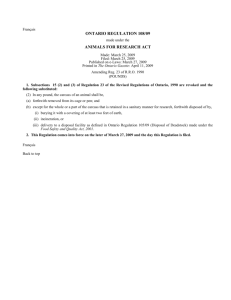
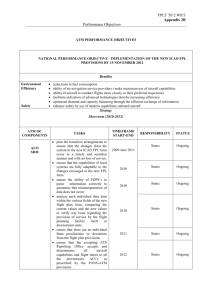
ASSIGNMENT COVER SHEET GRIFFITH AVIATION COURSE CODE 3515NSC COURSE NAME Safety Management ASSESSMENT ITEM NUMBER WRITTEN ASSIGNMENT (REVIEW) 1 ASSESSMENT TITLE A REVIEW OF THE SMS PROCESSES THAT COULD HAVE IDENTIFIED, AND POSSIBLY PREVENTED, THE F-28 ACCIDENT OF AIR ONTARIO DUE DATE 15th May 2015 STUDENT NAME REBECCA SPENCER STUDENT ID NUMBER S2942503 COURSE CONVENOR Peter Bryant WORD COUNT 1997 Self-Assessment Grading 5 1 Criteria 2 3 4 4 3 2 1 Assigned Total grade available Weighting % 4 /5 x 60 48 5 /5 x 15 15 4 /5 x 15 12 5 /5 x 10 10 TOTAL 85 GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 1 of 23 0.0 Executive Summary In March 1989, flight 1363 of Air Ontario crashed after take-off from Dryden Municipal Airport, Canada. This report aims to review the factors contributing to this preventable accident, relying mainly on the Honourable Virgil Moshansky’s report. After categorising key deficiencies of the air carrier into organisational, flight operations and maintenance, it was found that numerous latent conditions could have been rectified through a Safety Management System (SMS). Many of these conditions were found to be due to poor management throughout the organisation. By following the ICAO SMS Framework (Appendix A), this report considers the factors essential for identifying the latent conditions contributing to deficiencies. The processes which achieve these outcomes would have identified and possibly rectified the general failures leading towards the accident of flight 1363, had Air Ontario implemented an SMS. Through a top-down approach analysis, one sees that in order for Air Ontario to achieve their safety goals, the airline needed greater focus on their written safety policy and objectives, after defining implementation methods, with secured compliance. This report found that implementation of clear policies, ensuring standardisation and explicit documentation would have clarified the understanding of all involved in flight 1363. When making operational decisions under times of stress, maximum support is to be afforded to the flight crews. Through Hazard Identification (HID) processes and Internal Reporting Systems (IRS), Air Ontario would have identified deficiencies proactively, leaving time for active corrections to be made. These methods of Safety Risk Management (SRM) can assist in the assurance of safety for any organisation. GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 2 of 23 Table of Contents 0.0 Executive Summary ......................................................................................................... 2 0.1 List of Figures ....................................................................................................................... 5 0.2 Glossary ................................................................................................................................. 5 1.0 INTRODUCTION .................................................................................................................... 6 2.0 DEFICIENCIES WITHIN AIR ONTARIO ............................................................................... 7 GENERAL FAILURE TYPES ............................................................................................... 7 1. Communications .................................................................................................................. 7 2. Error / Violations ................................................................................................................ 7 3. Defences .............................................................................................................................. 7 4. Procedures and Policies ..................................................................................................... 8 5. Management ........................................................................................................................ 8 6. Organisation ........................................................................................................................ 8 3.0 SAFETY POLICY AND OBJECTIVES ................................................................................... 9 3.1 Appointment of Safety Roles and Accountabilities ........................................................ 9 3.2 Organisational Processes .............................................................................................. 10 3.2.1 3.3 Resource Allocation ............................................................................................... 10 Explicit Documentation .................................................................................................. 11 4.0 SAFETY RISK MANAGEMENT AND SAFETY ASSURANCE ........................................... 12 4.1 Internal Reporting System ......................................................................................... 12 4.2 Investigations and Documentation ............................................................................ 12 4.3 4.4 Defences to Accident Causation ................................................................................... 13 Management of Change ............................................................................................. 13 5.0 SAFETY PROMOTION ........................................................................................................ 14 5.1 5.1.2 6.0 Safety Culture ................................................................................................................ 14 Safety Culture Index .................................................................................................. 14 CONCLUSION ................................................................................................................. 15 7.0 REFERENCE LIST: .................................................................................................................. 16 GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 3 of 23 Appendix A – ICAO SMS Framework ....................................................................................... 18 Figure B – Air Ontario Inc. Flight Operations Organisation (March 1989) ............................ 19 Appendix C – Ideal Management Structure for a Safety-Conscious Organisation ................ 20 Appendix D – Effective Safety Reporting – Five Basic Characteristics ................................. 21 Appendix E – Accident Causation ............................................................................................. 22 Appendix F – CASA Safety Culture Index ......................................................................................... 23 GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 4 of 23 0.1 List of Figures 1 - ‘The Organisational Accident’ 2 – The Safety Space: Balance of the 2 P’s 3 – Levels of Efficiency for Hazard Intervention 0.2 Glossary ALARP As Low As Reasonably Possible APU Auxiliary Power Unit CASA Civil Aviation Safety Authority CRM Crew Resource Management HID Hazard Identification ICAO International Civil Aviation Organisation IRS Internal Reporting System MEL Minimum Equipment List SOC Systems Operational Control SMS Safety Management System SRM Safety Risk Management GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 5 of 23 1.0 INTRODUCTION This report reviews deficiencies noted in Air Ontario in the lead up to the accident of flight 1363. Though Canadian regulation did not require SMS implementation at the time, this report considers elements which would have identified key deficiencies, had an SMS been in place. Processes to achieve these elements are discussed, highlighting how they could have rectified the deficiencies and potentially prevented the avoidable accident of flight 1363. GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 6 of 23 2.0 DEFICIENCIES WITHIN AIR ONTARIO This report makes regular reference to the six groups of general failure types listed below, listing key deficiencies noted throughout Air Ontario. These issues have been numbered individually and are categorised further as organisational, flight operations or maintenance (represented by colour). GENERAL FAILURE TYPES 1. Communications 1.1 Lack of information exchange during and between flight operations 1.2.1 Use of sticky notes 1.2.2 Limited communication between cabin/flight crew and also with maintenance/ dispatchers 1.2 Pilots’ failure to report deficiencies/incidents leaving next crew in the unknown 1.3 Relied on “verbal interim” from Transport Canada as approval for MEL draft 1.3.1 Decisions based on assumption and second hand information 2. Error / Violations 2.1 Regulatory standards not abided to 2.2 Mishandling flight operations 2.3 Improper operational control of dispatch function and maintenance practices 2.4 Erroneous flight release 3. Defences 3.1 Did not employ pilots with previous experience on the F-28 or transport category jet aircraft 3.2 Failed to employ additional aircraft/crew as backup 3.3 Lack of resourcefulness (little involvement with Air Canada – the parent airline) 3.4 Limited training: 3.4.1 Ground-handling staff: lack of resources/facilities to support F-28 at Dryden 3.4.2 CRM: pilots not taught to share workload nor cross-check 3.4.2.1 Did not involve flight & cabin crew and maintenance & dispatchers 3.4.3 Flight attendants never received practical training for emergency procedures on F-28 3.4.4 Dispatchers lacked adequate job training and personnel qualification 3.4.5 SOC dispatch personnel did not appreciate importance of their function GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 7 of 23 4. Procedures and Policies 4.1 Maintenance problems noted in aircraft journey log continuously deferred, based on MEL 4.2 Pilots deferring maintenance, based on aircraft’s turn around period 4.3 Lack of airline’s own F-28 operations manual 4.4 Self-dispatch system, which lacked supervisions, developing into a hybrid system 4.5 Improper reporting and investigation systems 4.6 Safety operations procedures not written clearly for pilots 5. Management 5.1 Resource allocation balance of protection and production 5.1.2 No ground start facilities at Dryden to support the F-28 aircraft 5.2 Little commitment to and promotion of safety practices 5.3 Prioritising of key issues 5.3.1 Operational supervisors preoccupied with matters regarding labour relations 5.4 Managerial staff 5.4.1 Lacked experience (i.e. Tom Syme appointed director of maintenance but had no technical background or proficiency) 5.4.2 Numerous positions/roles appointed to individuals (e.g. Joseph Deluce concurrently held managerial roles as: F-28 chief pilot, chief instructor, check pilot and manager of Air Ontario F-28 program 6. Organisation 6.1 Policy making lack of standardisation 6.1.1 Prevention of pairing of two pilots with low experience 6.1.2 Lacking standardisation for training and competencies 6.2 Culture lacked safe practice emphasis 6.3 F-28 program needed greater project coordination 6.4 Absence of strong ‘interface’ with the regulator (Transport Canada) 6.5 Weak supervision procedures in place 6.5.1 Absence of monitoring for maintenance practices and competence 6.6 Delineated working conditions 6.6.1 Few interactions between top/middle management and staff 6.6.2 Weak relationship/support between management and staff 6.7 Prioritisation 6.7.1 Competition driven ‘jetitis’ 6.7.2 Management team assigned “low priority” over filling vacant safety positions 6.7.3 Rushed acquisition of the F-28 GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 8 of 23 3.0 SAFETY POLICY AND OBJECTIVES Figure 1 - ‘The Organisational Accident’ (Source: ICAO SMM, p 2-4). Safety improvements and identification of deficiencies must be completed simultaneously, in order to prevent accident causation. Risks arising from workplace or latent conditions can be mitigated via SRM and HID, which will be discussed in section 4.0. Figure 1 above emphasises monitoring of organisational processes, with methods to achieve this being outlined throughout the report. 3.1 Appointment of Safety Roles and Accountabilities The appointment of key safety roles is one of the first steps any safety-conscious organisation considers, showing commitment from top management and developing safety accountabilities (Appendix A). Though Air Ontario had a range of personnel appointed to organisational roles, no positions were safety specific1 (noted in Appendix B). Any successful SMS starts with top management and includes personnel on all levels, which is why each department must involve representatives with the ‘safety action group’ (refer to Appendix C for ideal structure). Had department representatives been involved in regular board meetings, this would have presented the opportunity for hazards to be addressed. 1- Captain Ronald Stewart was appointed as the safety officer, but this position was left vacant from 1987 until February 1989, leading into the F-28 accident. Furthermore, the management team “assigned a low priority” (p876) over filling this vacant position. GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 9 of 23 As this group includes representatives from senior management to staff, this generates clear communication throughout the entire organisation, also improving supervision. With a team solely responsible for safety, a board representing all departments can meet frequently for continuous monitoring and review of safety procedures. This proactive approach could have identified hazardous factors leading to general failures noted under: 1.1, 4.3, 4.4, 5.1 and all under category 6 (‘organisation’). 3.2 Organisational Processes Had safety management been a “core business function” (Bryant, 2015, Module 3) of Air Ontario, organisational processes would have achieved effective SMS through a topdown effect. This then affects the workplace conditions, influencing active failures (i.e. errors and violations) and addressing all deficiencies noted in Section 2.0. 3.2.1 Resource Allocation Lacking balance between resource input for protection and production causes deviations in an organisation’s safety space, as seen in Figure 2 below. Through IRS and continuous monitoring, management would have noted the need for greater resources for protection needs, maintaining appropriate balance of the “2 P’s” (Bryant, 2015, Module 3). For instance, had maintenance reported the lack of spares to supervisors, management could have sourced equipment necessary to enable aircraft operations (rectifying deficiencies 2.3, 2.4, 5.1, 6.5 and 6.7). Additionally, management should have seen the need for greater training, improving flight crew experience and the level of expertise among maintenance/dispatch personnel (addressing deficiencies 3.1, 3.3, 3.4, 5.4 and 6.1.2). A ‘bottom-up’ approach should have been employed, with improved training syllabuses eliminating latent conditions. GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 10 of 23 Figure 2 – The Safety Space: Balance of the 2 P’s (Source: ICAO SMM, p 2-14). 3.3 Explicit Documentation SMS must be explicit, ensuring all organisational activities are well documented and accessible. This is where the airline could have recorded (once creating) relevant flight operations manuals, training procedures and supervision reports. Explicit documentation improves communication across all departmental levels and achieves standardisation (through appropriate written policy). As seen in deficiencies 1.1 and 1.3, greater inter and intra correspondence was needed to avoid ambiguity. Improved communication alongside clear policy offers maximum support to flight crews when making difficult operational decisions, such as when operating with an unserviceable APU. With clear and accessible information, the following deficiencies would have been rectified: 2.1, 2.3, 3.3, 3.4, 4.3, 5.1, 5.3, 6.1 and 6.3. GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 11 of 23 4.0 SAFETY RISK MANAGEMENT AND SAFETY ASSURANCE 4.1 Internal Reporting System Strong HID processes, such as successful IRS, were needed throughout all levels of Air Ontario, identifying deficiencies noted under categories 1, 2 and 3 (Section 1.0). An effective IRS reflects organisations’ culture, with positive safety cultures eliminating reluctant attitudes towards honest and timely self-reporting, with emphasis placed on accountability and willingness (Appendix D). With an IRS identifying hazards, the airline could have become more proactive and taken corrective actions to eliminate their risks to at least a tolerable level. Additionally, Air Ontario could have adopted more in-depth pre-flight procedures, to account for unreported incidents in previous journey logs. 4.2 Investigations and Documentation Air Ontario needed to document safety risks and make the investigation accessible to relevant personnel via suitable collection/storage of incidents. As Air Ontario only investigated as a reactive response, risks developed without intervention. Greater use of a database alongside flight data analysis and continuous monitoring would have identified latent conditions actively, enabling corrective actions to minimise failures. Addressing deficiencies 1.1, 1.2 and 4.5, the monitoring of an investigation database can make an organisation predictive, becoming a highly efficient defence for SRM (Figure 3). Had Air Ontario been more predictive than reactive, the airline would have noted that two reported incidents before the Dryden crash showed commonalities with the serious F-28 accident. With similar adverse weather conditions, any pilot or supervisor should have foreseen the risk of continued flight operations in such circumstances, something which could have been easily prevented. GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 12 of 23 Figure 3 – Levels of Efficiency for Hazard Intervention (Source: Bryant, 2015, Module 3). 4.3 Defences to Accident Causation Proactively implementing effective defences (Appendix D) creates a safer operating environment. As noted in category 3 of general failures (‘defences’), it is evident that the airline failed to make proper use of all three intervention platforms, which would have rectified the following deficiencies: REGULATION 2.1, 2.2, 2.3 and 4.3 TRAINING 3.4 and 5.4 TECHNOLOGY 1.2.1 and 6.1 Despite emphasis for training improvement, many mistakenly place an over-reliance on training “as a means to improve safety” (Course notes, 2015), hence the need to combine training with safety practices under regulation and technology also. Continuous amendments to training and technology applications needed reference to previous experience/incidents, which standardisation (through policy making) and an investigation database would assist in. 4.4 Management of Change Air Ontario failed to see the importance of HID during their internal organisational changes, when introducing new equipment and management structure. These changes needed to be treated with their potential to introduce new hazards, hence why implementing the F-28 program during this time was risky and something to be avoided. SRM is associated with the apex of safety (Appendix A), highlighting that mitigation, alongside risk defences, can GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 13 of 23 “avoid, reduce [or] segregate” risks (Bryant, Module 5, 2015, p32), capturing deficiencies 3.3, 5.1, 5.3, 5.4, 6.3, 6.4 and 6.7. In terms of avoidance, the airline needed to rethink their operational priorities and resourcefulness, indicating the necessity for greater interface with the parent (and experienced) company. 5.0 SAFETY PROMOTION 5.1 Safety Culture Poor safety culture saw to violations, combined with error, leading to a disastrous outcome. Violations were executed by personnel on all levels (2.1), including a pilot of the Captain rank, showing poor role model qualities from the experienced. Poor practice was also seen in the cockpit, with flight crews responding to a cabin smoke problem by simply deactivating the smoke detector (2.2). Safety culture is paramount in creating an environment which encourages safe practices, such as cross-checks throughout all operations, to eliminate error to an ALARP level (6.1 and 6.2). Culture can be used to develop unquestionable standards of practice, making correct actions appear obvious to all personnel, guiding them to appropriate responses to hazards (Pidgeon, 1991). 5.1.2 Safety Culture Index Findings from the Moshansky Report have been used with CASA’s Safety Culture Index to determine that the airline had a ‘bureaucratic’ safety culture. With a safety score of 64 points (Appendix F), Air Ontario was below the minimum threshold for a positive safety culture, which requires a score of 93 (CASA, 2014). Air Ontario’s culture leading into the F28 accident saw to maintenance supervisors deferring problems, which had been logged by flight crew, due to aircrafts’ short turn around periods (2.3, 2.4, 4.1, 4.2, 5.3, 6.5 and 6.7). GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 14 of 23 6.0 CONCLUSION After reviewing the deficiencies noted through Air Ontario, it was found that most general failures occurred through management operations. Management, upon appointing key safety people to roles, needed to include safety representatives from all departments and clearly defined accountabilities. Further hazards would have been identified through an IRS and stronger investigations. These needed to be stored on a suitable database to be accessible by all relevant personnel. That would enable the air carrier to become predictive about flight operations. As well, improved resource allocation and training procedures are two processes which would have rectified many latent conditions. However, these decisions come down to the management team and policies of Air Ontario. GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 15 of 23 7.0 REFERENCE LIST: Bartsch, R. I. C. (2013). Aviation Law in Australia. Sydney, New South Wales, Australia: Thomson Reuters (Professional) Australia Limited Bryant, P. (2015). 3515NSC Safety Management Module 1: Course Introduction & Overview. Retrieved from Griffith University, School of Natural Sciences, Learning@Griffith website: https://bblearn.griffith.edu.au/bbcswebdav/pid-1211368-dt-content-rid3674264_1/courses/3515NSC_3151/Course%20Content/Module%201%20%20Course%20Introduction%20%26%20Overview%20ICAO%20SMS%20Template%20IC AO%20SMS%20Template/ICAO%20SMS%20Framework.pdf Bryant, P. (2015). 3515NSC Safety Management Module 2: Basic Safety Concepts. Retrieved from Griffith University, School of Natural Sciences, Learning@Griffith website: https://bblearn.griffith.edu.au/bbcswebdav/pid-1389403-dt-content-rid4162354_1/courses/3515NSC_3151/ICAO%20SMS%20Module%2002%20%20Basic%20Safety%20Concepts%20Part%201%282%29.pdf Bryant, P. (2015). 3515NSC Safety Management Module 3: Introduction to Safety Management. Retrieved from Griffith University, School of Natural Sciences, Learning@Griffith website: https://bblearn.griffith.edu.au/bbcswebdav/pid-1408063-dt-content-rid4245830_1/courses/3515NSC_3151/ICAO%20SMS%20Module%2003%20%20Introduction%20to%20Safety%20Management%282%29.pdf Bryant, P. (2015). 3515NSC Safety Management Module 5: Risks. Retrieved from Griffith University, School of Natural Sciences, Learning@Griffith website: https://bblearn.griffith.edu.au/bbcswebdav/pid-1413903-dt-content-rid4290069_1/courses/3515NSC_3151/ICAO%20SMS%20Module%2004%20%26%2005%20%20Hazards%20%26%20SRM.pdf GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 16 of 23 Bryant, P. (2015). 3515NSC Safety Management Module 8: SMS Planning. Retrieved from Griffith University, School of Natural Sciences, Learning@Griffith website: https://bblearn.griffith.edu.au/bbcswebdav/pid-1431645-dt-content-rid4415160_1/courses/3515NSC_3151/ICAO%20SMS%20Module%2008%20%20SMS%20Planning%283%29.pdf CASA (Civil Aviation Safety Authority). (2014). SMS for Aviation – A Practical Guide: Safety Assurance. http://casa.gov.au/wcmswr/_assets/main/sms/download/2014-sms-book4-safetyassurance.pdf Commission of Inquiry into the Air Ontario Crash at Dryden, Ontario (Canada), & Moshansky, V. P. (1992). Final report. Ottawa: The Commission. https://bblearn.griffith.edu.au/bbcswebdav/pid-1336051-dt-content-rid3984476_1/courses/3515NSC_3151/Moshansky%20Vol%201%20Dryden%20Report%281% 29.pdf ICAO (International Civil Aviation Organisation). (2013). Doc 9859 Safety Management Manual (SMM). http://www.icao.int/safety/SafetyManagement/Documents/Doc.9859.3rd%20Edition.alltext.e n.pdf Pidgeon, N. F. (March 1991). Safety Culture and Risk Management in Organizations. Journal of Cross-Cultural Psychology, 22(1). doi: 10.1177/0022022191221009 GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 17 of 23 Appendix A – ICAO SMS Framework (Source: Bryant, Module 1, 2015). Figure B – Air Ontario Inc. Flight Operations Organisation (March 1989) (Source: Moshansky, 1992, p419) GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 1 of 23 Appendix C – Ideal Management Structure for a Safety-Conscious Organisation (Source: Bryant, 2015, Module 3) GU | 3515NSC | NSC| Written Assignment 1 | Rebecca Spencer | s2942503 | Page 2 of 23 Appendix D – Effective Safety Reporting – Five Basic Characteristics (ICAO, 2013, p33). Appendix E – Accident Causation (Source, ICAO, 2013, p19). Appendix F – CASA Safety Culture Index (Source: CASA, 2014, p41)
 0
0
advertisement


Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users