Ceruminous Gland Adenocarcinoma of External Ear Canal
advertisement

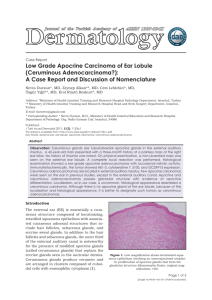
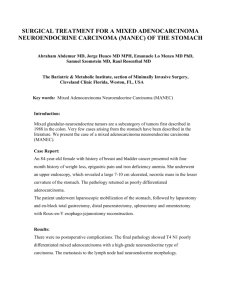
The Korean Journal of Pathology 2007; 41: 66-8 Ceruminous Gland Adenocarcinoma of External Ear Canal - A Case Report - Ceruminomas are rare tumors arising from the ceruminous gland, which is a modified apocrine gland in the skin of the external ear canal. There is controversy about these rare tumors regarding their histological classification, their origin and the importance of wide excision, and Department of Pathology, Hangang there is also terminological confusion for making the diagnosis. Ceruminous adenocarcinoSacred Heart Hospital, Hallym University, ma is a malignant subtype of ceruminoma. We report here on a case of adenocarcinoma of Seoul, Korea the ceruminous gland in a 71-year-old male patient. Jung Weon Shim Received : January 11, 2007 Accepted : January 17, 2007 Corresponding Author Jung-Weon Shim, M.D. Department of Pathology, Hangang Sacred Heart Hospital, 94-200 Yungdungpo-dong, Youngdeungpo-gu, Seoul 150-037, Korea Tel: 02-2639-5571 Fax: 02-2637-9352 E-mail: modshim@chol.net Key Words : Ear canal; Ear neoplasms pying the left EAC with involvement of the tympanic membrane and middle ear; it was infiltrating into the skin of the ear canal, and eroding into the regional bony tissue (Fig. 1). The patient underwent open cavity mastoidectomy and tympanoplasty of the left ear. The operation finding showed that the tumor was located at the intersection between the osseous and cartilaginous portions of the ear canal, filling approximately twothirds of the external ear and mastoid cavity. The tumor showed abundant feeding vessels growing into the regional dura and brain. Total excision of the soft portion within the tumor was done together with meatoplasty and reconstruction with using a free skin graft. The patient’s facial palsy persisted after the operation. Three months later, the tumor seemed to have invaded into the brain base. The excised tumor specimen was 1.5×1×1 cm in dimension. The cut surface of the mass showed a yellow white solid appearance with focal ulceration. Histologically, the tumor consisted of tubular or glandular lesion that was lined by stratified or single-layered tumor cells (Fig. 2). These cells showed abundant, granular, eosinophilic cytoplasm, and frequent apical snouts or blebs, indicating the decapitation-type secretion, being consistent with cells of apocrine derivation (Fig. 3). There was mod- The external ear canal (EAC) is divided into two sections: the inner two thirds are osseous, whereas the outer third is cartilaginous. The skin of the bony portion contains few appendages, and the skin of the cartilaginous portion shows numerous hair follicles, sebaceous glands and a specialized type of apocrine sweat glands: ceruminous gland. The eccrine sweat glands are absent in the EAC. Ceruminous gland tumors are rare, and only about 100 cases have been reported to date in the English literature.1 Several controversial issues such as nomenclature, classification, histogenesis and diagnosis remain. CASE REPORT A 71-year-old man presented with a 1-year history of otalgia and otorrhea in the left ear. He also complained of left facial weakness, intermittent dizziness and hearing problems; the rest of his medical history was unremarkable. The physical examination and otoscopy showed an exophytic, 2 cm sized mass that fulfilled the anterior part of the left EAC. The patient’s oral cavity, oropharynx, larynx, neck and thyroid examinations were normal. An MRI scan of the temporal bone showed a mass occu66 Ceruminous gland Adenocarcinoma of External Ear Canal 67 Fig. 2. Adenocarcinoma of ceruminous gland shows proliferation of tubular or glandular lesion (H&E, ×200). Fig. 1. An MRI scan shows a mass in the left external ear canal with destruction of regional bone tissue. Fig. 4. Adenocarcinoma destroys the regional bone tissue (H&E, ×200). Fig. 3. There is frequent snouting of the tumor cell cytoplasm into the lumen, being consistent with apocrine differentiation (H&E, ×400). erate nuclear pleomorphism and occasional mitoses, in keeping with adenocarcinoma. There were few myoepithelial cells, as was proved by perfoming immunohistochemistry for S-100 protein and smooth muscle actin. The surrounding tissue was desmoplastic with mixed acute and chronic inflammation. The tumor infiltrated into and destroyed the regional bone tissue (Fig. 4). DISCUSSION The term ‘‘ceruminoma’’ has long been used as a collective denomination for all ceruminous gland tumors. Such nomencla- ture has caused confusion regarding differentiating between a lesion’s benign and malignant nature. So, the term ‘ceruminoma’ was excluded from the WHO classification in 1991,2 but unfortunately, it is still being employed until now. Wetli et al.3 distinguished four categories for ceruminomas: the ceruminous adenoma, the ceruminous adenoid-cystic carcinoma, the ceruminous adenocarcinoma and the pleomorphic adenoma. In 1977, Pulec4 described two cases of a fifth entity: the mucoepidermoid carcinoma. A large cohort study on ‘ceruminoma’ has not yet been done and the only reported incidence of ceruminous adenocarcinoma arising out of ceruminoma was 9 out of 52 cases.3 The criteria for making the diagnosis of malignancy may be 1) cytologically bland features with an infiltrating margin or 2) the tumor has obviously malignant cytological features, such as significant nuclear pleomorphism, or a brisk mitotic rate.5 Ceruminous adenocarcinoma can be classified as a low or high grade adenocarcinoma depending on the degree of 68 atypia.6 The histology of ceruminous adenocarcinoma usually shows irregular glandular structures lined by cuboidal epithelium, and this epithelium shows apocrine features such as luminal blebbing or snouting.6 Adenoid cystic carcinoma could be differentiated from adenocarcinoma in that the former type shows cords and islands of uniform, rounded, darkly-staining cells that show pseudoglandular formation, but there is no peripheral palisading or evidence of true gland formation and there is a characteristic cribriform architecture and perineural invasion.6 It is clinically important to differentiate low-grade adenocarcinoma from a ceruminous adenoma. A sufficient tissue sample should be analyzed for the findings of stromal or bone invasion and desmoplasia in benign looking ceruminomas. Highgrade adenocarcinomas extensively infiltrate the surrounding tissues as irregular glands and sheets of overtly malignant cells. They show marked nuclear pleomorphism and abundant mitotic figures, and they may exhibit little or no evidence of apocrine derivation.7 In this case, tubular or glandular lesion with moderate cytological atypia, and invasive growth into the regional bone tissue matched the criteria of adenocarcinoma. The tumor cells frequently showed abundant eosinophilic cytoplasm and intraluminal decapitation that fit with a ceruminous gland origin. Ceruminous adenocarcinoma exhibits a prolonged subclinical phase, often lasting for years before presentation,8 as happened in our case. The clinical symptoms usually comprise a sensation of blockage in the EAC with or without hearing loss. Otoscopic examination usually demonstrates nodules covered by normal skin, with or without otorrhea, hemorrhage, lymphadenopathy or cranial nerve palsies. In contrast, ceruminous and pleomorphic adenomas present as painless nodules with or without hearing loss. Temporal bone CT scan or MRI is usually recommended to determine the extent of the lesion and the presence of osseous invasion, and to exclude extrapetrosal disease or metastasis.5 If the histopathologic analysis does not confirm a tumor’s benign nature, then the diagnosis, based on a large amount of tissue, should be reanalyzed and en bloc excision with resection Jung Weon Shim margins of 3 to 4 mm should be performed because the exact nature of the tumor is hardly identifiable at the time of surgery. Further, even benign and well-limited tumors, such as ceruminous adenomas have a high recurrence rate. Thompson et al.9 reported 4 out of 41 cerumious adenoma developed the recurrence due to incomplete excision. In Korea, one cerumious adenocarcinoma has been recently reported on. REFERENCES 1. Soon SL, Bullock M, Prince ME. Ceruminous adenocarcinoma: a rare tumor of the external auditory canal. J Otolaryngol 2001; 30: 373-7. 2. Lassaletta L, Patron M, Oloriz J, Perez R, Gavilan J. Avoiding misdiagnosis in ceruminous gland tumours. Auris Nasus Larynx 2003; 30: 287-90. 3. Wetli CV, Pardo V, Millard M, Gerston K. Tumors of ceruminous glands. Cancer 1972; 29: 1169-78. 4. Pulec JL. Glandular tumors of the external auditory canal. Laryngoscope 1977; 87: 1601-12. 5. Iqbal A, Newman P. Ceruminous gland neoplasia. Br J Plast Surg 1998; 51: 317-20. 6. Mills RG, Douglas-Jones T, Williams RG. ‘Ceruminoma’--a defunct diagnosis. J Laryngol Otol 1995; 109: 180-8. 7. Dehner LP, Chen KT. Primary tumors of the external and middle ear. Benign and malignant glandular neoplasms. Arch Otolaryngol 1980; 106: 13-9. 8. Garin P, Degols JC, Delos M, Marbaix E. Benign ceruminous tumours of the external ear canal. J Otolaryngol 1999; 28: 99-101. 9. Thompson LD, Nelson BL, Barnes EL. Ceruminous adenomas: a clinicopathologic study of 41 cases with a review of the literature. Am J Surg Pathol 2004; 28: 308-18. 10. Kwon YH, Choi JH, Kim HJ, Jung HH. A Case of Ceruminous Adenocarcinoma arising from the external auditory canal. Korean J Otolaryngol-Head Neck Surg 2004; 47: 1311-4.