tracheostomy homecare booklet
advertisement

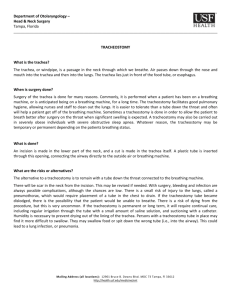
TRACHEOSTOMY HOMECARE BOOKLET IWK Health Centre, Halifax, N.S. PL-0570 Last Update: 06/13 Next Review: June 2016 1 TABLE OF CONTENTS INTRODUCTION Letter From IWK Health Care Team Learning List Phone List 3 4 5 TRACHEOSTOMY CARE What is a Tracheostomy? Parts of Tracheostomy Tubes Tracheostomy Suctioning Humidification Tracheostomy Skin Care and Tube Change Cleaning the Tracheostomy Tube Tracheostomy Tie/Chain Change 6 7 8 10 11 13 14 EMERGENCY CARE Emergency/Travel Bag Equipment Breathing Problems Mucus Plugging Accidental Tracheostomy Tube Dislodgement Aspiration Bleeding From the Tracheostomy Tube 15 15 16 16 16 17 HOME CARE and OTHER PARENTING QUESTIONS Home Care Tips 17 EQUIPMENT Equipment Maintenance Equipment List 20 21 REFERENCES 22 2 Dear Parents or Guardian: Your child will be receiving a tracheostomy to help him/her breathe. This Tracheostomy Home Care Booklet has been written to prepare you for your child’s hospital stay as well as for care in the home. To ensure the safest care for your child at all times, at least two caregivers must be educated in the care of the child with a tracheostomy. This must happen before discharge. Teaching starts as soon as the decision is made for a child to have a tracheostomy. The hospital staff will identify your learning needs and develop a plan to meet them. Before discharge we will complete a caregiver guide with you and the co-caregiver. As treatments change over time, caregivers should remain current in their skills and knowledge. This will ensure your child will always receive safe, up to date care. The length of time a child remains in hospital will vary depending on both their medical needs and the familiy’s learning needs. The social worker, the Community Care Resource Nurse (CCRN) or the Out of Province Liaison will help you with plans for home equipment and supplies. Hospital staff will provide information on medical equipment and supply companies. They will arrange contact with the appropriate one for your child. In the Maritimes, home tracheostomy care supplies are not routinely covered by the Department of Health, but this varies in each province. If your family has private insurance coverage, the CCRN or Out of Province Liaison will check into this coverage. For families without insurance, hospital staff will discuss options and help negotiate for alternative funding assistance. You will meet many members of our health care team throughout your child’s hospital stay. Please feel free to discuss any concerns you may have during this transition from hospital to home. Sincerely, IWK Health Care Team 3 CAREGIVER GUIDE FOR CARING FOR A CHILD WITH A TRACHEOSTOMY Before a child goes home, you and a co-caregiver will need to learn the following care. Any person a child will be staying with needs to learn all of this care. When you and your co-caregiver have completed trials of a skill or learning area on the following list, place a checkmark in the box below. Caregiver Co-caregiver 1. Why your child needs a tracheostomy tube ❑❑❑ ❑❑❑ 2. Type and size of your child’s tracheostomy tube ❑❑❑ ❑❑❑ 3. Why, when and how to suction the tracheostomy tube ❑❑❑ ❑❑❑ 4. Cleaning the skin around the tracheostomy tube ❑❑❑ ❑❑❑ 5. Why, when and how to change the ties/chain ❑❑❑ ❑❑❑ 6. Why, when and how to change the tracheostomy tube ❑❑❑ ❑❑❑ 7. Humidification, when it is needed ❑❑❑ ❑❑❑ 8. Supplies to have with your child at all times ❑❑❑ ❑❑❑ 9. Potential emergencies and how to help your child ❑❑❑ ❑❑❑ 10. The signs of respiratory distress and infection ❑❑❑ ❑❑❑ 11. Activities your child can do and activities to avoid ❑❑❑ ❑❑❑ 12. How to give medications, aerosols if needed ❑❑❑ ❑❑❑ 13. Competent in the use of necessary equipment and monitors ❑ ❑ ❑ ❑❑❑ 14. How to give oxygen through the tracheostomy tube ❑❑❑ ❑❑❑ 15. Rooming in 24 hour transitional care completed ❑ ❑ 16. Other ___________________________________ ❑❑❑ ❑❑❑ We have read the Tracheostomy Care Booklet, and we understand what is required before _______________________________ is released in our care. Caregiver ____________________________________________________ Co-caregiver__________________________________________________ 4 IMPORTANT PHONE NUMBERS TO KEEP NEXT TO THE PHONE AND IN TRAVEL/EMERGENCY KIT SERVICE NAME and PHONE NUMBER 911 For Emergency Local Physician _________________________________ Local Hospital _________________________________ Local Friend/Neighbour _________________________________ Equipment Company ________________________________ Equipment Supplies Contact _________________________________ Community Care Resource/Liaison Nurse _________________________________ ENT Clinic (IWK Health Centre) _________________________________ Nursing Unit (IWK Health Centre) _________________________________ Social Worker _________________________________ Other _________________________________ 5 What is a Tracheostomy? The picture above shows the location for the trachea (wind pipe), vocal cords, and esophagus (food pipe). It is important to understand where these structures are located. It will help you to understand where the tracheostomy is, why your child has one, and how it affects the air that they breathe. A tracheostomy is an opening into the windpipe (trachea) though the neck. The windpipe carries the air we breathe into the lungs. A tracheostomy tube is inserted into an opening (stoma) into the trachea. This allows the air to go directly to the lungs without passing through the nose, mouth, or the larynx (voice box). Your child will not be able to produce sounds; however there are other ways to produce sound. Voice and communication is discussed later in the booklet. The doctor will decide which type of tracheostomy tube is best for your child’s needs depending on the reason for the tracheostomy. The doctor may need to increase the tracheostomy size as your child grows. The reason your child has a Tracheostomy is: _______________________________________________________________________________________ _______________________________________________________________________________________ The type and size of your child’s Tracheostomy Tube is: Type: _______________________ Length: _______________________ Size: ______________ 6 Parts of the Tracheostomy Tube Flange – the soft “winged” collar that lies against the child’s neck Shaft – the main body of the tracheostomy tube Obturator – serves as a guide during tube insertion. The inner cannula (if present) is removed and the obturator inserted. The olive shaped tip should extend just beyond the end of the tube and is used to prevent harm to the windpipe by the blunt edges of the tracheostomy tube. It is removed immediately after the tube is inserted and should be kept in a safe location. Cuff – a soft, inflatable band around the end of a cuffed tracheostomy tube. Cuffed tubes are used when it is not desirable to have a leak around the tracheostomy tube, for instance when the leak interferes with mechanical ventilation. HOME PROCEDURES Balloon – Some tracheostomy tubes have a cuff on the end. This is a balloon that is filled with air to create an airtight seal between the tracheostomy tube and the windpipe. th Both photos reproduced with permission from Susan Gilbert personal communication, December 15 , 2008 Most children have tracheostomy tubes without the cuff and balloon. 7 PROCEDURES Hand washing before and after all of the following procedures is very important for you and your child’s health. SUCTIONING A TRACHEOSTOMY TUBE PURPOSE: To keep the airway open and free of mucus and dry secretions that may block the tracheostomy tube, allowing your child to breathe more easily. WHEN TO SUCTION: Secretions can be heard bubbling in the tracheostomy tube or trachea, and your child cannot cough them out on their own. You can hear a wheezy sound. The nostrils flare out with each breath. Your child complains of difficulty breathing. The skin sucks in between the ribs with each breath (in-drawing). A child in distress may be warm, flushed, perspiring, restless, anxious, and may be struggling to breathe. Your child may appear pale, bluish or greyish in color. SUPPLIES NEEDED: Suction machine, tubing and size __catheter Breathing bag (for some children) Clean cup/bowl with fresh water or saline to rinse catheter Oxygen if needed Tissues Gloves(optional for home care; if used use powder free) HOW TO SUCTION: Keep a suction catheter near the bedside that is measured and marked against the length of the tracheostomy tube. It should be measured against the first hole in the suction catheter’s farthest end, not the end of the catheter. A measuring tape affixed to the crib/bed that is marked with the appropriate length could also be used. 1. Connect catheter to tubing of suction machine and turn on machine. Suction some saline through catheter to be certain catheter is clear and suction is working. When you obtain your home suction machine, the suction limit will be preset. A representative from the company supplying the machine will show you how to operate the suction as well as cleaning procedures. 2. Some children need extra breaths with a manual resuscitator (Ambu bag). Manual breaths are usually not needed for stable children with no additional breathing problems. If bagging is needed, be sure to suction any visible secretions first, and then give 2-3 breaths. Pre-oxygenate if ordered by your doctor. 3. The distance the catheter will be inserted will be determined according to your child’s tracheostomy type and size. Slide the catheter gently down the tracheostomy tube to that distance. DO NOT APPLY SUCTION WHEN INSERTING THE CATHETER. 4. Apply suction by placing your thumb over the special opening at the far end of the catheter closest to the suction tubing. Using a rotating motion, gently withdraw the catheter out of the tracheostomy tube. Rotate by using a rolling motion with the catheter held between the thumb and forefinger. 5. Continue steps 3 and 4 rinsing the catheter each time it is removed to clear the secretions out of the catheter, until the tracheostomy tube is clear of secretions. 8 Tips: If your child’s secretions should become thicker, stickier or foul smelling: Your child’s fluid intake may need to be increased. Children who have vomiting/diarrhea may get dehydrated. Your child may need more humidification. You may have to instill the tracheostomy. You may have to change the tube more often as it may block when the secretions are thick. Seek medical attention if your child has brown/green/ or bloody secretions INSTILLATIONS: Routine instillation is not recommended Only instill when secretions are thick or blood tinged. Supplies used for routine suctioning need to be on hand. Instill _____ mls of room temperature saline into your child’s tracheostomy tube. Saline on hand If you are using a breathing bag - have it ready to use. Suction catheter hooked up and ready to use. Suction the tracheostomy once before you instill the saline, to ensure you can pass the catheter. Instill the required amount of saline into the tracheostomy tube. Your child will probably cough when the saline is instilled. If your child requires manual inflation of the lungs, attach the breathing bag to the tracheostomy tube and gently inflate the lungs two times, or as ordered. Suction the tracheostomy. If you are using a breathing bag, gently inflate the lungs 2-3 times and then listen to see if the airway sounds clear. You may have to repeat the instillations if the secretions are very thick and you can’t clear them just with suctioning. How to make normal saline (optional): Sterile saline should be used for instilling, but you may wish to make up your own normal saline solution for rinsing/flushing suction catheters. Use water supply that is known to be safe (tested well water or city supply) There are two methods A) Saline tablets - these may be obtained at most pharmacies and cost very little. Follow directions on package, using water that has been boiled for 5 minutes. B) Boil water for 5 minutes. Pour 2 cups into clean container with watertight lid. Add one teaspoon table salt using clean spoon. Close lid. Shake well. Mix new batch daily. How to sterilize water for nebulizers: Boil tap water for 10 minutes. Allow to cool, then place in a clean jar and refrigerate for up to 24 hours. Make new batch daily. 9 HUMIDIFICATION: Normally the air we breathe in is warmed, filtered and humidified as it passes through the nose and mouth to the lungs. This does not happen with a tracheostomy because the air enters the lungs through the tracheostomy tube. It is necessary to artificially humidify air breathed in through a tracheostomy to prevent drying of lining of the respiratory tract and to keep secretions loose and easy to cough or suction out. Adding humidity to the airway should be part of your child’s daily routine. Humidification Devices –Heat and Moisture Exchangers The artificial nose is a small plastic device with an inside coil of paper that fit directly over the outside of the tracheostomy. It captures and holds moisture that is in your child’s exhaled air. Humidification Machine with mask and tubing Artificial Nose A tracheostomy mask, also known as a mist collar is illustrated above. The mask should be worn when your child is asleep, if using oxygen through the tracheostomy, or if secretions are thick or bloody. If your child refuses to wear a mist collar, try a loose fitting cloth bib without plastic backing. 10 TRACHEOSTOMY SKIN CARE Purpose: Skin at the tracheostomy site needs to remain clean and dry. If drainage collects around the tracheostomy tube, germs can grow and cause infection or skin rashes. When: It is important to do this 2-3 times a day, or as needed if there is redness, irritation or secretions sitting on the skin. Supplies Needed: Cotton swabs Saline or clean water in a cup or bowl Mild soap and water (use only on healthy skin) Tracheostomy dressing if needed How to Clean: 1. Look at the neck; note cuts or signs of infection 2. Dip the cotton swab in saline or clean water 3. Starting at the stoma, stroke away from the tracheostomy opening, using one stroke per swab. Discard swab. Repeat around stoma area. 4. Clean the skin under the ties/chain with mild soap and water, followed by clean water or saline. Dry the skin well the same way you cleaned it with the dry cotton swab. 5. Apply a dressing if tracheostomy tube is rubbing the skin. TRACHEOSTOMY TUBE CHANGE Purpose: To prevent mucus plugs in the tracheostomy tube and to keep the tracheostomy tube clean. When: Change the tracheostomy tube every 1-2 weeks. Supplies: Breathing bag Scissors/wire cutters depending on type of ties/chain Supplies for suctioning Tracheostomy tube ties, chain or self fastening ties Clean current size tracheostomy tube with obturator inserted ½ Size smaller tracheostomy tube with obturator inserted Rolled towel Lubricant (all the lubricants should be water soluble) 11 How to change: 1. Two people must be present to change a tracheostomy tube. There are two roles, the main role and the helper role. The person who performs the main role changes the tracheostomy tube, holds the tube in place until helper is finished securing the ties, assesses and maintains airway. The helper is needed to hold your child in the correct position, removes ties, cleans neck and stoma, suctions and secures ties when tube is changed. 2. Lubricate the clean tracheostomy tube with water soluble lubricant. Try to prevent the lubricant form entering the tube lumen (the hole in the end of the tracheostomy tube). 3. Place the obturator into the clean tracheostomy tube. 4. Tie the tracheostomy tube ties OR attach chain to the clean tracheostomy tube to be inserted. When using a chain, be sure to check every time you change it that the length is still right for your child - it may be necessary to add or remove balls from one change to the next. 5. Place a rolled towel under your child’s shoulders so that the head is bent back with the neck extended so that the hole in the skin can be clearly seen. Some children prefer to sit up. 6. Suction the tracheostomy tube and clean around the stoma. 7. Have your helper hold your child’s chin up. It may be necessary to gently hold your child’s hands away from the tracheostomy site during tube change. 8. To remove the old tracheostomy tube: Cut the tracheostomy tube ties, OR unfasten the chain. This is a good time to wash, dry and inspect the back of the neck. Remove the old tracheostomy tube. 9. Insert the clean tracheostomy tube using one single motion following the curve of the trachea. Make sure your thumb pushes gently on the obturator during insertion. 10. Hold the tracheostomy in place and remove the obturator immediately, to allow your child to breathe. 11. The helper can secure the ties/chain. Bend your child’s head forward and tie the tracheostomy ties securely to the side of the neck OR fasten neck chain making sure that one of your fingers can fit comfortably under the ties or chain. The ties or chain should be neither too loose nor too tight. Check around the back of the neck to ensure ties are not twisted or wrinkled, as this could cause areas of irritation on the skin. Keep the obturator in an easy-to-find location so that it can be used to re-insert the tracheostomy tube if it should happen to fall out. 12 PROCEDURE FOR CLEANING TRACHEOSTOMY TUBES: What you will need: 2 small bowls/basins (1 “dirty”, 1 “clean”) Soiled tracheostomy tube and obturator Pipe cleaners Mild dish detergent Tap water Twill tape/Self Fastening ties or tracheostomy chain Clean cloth/paper towel Clean jar with lid or clean zip-loc bag 1. Soak the tracheostomy tube in some warm soapy water to loosen secretions. Moisten a pipe cleaner to clean inside the tube. A dry pipe cleaner may leave lint behind. 2. Wash the tracheostomy tube and obturator in warm soapy water, using pipe cleaners as needed for inside tube. 3. Rinse well with tap water. 4. Inspect the tracheostomy tube for cracking, rough spots or breakage - discard if problems noted. 5. Place tracheostomy tube on clean cloth/paper towel and allow to air dry. (Note: DO NOT USE hair dryer to dry) 6. Attach twill tape, chain or self fastening ties. Store in a clean jar with a lid or a zip-loc bag. PVC plastic tracheostomy tubes are discarded 29 days after the package is opened, or when the tube shows signs of wear. Silicone tracheostomy tubes can be used indefinitely as long as they do not show signs of damage. Cleaning the Tracheostomy Tube Chain: Scrub well with soap and water and rinse well with tap water. Dry well with a soft cloth. Store in a closed container or bag and keep it close to your child at all times. 13 Tracheostomy Tie/Chain Change Purpose: Tie changes are done to prevent the tracheostomy tube from falling out and to prevent rashes and skin breakdown. When: Ties are changed daily or when ties are wet/dirty. Supplies: Twill tape/tracheostomy chain/self fastening ties Scissors or wire cutters Second person to hold tracheostomy in place Supplies for suctioning Supplies to clean around neck after ties/chain is removed (i.e.: facecloth, towel) How to change: Alternate the side of the neck that the clasp or knots lies on with each change. Chain clasp needs to be readily accessible in the event of an emergency. If unable to unclasp chain, cut with wire cutters. Fasten and unfasten the chain clasp several times to ensure it will undo easily in an emergency. This procedure always requires two people. Spare chain and wire cutters should always be on hand. Chains and wire cutters may be purchased at most department or hardware stores. 1. Cut the length(s) of twill tape needed or count and measure the chain. The length of the chain is determined by encircling the neck with a chain and noting the length at which the chain is secure. Measure from end to end including the clasp. Cut off excess chain with wire cutters. Each time a new chain is applied it should be according to the size of the child’s neck making sure the chain permits one finger to slide under it comfortably. Ensure the integrity of self fastening ties in that it grabs well. 2. Remove the self fastening ties or cut and remove the soiled twill tape or chain while the second person holds the tracheostomy tube in place. 3. Twill tape: Using one piece of twill tape, place one end up through the underside of one tracheostomy flange hole. Bring the other end of the twill tape around the back of the neck. Place tape through the underside of the other hole and bring this end back to the other side. Pull both ends snugly to the side of the neck and tie them together in a triple knot over one finger/allowing one finger width of slack. 14 4. Chain: If using a PVC tracheostomy, thread chain up through the opening of one tracheostomy flange across and down through the opening of the other tracheostomy flange. If using a silicone tracheostomy, place chain through the underside of the hole, then bring the other end of the chain around the back of the neck, place the chain through the underside of the other hole and bring this end back to the other side. For either type of tube, the clasp should be located on the side of the neck, fasten clasp. Recheck that chain is secure and tight enough by checking clasp and inserting one finger between chain and neck. 5. Self fastening ties: Thread one end of the tie up through the hole on one tracheostomy tube flange and hook fastener to the fuzzy side of the tie. Repeat this procedure on the other side. Ensure sharp edges of the self fastening ties are not touching your child’s skin. These ties must be hand washed only and air-dried a maximum of 5 times. Mark a dot on the back of the ties with a permanent marker each time they are washed. Discard after the sixth wearing. If your child is prone to pulling the tracheostomy tube or ties, self-fastening ties are not a good option for your child. EMERGENCY CARE: The following equipment can be placed in a sturdy bag with a secure closure. Suggestions are diaper bag, large purse or backpack. Emergency/Travel Bag Equipment Spare tracheostomy tube with ties/chain attached in case you need to change the tracheostomy tube. Tracheostomy tube ½ size smaller than one in place with ties/chain attached. Extra tracheostomy ties/chain Spare humidification device/speaking valve (if used). Small clean jar with saline/water for cleaning suction catheter. Scissors/wire cutters Breathing bag (this should be included if your child needs it when you suction) Fully charged portable suction machine and suction catheters ( proper size for both current tracheostomy tube and smaller tracheostomy tube) Normal saline Fully charged cellular phone/pager with phone list Equipment bag list of supplies, keep in kit for restocking Recognizing Breathing Problems Sometimes, immediate action is necessary when your child has breathing problems. If any of the following problems occur, it is important that you DO NOT PANIC. You need to STAY CALM, and care for your child. You will learn the signs that your child has trouble breathing before you leave the hospital. Early signs of breathing trouble: Noisy breathing Fast breathing Sweaty ,clammy skin Restlessness Change in breathing pattern Later signs of breathing trouble: Chest, neck or ribs sucking in or head bobbing Flared nostrils Blue or grey color around the lips, nails and skin Your child does not wake to your touch 15 Mucus Plugging If the tracheostomy tube becomes plugged, your child will not be able to breathe through it. 1. Suction-do not force 2. If you cannot clear, remove the plugged tracheostomy tube immediately. 3. Put a new tracheostomy tube in place. Your child should be able to breathe through the new tube. 4. Call 911 if your child is not breathing and begin Emergency Response Sequence/CPR. 5. When your child recovers, remember to assess if he needs more humidity. If a tracheostomy tube has blocked, it is usually from thick, dried mucus in the tube. Your child may need more humidity and offer plenty of fluids to keep the mucus thin and easy to cough/suction. Accidental Tracheostomy Tube Dislodgement: 1. Put a new tracheostomy tube in place - IMMEDIATELY 2. If you do not have a new tracheostomy tube with the child, put the old one back in place after cleaning mucus from the tube. 3. Change to a clean tracheostomy tube as soon as you can. 4. If you cannot get a new tracheostomy tube in place call 911 and start Emergency Response Sequence/CPR if needed. It is strongly recommended that the child’s home caregivers be certified in CPR before discharge. It is also important to keep up to date in CPR skills by being recertified on a yearly basis. Recognizing Aspiration: Aspiration is the passage of liquids, solids or saliva from the esophagus (feeding tube) into the airway. Watch your child eat and drink. Signs of a child aspirating would be: choking or coughing with swallowing watery tracheostomy secretions, especially after swallowing drooling or holding fluids in the mouth the color of the food or liquid your child is swallowing is coughed/suctioned from tracheostomy tube frequent chest infections Ways to prevent aspiration: Thicken liquids with thickeners or puddings, baby foods, cereals, or yogurt. Thicker liquids are easier to swallow than thinner liquids Encourage slower eating and swallowing Sitting upright while eating/drinking Ways to handle aspiration: Suction the tracheostomy tube until clear of food/fluid, saline instillations may be necessary to clear Change the tracheostomy tube if you’re the tube is plugged with food or liquids Call your doctor if your child has continued signs of aspiration as listed above. Your doctor may recommend working with a feeding therapist Children can also aspirate if vomiting. Turn your child’s head to the side and suction tracheostomy as necessary. Place babies on their side for sleeping unless it is not recommended for your child. 16 Recognizing Bleeding: Bloody streaks in the mucus can occur from dry air, frequent or vigorous suctioning, infection, coughing especially if loose ties, trauma from the tube, foreign body in the airway Bright red blood from the tube is serious Ways to prevent bleeding Use humidity and suction with the technique outlined in this handout See your doctor early if signs of infection or increased coughing Regular checkups to unsure proper fit of the tracheostomy tube Ways to handle bright red bleeding: 1. Call 911 2. Stay calm 3. Gently suction the length of the tracheostomy tube 4. Possible use of cooler saline to gently instill, soothing the airway and preventing plugs 5. If bleeding subsides use humidity until help arrives Ways to handle blood streaked mucus: 1. Gently suction the length of the tracheostomy tube 2. Increase use of humidity 3. Wet the end of tracheostomy tube with saline or lubricant when changing 4. Instill with saline if indicated 5. Call your doctor for a checkup HOME CARE TIPS Here are some tips for you to consider in your child’s care. Feel free to write down your own tips and share them with your nursing staff and health care team. If you have to suction your child during a meal, do so gently to decrease the chance of vomiting. Your child should not go under water! Bath time should be closely watched to prevent water from entering the tracheostomy tube. An artificial nose should be worn on the tracheostomy tube to prevent splashed water from entering the tube. Children with tracheostomies should not swim. When washing your child’s hair, carefully pour water over the hair with a cup as your child is lying back with his or her head and neck supported (see drawing below). At first you may need a second person to assist. 17 Suction just before feeding and avoid for two hours after feeding, to avoid risk of vomiting. Suction gently if necessary during feeding. Do not use powders or aerosol sprays around your child. Contact sports should be avoided. Avoid hairy or fuzzy clothing around the tracheotomy tube. Also do not use clothing that blocks the tracheotomy tube (for example, turtle neck shirts). When choosing a pet, consider one that can live outside or that will not shed. Do not smoke around your child. Smoke is very irritating to your child’s airway, lungs, and ears. Your child should avoid areas with sand. Your child may play outdoors, but may need to wear a scarf/bib over tracheostomy tube and should be supervised. Caution advised with small objects your child may put in his tracheostomy tube i.e. beans, small toys pieces etc. Speech and communication: Speaking Valves: A speaking valve is a small plastic one-way valve that attaches to the outside of a tracheostomy tube. It allows the child to breathe in through the tracheostomy tube, but on exhalation the air is directed around the tracheostomy and through the vocal cords, allowing sounds to be made. There are different types of speaking valves on the market and each has specific instructions for use and cleaning depending on the brand. Speaking valves are only to be used when your child is awake and under direct supervision. Before a speaking valve can be used, there must be enough room for air to move around the tracheostomy tube and through the vocal cords. The doctor will tell you if and when your child may be able to use one. Please follow manufacture’s instructions for cleaning the speaking valve. Your child may have difficulties communicating and will work with a speech-language pathologist to work on communication skills. School: Almost every child with a tracheostomy tube can go to a regular school. The school should be given as much advanced notice as possible about your child so they have enough time to assess the child’s needs and put any necessary arrangements in place. The school teacher and some other school staff will need to know how to help your child care with his tracheostomy tube, so your child is in a safe learning environment. Sleeping arrangements: Parents often worry that their child may need suctioning at night while they are sleeping and that they would not wake up. There are things you can do so that you will wake up if your child needs you. A bell can be placed at the bedside of an older child should he/she be not able to call for help. For younger children portable intercoms may be used between the baby’s room and the parents throughout the house. Additionally, a bracelet or anklet of bells can alert parents to excessive movement caused by breathing difficulty. Intercoms can be bought at radio, electronic and department stores. When you plan to leave the house, the following may be helpful: If your child is suctioned routinely, suction before leaving your home. Check to make sure your travel kit has all the supplies you need. You may want to make a list of the supplies and keep it with your kit. If you are going away for any length of time you should check out local emergency, power and phone services - plus phone numbers where you will be staying. Let them know your child is in the area and what possible needs there may be. 18 Weather and inside heating / air conditioning: Different kinds of weather may affect your child and the tracheostomy tube. You will need to be aware of the effects and what you may need to do to help your child. Cold Weather - may cause secretions to become thicker and dryer. It is also uncomfortable to breathe very cold air into the trachea. You should watch for thickening of secretions and increase humidity if needed. When your child is outside you can use a scarf or bandanna loosely around the tracheostomy tube to help warm the air breathed. An artificial nose may be helpful in addition to protective clothing. Mild, humid weather - may help keep secretions loose, making it easier for your child to cough them up. Windy, dusty weather - may get dust into trachea and cause more thick secretions. You may need to suction your child more frequently. A bib or scarf over your child’s tracheostomy tube may help to keep some dust out of it. Heaters and air conditioners - often pull some of the moisture out of the air. This may cause your child’s secretions to become thick and dry. If home humidifiers are used it is very important to keep devices extremely clean to prevent spore and mold growth. Before Going Home from the Health Centre: 1. 2. 3. 4. 5. 6. Learn all the care associated with the tracheostomy tube and practice this care as much as possible. At least 24 to 48 hours to be spent with the child before discharge on the child’s own unit. Ensure you are familiar with the use of all necessary equipment and supplies. Discuss the need of respite care with the health care team. Prepare an emergency list and keep it close to your phone. If living in rural area, the Department of Highways should be notified to ensure snow ploughing for your area is a priority 7. The local hospital should be notified of the child’s condition. The local hospital should also have an IWK contact number if the need should arise. 19 EQUIPMENT MAINTENANCE Equipment maintenance is very important in your child’s care. Cleaning the equipment as directed will help to prevent infection. Maintaining the equipment as directed also insures the safety and proper functioning of the equipment. The maintenance of your equipment will vary based on your child’s needs. Equipment will also vary from different equipment companies; therefore, follow your equipment company’s recommendations for maintenance. The equipment company will also have a person on call 24 hours a day should you have any questions or problems. Below are some guidelines for cleaning suction and humidity equipment. Suction Equipment: The following tips apply to cleaning suction equipment: Empty the suction bottle in the toilet. Clean bottle with warm, soapy water once a day. Rinse with clean water and allow to air dry. Once the bottle is clean a small amount of vinegar can be put in the bottle to absorb odors. Replace disposable bottles once a month or sooner if permanently soiled or damaged. Wash the connecting tube daily with warm, soapy water. Rinse with clear water and allow to air dry. Having two tubings in use at a time is helpful to alternate. Discard and replace the suction connecting tubing every month or more often if needed. Do not boil plastic connecting tubing. Two suction catheters are allotted for a 24 hour period. After suctioning, the catheter is rinsed with saline (see instructions for making saline at home, page 9). Wipe the outside of the catheter with an alcohol swab and store catheter in the suction packaging. Discard catheter after 24 hours. Humidification Equipment: Change artificial nose when wet or full of secretions Disassemble and clean nebulizer bottles and aerosol tubing 2-3 times per week, replacing them as needed. Clean tracheostomy mask daily with soap and water, rinse well with water, air dry. Change the compressor filter monthly. 20 TRACHEOSTOMY EQUIPMENT & SUPPLY LIST □ Pulse Oximeter □ Portable Suction Unit circle requirement: 1 or 2 □ Air Compressor All Purpose Nebulizer □ High Humidity Compressor □ Resuscitation Bag □ Stethoscope Indicate MONTHLY Quantities: Trach Tube: Size : _________ Length: ______ (½ Size Smaller Trach Tube Size: ______ ) Brand: _________ Description: _____________________________________ Trach Chain: Length: ____ inches Qty: _____ Posey Ties: circle: Sm / Med / Lge Qty: _____ Speaking Valve: Type: ______________ Qty: _______ Trach Mask: circle: Pediatric / Adult Qty: _______ Medication Nebulizer: Qty: ______ Sterile Saline Instills: Qty: ______ Saline Tubs: Qty: ______ Humidivents: Qty: ______ Humidivent Minis: Qty: _____ Oxygen Saturation Probes: Qty: _______ Corregated Tubing for High Humidity Compressor: Qty: ______ 48” lengths Connector for Corregated Tubing: Qty: ______ Suction Connecting Tubing: Qty:_____ Suction Catheters: Size: _____FR Qty:_____ Suction Cannister, Filter & Elbow: Qty: ______ per year Gloves, Non‐Sterile: circle: Sm / Med / Lge Qty: _________box(es) of 100 Pipe Cleaners: Qty: _________ Waterproof Tape: circle: 1 inch / 2 inch Qty: _______ Water Soluble Lubricant (Muko): Qty: _______ box(es) of 100 Cotton Tipped Applicators: Qty: _____ box(es) of 100 Scissors / Wire Cutters ___________ Gauze: Type: ________________ Qty: __________ Any Other Supplies: _____________________________________________________________ Home Oxygen: Mode of delivery _________ Provided by _____________________ Concentrator/litre flow _____________ Portable O2 Tanks __________________ □ CPAP _____________________________ □ BiPAP _____________________________ Home Ventilator: Settings: ______________________________________________________ 21 References 1. American Head and Neck Society (2009). Patient Education – Tracheostomy Care. Retrieved January 2009 from http://www.headandneckcancer.org 2. Bissell, C. M. (2008). Pediatric Tracheostomy Home Care Guide. Sudbury, MA: Jones and Bartlett Publishers 3. Bissell, C.M. (2008). Aaron’s Tracheostomy Retrieved January 2009 from http://tracheostomy.com/networking/parent/index/htm. 4. Bowers, B., Scase, C., (2007). Tracheostomy: Facilitating Successful Discharge from Hospital to Home. British Journal of Nursing 5. Cincinnati Children’s Hospital ENT Team (2008). Tracheostomy Care Handbook, Retrieved March 2009 from http://cincinnatichildrens.org/suc/alpha/o/ent/resources/trach-handbook/defauly.htm 6. Johnston, K., Zevenhuizen, J., (2009) Tracheostomy Care Self Directed Learning Program. Halifax, NS: IWK Health Centre. 7. Mauricio, R.V., Montagnino, B.A. (2004) The Child With A Tracheostomy and Gastrostomy: Parenteral Stress and Coping in the Home –A Pilot Study, Pediatric Nursing Journal 8. Mayo Foundation for Medical Education and Research, 1998-2009. Tracheostomy, Retrieved January, 2009 from http://mayoclinic.com/health/tracheostomy/MY00261/DSECTION 1-4,. 9. O’Brien, M. E., Wegner, C.B. Rearing the Child Who Is Technology Dependant: Perceptions of Parents and Home Care Nurses, Journal for Specialists in Pediatric Nursing 10. Rice, Robyn (2006). Home Care Nursing Practice, Philadelphia, PA,: Mosby Elsevier. 11. Thomson Micromedex (1974-2009) Tracheostomy Care for Children Retrieved January 2009 from http://thomsonhc.com/carenotes/tracheostomycareforchildren 22 23