Koulia K, Tsavari A, Myoteri D, Zisi A, Skafida E, Grammatoglou X

Koulia K, Tsavari A, Myoteri D, Zisi A, Skafida E, Grammatoglou X,
Vasilakaki T. Ceruminous gland adenoma of the external auditory canal: A case report. OA Case Reports 2013 Jun 21;2(5):45.
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Ceruminous gland adenoma of the external auditory canal: A case report
K Koulia
1
, A Tsavari
1
, D Myoteri
1
, A Zisi
2
, E Skafida
1
, X Grammatoglou
1
, T
Vasilakaki
1
1
Department of pathology “Tzaneion” General Hospital of Piraeus, Greece
2
Department of chemistry, University of Athens “Kapodistriako”, Greece
Corresponding author: Evangelia Skafida e-mail : evelinaskafida@yahoo.gr
Abstract
Ceruminous gland adenoma is a very rare bening neoplasm of the external auditory canal. This tumour composed of the ceruminous gland cell (modified apocrine sweat glands). We report a case of a 39 year old man who presented with signs of scratching at the left ear. Otoscopic examination revealed an exophytic skin covered smooth nodule 1,2 cm in greatest dimension on the posterior wall of the external auditory canal. Local wide resection of the lesion was performed. Microscopically the lesion composed of oxyphil glands and small cysts in a hyalinized stroma. The glandular epithelium was bilayered. In the immunohistochemical study the luminal cells were strongly positive with CK7 while the basal cells were highlighted with
CK5/6, p63 and S100 protein. The diagnosis was ceruminous gland adenoma. Three years later there was no evidence of recurrence. Complete surgical excision is therefore the treatment of choise.
Key words : Ceruminous adenoma, Ear canal, Sweat gland, Immunohistochemistry
Introduction
Ceruminous adenoma is a rare neoplasm of the external auditory canal with benign clinical behavior. Tumour arising from ceruminous glands. These are modified apocrine glands found in the external ear canal that produce a brown waxy material
[1,2,3,4]. Ceruminous glands demonstrate a dual cell population of basal myoepithelial cells and luminal secretory cells. These glands are localized deep in the skin mostly in the cartilaginous part of the external auditory canal. Less than 150 cases have been reported to date. [1,5]
Case report
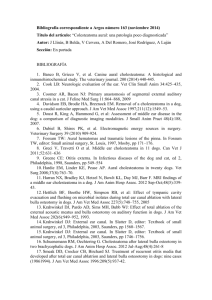
We report a case of a 39 year old man who came to our hospital with signs of scratching at the left ear. Otoscopic examination of the ear canal revealed an exophytic skin covered smooth nodule 1,2 cm in greatest dimension with broad base on the posterior wall of the external auditory canal. A wide local resection of the lesion was performed. Microscopically the lesion composed of oxyphil glands and small cysts. A hyalinized stroma created an infiltrative pattern of growth. The glandular epithelium was bilayered. The inner luminal secretory cells had apocrine decapitation secretions and abundant granular eosinophilic cytoplasm. There was no pleomorphism and a lack of necrosis. Overlying epidermis involvement was not seen
(fig. 1,2). In the immunohistochemical study the luminal cells were strongly positive with CK7 while the basal cells were highlighted with CK5/6, p63 and S100 protein
(fig. 3,4). Based on the above characteristic morphologic and immunohistochemical finding a diagnosis of ceruminous gland adenoma was made. Three years later there was no evidence of recurrence.
Discussion
External ear benign neoplasms derived from ceruminous glands are very rare. Most of these tumours are small and they are separated histologically into three types: 1) ceruminous adenoma, 2) ceruminous pleomorphic adenoma and 3) ceruminous syringocystadenoma papilliferum. The latter two are exceedingly uncommon.[6,7,8,9]
Ceruminous adenoma accounts for < 1% of all external ear tumours and occur with equal frequency in men and women usually affecting middle aged. Only two pediatric cases have been reported [5]. The symptoms of this lesion are unilateral hearing loss, pain, otorrhea and head shaking. These tumours tend to be well circumscribed but not encapsulated [1, 2, 3, 4,10]. Complete surgical excision with adequate margins of the normal tissue will be curative with incomplete excision associated with an increased risk of recurrence. The prognosis of these tumours is good [1, 2, 10,
11].
References
1) Rancic D., Zivic M., IIic I.,Katic V.,Radovanovc Z.: Clinical,histological and immunohistochemical features of ceruminous adenoma. AO Yu / Archlve
2007, Vol 15 no 3-4
2) Namyslowski G., Sciersky W., Misiolek M., Czeclor E., Lange D.: Ceruminous gland adenoma of the external auditory canal: a case report. Otolaryngol Pol
2003, 57 (5): 755-9
3) Thomson LD., Nelson BL., Barnes EL.: Ceruminous adenomas: a clinicopathologic study of 41 cases with a review of the literature. Am. J. Surg.
Pathol. 2004, 28(3): 308-18
4) Hicks GW.: Tumors arising from the glandular structures of the external auditory canal. Laryngoscope 1983, 93 (3): 326-40
5) Magliulo G., Bertin S.: Adenoma of the ceruminous gland. Otolaryngology
Head and Neck Surgery 2010, 143: 459-460
6) Markou K., Karasmanis I., Vlachtsis K., Petridis D., Nikolaou A., Vital V.:
Primary pheomorphic adenoma of the external ear canal. Report of a case and literature review. Am. J. Otolaryngol. 2008, 29(2): 142-6
7) Tsukahara K.,Suzuki M.,Tokashiki R., Motohashi R., Iwaya K.: Pheomorphic adenoma of the external auditory canal complicated by hearing loss secondary to chronic otitis media. Auris Nasus Larynx 2006, 33 (2): 183-6
8) Lee CK., Jang KT., Cho YS.: Tubular apocrine adenoma with syringocystadenoma papilliferum arising from the external auditory canal. J.
Laryngol. Otol. 2005, 119(12): 1004-6
9) Baldus SE., Streppel M., Slennert E., Dienes HP.: Pleomorphic adenoma of the external auditory canal. Differential diagnosis of the tumours of the ceruminous glands. Pathologe 1999, 20(2): 125-9
10) Lynde CW., McLean DI., Wood WS.: Tumors of ceruminous glands. J. Am.
Acad. Dermatol. 1984, 11(5): 841-7
11) Schenk, Handisurya A., Steurer M. Ultrastructural morphology of a middle ear ceruminoma. ORL J. Otorhinolaryngol Relet Spec. 2002, 64(5): 358-63
Legends
Figure 1
Ceruminous adenoma H-
Ε ×100
Figure 2
Ceruminous adenoma H-E ×200
Figure 3
The luminal cells were strongly immunoreactive with CK7 ( ×200)
Figure 4
Myoepithelial cell layer positive staining with CK5/6 ( ×200)
Fig.1 Ceruminous adenoma H-
Ε ×100
Fig.2 Ceruminous adenoma H-E ×200
Fig.3 The luminal cells were strongly immunoreactive with CK7 ( ×200)
Fig.4 Myoepithelial cell layer positive staining with CK5/6 ( ×200)