Your diagnosis?
advertisement

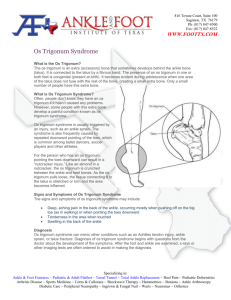
n radiologic case study Enhance your diagnostic skills with this “test yourself” monthly column, which features a radiograph and challenges you to make a diagnosis. The case: A 36-year-old man presented with chronic posterior left ankle pain. A B Figure: Lateral radiograph (A) and sagittal inversion-recovery magnetic resonance image (B) of the left ankle. Your diagnosis? For answer see page 63 JANUARY 2013 | Volume 36 • Number 15 n radiologic case study Section Editor: Terrence C. Demos, MD S P OT L I G H T O N foot and ankle Diagnosis: Os Trigonum Syndrome Albert J. Song, MD; Matthew Del Giudice, MD; Martin L. Lazarus, MD; Laurie M. Lomasney, MD; Terrence C. Demos, MD; Katherine Dux, DPM Answer to Radiologic Case Study Case facts appear on page 5 A 36-year-old man presented with chronic posterior ankle pain. A lateral radiograph of the left ankle showed tibiotalar and posterior subtalar joint effusions (Figure 1A). In addition, an isolated ossicle was observed posterior to the talus—an os trigonum. Infiltration at Kager’s fat pad was nonspecific. A sagittal inversion-recovery magnetic resonance image of the left ankle confirmed a posterior subtalar joint effusion and inflammation of Kaeger’s fat pad (Figure 1B). Also, an abnormal bone marrow edema pattern was observed with high signal in the os trigonum, as well as the adjacent posterior talus and superior calcaneus. In a patient with chronic posterior heel pain, this is characteristic of os trigonum syndrome. Incidentally, the Achilles tendon has normal imaging characteristics. Impingement syndrome of a joint refers to the mechanical obstruction or restriction of motion by intervening soft tissues or osseous structures, resulting in a chronic painful arc. Impingement syndromes of the ankle can be anterior, anterolateral, anteromedial, posteromedial, or posterior to the joint.1 The authors are from the Department of Radiology (AJS, MDG, LML, TCD) and the Division of Podiatry (KD), Loyola University Medical Center, Maywood, and the Department of Radiology (MLL), Northshore University Health System, Evanston, Illinois. The authors have no relevant financial relationships to disclose. Correspondence should be addressed to: Laurie M. Lomasney, MD, Department of Radiology, Loyola University Medical Center, 2160 S First Ave, Maywood, IL 60153 (llomasn@lumc.edu). doi: 10.3928/01477447-20121217-01 1A 1B Figure 1: Lateral radiograph of the left ankle showing tibiotalar and posterior subtalar joint effusions posteriorly (white arrow). Note the isolated ossicle (yellow asterisk) posterior to the talus—an os trigonum (A). Sagittal inversion-recovery magnetic resonance image of the left ankle showing posterior joint effusion, inflammation of Kager’s fat pad (white arrows), abnormal bone marrow edema pattern with high signal in the os trigonum (yellow asterisk), and adjacent posterior talus and superior calcaneus (red arrows) (B). Posterior ankle impingement syndrome has been termed os trigonum syndrome, talar compression syndrome, posterior tibiotalar impingement syndrome, and posterior block of the ankle.2-5 Although extensively described in ballet dancers, os trigonum syndrome has also been reported in soccer, football, and volleyball players, downhill runners, and even nonathletes.2,3,5-7 Anatomy and Pathophysiology The posterior process of the talus consists of medial and lateral tubercles and the intervening groove for the flexor hallucis longus tendon. An os trigonum results from failure of a secondary ossification center to fuse to the lateral tubercle of the posterior process of the talus (Figure 2). This secondary ossification center appears between ages 8 and JANUARY 2013 | Volume 36 • Number 163 Cover Story Cover illustration © Scott Holladay 64 ORTHOPEDICS | Healio.com/Orthopedics n radiologic case study 13 years and typically fuses within 1 year.2,5,6 An os trigonum is seen in up to 14% of the general population.1 The os trigonum has 3 surfaces: anterior, inferior, and posterior. The anterior surface forms a synchondrosis with the posterior process of the talus. The inferior surface can articulate with either the calcaneus or the posterior subtalar joint. The posterior talofibular ligament inserts onto the posterior surface of the os trigonum.2 Impingement and pain can result from several specific pathologies affecting this complex regional anatomy. Classically described in ballet dancers who perform enpointe and demi-pointe, os trigonum syndrome is due to repetitive dorsi- and plantarflexion of the ankle causing impingement of posterior ankle soft tissue and osseous structures.6 Direct compression of the os trigonum or disruption of the synchondrosis may be observed. An enlarged os trigonum increases the probability of chronic impaction injury.1,6 An elongated lateral tubercle, known as a Steida process, extends from the posterior process of the talus and is thought to predispose individuals to posterior ankle impingement.7 Compression of the Steida process has been implicated as a cause of posterior ankle impingement. Distinguishing a fracture of the Steida process, called a Shepherd’s fracture, from os trigonum syndrome can be a diagnostic dilemma because both can present acutely after an injury involving extreme ankle plantar flexion.2 Posterior ankle impingement is also associated with a thickened posterior intermalleolar ligament and stenosing tenosynovitis of the flexor hallucis longus. The posterior intermalleolar ligament (IML) has been implicated as a cause of posterior ankle impingement, but details of the role of this ligament in impingement are not fully understood. Found in up to 56% of the population, the IML is located between the posterior tibiofibular and the posterior talofibular ligaments (Figure 3).6 Some consider the IML to be an extension of the posterior talofibular ligament. A similar ligament is found in primate ankles, so the IML is also referred to as the tibial slip of the posterior talofibular ligament and the marsupial meniscus. Intermalleolar ligament tears or entrapment can also cause posterior ankle impingement symptoms.8,9 The relationship of posterior impingement and tenosynovitis of the flexor hallucis longus is unclear. At the posterior ankle, the flexor hallucis longus tendon travels within the sulcus between the medial and lateral tubercles of the talar posterior process, a region where direct compression by the os trigonum may exist.10 However, flexor hallucis longus tenosynovitis is common in ballet dancers with or without posterior ankle impingement.10 Also, although tenosynovitis of the flexor hallucis longus can be seen in up to 68% of patients with posterior 2 Figure 2: Superior view volumerendered 3-dimensional computed tomography scan of the talus with an os trigonum (black asterisk) showing the anatomy of the posterior process. Synchondrosis between the posterior process and os trigonum (white arrow), the groove for the flexor hallucis longus tendon (white asterisk), and the medial tubercle of the posterior process (arrowhead) are shown. ankle impingement, a causal relationship has yet to be established.2,7,10 Although not included in os trigonum syndrome due to the acute presentation, acute chondro-osseous disruption can occur as a result of impaction during plantarflexion or the ossicle can be avulsed due to tension at the insertion of the posterior talofibular ligament while in dorsiflexion.2 Interestingly, those who present with acute posterior ankle impingement symptoms tend to be nonathletes, suggesting that the mechanism is acute disruption of the synchondrosis or osseous contusion rather than chronic repetitive motion. Clinical Presentation Os trigonum syndrome classically presents as chronic posterior ankle pain, typically as a result of an overuse syndrome.1 Ankle stiffness, lock- 3 Figure 3: Coronal proton-density magnetic resonance image of the left ankle of a 12-year-old boy showing the posterior intermalleolar ligament (arrowhead) as a thin fibrous band arising from the malleolar fossa of the fibula coursing between the posterior tibiofibular ligament (white arrow) and posterior talofibular ligament (black arrow), inserting on the posterior tibia. ing, and posterior soft tissue swelling are symptoms of os trigonum syndrome. Physical examination reveals posterior ankle tenderness and soft tissue fullness anterior to the Achilles tendon. Ankle pain can be exacerbated by forced plantar flexion or push-off maneuvers, such as those that occur during dancing, running downhill, or kicking.1,2 The ankle may be inverted to prevent the impingement symptoms, frequently resulting in recurrent ankle sprains.7 Although symptoms are often relieved with rest, pain frequently recurs with return to activity.6 Posterior ankle pain can be complex, with a differential diagnosis that includes Achilles pathology, retrocalcaneal bursitis, flexor hallucis longus and peroneus JANUARY 2013 | Volume 36 • Number 165 n radiologic case study 4A 4B 4C Figure 4: Lateral radiograph of the left ankle of a 12-year-old girl with a great toe fracture (not shown) with incidental note of multipartite or immature Stieda process (white arrow) posterior to the talus (A). Lateral radiograph of the left ankle of a 24-year-old man with a similar fragmented appearance of the Stieda process (white arrow) (B). Sagittal computed tomography scan of the same ankle in 4B confirming an acute fracture (white arrow) of the Stieda process (C). 5A 5B 5C Figure 5: Lateral radiograph of the left ankle of a 49-year-old man with hindfoot pain showing sclerosis and subcortical cystic change (arrow) at the synchondrosis of the os trigonum (A). Sagittal computed tomography scan of the ankle/ hindfoot showing degenerative arthropathy and subluxation (white arrow) of the posterior subtalar joint. A secondary abnormal articulation is shown between the os trigonum and the posterior subtalar facet of the calcaneus. Computed tomography confirms degenerated synchondrosis (black arrow) of os trigonum (B). Oblique axial computed tomography scan of the ankle showing flexor hallucis tenosynovitis (white arrow) with fluid and inflammation around the tendon (C). pathology, degenerative and inflammatory arthropathies of the ankle and hindfoot, ankle instability, tarsal tunnel syndrome, talar osteochondral lesions, Haglund syndrome, coalition, and, in the pediatric population, Sever’s disease.3 Radiology Radiography Radiography is the imaging of choice for the initial radiologic evaluation of ankle pain. Unfortunately, findings of posterior ankle impingement can be nonspecific or inconclusive on radiographs. The presence 66 of an os trigonum is not diagnostic of posterior ankle impingement because up to 14% of people without posterior ankle symptoms have an os trigonum.1 Although an os trigonum larger than 1 cm has been associated with os trigonum syndrome, size does not correlate with symptoms.2 Fracture and fragmentation of the os trigonum are also difficult to distinguish from a normal multipartite ossicle on radiographs (Figure 4).3 Degeneration of the synchondrosis is characterized by an irregular, sclerotic, or cystic articulation (Figure 5).1,2 Dynamic fluoroscopic evaluation or static lateral radiographs of the ankle in plantarflexion may show osseous impingement, whereas contrast intravasation at the synchondrosis during ankle arthrography confirms disruption.1,5,7 Although potentially contributory, none of the associated anatomic variations provide a definitive diagnosis. In a review by Peace et al,6 a prominent superior calcaneal tuberosity was present in 64% of cases of clinical os trigonum syndrome. A prominent superior calcaneal tuberosity is defined as any osseous prominence of the posterior superior calcaneus extending above the superior parallel calcaneal pitch line, which is a line drawn from the posterior superior edge of the posterior subtalar calcaneal facet parallel to the calcaneal plantar cortex (Figure 6). Furthermore, a prominent downward sloping posterior tibia was seen in 25% of cases in the same study.6 A downward slope is defined as a posterior malleolus extending beyond 5 mm distal to a line drawn tangentially along the anterior tibial plafond on lateral views and parallel to the physeal scar.6 Scintigraphy Bone scintigraphy is nonspecific and not commonly performed for the diagnosis of an os trigonum. Furthermore, poor spatial resolution makes localization of uptake in relatively small structures such as the os trigonum difficult. However, a negative study confidently rules out the syndrome.5,7 On positive studies, a 3-phase bone scan shows increased blood flow and increased uptake of radiotracer in the symptomatic os trigonum. Single-photon emission computed tomography can also be used to localize uptake and differentiate posterior ankle impingement from other nearby abnormalities of the ankle, such as subtalar osteoarthritis.2,3,5,6 Ultrasound Ultrasound can show nodular capsular thickening at the posterior ankle or lateral to the ORTHOPEDICS | Healio.com/Orthopedics n radiologic case study 6A os trigonum. Doppler interrogation is typically negative. However, ultrasound is most useful for image guidance during diagnostic or therapeutic injection, allowing precise anatomical administration of anesthetics or steroids (Figure 7).1,5,11 Computed Tomography Computed tomography imaging mirrors radiographic findings but provides better anatomic and soft tissue detail. Computed tomography may better demonstrate degenerative synchondrosis, fragmentation, or fractures of involved osseous structures, osseous pressure erosions, and soft tissue infiltration (Figures 4, 5).1 Computed tomography can play a role in presurgical planning. Magnetic Resonance Imaging Magnetic resonance imaging (MRI) is the imaging mo- 7 6B Figure 6: Lateral ankle radiograph of the left ankle a 35-year-old man with chronic posterior ankle pain exacerbated by plantar flexion showing os trigonum (asterisk) and soft tissue attenuation in Kaeger’s fat pad (black arrow). An osseous prominence (white arrow) of the posterior superior calcaneus extending superior to the upper parallel pitch line (top white line) represents a prominent superior calcaneal tubercle (A). T2-weighted fat saturated magnetic resonance imaging showing bone marrow edema of os trigonum (asterisk) and opposing calcaneus (block arrow) with increased signal. Note joint effusions in the posterior recess of the ankle joint. Subtle intermediate soft tissue signal linear filling defects within the joint effusion represent synovial hypertrophy is shown. Infiltrative high T2 signal in Kaeger’s fat pad represents additional inflammation (B). dality of choice for the diagnosis and evaluation of an os trigonum. Pain usually occurs after development of soft tissue inflammation and synovitis of the posterior ankle and posterior subtalar joints (Figure 6), and synovitis has been reported in up to 100% of posterior impingement cases.1,6 Synovitis and inflammation are characterized on MRI as increased T2 signal in soft tissues with capsular and synovial thickening. The normally high T1 signal in Kager’s fat pad and the adjacent lipomatous tissue is decreased when inflamed. In the presence of a joint effusion, intermediate T2 signal intraarticular soft tissue filling defects indicate synovial proliferation. Imaging the ankle while in plantarflexion may demonstrate the entrapment of soft tissues. Opposing posterior ankle osseous structures may have Figure 7: Longitudinal ultrasound image of the ankle obtained during guided injection of os trigonum in a 28-year-old man with posterior ankle impingement. Notice the needle (arrows), os trigonum (asterisk), and calcaneus (C). patchy areas of increased T2 and decreased T1 signal due to bone marrow edema. This is most common in the os trigonum, but the posterior tibia, talar posterior process, and calcaneus can also be involved (Figure 6).1,5,6 Hyperintense fluid at the synchondrosis of the os trigonum on T2weighted images indicates disruption.1,2,5 Areas of bone sclerosis are hypointense on all sequences. Chronic disruption of the synchondrosis is characterized by sclerosis and cystic change (Figure 8). With regard to other pathologies seen with posterior impingement, the flexor hallucis longus tendon and sheath should be inspected on MRI. The flexor hallucis longus tendon sheath normally communicates with the subtalar joint and the flexor digitorum longus tendon sheath.1 Also, the flexor hallucis longus tendon sheath communicates with the ankle in 20% of normal patients.10 Therefore, fluid within the flexor hallucis longus tendon sheath can be physiologic. However, fluid in the tendon sheath out of proportion to ankle or subtalar joint effusion is suspicious for tenosynovitis.10,12 Septations within the distended tendon sheath also suggest tenosynovitis. Occasionally, edema is seen at the distal flexor hallucis longus myotendinous junction. This may be secondary to impingement of this region with dorsiflexion (Figure 5).6 Although the posterior IML was identified in 56% of dissected cadaveric ankles, Rosenberg et al8 detected the IML in only 19% of 97 ankle MRI examinations. It is thought that an IML 1 to 8 mm wide may be too small for the spatial resolution of MRI. Therefore, this ligament is not routinely inspected. However, easy identification of this ligament is potentially pathologic. In the same study by Rosenberg et al,8 the IML was found to be thickened in up to half of patients with an os trigonum.8 Treatment Os trigonum syndrome is initially treated conservatively with rest, activity modification, nonsteroidal anti- JANUARY 2013 | Volume 36 • Number 167 n radiologic case study syndromes of the ankle: role of imaging in diagnosis and management. Radiographics. 2002; 22(6):1457-1469. 6. Peace KAL, Hilier JC, Hulme A, Healy JC. MRI Features of posterior ankle impingement syndrome in ballet dancers: a review of 25 cases. Clin Radiol. 2004; 59(11):1025-1033. 8A 8B 8C Figure 8: Axial T2-weighted magnetic resonance image of the ankle of a 13-year-old boy with acute posterolateral ankle pain showing bone marrow edema at the posterior talus and within the os trigonum (black arrow). Note the posterior talofibular ligament (white arrow) inserting at the lateral facet of the os trigonum (A). Sagittal proton-density magnetic resonance image showing disruption (black arrow) of synchondrosis (B). Sagittal fat-saturated T2-weighted magnetic resonance image showing the opposing bone marrow edema at synchondrosis (white arrow). inflammatory drugs, and physical therapy.7 Immobilization may be initiated in severe cases. Ultrasound-guided injections play diagnostic and therapeutic roles in patients with posterior ankle impingement.1 Although variable responses to steroid and anesthetic injection have been reported, Robinson and Bollen11 reported a series of 10 patients who had immediate symptom relief after ultrasound-guided injections. When conservative treatment fails, posterolateral arthroscopic resection with or without capsulectomy or debridement of the os trigonum4,7,13 or resection of a torn IML1 may result in improved symptoms. Arthroscopy is less aggressive than open surgery and offers the added advan- 68 tage of less patient morbidity and less postoperative pain to allow for early functional rehabilitation. This is an uncommonly performed surgery. Conclusion Os trigonum syndrome is the result of impingement of posterior ankle structures, most notably the os trigonum. The evaluation of posterior ankle pain can be complex and has a lengthy differential diagnosis. Radiographic findings can suggest the diagnosis, but the mainstay of imaging evaluation is MRI. Detection of bone marrow edema in opposing posterior ankle osseous and soft tissue structures differentiates an inconsequential os trigonum from one causing posterior ankle impingement. In addition, superior soft tissue evaluation by MRI allows identification of associated findings, including synovitis, soft tissue inflammation, tenosynovitis of the flexor hallucis longus, and IML pathology. References 1.Donovan A, Rosenberg ZS. MRI of ankle and lateral hindfoot impingement syndromes. AJR Am J Roentgenol. 2010; 195(3):595-604. 2. Karasick D, Schweitzer ME. The os trigonum syndrome: imaging features. AJR Am J Roentgenol. 1996; 166(1):125129. 3. Bureau NJ, Cardinal E, Hobden R, Aubin B. Posterior ankle impingement syndrome: MR imaging findings in seven patients. Radiol. 2000; 215(2):497-503. 4. Abramowitz Y, Wollstein R, Barzilay Y, et al. Outcome of resection of a symptomatic os trigonum. J Bone Joint Surg Am. 2003;85(6):1051-1057. 5. Robinson P, White LM. Softtissue and osseous impingement 7. Wukich DK, Tuason DA. Diagnosis and treatment of chronic ankle pain. J Bone Joint Surg Am. 2010; 92(10):20022016. 8. Rosenberg ZS, Cheung YY, Beltran J, Sheskier S, Leong M, Jahss M. Posterior intermalleolar ligament of the ankle: normal anatomy and MR imaging features. AJR Am J Roentgenol. 1995; 165(2):387-390. 9. Fiorella D, Helms CA, Nunley JA II. The MR imaging features of the posterior intermalleolar ligament in patients with posterior impingement syndrome of the ankle. Skeletal Radiol. 1999; 28(10):573-576. 10. Lo LD, Schweitzer MR, Fan JK, Wapner KL, Hecht PJ. MR imaging findings of entrapment of the flexor hallucis longus tendon. AJR Am J Roentgenol. 2001; 176(5):1145-1148. 11. Robinson P, Bollen SR. Posterior ankle impingement in professional soccer players: effectiveness of sonographically guided therapy.” AJR Am J Roentgenol. 2006; 187(1):W53-W58. 12. Rosenberg ZS, Beltran J, Bencardino JT. From the (Wukich DK, 2010) RSNA refresher courses. Radiological Society of North America. MR imaging of the ankle and foot. Radiographics. 2000; 20:S153-S179. 13. Nickisch F, Barg A, Saltzman CL, et al. Postoperative complications of posterior ankle and hindfoot arthroscopy. J Bone Joint Surg Am. 2012; 94(5):439-446. ORTHOPEDICS | Healio.com/Orthopedics