The Retroperitoneoscopic Repair of a Lumbar Hernia of
advertisement

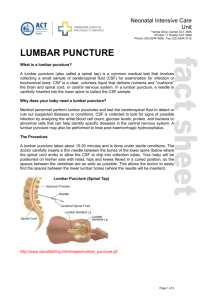
Acta chir belg, 2004, 104, 330-334 The Retroperitoneoscopic Repair of a Lumbar Hernia of Petit Case report and Review of Literature A. Grauls*, B. Lallemand*, M. Krick** Department of Surgery, St Joseph Hospital*, Liège and O.L.V. Hospital**, Asse, Belgium. Key words. Hernia ; Petit ; inferior lumbar triangle ; retroperitoneoscopy ; Marlex. Abstract. In this paper, we comment on a patient who consulted us because of his «lower backpain» together with the appearance of a small swelling at the left side. Anamnesis and clinical examination were suggestive and further simple diagnostic methods confirmed the exceptional diagnosis of a «lumbar hernia of Petit». We describe the retroperitoneoscopic approach of this hernia, its reduction and the fixation of a polypropylene mesh at the surrounding structures with a Tacker. This approach provided a good postoperative comfort, a shorter hospital stay and an early recovery of autonomy and activity. Furthermore, we give a review of the literature concerning lumbar hernias and the evolution of the different reconstruction techniques. Introduction With only 250 to 300 cases reported in the literature (13), lumbar hernias are rare defects that involve the extrusion of retroperitoneal fat or viscera through a weakness in the posterolateral abdominal wall (1). Within this region there are two anatomically defined weaker triangles, «the triangle of Petit» and «the triangle of Grynfelt-Lesshaft» (7-8). The “triangle of Petit” or “the inferior lumbar triangle” is an upright triangle bound by the crista ilica, the musculus obliquus externus and the musculus latissimus dorsi (Fig. 7 and Fig. 8). The superior lumbar triangle is an inverted triangle bordered by the 12th rib, the musculus serratus posterior inferior, the musculus quadratus lumborum, the musculus erector spinae and the musculus obliquus internus (1, 4-6, 8). The most common clinical sign presenting a lumbar hernia is a posterior protruding bulge found by the patient. It may be asymptomatic, associated with a sense of discomfort, or the cause of notable localized tenderness (1, 5-6). -We distinguish a reducible from a nonreducible hernia ; 25% of the spontaneous lumbar hernias have an incarcerated content, with an overall stangulation risk of 8% (1). Because lumbar hernias are rare, the differential diagnosis must be made with a lipoma, a soft tissue tumour, a haematoma, an abcess, an atheromatous cyst, a renal tumour, a panniculitis and a muscle hernia. Repairing these lumbar hernias is often difficult because of the weakness of the surrounding structures (1, 10-12). Many different «open» surgical techniques have been used to repair the defect and since several years the laparoscopic approach has been successful (13, 8, 10, 12). We repaired a lumbar hernia of Petit retroperitoneoscopically. Case Report A 49-year old man of Iraqui origin had a history of lower backpain of 3 days duration. The pain was localized on lumbar level, radiating to the left flank and increasing by lifting heavy objects. Herewith the patient felt a small swelling in the left flank, which was slightly painful at night when lying on that side. The patient reported that the soreness was accentuated with hard physical efforts. His medical history was notable for the resection of an atheromatous cyst of the back in 1996, acute backache treated with a support bandage in 1998, and the resection of an abscess of the back on 08-02-1999. The patient smoked one packet of cigarettes a day and he was obese. By clinical examination, we found a visible swelling in the left flank, at the triangle of Petit, with a diameter of 2.5 cm. By percussion, we found dullness over the swelling and palpation revealed a supple, well defined and reducible mass, increasing by Valsalva and reducing while lying down. In spite of a suggestive anamnesis and clinical examination, we made an ultrasound of the lumbar region, because of the rareness of lumbar hernias. This way we could differentiate the lumbar hernia from other pathologies. Excluding vertebral pathologies, we made X-rays of the lumbar and thoracic The Retroperitoneoscopic Repair Fig. 1 CT-scan with double contrast at the level of the triangle of Petit : visualization of a lumbar hernia, containing intraperitoneal fat (arrow). vertebrae, on which we could not visualize any relevant anomalies. We made a contrast CT-scan of the abdomen (Fig. 1), in order to visualize the contents of the hernial sack and the relation with the surrounding structures. A lumbar hernia, containing intraperitoneal fat, with a maximal diameter of 5 cm, was visualized at the level of the triangle of Petit. Under general anaesthesia we performed a retroperitoneoscopic repair of the defect, with a polypropylene Marlex prosthesis, one month after the first consultation. The patient was placed in a semilateral position, on his right side, which optimized exposure and allowed the viscera to fall away from the operative field (Fig. 2). A small incision was made under the tip of the 12th rib to accommodate a 12 mm distention balloon, placed into the retroperitoneal space. By insufflation, the retroperitoneal space could be dissected. The distention balloon was replaced by a 10 mm structural trocar, and with an extra 5 mm trocar near the 11th rib, the retroperitoneal dissection was continued towards the lateral border of the left rectus sheath. A 10 mm trocar was introduced at the umbilicus and a final 5 mm trocar at the left fossa iliaca (Fig. 3). The camera was displaced to the 10 mm trocar at the umbilicus. After dissection of the posterior part of the retroperitoneal space, the defect, with a maximal diameter of 5 cm, was visualized (Fig. 4). The hernia, containing intraperitoneal fat, was reduced and the borders of the opening were cleared. A 15 15 cm Marlex mesh was used to occlude the defect, and it was fixed with the Tacker at the crista iliaca, the musculus quadratus lumborum and the musculus transversus abdominis (Fig. 5). A redon drainage was placed. The postoperative sequelae were uneventful, and the patient was discharged on the 5th postoperative day. Six weeks later he could resume work, without any com- 331 Fig. 2 Position of the patient during the operation : the semilateral position, on the right side, optimized the exposure and allowed the viscera to fall away from the operative field. plaints. During 24 months of follow-up, neither recurrence of hernia nor any related complaints were recorded. Both the ultrasound examinations and the CT-scan, performed after 12 months (Fig. 6), were negative. Discussion Our patient had a reducible, non incarcerated lumbar hernia at the triangle of Petit. The ultrasound and the CT-scan could confirm the suggestive anamnesis and clinical examination. We successfully performed a retroperitoneoscopic repair of the defect, which provided good postoperative comfort, a short hospital stay and an early recovery of autonomy and daily activities. There are several classifications on lumbar hernias, made according to the origin, the anatomical localization and the contents of the hernia. We distinguish a congenital hernia from an acquired form, which can arise primary or secondary after surgery, infection or trauma. On localization we differentiate diffuse lumbar hernias from the hernias localized within the superior or inferior lumbar triangle. Furthermore, lumbar hernias differ from each other by the contents of its hernial sac (1, 8, 13). Because lumbar hernias seldom cause strangulation, the prognosis is often good. However, their volume increases progressively and they become more symptomatic. The larger the hernia, the more difficult the operation. That is why most of the hernias should be operated as soon as the diagnosis has been made (1-5). After the hernial sac and its contents are identified and reduced, the recontruction of the defect can be performed. This reconstruction is difficult because of the weakness of the surrounding tissues and because of the complicated anatomical boundaries (1, 8, 10-12). A preoperative CTscan should be made, with attention to the colon and the urinary tract (1, 4, 6-7, 9, 13). 332 Fig. 3 Position of the 4 trocars : 1 : at the tip of the 12th rib ; 2 : cranial and anterior from the 11th rib ; 3 : at the umbilicus ; 4 : at the left fossa iliaca. Fig. 4 Endoscopic visualization of the anatomical defect, bounded by the crista iliaca and the musculus quadratus lumborum. Over the years, several reconstruction techniques for lumbar hernias have been described. Primary closure has been tried, but was often inadequate for repair. Probably the most cited and certainly an adequate repair in most lumbar hernias is the classical reconstruction technique described by DOWD in 1907 (4, 8) (Fig. 9). DOWD turned up a flap from the fascia lata and the aponeurosis of the musculus gluteus maximus and sutured it to the lumbar fascia, the musculus obliquus externus and the musculus latissimus dorsi. WARBASSE modified DOWD technique by undercutting the transversalis so that it could be imbricated without tension (Fig. 10). RISHMILLER split the musculus latissimus dorsi and slid it over the defect as a flap. He reinforced the repair by approximating the musculus obliquus externus and the musculus latissimus dorsi (Fig. 11). Probably the first use of free fascial grafts in lumbar repair was made A. Grauls et al. Fig. 5 Endoscopic visualization of the Marlex mesh, fixed with the Tacker. Fig. 6 CT-scan at the level of the triangle of Petit, performed 12 months postoperatively : No recidive hernia can be detected. We notice the Tacker fixation points at the musculus quadratus lumborum (red arrow) and the musculus transverses abdominis (blue arrow) by RAVDIN in 1923. He closed the transversalis defect and reinforced it with a free fascia graft, taken from the fascia lata. In 1954, SWARTZ described the use of free fascia lata strips to approximate and close the defect in small and moderate-sized lumbar hernias (Fig. 12). KOONTZ described mobilization of massive flaps of fascia lata and lumbar fascia to reinforce massive defects (8). Because all these methods required large planes of dissection and had the potential disadvantage of creating flaps with compromised vascularization, the use of prosthetic meshes was introduced. But this technique also required a large incision, dissection and exploration (2, 4, 8, 13). The Retroperitoneoscopic Repair 333 Fig. 9 DOWD technique included mobilization of a flap of the musculus. gluteus maximus and the fascia lata, approximation of the musculus obliquus externus and the musculus latissimus dorsi and reinforcement with a facial flap from the musculus latissimus dorsi. Many subsequent techniques are modifications of this original procedure (8). Fig. 7 Inferior lumbar triangle : LD : musculus latissimus dorsi ; EO : musculus obliquus externus ; IC : crista iliaca ; GM : musculus gluteus maximus ; ILT : inferior lumbar triangle ; B : crosssectionpoint of Figure 8. Fig. 10 WARBASSE modified DOWD repair by imbricating the transversalis and covering the defect with a flap turned up from the fascia lata and the m. gluteus maximus (8). Fig. 8 Inferior lumbar triangle, section across point B of Figure 10 : Above : normal anatomy. Under : hernia. PS : musculus psoas ; QL : musculus quadratus lumborum ; SS : musculus sacrospinalis ; LDF : lumbodorsal fascia ; P : peritoneum ; TF : transversal fascia ; TA : musculus transversus abdominis ; IO : musculus obliquus internus ; EO : musculus obliquus externus ; LD : musculus latissimus dorsi ; HS : hernial sac. Fig. 11 RISHMILLER slid over a flap from the free border of the musculus latissimus dorsi and reinforced the repair by approximating the musculus latissimus dorsi and the musculus obliquus externus (8). 334 Since several years, lumbar hernias have been successfully repaired laparoscopically. This approach allows an exact visualization of the anatomical defect so that damage to boundary structures, such as the ureter and nerves, can be avoided. It is minimal invasive, with less postoperative pain, a minimal morbidity, a shortened hospital stay, better cosmetic results and minimal lifestyle intrusion (1-2, 4, 10-12). Since this transabdominal approach needs a strong transmuscular fixation of the intraabdominal mesh we looked for another approach, avoiding transmuscular stitches and direct contact between the mesh and the intraperitoneal content (1-2, 4). We used this retroperitoneoscopic technique without entering the peritoneal cavity, and we fixed a Marlex mesh with a Tacker, as seen in preperitoneal inguinal hernia repair. We could conclude that this technique is safely feasible, with an excellent postoperative result. Our patient had little or no pain and 24 months of follow-up could not reveal recurrence. References 1. HENIFORD B. T., IANNITTI D. A., GAGNER M. Laparascopic Inferior and Superior Lumbar Hernia Repair. Arch Surg, 1997, 132 : 11414. 2. BICKEL, HAJ M., EITAN A. Laparascopic Managment of Lumbar Hernia. Surg Endosc, 1997, 11 : 1129-31. A. Grauls et al. 3. SUTHERLAND R. S., GEROW R. R. Hernia after dorsal incision into the lumbar region. J Urol, 1995, 382-4. 4. ARCA et al. Laparascopy for lumbar hernia. J Am Coll Surg, 1998, 187 : 146-52. 5. HOROVITZ I. L., SCHWARZ H. A., DELAN A. A lumbar hernia presenting as an obstructing lesion of the colon. Dis Colon Rectum, 1986, 29 : 742-4. 6. WECHSLER R. J., KURTZ A. B., NEEDLEMAN L. et al. Cross-sectional Imaging of Abdominal Wall Hernias. Am J Roentgenol, 1989, 153 : 517-21. 7. BAKER M. E., WEINERTH J. L., ANDRIANI R. T., COHAN R. H., DUNNICK N. R.. Lumbar hernia diagnosis by CT. Am J Roentgenol, 1987, 148 : 565-7. 8. SWARTZ W. T. Lumbar Hernia. In : Hernia, 2nd ed., edited by L. M. NYHUS and R. E. CONDON, Philadelphia, pp. 409-26. 9. LIGHT H. G. Hernia of the Inferior Lumbar Space. A cause of back pain. ARCH SURG, 1983, 118 : 1077-80. 10. MORENO-EGEA A., AGUAYO J. L. Ambulatory laparoscopic repair of inferior lumbar or Petit hernia : a case report. Surg Endosc, 2002, 16 : 1107. 11. HABIB E., ELHADAD A. Retroperitoneoscopy in tension-free repair of lumbar hernia in adults. Ann Chir, 2001, 126 : 1016-8. 12. WOODWARD A. M., FLINT L. M., FERRARA J. J. Laparoscopic retroperitoneal repair of recurrent postoperative lumbar hernia. J Laparoendosc Adv Surg Tech, 1999, 9 : 181-6. 13. SHIIKI S., KUWATA Y., KASHIHARA E., UEDA U., FUCHIMOTO S., ORITA K. A case of Superior Lumbar hernia. Jpn J Surg, 1991, 21 : 696-9. 14. QUILICI P. J. Interventional Laparoscopy. In : The State of the Art for the New Millenium, 6th edition, year, 2002, online Laparoscopic Technical Manual. A. Grauls Staaien 20 B-3800 Sint-Truiden, Belgium