Pediatr Radiol. 1985;
15(2):105–109
14. Whiting P, Rutjes AW, Reitsma JB, Bossuyt
PM, Kleijnen J. The development of QUADAS:
a tool for the quality assessment of studies
of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol.
2003;3(25):1–13
15. Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models. Med Decis Making. 2006;26
(6):565–574
16. Belhadj-Tahar H, Coulais Y, Tafani M,
Bouissou F. Procalcitonin implication in
renal cell apoptosis induced by acute pyelonephritis in children. Infect Drug Resist.
2008;1:17–20
878
17. Benador N, Siegrist CA, Gendrel D, et al.
Procalcitonin is a marker of severity of
renal lesions in pyelonephritis. Pediatrics.
1998;102(6):1422–1425
18. Bressan S, Andreola B, Zucchetta P,
et al. Procalcitonin as a predictor of
renal scarring in infants and young
children. Pediatr Nephrol. 2009;24(6):
1199–1204
19. Fernández Lopez A, Luaces Cubells C,
García García JJ, Fernández Pou J; Spanish Society of Pediatric Emergencies.
Procalcitonin in pediatric emergency departments for the early diagnosis of invasive bacterial infections in febrile
infants: results of a multicenter study and
utility of a rapid qualitative test for this
marker. Pediatr Infect Dis J. 2003;22(10):
895–903
20. Fernández López A, Luaces Cubells C, Valls
Tolosa C, et al. Procalcitonin in the early
diagnosis of invasive bacterial infection in
febrile infants [in Spanish]. An Esp Pediatr.
2001;55(4):321–328
21. Gervaix A, Galetto-Lacour A, Gueron T,
et al. Usefulness of procalcitonin and
C-reactive protein rapid tests for the
management of children with urinary
tract infection. Pediatr Infect Dis J. 2001;
20(5):507–511
22. Güven AG, Kazdal HZ, Koyun M, et al. Accurate diagnosis of acute pyelonephritis: How
helpful is procalcitonin? Nucl Med Commun. 2006;27(9):715–721
23. Pecile P, Miorin E, Romanello C, et al.
Procalcitonin: a marker of severity of
acute pyelonephritis among children. Pediatrics. 2004;114(2)e249–e254. Available
at: www.pediatrics.org/cgi/content/full/
114/2/e249
24. Tuerlinckx D, Vander Borght T, Glupczynski
Y, et al. Is procalcitonin a good marker of
renal lesion in febrile urinary tract
infection? Eur J Pediatr. 2005;164(10):
651–652
25. Bigot S, Leblond P, Foucher C, Hue V,
D’Herbomez M, Foulard M. Usefulness
of procalcitonin for the diagnosis of
acute pyelonephritis in children [in
French]. Arch Pediatr. 2005;12(7):1075–
1080
26. Gürgöze MK, Akarsu S, Yilmaz E, et al.
Proinflammatory cytokines and procalcitonin in children with acute pyelonephritis. Pediatr Nephrol. 2005;20(10):
1445–1448
27. Karavanaki K, Haliotis FA, Sourani M, et al.
DMSA scintigraphy in febrile urinary tract
infections could be omitted in children with
low procalcitonin levels. Infect Dis Clin
Pract. 2007;15(6):377–381
LEROY et al
Downloaded from by guest on March 5, 2016
28. Smolkin V, Koren A, Raz R, Colodner R,
Sakran W, Halevy R. Procalcitonin as
a marker of acute pyelonephritis in infants
and children. Pediatr Nephrol. 2002;17(6):
409–412
29. Kotoula A, Gardikis S, Tsalkidis A, et al.
Comparative efficacies of procalcitonin
and conventional inflammatory markers
for prediction of renal parenchymal inflammation in pediatric first urinary
tract infection. Urology. 2009;73(4):782–
786
30. Kotoula A, Gardikis S, Tsalkidis A, et al.
Procalcitonin for the early prediction of
renal parenchymal involvement in children
with UTI: preliminary results. Int Urol
Nephrol. 2009;41(2):393–399
31. Galetto-Lacour A, Zamora SA, Gervaix A.
Bedside procalcitonin and C-reactive protein tests in children with fever without
localizing signs of infection seen in a referral center. Pediatrics. 2003;112(5):1054–
1060
32. Andreola B, Bressan S, Callegaro S, Liverani
A, Plebani M, Da Dalt L. Procalcitonin and
C-reactive protein as diagnostic markers of
severe bacterial infections in febrile
infants and children in the emergency department. Pediatr Infect Dis J. 2007;26(8):
672–677
33. Nikfar R, Khotaee G, Ataee N, Shams S.
Usefulness of procalcitonin rapid test for
the diagnosis of acute pyelonephritis in
children in the emergency department.
Pediatr Int. 2010;52(2):196–198
34. Preda I, Jodal U, Sixt R, Stokland E, Hansson
S. Normal dimercaptosuccinic acid scintigraphy makes voiding cystourethrography unnecessary after urinary tract
infection. J Pediatr. 2007;151(6):581–584,
584, e1
35. Song F, Khan KS, Dinnes J, Sutton AJ.
Asymmetric funnel plots and publication
bias in meta-analyses of diagnostic
accuracy. Int J Epidemiol. 2002;31(1):88–
95
36. Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and
other sample size effects in systematic
reviews of diagnostic test accuracy was
assessed. J Clin Epidemiol. 2005;58(9):882–
893
37. Shaikh N, Ewing AL, Bhatnagar S, Hoberman A. Risk of renal scarring in children
with a first urinary tract infection: a systematic review. Pediatrics. 2010;126(6):
1084–1091
38. American Academy of Pediatrics. Committee on Quality Improvement. Subcommittee on Urinary Tract Infection.
Practice parameter: the diagnosis, treatment,
ARTICLE
and evaluation of the initial urinary tract
infection in febrile infants and young
children. Pediatrics. 1999;103(4 pt 1):843–
852
39. Downs SM; The Urinary Tract Subcommittee of the American Academy of
Pediatrics Committee on Quality Improvement. Technical report: urinary tract
infections in febrile infants and young
children. Pediatrics. 1999;103(4):e54. Available at: www.pediatrics.org/cgi/content/
full/103/4/e54
(Continued from first page)
Dr Leroy designed the study, helped in collecting the data, analyzed the data, interpreted results, drafted the manuscript, and approved the article version to be
published; Drs Fernandez-Lopez, Nikfar, Romanello, Bouissou, Gurgoze, Bressan, Smolkin, Leblond, Mr Vaos, and Mr Gervaix contributed to the study design,
acquired all the data in their individual centers, revised the paper for important intellectual content, and approved the article version to be published; Drs
Tuerlinckx and Gungor contributed to the study design, acquired all the data in their centers, and revised the paper for important intellectual content; Mr
Stefanidis had great input in the conception of the study, realized the data collection in his center, performed in-depth revision of the manuscript, and approved
the article version to be published; and Ms Gendrel and Mr Chalumeau contributed to the study design and interpretation of results, critically revised the
manuscript, and approved the article version to be published.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-2408
doi:10.1542/peds.2012-2408
Accepted for publication Jan 24, 2013
Address correspondence to Sandrine Leroy, MD, PhD, Centre for Statistics in Medicine, University of Oxford, Wolfson College Annexe, Linton Rd, Oxford OX2 6UD,
United Kingdom. E-mail: sandrin.leroy@gmail.com
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Dr Leroy was funded by a postdoctoral fellowship grant from the French Society of Nephrology and from the Fondation Bettencourt.
PEDIATRICS Volume 131, Number 5, May 2013
879
Downloaded from by guest on March 5, 2016
Association of Procalcitonin With Acute Pyelonephritis and Renal Scars in
Pediatric UTI
Sandrine Leroy, Anna Fernandez-Lopez, Roya Nikfar, Carla Romanello, François
Bouissou, Alain Gervaix, Metin K. Gurgoze, Silvia Bressan, Vladislav Smolkin,
David Tuerlinckx, Constantinos J. Stefanidis, Georgos Vaos, Pierre Leblond, Firat
Gungor, Dominique Gendrel and Martin Chalumeau
Pediatrics 2013;131;870; originally published online April 29, 2013;
DOI: 10.1542/peds.2012-2408
Updated Information &
Services
including high resolution figures, can be found at:
/content/131/5/870.full.html
Supplementary Material
Supplementary material can be found at:
/content/suppl/2013/04/24/peds.2012-2408.DCSupplemental.
html
References
This article cites 38 articles, 13 of which can be accessed free
at:
/content/131/5/870.full.html#ref-list-1
Citations
This article has been cited by 1 HighWire-hosted articles:
/content/131/5/870.full.html#related-urls
Subspecialty Collections
This article, along with others on similar topics, appears in
the following collection(s):
Urology
/cgi/collection/urology_sub
Permissions & Licensing
Information about reproducing this article in parts (figures,
tables) or in its entirety can be found online at:
/site/misc/Permissions.xhtml
Reprints
Information about ordering reprints can be found online:
/site/misc/reprints.xhtml
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned, published,
and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk
Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of Pediatrics. All
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from by guest on March 5, 2016
Association of Procalcitonin With Acute Pyelonephritis and Renal Scars in
Pediatric UTI
Sandrine Leroy, Anna Fernandez-Lopez, Roya Nikfar, Carla Romanello, François
Bouissou, Alain Gervaix, Metin K. Gurgoze, Silvia Bressan, Vladislav Smolkin,
David Tuerlinckx, Constantinos J. Stefanidis, Georgos Vaos, Pierre Leblond, Firat
Gungor, Dominique Gendrel and Martin Chalumeau
Pediatrics 2013;131;870; originally published online April 29, 2013;
DOI: 10.1542/peds.2012-2408
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
/content/131/5/870.full.html
PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
publication, it has been published continuously since 1948. PEDIATRICS is owned,
published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point
Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.
Downloaded from by guest on March 5, 2016