Sites rate the best sponsors 2013
advertisement

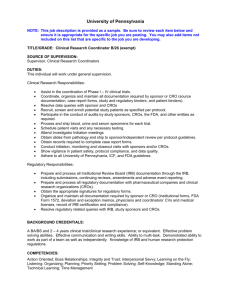
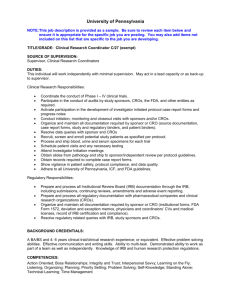
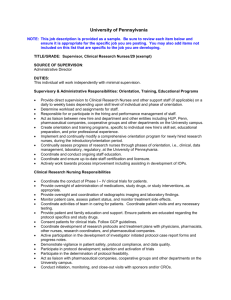
March 2013 A CenterWatch Publication Volume 20, Issue 03 Sites rate the best sponsors 2013 Largest survey response ever puts Biogen Idec, Forest Labs, Bayer at top By Karyn Korieth and Annick Anderson A new CenterWatch survey has found sponsors have done a good job maintaining, but not improving, the quality of their relationships with investigative sites during the past two years. Interestingly, as sponsors increasingly adopt integrated and strategic alliances with CROs, sites reported their relationships with sponsors are less effective in several key areas. More than 75% of sites worldwide rated the overall quality of their working relationships with the average sponsor as “excellent” or “good.” But as sponsors hand over an increasing amount of study conduct to CROs and have less direct contact with sites, investigators expressed frustration—both through the survey and in interviews—with not hav- Sponsors receiving top relationship ratings from their sites Average percent of sites rating ‘Excellent’ across all attributes Total number of attributes for which sponsor was ranked among the top 3/ percent of all attributes 51.4% 27/82% Forest Labs 51.4% 23/70% Bayer 49.7% 25/76% Novo Nordisk 47.8% 11/33% Takeda 47.5% 13/39% Boehringer-Ingelheim 46.7% 8/24% Gilead 46.4% 10/30% Daiichi Sankyo 45.9% 6/18% Roche 45.0% 2/6% Top sponsors out of 22 unique companies rated Biogen Idec Source: CenterWatch 2013 Global Survey of 2,032 Investigative Sites ing enough access to sponsor staff when issues escalate and need to be resolved. Sites gave sponsors poorer marks this year in areas increasingly outsourced to CROs, including managing study monitoring support and prompt payment of grants. In addition, sponsors received fewer excellent marks for effectively working with CROs and maintain- ing open communication with sites, falling by 13% and 10.5%, respectively, during the past two years. In the survey—the largest CenterWatch has conducted to measure the quality of working relationships between sponsors and sites around the world—three companies emerged see Relationship Quality on page 9 As CRO industry turns 30, a look back at modest beginnings Phenomenal growth, strategic partnering highlight evolution of CROs By Daphne Butas S ome of the most well-known CROs—including Chiltern, Quintiles and Parexel—are marking their 30th anniversaries, highlighting the once uncertain road CROs traveled as they evolved from being a market trend to an integral piece of the drug development landscape. The early years In the early 1980s, the drug world was not thinking about outsourcing. The pharmaceutical arena was busy growing in response to the health issues of the decade and conducting groundbreaking research, but was plagued by secrecy, disorganization and a lack of transparency. “Our veterans will tell you that back then, it may have taken six months to enter and analyze clinical data once the last patient in a trial was seen, and that was the norm,” said Phil Bridges, director of corporate communications for Quintiles. Globalization of clinical trials and innovative ideas for expansion were not even on pharma companies’ radars, because the industry was “disorganized,” according to Josef von Rickenbach, Parexel’s founder, CEO and chairman. There were no standard regulations for clinical trials, so doctors wrote each protocol and tried new operating procedures with each trial. Senior-level executives of large pharmas © Copyright 2013. CenterWatch. Duplication or sharing of this publication is strictly prohibited. see CROs: 30 years on page 14 IndustryNews CROs: 30 years 30 years of expanding services and outsourcing models continued from page 1 were unaware of what was happening in R&D, and the privacy stigma attached to the industry made transparency of any kind completely nonexistent. Bridges said industry veterans have told him they remember when there was so much research going on, with no systems or standards in place, that “many pharma companies had reams of data sitting on the shelves, waiting for an analysis to be complete.” Jamie Macdonald, CEO of INC Research, said that in the 1980s, CROs were all about covering the gaps in capacity. “At that time, they were not yet equipped to partner with biopharmaceutical organizations on a global scale to support their drug development efforts,” he said. The turning point: 1982, not only because now-major CROs including Quintiles and Parexel were established, but also because no one knew what might happen to this nascent industry. Quintiles was founded as a biostatistics consulting firm in 1982 by Dennis Gillings, who had been consulting with pharmaceutical customers since 1974 as a professor at the University of North Carolina, Chapel Hill. Gillings wanted to focus on the core competency as a provider of statistical and management consulting services for drug sponsors. Parexel also was born from intention, not from calculated planning or strategic expansion aimed at being anything more than a cottage industry. Also founded in 1982, von Rickenbach and organic chemist Anne Sayigh started Parexel with the purpose of helping foreign companies navigate the U.S regulatory environment. “After about two years, I was really starting to get worried because I was not aware we had competitors,” von Rickenbach told CenterWatch in an earlier interview. “It’s okay to march to your own drummer. But if you are the only marcher, it’s a little concerning.” 14 The CenterWatch Monthly | March 2013 Most commonly outsourced services Prevailing outsourcing model used by sponsors Late 1980s-1990s Study monitoring Statistical analysis Dossier preparation Data management Transactional 2000s Study monitoring Statistical analysis Medical writing Data management Site selection Regulatory support Transactional Preferred provider 2010s Study monitoring Statistical analysis Medical writing Data management Site selection and management Patient recruitment Regulatory support Transactional Preferred provider Functional service provider Multi-functional service provider Integrated alliance Embedded alliance When laws passed in 1983 established a legal system for generic drugs, dramatic changes occurred in the pharmaceutical industry: competition came into play. “Pharma needed additional resources to manage more robust clinical trials,” said Bridges, which is why Quintiles began its global expansion, opening its first international office in 1987. John R. Vogel, Ph.D, drug development consultant, said, “prior to 1993 pharma did little outsourcing to CROs because, by design, they did everything in-house and did not need CROs.” In the mid-to-late 1980s, the legal system had established laws fueling the market for generic drugs and, in turn, making clinical trials and R&D more competitive. It was a prime time for overseas expansion, said Vogel, because companies found “they could enroll patients as quickly as expected and, by moving abroad, CROs were able to find larger pools of subjects for drug testing. Also, in many cases patients were therapeutically naïve, which simplified the clinical trial.” As the 1980s drew to a close, a small force of early CROs existed that—while most thought would remain a cottage indus- try—already were starting to show signs of cleaning up the industry with system implementation, organization and greater transparency. The 1990s: Building a better CRO Thirty years ago, if a sponsor, doctor or other industry expert were asked what the CRO industry would look like in 2013, most would not have predicted such explosive growth. “I always thought it would be a big opportunity,” said von Rickenbach. “But I could not convince anybody. Absolutely nobody believed it.” Vogel said the tipping point that led to the expansion of outsourcing was the Clinton administration. Hillary Clinton was outspoken on the issues surrounding healthcare reform, and her eloquence and spot-on ability to drill down on key issues made pharma companies begin to take notice—and examine their options for maintaining the necessary resources while also cutting costs and reducing overhead. “CROs are effective at helping pharmaceutical companies manage the variability of their business,” said Linda Drumright, general manager, clinical trials optimiza- vices, but also resources on a global scale growth per year. Between 2003 and 2008, tion solutions at IMS Health. Through the that could meet the needs of the growing the CRO industry had a great run, for a provision of resources virtually on demand, industry. number of reasons. New approaches and systems were imple“CROs enable pharmaceutical companies to First, CROs began to promote more sermented so that certain protocols and stan- vices. International studies came to the forepredictably deliver drugs to market.” In addition to offering resources on de- dardization in clinical trials became the front of the drug industry, and biotech outmand for pharmas, CROs also were able to norm, not the exception. As trials became sourcing increased as well. “The notion at this point was how fast bring some order and consistency to a pre- more consistent and efficient, people became viously somewhat chaotic and disorganized less guarded about sharing information, and you could reach the peak of market sales, industry. In the 1990s, CROs were able to scalability and transparency became more thereby maximizing profit over the product life cycle,” said Vogel. Drug companies step in at a pivotal point and offer specific attainable. often spent a fortune attemptresources and completion of ing to get a drug to phase III “projects” with “just-in-time “CROs realized they had to so it could be sent to the FDA resources” to help satisfy the for approval only to have their explosion of compounds being either develop the expertise and hopes dashed, he explained, tested and headcount shortages capacity to perform these specialized leaving them devoid of funds, at sponsors. resources and product. This meant large pharmas services, such as electronic data CROs quickly embraced no longer had to carry overcapture, or partner with niche CROs the idea that the faster a drug head for resources that were could get through the phases not used consistently and inwho could provide them.” of development and approval, stead could outsource pieces —John R. Vogel, Ph.D, drug development consultant the faster sponsors would see of the work puzzle as needed, a return on investment. They allowing them to focus more As a result of CROs’ ideal timing in the were able to both establish an international attention on filling and expanding their pipelines through mergers and acquisitions. late 1990s, the industry saw 20% growth presence and embrace the technological ca“With a largely paper-based FDA, CROs each year between 1998 and 2002. For exam- pabilities for incoming trends such as elecemerged as key resources to shepherd spon- ple, PPD Pharmaco’s CRO/SMO stock prices tronic data capture (EDC). “There has been an accelerated shift to sors through the drug approval process,” saw 99% improvement from December 1997 ($13.625) to December 1998 ($27.188). clinical trial globalization and off-shoring said Macdonald. While the CROs of the 1980s really were over the past 10 years,” said James D. Esinhart, Ph.D., CEO of Chiltern. “This trend able only to be project-based, the CROs of The early 2000s: The boom years the 1990s rolled out a revamped, more cawill continue yet, at the same time, there are pable and experienced offering, capable of By 2003, M&A activity had slowed and compelling reasons to focus patient recruitoffering not only a higher quality set of ser- the top CROs were still tracking about 18% ment in established markets, partly due to the fact that established markets are rapidly evolving economically, demographically High global demand for CRO services and structurally.” Global market size in U.S. billions Vogel said, “CROs realized they had to $26.9 either develop the expertise and capacity to perform these specialized services, such as electronic data capture, or partner with $14.8 niche CROs who could provide them.” $8.6 CROs expanded their capabilities and $3.7 grew their repertoire of services, solidifying $1.6 $0.7 their foothold as a key player in the industry. 1985 1990 1995 2000 2005 2010 Success with EDC led to opportunities in Note: Includes non-clinical, clinical and central lab services Source: CenterWatch see CROs: 30 years on page 16 March 2013 | The CenterWatch Monthly 15 IndustryNews CROs: 30 years continued from page 15 patient recruitment, IRBs, central laboratories and study conduct abroad. But the largest growth driver in contract clinical outsourcing during the past decade has been the establishment of more strategic, integrated relationships including functional and multifunctional service provider, integrated alliance and embedded partnerships between CROs and sponsors. Some industry insiders consider 2005 a “tipping point,” when sponsors embraced working with their CRO partners under preferred provider arrangements with shared governance, systems and processes. Before 2000, said Vogel, the majority of sponsor-CRO deals were transactional—the sponsor contracted for a defined set of services in a single clinical trial or group of studies. The advent of various partnership models promised lower in-house costs, cheaper rates and better quality. “These partnership models ranged from preferred providers (the sponsor pre-qualifies a list of CROs to which it contracts most of its work in return for discounted rates), risk-sharing (the CRO’s bonuses and penalties are based on mutual performance standards), alliances (the CRO derives part of its fee from royalties on product sales) and integration (the sponsor and CRO create a jointly Leading CROs 1995 owned entity),” Vogel explained. Partnering, he said, had a favorable effect on sponsor-CRO relationships, as sponsors “began to question what is their own ‘core competency’ (that which they do best) and what can be done just as well by a CRO partner?” Some sponsors, he said, greatly downsized their internal departments in favor of outsourcing specific activities, increasing the volume and size of sponsor-CRO deals. The late 2000s: Economic downturn Since the global economic downturn in late 2008, sponsors have reduced headcount dramatically and divested underutilized fixed costs (e.g., facilities). This operating environment has accelerated sponsor demand for, and adoption of, more integrated and strategic relationships, in which CROs assume the operating and resource risk for entire portions of a sponsor’s portfolio. Integrated and embedded alliances—when effective—appear to offer sponsors access to dedicated talent and capacity under substantially lower costs. “Over the last decade, the clinical outsourcing paradigm in the pharmaceutical industry has shifted dramatically, from a traditional, capacity-based tactical outsourcing model to more strategic, development-oriented partnerships,” said Samir Shah, EVP of SD and R&D business operations for CRO 2011 Revenue in U.S. millions Corning Quintiles ABPI Parexel ClinTrials IBAH PPD Phoenix International Collaborative Clinical Research $400 $156 $134 $59 $58 $42 $38 $32 $10 Revenue in U.S. billions Quintiles Covance PPD Parexel ICON INC Research PRA International RPS Medpace $3.0 $1.9 $1.5 $1.2 $0.9 $0.6 $0.5 $0.3 $0.2 Source: CenterWatch research of financial analyst and company reports 16 The CenterWatch Monthly | March 2013 ReSearch Pharmaceutical Services (RPS). “The two distinct alliance models that have emerged are programmatic models and the embedded model.” In the programmatic alliance model, the sponsor in a sense “stays out of the kitchen” and receives the output/deliverables, Shah explained, while in the embedded model, overall strategy and direction are retained by the sponsor, but overall responsibility for execution and management of the pipeline across critical but non-core activities resides with the provider. According to RPS, in 2008 the FSP model evolved into the first embedded model. In 2009, when many large and mid-sized pharma were facing both pipeline and financial pressures, the embedded model gained market momentum. The immediate effects were “tremendous cost saving and flexibility to pharma, and a new way for managing their portfolio without losing strategic control,” said Daniel Perlman, chairman and CEO of RPS. “The long-term effects are sustaining cost saving, while preserving quality operations through continual innovation of processes and systems.” Most sponsors—particularly small biotech and pharma companies—continue to use full-service and niche service providers under transactional relationships. But the adoption of integrated alliances (functions managed wholly by external partners) and embedded alliances (functions staffed internally by contract FTEs) has increased rapidly. A recent study conducted by CenterWatch found nearly 90% of the top 30 largest pharma companies have now entered into at least one strategic alliance with a CRO, up from 63% four years ago. Looking ahead CROs will continue to outsource—it is how they began and at the very core of who they are. Experts see CROs expanding their reach into other R&D domains—i.e., discovery, nonclinical, regulatory, commer- Proportion of top 30 pharma companies in at least one FSP/multi-FSP/integrated alliance 63% 47% 2004 87% 2008 2012 Source: CenterWatch cial—in which the outsourcing practice is less mature. “We expect more innovative strategic partnership models to become the standard, as biopharmaceutical companies look for partnership structures that consistently provide more long-term value,” said Macdonald of INC Research. “The cost-cutting trend of recent years will be replaced by more innovative approaches to bring new drugs to market while still growing shareholder value.” “The world has become smaller, where both large and mid-sized global CROs all have a place at the table,” said Esinhart of Chiltern. “Today, service and relationship continue to be key to a CRO’s success.” According to Perlman, both the FSP model and embedded solutions already have effected transformational change within the top 20 biopharma companies. “It remains unclear how CROs will react to this model,” he said. “Several have tried to ‘reinvent’ themselves DUCATIONAL ERVICES Clinical Trial Second Annual oversight summit Vendor Management in Clinical Trials Daphne Butas specializes in health, medical and healthcare-related educational content and writes innovative healthcare documents for government agencies such as the Health Resources Services Administration (HRSA), the Office of Minority Health (OMH) and the National Institutes of Health (NIH). She holds a B.A. from the University of Maryland. Her work has appeared in The Fairfax Times, AOL, The Navy Mutual Aid Association Newsletter and various books. BARNETTES Register by April 12 and SAVE up to $200! Mastering Clinical Trial Monitoring offering grass-roots, FSP-type solutions. Others have shunned away and are moving down the programmatic alliance continuum.” “The biopharmaceutical industry faces unprecedented challenges—cost, regulatory and pipeline driven—necessitating radical change,” said Perlman. “As pharmas reinvent themselves, CROs will need to change their approach to survive long term.” BARNETT EDUCATIONAL SERVICES June 3 - 6, 2013 hilton Back Bay | Boston, mA Clinical Auditing Forum Clinical Quality Risk Management Please reference key code CW1A upon registering. Organized by Cambridge Healthtech Institute ClinicalTrialSummit.com March 2013 | The CenterWatch Monthly 17