Treating female pattern hair loss
advertisement

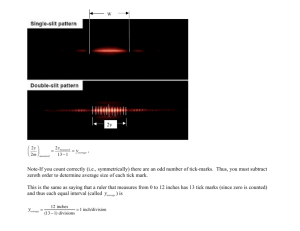
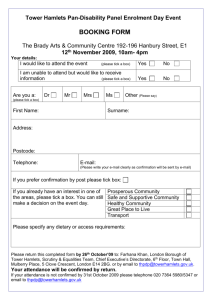
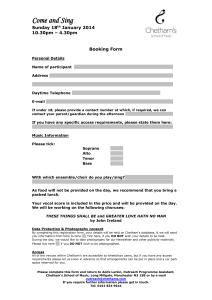
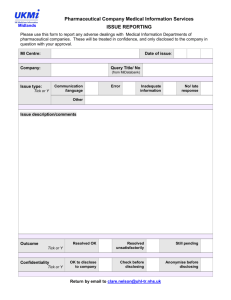
VOLUME 16 • NUMBER 10 JUNE 2009 Treating female pattern hair loss Noticeable hair loss can be deeply distressing. Here are some medical treatments that may help. A bout one-third of women experience hair loss (alopecia) at some time in their lives; among postmenopausal women, as many as two-thirds suffer hair thinning or bald spots. Hair loss often has a greater impact on women than on men, because it’s less socially acceptable for them. Alopecia can severely affect a woman’s emotional well-being and quality of life. The main type of hair loss in both sexes— and the subject of this article—is androgenetic alopecia, or female (or male) pattern hair loss. In men, hair loss usually begins above the temples, and the receding hairline eventually forms a characteristic “M” shape; hair at the top of the head also thins, often progressing to baldness. In women, androgenetic alopecia begins with gradual thinning at the part line, followed by increasing diffuse hair loss radiating from the top of the head. A woman’s hairline rarely recedes, and women rarely become bald. There are many potential causes of hair loss, including medical conditions, medica- tions, and physical or emotional stress. If you notice unusual hair loss of any kind, it’s important to see your primary care provider or a dermatologist, to determine the cause and appropriate treatment. You may also want to ask your clinician for a referral to a therapist or support group to address emotional difficulties. Hair loss can be frustrating, but recent years have seen an increase in resources for coping with the problem. What is androgenetic alopecia? Almost every woman eventually develops some degree of female pattern hair loss. It can start any time after the onset of puberty, but women tend to first notice it around menopause, when hair loss typically increases. The risk rises with age, and it’s higher for women with a history of hair loss on either side of the family. As the name suggests, androgenetic alopecia involves the action of the hormones called androgens, which are essential for normal male sexual development and have other important functions in both sexes, including sex drive and Patterns of female hair loss regulation of hair growth. The condition may be inherited and involve several different genes. It can also result from an underlying endocrine condition, such as overproduction of androgen or an androgensecreting tumor on the ovary, pituitary, or adrenal gland. Type I Type II Type III In either case, the alopecia Clinicians use the Ludwig Classification to describe female pattern is likely related to increased hair loss. Type I is minimal thinning that can be camouflaged with hair andro gen activity. But unstyling techniques. Type II is characterized by decreased volume and like androgenetic alopecia in noticeable widening of the mid-line part. Type III describes diffuse men, in women the precise thinning, with a see-through appearance on the top of the scalp. role of androgens is harder to IN THIS ISSUE Avoiding tick-borne 4 illness Diseases spread by ticks are becoming more common. Here are some ways to help reduce your chances of getting one. In the journals 7 Shift work and health; triplenegative breast cancer in African American women. By the way, doctor 8 What can I do about strep B vaginitis? What’s normal vaginal discharge? What’s new Positive Psychology Hypertension: Controlling the “silent killer” Special Health Reports from Harvard Medical School To order, call 877-649-9457 (toll-free) or visit us online at www.health.harvard.edu. Contact us Write to us at womens _health@ hms.harvard.edu For customer service, write us at harvardWL@ strategicfulfillment.com This Harvard Health Publication was prepared exclusively for Amy Quach - Purchased at http://www.health.harvard.edu/ Hair loss continued EDITORIAL BOARD Board members are associated with Harvard Medical School and affiliated institutions. They review all published articles. Editor in Chief Cardiology Dermatology Endocrinology Epidemiology Gastroenterology Genetics Gynecology Internal Medicine Neurology Nutrition Oncology Psychiatry Radiology Surgery Celeste Robb-Nicholson, M.D. Paula Johnson, M.D., M.P.H. Suzanne Olbricht, M.D. Anne Klibanski, M.D. JoAnn Manson, M.D., Dr.P.H. Karen K. Miller, M.D. I-Min Lee, M.D., Sc.D. Stephen E. Goldfinger, M.D. Susan P. Pauker, M.D. Martha K. Richardson, M.D. Isaac Schiff, M.D. Karen Carlson, M.D. Nancy Rigotti, M.D. Beverly Woo, M.D. Anne B. Young, M.D., Ph.D. Bruce Bistrian, M.D., Ph.D. Helen K. Delichatsios, M.D., S.M. Judy E. Garber, M.D., M.P.H. Ellen Blumenthal, M.D. Malkah T. Notman, M.D. Margaret S. Ross, M.D. Barbara Weissman, M.D. Barbara Smith, M.D., Ph.D. E D I T O R I A L S TA F F Editor Managing Editor Copy Editor Contributing Editors Art Director Production Editor Carolyn R. Schatz Nancy A. Ferrari James C. Sellman Christine Junge, Kristie Reilly Heather Derocher Charmian Lessis CUSTOMER SERVICE Phone: 877-649-9457 (toll-free) E-mail: HarvardWL@StrategicFulfillment.com Online: www.health.harvard.edu/ customer_ service Mail: Harvard Women’s Health Watch P.O. Box 9308 Big Sandy, TX 75755-9308 Subscriptions $32 per year (U.S.) Bulk subscriptions StayWell Consumer Health Publishing One Atlantic St., Suite 604 Stamford, CT 06901 888-456-1222, ext. 31106 (toll-free) 203-653-6266 ddewitt@staywell.com Corporate sales and licensing StayWell Consumer Health Publishing One Atlantic St., Suite 604 Stamford, CT 06901 jmitchell@staywell.com Editorial correspondence E-mail: carolyn _schatz@hms.harvard.edu Letters: Harvard Women’s Health Watch 10 Shattuck St., 2nd Floor Boston, MA 02115 Permissions Copyright Clearance Center, Inc. Online: www.copyright.com Published by Harvard Health Publications, a division of Harvard Medical School Editor in Chief Anthony L. Komaroff, M.D. Publishing Director Edward Coburn © 2009 Harvard University (ISSN 1070-910X) Proceeds support the research efforts of Harvard Medical School. Harvard Health Publications 10 Shattuck St., 2nd Floor, Boston, MA 02115 The goal of the Harvard Women’s Health Watch is to interpret medical information for the general reader in a timely and accurate fashion. Its contents are not intended to provide personal medical advice, which should be obtained directly from a physician. We regret that we cannot respond to inquiries regarding personal health matters. PUBLICATIONS MAIL AGREEMENT NO. 40906010 RETURN UNDELIVERABLE CANADIAN ADDRESSES TO: CIRCULATION DEPT., 1415 JANETTE AVENUE WINDSOR, ON N8X 1Z • E-mail: ddewitt@staywell.com 2| Harvard Women’s Health Watch | determine. On the chance that an androgensecreting tumor is involved, it’s important to measure androgen levels in women with clear female pattern hair loss. In either sex, hair loss from androgenetic alopecia occurs because of a genetically determined shortening of anagen, a hair’s growing phase, and a lengthening of the time between the shedding of a hair and the start of a new anagen phase. (See “Life cycle of a hair.”) That means it takes longer for hair to start growing back after it is shed in the course of the normal growth cycle. The hair follicle itself also changes, shrinking and producing a shorter, thinner hair shaft—a process called “follicular miniaturization.” As a result, thicker, pigmented, longer-lived “terminal” hairs are replaced by shorter, thinner, non-pigmented hairs called “vellus.” A clinician diagnoses female pattern hair loss by taking a medical history and examining the scalp. She or he will observe the pattern of hair loss, check for signs of inflammation or infection, and possibly order blood tests to investigate other possible causes of hair loss, including hyperthyroidism, hypothyroidism, and iron deficiency. Unless there are signs of excess androgen activity (such as menstrual irregularities, acne, and unwanted hair growth), a hormonal evaluation is usually unnecessary. Treatment with medications Medications are the most common treatment for female pattern hair loss. They include the following: Minoxidil (Rogaine, generic versions). This drug was introduced as a treatment for high blood pressure, but people who took it noticed that they were growing hair in places where they had lost it. Research confirmed that a 2% solution of minoxidil applied directly to the scalp could stimulate hair growth. How it works is still not clear. Two double-blind studies of women ages 18 to 45 demonstrated its effectiveness. In one study, 13% of female minoxidil users had moderate hair growth, and 50%, minimal growth (compared with 6% and 33%, respectively, in the placebo group). In the second study, 60% of women in the minoxidil group reported new hair growth, compared with 40% in the placebo group. As a result of these studies and others, over-the-counter 2% minoxidil is FDA-approved for treating androgenetic alopecia in women. Clearly, minoxidil is not a miracle drug. While it can produce some new growth of fine hair in some—not all—women, it can’t restore the full density of the lost hair. It’s not a quick fix, either. You won’t see results until you use the drug for two months. The effect often peaks at around four months, but it could take longer, so plan on a trial of six to 12 months. If Life cycle of a hair minoxidil works for you, you’ll need to keep using it to mainA B C tain those results. If you stop, you’ll start to lose hair again. How to use minoxidil: Be sure that your hair and scalp are dry. Using the dropper or spray pump that’s provided Follicle Dermal Hair with the over-the-counter solupapilla shaft tion, apply it twice daily to every area where your hair is thinEach hair develops from a follicle—a narrow pocket in the ning. Gently massage it into the skin—and goes through three phases of growth. Anagen (A), scalp with your fingers so it can the active growth phase, lasts two to seven years. Catagen (B), reach the hair follicles. Then airthe transition phase, lasts about two weeks. During this phase, dry your hair, wash your hands the hair shaft moves upward toward the skin’s surface, and the thoroughly, and wash off any dermal papilla (the structure that nourishes cells that give rise solution that has dripped onto to hair) begins to separate from the follicle. Telogen (C), the your forehead or face. Don’t resting phase, lasts around three months and culminates in shampoo for at least four hours the shedding of the hair shaft. afterwards. June 2009 www.health.harvard.edu This Harvard Health Publication was prepared exclusively for Amy Quach - Purchased at http://www.health.harvard.edu/ Some women find that the minoxidil solution leaves a Hair transplantation deposit that dries and irritates their scalp. This irritation, Hair transplantation, a procedure used in the United States called contact dermatitis, is probably caused not by the for more than 50 years, involves removing a strip of scalp minoxidil itself, but rather by the alcohol that is included from the back of the head and using it to fill in a bald patch. to facilitate drying. A 5% solution Today, 90% of hair-transplant sur(available only by prescription and Follicular unit transplantation geons use a technique called follicuapproved only for men) is more effeclar unit transplantation, which was tive than the 2% formulation and introduced in the mid-1990s. C may be prescribed off-label for womDuring this procedure, surgeons en. The 5% version comes in a foam, remove a narrow strip of scalp and which appears to cause less irritation divide it into hundreds of tiny grafts, B than the liquid. each containing just a few hairs. Side effects and concerns: MinoxiEach graft is planted in a slit in the dil is safe, but it can have unpleasscalp created by a blade or needle in ant side effects even apart from the the area of missing hair. Hair grows naturally this way, in small clusters of alcohol-related skin irritation. Someone to four follicles, called follicular times the new hair differs in color A units. As a result, the graft looks betand texture from surrounding hair. ter than the larger “plugs” associated Another risk is hypertrichosis— with hair transplants of yesteryear. excessive hair growth in the wrong The transplanted hair will shed places, such as the cheeks or forewithin two to three weeks, and new head. (This problem is more likely growth will start at around three with the stronger 5% solution.) Bemonths. After six to nine months, cause the patent on Rogaine (the most people will have achieved 60% brand-name version of minoxidil) of new hair growth. Some surgeons has expired, many generic products This procedure can take several hours. First, prescribe minoxidil after the operaare available. They all contain the surgeons remove an elliptical strip 3 to 4 tion, but this approach hasn’t been same amount of minoxidil, but some inches long from the back of the scalp and studied enough to determine its include additional ingredients, such trim the hairs short (A). The strip is then divided effectiveness. as herbal extracts, which might trig- into 500 to 2,000 separate follicular units, each containing only a few hairs (B). The units are then Side effects and concerns: Around ger allergic reactions. the time new hair growth starts, Anti-androgens. Androgen recep- planted in an equivalent number of slits made in the scalp in the area of missing hair (C). some women experience folliculitis tor–blocking drugs such as spirono(inflammation of the follicle). This lactone (Aldactone) and finasteride (Propecia) are not approved for the treatment of female minor complication can be treated with compresses and pattern hair loss, and there is little reliable evidence that antibiotics. A more serious hazard is shock loss, the sudden they are effective. However, some case studies suggest that loss of hair that normally grows in the area of the transplant. women who don’t respond to minoxidil may benefit from Shock loss affects 30% to 50% of female hair-transplant the addition of spironolactone. In the relatively uncommon recipients; fortunately, the loss is usually temporary, and cases where there is an excess of androgen, a clinician may the hair will regrow. One drawback is that there’s a finite prescribe 100 to 200 milligrams of an androgen receptor– amount of donor hair, and it may not be enough to fill in blocking drug daily, together with an oral contraceptive for the transplant site as densely as before, especially if the area women of reproductive age. (A woman taking one of these of thinning hair is large. A transplant procedure can cost drugs should not become pregnant because they can cause from $4,000 to $15,000 and is rarely covered by insurance. genital abnormalities in a male fetus.) Possible side effects include weight gain, loss of libido, depression, and fatigue. Selected resources Iron supplements. In some women, iron deficiency could A Woman’s Guide to Hair Loss and Excess Hair, a Special Health be a cause of hair loss. Your clinician may test your iron level, Report from Harvard Medical School, available from Harvard particularly if you’re a vegetarian, have a history of anemia, Health Publications. To order, call 877-649-9457 (toll-free) or or have heavy menstrual bleeding. Iron supplements are go to www.health.harvard.edu/WHL. recommended if a woman’s iron level is less than 70 nanoAmerican Academy of Dermatology grams per milliliter. However, there’s no reliable evidence 866-503-7546 (toll-free) that iron supplementation is helpful for female pattern www.aad.org hair loss. www.health.harvard.edu June 2009 | Harvard Women’s Health Watch This Harvard Health Publication was prepared exclusively for Amy Quach - Purchased at http://www.health.harvard.edu/ |3 Recognizing and avoiding tick-borne illness Most tick bites won’t make you sick, but the ones that do can be serious. J une is here and the bugs are out—in yards and gar- tick looks like a tiny spider and is not quite onedens, at the beach, and along hiking trails and pathways. eighth of an inch long (other tick species may Lone star tick* Most are just an annoyance, but some are vectors, or be slightly larger). An adult tick engorged with blood transmitters, of disease. may be the size of a small marble. To mature from one stage In the United States, the chief culprits are ticks—in par- to the next, the tick needs a blood meal. Larvae and nymphs ticular, the deer tick (also called the black-legged tick), feed on small vertebrates such as birds and rodents (in parwhich can carry and transmit the bacterium responsible for ticular, the white-footed mouse). Adult ticks attach to larger Lyme disease. Considered somewhat rare hosts—chiefly deer—where they mate and just 25 years ago, Lyme disease is now the How big is a tick? feed before the female drops off to lay eggs. most common vector-borne illness in the Over a lifetime, a tick may feed on a wide United States. About 20,000 cases are revariety of animals, potentially putting it in contact with several infectious organisms. ported annually to the CDC, and the agenIf ticks weren’t bloodsucking, diseasecy says that’s only 10% of the total. spreading parasites, we might be more inWe consulted tick expert Dr. Jonathan clined to admire how well engineered they Edlow of Harvard Medical School and are. They have receptors on their front legs Boston’s Beth Israel Deaconess Medical that detect small vibrations and the breath Center, whose book Bull’s Eye: Unraveling the Medical Mystery of Lyme Disease, outof passing animals and people. A tick that is Adult “questing”—seeking a blood meal—will perch lines the history of this emerging infectious Nymph tick disease. According to Dr. Edlow, there are on tall grass or low bushes and wave its front several reasons for the rising incidence of legs, which are equipped with small barbs for Lyme disease. Its geographical range has expanded, mostly latching on to fur, feathers, or skin. Once it gets on its host, because of the growing deer population, which harbors the the tick may crawl around for several hours before attaching. ticks. Also, land once cleared for farming has become reTo feed, the tick inserts a tube-like mouthpart called a forested, attracting more deer (and other tick hosts) as well hypostome into the skin (see the illustration on page 6) and as suburban development. As a result, says Dr. Edlow, “peo- secretes a salivary cement to hold the mouthpart in place. ple’s day-to-day activities—their hobbies, their work, and Backward-pointing barbs on the hypostome help secure where they live—put them in closer contact with wildlife the connection. Tick saliva also contains substances that than they were 50 years ago.” Finally, both patients and cli- facilitate feeding (and disease transmission), including antinicians recognize the disease more readily than ever before. coagulants, anti-inflammatory and immunosuppressive Lyme disease is the predominant tick-borne illness in agents, and vasodilators. During the blood meal, pathothe United States, but it’s not the only one. Ticks can spread genic (disease-causing) organisms in the tick’s gut migrate other bacterial and viral diseases, including babesiosis, ana- to the salivary gland and can be transmitted to the host. plasmosis, ehrlichiosis, tularemia, Rocky Mountain spotIt’s not clear how long an infected tick must be attached ted fever, relapsing fever, Colorado tick fever, and southern before it transmits a disease (a crawling tick doesn’t transtick-associated rash illness (STARI). Tick paralysis, another mit anything). For Lyme disease, it probably takes one to tick-borne disease, is caused not by an infectious organism three days. “It’s a spectrum, but the faster you get it off, the but by a toxin that the tick itself produces. Most tick bites less likely you are to get sick from it,” says Dr. Edlow. won’t give you a disease, but some can, and there is no vaccine to protect you from the vast majority of these diseases. Signs, symptoms, and treatment (There is a vaccine for European tick-borne encephalitis). Tick-borne diseases occur throughout the United States, It’s almost impossible to avoid ticks completely, especially chiefly in late spring and summer, when ticks are most if you spend time outdoors. But you can take steps active and most likely to come in contact with humans. to lower your risk of getting bitten or, if you’re Symptoms vary but usually include fever, chills, muscle bitten, of becoming ill. aches and pains, headache, and sometimes nausea or a rash. Lyme disease, caused by the bacterium Borrelia burgdorferi, Deer tick* is usually heralded by erythema migrans (EM), an expandWhat makes a tick tick? A deer tick’s life cycle typically spans two years and involves ing area of redness surrounding the tick bite. Rocky Mounfour stages of development: egg, larva, nymph, and adult. tain spotted fever and tick-borne relapsing fever start with At the larval stage, the tick is barely bigger than a pinpoint. sudden high fever and chills. A nymph tick is about the size of a poppy seed. An adult *Tick photos, courtesy of the CDC, are not true size. 4| Harvard Women’s Health Watch | June 2009 www.health.harvard.edu This Harvard Health Publication was prepared exclusively for Amy Quach - Purchased at http://www.health.harvard.edu/ Most tick-borne illness is caused by bacteria, so it can be treated with antibiotics. But it’s important to diagnose the problem early, to avoid complications. For example, a delay in diagnosing Lyme disease can result in cardiac symptoms, neurological problems, and arthritis. Luckily, most people develop EM, the telltale early sign, although you can miss it if it appears on the scalp or another hard-to-see area. Some EM clears centrally to form a “bull’s eye,” which is regarded as a diagnostic sign of Lyme disease and a reason to start antibiotic therapy. But the most common pattern is “a uniform redness without the bull’s eye,” says Dr. Edlow. The most lethal tick-borne disease in the United States is Rocky Mountain spotted fever, caused by the Rickettsia rickettsii bacterium. Despite its name, the disease is found Tick-borne diseases affecting humans in the United States Infectious organism Tick vector Symptoms Initial treatment Lyme disease Borrelia burgdorferi (bacterium) Ixodes (I.) scapularis, I. pacificus (deer or black-legged tick) Erythema migrans (expanding area of redness or rash around the bite), fatigue, fever, chills, muscle aches, headache. Antibiotics (doxycycline, tetracycline, amoxicillin) Northeast, Southeast, South Central, Pacific Coast Anaplasmosis Anaplasma phagocytophilum (bacterium) I. scapularis, I. pacificus (deer or black-legged tick) Fever, chills, headache, muscle pain, nausea, cough, sore throat—rarely, rash. Antibiotics (doxycycline, tetracycline) Northeast, upper Midwest, Pacific Coast Babesiosis Babesia microti (protozoan parasite) I. scapularis, I. pacificus (deer or black-legged tick) Fatigue, fever, sweats, headache, muscle pain, gastrointestinal symptoms, enlarged spleen. Combination clindamycin and quinine or azithromycin and atovaquone Northeast, upper Midwest, Pacific Coast Ehrlichiosis Ehrlichia chaffeensis, Ehrlichia ewingii (bacterium) Amblyomma (A.) americanum (lone star tick) Fever, chills, headache, muscle pain, nausea, cough, sore throat—rash in 30% to 40% of adults. Antibiotics (doxycycline or tetracycline; resistant to many other antibiotics) Mid-Atlantic, Southeast, and South Central Southern tickassociated rash illness (STARI) Unknown, possibly a new type of Borrelia bacterium A. americanum (lone star tick) Erythema migrans (see Lyme disease, above). Antibiotics (tetracycline) Southeast, South Central, East Coast into Maine Colorado tick fever Colorado tick fever virus Dermacentor (D.) andersoni (Rocky Mountain wood tick) Fever, chills, headache, muscle pain; fever may remit then return—rarely, a spotted rash. Supportive care (rest, fluids, ibuprofen or acetaminophen) Mostly Colorado, Utah, and Montana Rocky Mountain spotted fever Rickettsia rickettsii; Rickettsia parkeri (bacterium) D. andersoni (Rocky Mountain wood tick); D. variabilis (American dog tick); A. americanum (lone star tick) Fever, nausea, vomiting, muscle pain, headache, elevated liver enzymes, gastrointestinal problems—spotted rash two or three days after fever onset. May cause coma or death. Antibiotics (tetracycline, chloramphenicol), fluids Widespread in the United States, except for the Southwest Tularemia Francisella tularensis (bacterium) D. andersoni (Rocky Mountain wood tick); D. variabilis (American dog tick) Fever, chills, headache, vomiting, sore throat, skin ulcers, lymph node enlargement—may affect the eyes or lungs. Antibiotics (streptomycin, tetracycline, chloramphenicol, fluoroquinolones) Mostly South Central Tick-borne relapsing fever Various Borrelia species (bacterium) Ornithodoros species (soft tick) Recurring episodes of fever, chills, sweats, headache, muscle pain, joint pain, vomiting. Antibiotics (tetracycline, erythromycin) West of the Mississippi Tick paralysis Neurotoxin produced by the tick Various (depends on region) Paralysis, starting at the feet and progressing to the face. May result in death. Recovery begins as soon as tick is removed, but can be fatal if the tick isn’t removed Mostly in the Northwest Disease www.health.harvard.edu June 2009 | Area of the United States Rocky Mountain wood tick* Harvard Women’s Health Watch This Harvard Health Publication was prepared exclusively for Amy Quach - Purchased at http://www.health.harvard.edu/ |5 How to remove a tick Pull tick slowly up and away from the skin Hypostome Tweezers Barbs A tick feeds by way of a two-pronged mouthpart (hypostome) held in place with salivary cement and secured with tiny backward-pointing barbs. To remove the tick, use narrow-tipped tweezers and grasp it as close to the skin as possible; then pull upward slowly and steadily. If the mouthpart remains in the skin, try to remove it. If you can’t, check with your clinician. Wash your skin and hands with soap and warm water. Never crush or squeeze an attached tick, don’t try to burn it with a lighted match, and don’t apply any substance like petroleum jelly, fingernail polish, alcohol, or pesticides. If you do, the tick may regurgitate its stomach contents into your skin, increasing the chance of infection. the DEET directly on your face; spray it into your hands and then apply it to the face. Consult a pediatrician before using it on young children. Wash your hands afterward to avoid getting it into your eyes and mouth. Use permethrincontaining products on clothing, footwear, and camping gear (including cots, nets, and tents). Spray items for 30 to 45 seconds and allow them to dry for two to four hours before wearing or using them. Permethrin should not be applied to the skin. Do a tick drag. This is a way to find out whether there are ticks in your yard. Attach a square yard of white flannel to a 3-foot stick and tie a rope to each end of the stick. Drag the cloth over the lawn and leaves, and examine it for ticks that have latched on. Do this several times. To check bushy or grassy vegetation, use a tick “flag,” which is similar to the drag but mounted like a flag on a stick. (This tip comes from the Tick Management Handbook, available from the Connecticut Agricultural Experiment Station Web site, www.ct.gov/CAES.) Reduce the number of ticks in your yard by clearing leaf litter, low brush, and tall grasses. You may also How to protect yourself Selected resources want to contact a pest-control profesIf you may have been exposed to ticks Centers for Disease Control sional about chemical options and wildand you develop flulike symptoms or and Prevention life control. a rash, see your clinician—even if the 800-232-4636 (toll-free) www.cdc.gov/Features/StopTicks Check yourself. If you’re in an area symptoms go away on their own. Tickinhabited by ticks, check yourself once borne infection usually causes no lasting National Institute of Allergy and Infectious Disease harm if it’s recognized and treated early. a day. (Check children and pets in your 866-284-4107 (toll-free) Of course, it’s better to avoid getting incare, too.) To remove ticks from clothwww3.niaid.nih.gov/topics/tickborne fected in the first place. To that end, here ing, you can use an adhesive lint brush American Lyme Disease Foundation are some measures you can take: or masking or cellophane tape rolled www.aldf.com Protect yourself. Whenever possible, around your hand, sticky side out. Unavoid tick habitats—wooded, bushy, or dress and examine your skin, using a grassy areas, including those near beaches and sand dunes. mirror (or mirrors) for hard-to-see places, such as the back If you’ll be outdoors in tick-infested areas, wear light- of the knees, armpits, back of the neck, and scalp. If you colored clothing (to make ticks easier to spot) with long find a tick attached to your skin, remove it as soon as possleeves and long pants tucked into your socks (to keep ticks sible. (See “How to remove a tick.”) Note the date, and save away from your skin). Use a DEET-containing insect repel- the tick for a month for reference or testing in case you lent on exposed skin (but not under clothes). Don’t spray develop symptoms. mostly in the southeastern United States; 600 to 1,000 cases are reported each year, but health experts think many more cases are not reported. Cells in the lining and walls of blood vessels are infected and organs and systems throughout the body may suffer. Even with prompt treatment, 3% to 5% of cases result in death; without treatment, mortality may be as high as 25%. Other emerging tick-borne diseases in humans include babesiosis, a malaria-like parasitic infection that was once largely a veterinary problem, and anaplasmosis and ehrlichiosis, which have similar symptoms but are caused by different organisms. Tick-borne encephalitis, a viral disease, is found throughout Europe and Asia but is still rare in the United States. Some ticks transmit more than one disease, sometimes from the same bite. The deer tick can transmit babesiosis and anaplasmosis as well as Lyme disease. Lone star ticks are linked to human ehrlichiosis and STARI, a Lyme-like disease. The American dog tick carries Rocky Mountain spotted fever and tularemia; it can also cause tick paralysis. 6| Harvard Women’s Health Watch | June 2009 www.health.harvard.edu This Harvard Health Publication was prepared exclusively for Amy Quach - Purchased at http://www.health.harvard.edu/ in the journals Scientists discover how shift work may threaten health P eople who work on night or rotating shifts are at increased risk for obesity, diabetes, and cardiovascular disease. The biological mechanism leading to such workrelated health outcomes has been largely unknown—until now. A new study has found that a mismatch between the body’s circadian rhythms and behavioral “rhythms” such as the sleep/wake and eating/fasting cycles causes abnormal changes in hormonal and metabolic functions. Such a mismatch—called circadian misalignment—may also explain jet lag. Results were published in the March 17, 2009, issue of the Proceedings of the National Academy of Sciences. To investigate the physiological effects of circadian misalignment, researchers at Boston’s Brigham and Women’s Hospital studied 10 healthy volunteers for 10 days in a laboratory free of time cues. The subjects were placed on a 28-hour day, each day beginning four hours later than the one before, until their sleep/wake cycles were reversed. Activities and meals were also carefully controlled. As a result, the volunteers slept and ate at all phases of their internal circadian cycles, or body clocks. The researchers took hourly measurements of glucose, insulin, cortisol (the socalled stress hormone), and leptin (an appetite-regulating hormone that sends fullness signals to the brain) and daily measurements of blood pressure, heart rate, and other functions, including brain wave activity during sleep. Among the findings: circadian misalignment lowered leptin levels (a factor contributing to increased appetite and possibly obesity), raised waking blood pressure, and increased glucose (despite increases in insulin levels). Three of the 10 subjects showed signs of prediabetes. Circadian misalignment also disrupted normal cortisol cycling, which the authors say could contribute to insulin resistance. Theoretically, a permanent move to night work might alleviate the unhealthy changes triggered by circadian misalignment. But even people who regularly work the night shift “typically don’t get their circadian system properly aligned with the inverted sleep/wake cycle,” says lead author Dr. Frank Sheer. The reason? Most revert to a normal schedule on weekends and days off. Also, even the small exposure to daylight during the morning commute home can reset their circadian system. The researchers concluded that the changes they observed, if sustained chronically, could contribute to night-shift workers’ increased risk for obesity, diabetes, and cardiovascular disease. Triple-negative breast cancer rate is triply high in black women A frican American women in the United States are less likely to develop breast cancer than white women, but they’re more likely to die of the disease, especially at a younger age. Explanations for this disparity include differences in income, education, and access to health care. Researchers have also been investigating biological factors—in particular, an aggressive form of the disease called triplenegative breast cancer, which is more common not only in black women but also in women with BRCA1 mutations and premenopausal women. A new study has found that the rate of triple-negative breast cancer is three times higher in African American women than white women. Earlier research indicated that young African American women were especially vulnerable, but this latest research finds that age makes no difference. The results were published in Breast Cancer Research (online, March 25). Recognized only in recent years as a distinct subtype, triplenegative breast cancer is so named because it lacks receptors for three substances that fuel most breast cancers: estrogen, progesterone, and human epidermal growth factor 2 (HER2). Some of the best breast cancer therapies— anti-estrogen drugs (tamoxifen and aromatase inhibitors) and the anti-HER2 drug Herceptin—target these receptors and thus are useless in treating triple-negative breast cancer. www.health.harvard.edu The researchers created a database of women treated for invasive breast cancer at Boston University Medical Center. Data included tumor type, grade, stage, and receptor status as well as age, body mass index (BMI), and ethnic group. Among the 415 women in the database, 43% were black; 36%, white; and 10%, Hispanic; the rest were Indian or Middle Eastern. Triple-negative breast cancer was found in 20% of the group as a whole, but black women were disproportionately affected: 30% had triple-negative breast cancer, compared with 11% to 13% in the other groups. Premenopausal and postmenopausal black women were equally affected, and BMI was not a factor. In the group as a whole, the risk of triple-negative breast cancer fell as BMI rose. Although there are fewer targeted options for triplenegative breast cancer, combinations of conventional chemotherapeutic drugs, including cyclophosphamide, doxorubicin (an anthracycline), and paclitaxel and docetaxel (taxanes) are often effective. The platinum drugs cisplatin and carboplatin appear promising, and are being evaluated in clinical trials. Other approaches now under investigation include anti-angiogenic drugs (which block the growth of blood vessels that feed the malignancy) and PARP inhibitors, agents that may improve the susceptibility of certain cancer cells to chemotherapy and act on their own as well. June 2009 | Harvard Women’s Health Watch This Harvard Health Publication was prepared exclusively for Amy Quach - Purchased at http://www.health.harvard.edu/ |7 by the way, doctor Q incontinence, burning, and more frequent urinary infections. Especially in postmenopausal women, vulvovaginal symptoms could also result from skin conditions, including allergic reactions to soaps, pads, or feminine hygiene products. You should contact your clinician for another evaluation. She or he may repeat your exam, reSome vaginal discharge is normal. It helps evaluate the discharge, and prescribe a second, to protect against vaginal infections and perhaps longer, course of amoxicillin—or maybe provides lubrication for the vaginal tissues. The try another medication targeting a different condidischarge consists of vaginal skin cells, mucus, tion. If atrophic vaginitis is involved, your clinician and fluid, as well as Candida (a type of yeast) and may prescribe vaginal estrogen. In the meantime, vaginal flora, the bacteria normally found in the you could try using Replens, an over-the-counter vagina. Strep B, or group B streptococcus, is one vaginal moisturizer. Used regularly, it helps relieve possible constituent of the vaginal flora. Most vaginal dryness and irritation by reducing the of the time, vaginal flora and Candida co-exist acidity of the vagina and promoting a healthy balpeacefully. But a change in the balance and in ance among vaginal flora and other organisms. vaginal pH (acidity) may result in vaginal inflammation, or vaginitis. Group B streptococcus is not usually a cause Celeste Robb-Nicholson, M.D. of vaginitis. Even when strep B is found in a labEditor in Chief, HWHW oratory culture of vaginal discharge, it’s hard to tell whether it’s the culprit or just an innocent bystander, since it harmlessly colonizes the vagina What’s normal vaginal discharge? in up to about one-third of women. If strep B is All women have some amount of vaginal discharge. causing the symptoms, then a course of amoxiIt’s produced as part of the process that keeps cillin would be the right treatment. The fact that the vagina healthy. Fluids secreted by the cervix your discharge returned after taking amoxiciland vagina exit the vagina daily, along with sloughedlin suggests that the infection wasn’t completely off epithelial cells, normal bacteria, and mucus. treated—or that other factors may be contributing The amount of normal discharge varies from to your symptoms. One possible cause is bacterial woman to woman and in response to changes vaginosis—a condition in which there is an overin estrogen levels. growth of certain unhealthy bacteria, often causIn premenopausal women, it’s normal to have oneing a fishy odor. This condition may respond to quarter to nearly one teaspoon of white or clear amoxicillin, but metronidazole and clindamycin discharge every day. It may have a slight odor, but are more likely to cure it. it should not smell bad. It’s also normal for this Another possibility to consider is vaginal atrodischarge to be heavier in women who are pregnant phy, a common cause of vulvovaginal symptoms or using estrogen-containing contraceptives. The amount and consistency may vary depending in postmenopausal women. Because estrogen on the phase of a woman’s menstrual cycle. For helps maintain blood flow to the vagina and helps example, discharge may be minimal and sticky right keep tissues plump, elastic, and moist, a decline after the menstrual period and heavy, clear, and in estrogen can cause vaginal tissues to become stringy closer to ovulation. Postmenopausal women thinner and more vulnerable to infection, inhave less vaginal discharge due to the loss of estroflammation, and trauma during activities such as gen, although the use of hormone therapy can sexual intercourse. Symptoms of vaginal atrophy change that equation. (also called atrophic vaginitis) include vaginal Signs of abnormal vaginal discharge, and perhaps dryness, itching, and a burning, watery discharge. infection, include yellowish, grayish, or greenish color; The condition can also produce pain with intercottage cheese–like or foamy consistency; and foul course and a feeling of pressure due to shortenor fishy odor, possibly accompanied by pain, redness, ing or tightening of the vaginal canal. There may swelling, itching, or burning in the vulvovaginal area. also be urinary symptoms, including urgency, I’m 61 and recently began to have a vaginal discharge. It’s not itchy, but sexual intercourse is painful. My doctor diagnosed it as strep B vaginitis and prescribed amoxicillin, which helped. But the discharge returned within a week. What do you recommend? What can I do about strep B vaginitis? Send us a question for By the way, doctor Harvard Women’s Health Watch 10 Shattuck St., 2nd Fl. Boston, MA 02115 womens _ health@hms. harvard.edu Because of the volume of mail we receive, we can’t answer every letter, nor can we provide personal medical advice. 8| A Harvard Women’s Health Watch | June 2009 www.health.harvard.edu This Harvard Health Publication was prepared exclusively for Amy Quach - Purchased at http://www.health.harvard.edu/