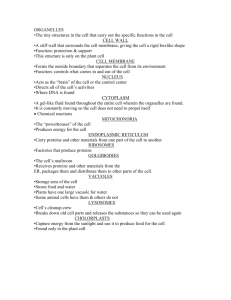
Sabotage of the Cell Signal - Center for Precollegiate Education and
advertisement

Sabotage of the Cell Signal Curriculum Curriculum Introduction Lesson 1 Teacher Instructions Group Assignments Scenario Pt. 1 Scenario Pt. 2 Scenario Pt. 3 – G’ment Response Scenario Pt. 3 – Hospital Personnel Scenario Pt. 3 – Labs Scenario 3 Questions Lesson 2 Teacher Instructions ELISA Plates Student Instructions Data Sheet Lesson 3 Teacher Instructions Science Lab Report Rubric Student Instructions NIH Curriculum: Sabotage of the Cell Signal - A teaching module on the effect of Anthrax toxins on cell signaling. Introduction The signaling systems discussed in this module are only a few of the many ways that cells send messages between cells and the extracellular matrix, and within themselves. Many of the signaling pathways are interconnected with one another, creating an incredibly complex system. Though the system is complex, there are two main points that bear describing. One of the most important aspects of cell signaling regards the protein macromolecules that make are involved in all three stages of signaling, reception, transduction, and response. The second major issue in conducting a message through or between cells involves the many steps that is needed to pass molecule to molecule and create the important cascade that is needed. Each of the following activities in this module fit together to drive home the complexity of the system, and how health and community can be affected if the system is interrupted. Background Information Cell Signaling Cell to cell communication is essential for multicellular organisms because they must coordinate their activities. Cells most often communicate with each other by chemical signals. Communicating cells may be close together or far apart. Cells in a multicellular organism usually communicate by releasing chemical messengers targeted for cells that may not be immediately adjacent. Local regulators are chemicals that stimulate cells nearby, such as the release of growth factors or axon terminals releasing neurotransmitters into a synapse to stimulate receptor cells. Cells can also communicate through direct contact where cell membrane molecules connect, such as developing cells in an embryo or immune system cells. Specialized proteins called integrins are present in the plasma membrane to mediate attachment to the extracellular matrix or neighboring cells. The three stages of cell signaling are reception, transduction, and response. A signal molecule binds to a receptor protein, causing the protein to change shape. Only certain, specific, target cells can detect and react to a signal due to receptors complementary to the signal molecule. Signal molecules work like a ligand, any small molecule that binds to a specific larger molecule, and often stimulate the receptor molecule to change shape. Often this new shape fits the shape of other molecules within a cell. When they bind, the internal molecule now becomes active. Most signal receptors are plasma membrane proteins that are water-soluble and too large to pass freely through the plasma membrane so they must bind to receptors on the outside of a cell. This receptor then transmits information into the cell. There are three major types of cell membrane receptors. a) G-Protein-Linked Receptor is a plasma membrane receptor that activates G proteins within the cytoplasm by removing GDP and replacing it with GTP. The G protein is now active and can bind to another protein, usually an enzyme, in order to stimulate the next step in the pathway. This lasts only a short while because the activated G protein also functions as an enzyme that removes its GTP molecule and replaces it with GDP, to return itself back to the inactive state. Without the GTP, the G protein will also separate from the enzyme. G protein receptor systems function during embryonic development, vision and smell. Some bacteria toxins cause disease by blocking G proteins, and therefore blocking the next step in a signal pathway. b) Tyrosine-Kinase Receptors have enzymatic activity within a cell. For example, when a growth factor ligand binds to tyrosine-kinase receptors on the outside of a plasma membrane it stimulates two separate polypeptides to bind into one active molecule. The part extending into the cytoplasm now functions as an active enzyme to add phosphates to its tyrosine amino acids. This activates the receptor protein so it can activate relay proteins within the cytoplasm. One of these activated tyrosine-kinase dimers has the ability to activate ten different relay proteins that can activate different signal-transduction pathways. c) Ion-Channel Receptors are channel proteins in a plasma membrane that can open or close in response to a signal from a ligand. These channels are important in the functioning of the nervous system. d) Intracellular Receptors are proteins dissolved in the cytosol or nucleus of target cells. Because they are in the cytoplasm their signal ligand must be able to pass through the plasma membrane. Steroids and nitric oxide (NO) have this ability. For example, the male hormone testosterone (a steroid) is released by the testes, passes into a target cell, and binds with a receptor protein in the cytoplasm to activate it. This active protein is now a transcription factor that can bind to a promoter and initiate transcription of mRNA. Pathways relay signals from receptors to cellular responses 1. Proteins are the most common relay molecules in signal transduction pathways. Stimulus by one signal ligand can be amplified many times as it is passed along a pathway. Often these relay proteins are activated by phosphorylation. Protein phosphorylation, a common mode of regulation in cells, is a major mechanism of signal transduction The general name for an enzyme that transfers phosphate groups is protein kinase. They differ from tyrosine kinase proteins in that they phosphorylate other proteins, while tyrosine-kinase phosphorylates itself. Many of the relay molecules in signal transduction pathways are protein kinases that work by phosphorylating each other in a cascading sequence. Enzymes called protein phosphatases function to remove phosphates from activated protein kinases, thus turning off a pathway. 2. Certain small molecules and ions are key components of signaling pathways. Many signaling pathways involve small, non-protein, water-soluble molecules or ions called second messengers. Once a ligand has attached to a plasma membrane receptor and activated it, a second messenger such as cyclic AMP or calcium ions (Ca2+) can function in a pathway by moving rapidly throughout the cytosol. Cyclic AMP is a modified ATP. For example, epinephrine stimulates a G protein receptor that activates a G protein that activates an enzyme embedded in the plasma membrane. This activated enzyme converts ATP into cyclic AMP (cAMP) which in turn activates a protein kinase. The activated protein kinase can now phosphorylate other proteins in its pathway in order to lead to glycogen conversion into glucose in the liver and provide fuel for “fight or flight”. Another enzyme in the cytoplasm functions to inactivate cAMP and keep the signaling pathway from going on indefinitely. Inactivates cAMP Epinephrine G protein receptor Activates G protein Activates enzyme in membrane Converts ATP to cAMP Activates protein kinase Phosphorylates other proteins An example of the effects caused by interrupting the signaling pathway can be seen by the toxins released by the Vibrio cholera bacteria that keep G proteins active. These active G proteins keep stimulating the production of cAMP and stimulate the cells lining our intestines to secrete large amounts of water and salts. This can lead to diarrhea, dehydration and death, especially in infants. Calcium functions as a second messenger more often than cAMP. Increasing the concentration of Ca2+ in the cytoplasm can stimulate muscle cell contraction, cell division and secretion of other substances. Ca2+ functions as a second messenger in both G protein and tyrosine-kinase pathways. Animals have high concentrations of Ca2+ in their interstitial fluid and within their endoplasmic reticulum. There are low concentrations in the cytosol. Slight changes in cytosol concentration can activate a protein in a signal transduction pathway. In some cases, an activated G protein can stimulate the production of a second messenger called Inositol Triphoshpate, or IP3. IP3 then acts as a ligand to stimulate the release of Ca2+ from the endoplasmic reticulum into the cytosol. This released Ca2+ also acts as a second messenger ligand by binding to a protein called calmodulin which becomes an active messenger that can bind to other proteins to stimulate a cellular response, such as apoptosis or cell death. Cellular Responses to Signals: In response to a signal, a cell may regulate activities in the cytoplasm or transcription in the nucleus. A signal may cause an ion channel to open (e.g., nervous or muscular systems) or a change in metabolism (e.g., epinephrine and glycogen to glucose). Other signaling pathways stimulate genes to make proteins in response to a signal. Elaborate pathways amplify and specify the cell’s response to signals. Signal Amplification may occur at each step in transduction of a signal. This allows the cell’s response to be greater than if there was no amplification, e.g., the binding of one epinephrine molecule can result in the production of thousands of enzymes to hydrolyze glycogen into glucose. The Specificity of Cell Signaling is due to different types of signal receptor proteins in plasma membranes and different types of transduction proteins in the cytosol of a cell. Due to this, one type of signal ligand can cause different cells to respond in different ways. Remember that there must be ways to turn off each signal transduction pathway. Otherwise a cell would not be able to respond to a new stimulus. Anthrax (Bacillus anthracis) Gram stained B. anthracis Spores Anthrax is an infectious disease caused by bacteria called Bacillus anthracis (shown above). The bacteria are rod-shaped and tests gram positive when exposed to Gram stain, meaning it has an exterior peptidoglycan layer. The cells are large with square ends and they have centrally located spores. The bacteria can be grown in ordinary nutrient medium aerobically, or anaerobically. The pathogenic effects of the bacteria are primarily caused by the fact that it produces two types of toxins, lethal toxin and edema toxin, along with a protective capsule. Anthrax is primarily a disease of domesticated and wild animals, particularly herbivorous animals, such as cattle, sheep, horses, mules and goats. Humans become infected when brought into contact with diseased animals, which includes their flesh, bones, hides, hair and excrement. Although the spores have been found naturally in soil samples from around the world, in the United States there are only recognized areas of infection in South Dakota, Nebraska, Arkansas, Texas, Louisiana, Mississippi, California and small areas that exist in other states. Even in endemic areas, anthrax infections occur irregularly, often with many years between occurrences. In the United States, the incidence of naturally-acquired anthrax is extremely rare (1-2 cases of cutaneous disease per year). Worldwide, the incidence is unknown, although B. anthracis is present in most of the world. Unreliable reporting makes it difficult to estimate the true incidence of human anthrax worldwide. However, in fall 2001, 22 cases of anthrax (11 inhalation, 11 cutaneous) were identified in the United States following intentional contamination of the mail. The most common form of the disease in humans is cutaneous anthrax, which is usually acquired via injured skin or mucous membranes. A minor scratch or abrasion, usually on an exposed area of the face or neck or arms, is inoculated by spores from the soil or a contaminated animal or carcass. The spores germinate, vegetative cells multiply, and a characteristic gelatinous edema develops at the site. This develops into papule within 12-36 hours after infection. The papule changes rapidly to a vesicle, then a pustule (malignant pustule), and finally into a necrotic ulcer from which infection may disseminate, giving rise to septicemia. Lymphatic swelling also occurs within seven days. In severe cases, where the blood stream is eventually invaded, the disease is frequently fatal. Another form of the disease, inhalation anthrax (called woolsorters' disease in the past), results most commonly from inhaling spore-containing dust where animal hair or hides are being handled. The spores can have a 7 – 42 day germination period, but when the disease begins it is usually brought on suddenly with high fever and chest pain. It progresses rapidly to a systemic hemorrhagic pathology and is often fatal if treatment cannot stop the invasive aspect of the infection. Gastrointestinal anthrax is similar to cutaneous anthrax but occurs on the intestinal mucus lining. The bacteria spread from inflammation in the intestinal tract to the lymphatic system. Intestinal anthrax results from the ingestion of poorly cooked meat from infected animals. Gastrointestinal anthrax is rare but may occur as explosive outbreaks associated with ingestion of infected animals, and has an extremely high mortality rate. Clinical manifestations of Anthrax infection may include blood vessel leakage, pleural effusion, hemorrhaging, sepsis and shock. Treatment is with antibiotics such as ciprofloxacin, which must be administered immediately. The earlier treatment can be administered, particularly for inhalation anthrax, the better the chances will be of recovery. Though not readily available, people can be vaccinated against anthrax. Dysfunction of Normal Cell Signaling By Anthrax The virulence of B. anthracis, is due to the multicomponent anthrax toxins made up of PA (protective antigen), LF (Lethal Factor), and EF (Edema Factor). PA binds to the surface of host cells, allowing the LF and EF to enter. The component, lethal factor (LF), is a metalloprotease, known to cleave most isoforms of mitogen-activated protein kinase (MAPK)-kinases (MAPKKs) close to their N-terminus. This interferes with a major signaling pathway linking the activation of membrane receptors, such as toll-like receptors, to the transcription of several genes. Our normal cell signaling requires kinases phosphorylating downstream substrates. LF prevents this by cleaving the MEK kinases, thus stopping our normal cell signaling (by blocking downstream phosphorylation). This has detrimental effects on our cells including: inhibiting cell growth, blocking phagocytosis, stopping our adaptive immune response, along with cell death. EF is a calcium-dependent adenylyl cyclase which converts ATP to cAMP. This leads to high levels of cAMP inside our cells, causing an unregulated activation of the cAMP pathway. EF has an overall inhibitory effect on our cells. These effects include: inhibiting microbicidal activity, preventing phagocytosis, and blocking cytokine production. LF gains access to the host cell cytosol after it is secreted by newly germinated spores (vegetative bacteria, early infection) or after it is endocytosed from circulation during later, systemic infection. Sabotage of the Cell Signal National Science Education Standards (1996) Center for Science, Mathematics, and Engineering Education (CSMEE) Standard: As a result of activities in grades 9-12, all students should develop abilities necessary to do scientific inquiry and understanding about scientific inquiry. (Activity 1, 2, 3) Understanding of scientific concepts. An appreciation of "how we know" what we know in science. Understanding of the nature of science. Skills necessary to become independent inquirers about the natural world. The dispositions to use the skills, abilities, and attitudes associated with science. Standard: As a result of activities in grades 9-12, all students should develop an understanding about science in personal and social perspectives. (Activity 1, 2, 3) Natural and human induced hazards Issues regarding personal and community health Science and technology in local, national, and global challenges Natural resources and environmental quality Standard: As a result of activities in grades 9-12, all students should develop abilities of technological design and understandings about science and technology. (Activity 1, 2, 3) Abilities and understandings of technological design. Creativity, imagination and a good knowledge base are required in the work of engineering and science. Scientists in different disciplines ask different questions, use different methods of investigation, and accept different types of evidence to support these explanations. Florida Sunshine State Standards SC.912.N.1.1 (Activity 1 – 3): Define a problem based on a specific body of knowledge, for example: biology, chemistry, physics, and earth/space science, and do the following: 1. pose questions about the natural world; 2. conduct systematic observations; 3. examine books and other sources of information to see what is already known; 4. review what is known in light of empirical evidence; 5. plan investigations; 6. use tools to gather, analyze, and interpret data (this includes the use of measurement in metric and other systems, and also the generation and interpretation of graphical representations of data, including data tables and graphs); 7. pose answers, explanations, or descriptions of events; 8. generate explanations that explicate or describe natural phenomena (inferences); 9. use appropriate evidence and reasoning to justify these explanations to others; 10. communicate results of scientific investigations; and 11. evaluate the merits of the explanations produced by others. SC.912.N.1.6 (Activity 1,2,3) Describe how scientific inferences are drawn from scientific observations and provide examples from the content being studied. SC.912.L.14.2 (Activity 3) Relate structure to function for the components of plant and animal cells. Explain the role of cell membranes as a highly selective barrier (passive and active transport). SC.912.L.14.6 (Activity 1,2,3) Explain the significance of genetic factors, environmental factors, and pathogenic agents to health from the perspectives of both individual and public health. SC.912.L.16.10 (Activity 1,2,3) Evaluate the impact of biotechnology on the individual, society and the environment, including medical and ethical issues. SC.912.L.18.10 (Activity 3) Connect the role of adenosine triphosphate (ATP) to energy transfers within a cell. SC.912.L.18.11 (Activity 3) Explain the role of enzymes as catalysts that lower the activation energy of biochemical reactions. Identify factors, such as pH and temperature, and their effect on enzyme activity. HE.912.C.1.8 (Activity 2, 3) Analyze strategies for prevention, detection, and treatment of communicable and chronic diseases. LA.910.2.2.3 (Activity 1, 3) The student will organize information to show understanding or relationships among facts, ideas, and events (e.g., representing key points within text through charting, mapping, paraphrasing, summarizing, comparing, contrasting, or outlining). Vocabulary cAMP: cyclic adenosine monophosphate, a molecule derived from ATP and used as a secondary messenger in cells for intracellular signal transduction. Cytokines: small secreted proteins; important in mediating immune system and inflammation. Conformational change: alteration in the shape, usually the tertiary structure of a protein, as a result of alteration in the environment, pH, temperature, ionic strength or the binding of a ligand (to a receptor) or binding of substrate (to an enzyme).Heterodimers (dimers): 2 separate interacting polypeptide chains which are not the same. Fibronectin: ECM glycoprotein; important in cell migration and wound healing. GTPases (Rho family): GTP binding proteins Integrins: superfamily of cell surface/transmembrane proteins that are involved in binding to extracellular matrix components, most are heterodimeric (two amino acid chains). Ligand: a substance that forms a complex with a biomolecule to serve a biological purpose. In a narrower sense, it is a signal triggering molecule, binding to a site on a target protein. MAPK/ERK (mitogen activated protein kinase or extracellular signal-related kinase) signal pathway: Mitogen-activated protein kinase/extracellular signal-regulated kinase; a family of serine/threonine kinases, which are phosphorylated by other kinases for full activity. Important for gene transcription and regulation. Phosphorylation: addition of a phosphate (PO43-) group to a protein or other organic molecule; can activate or deactivate proteins. Protein Kinases: phosphokinases, a family of enzymes that catalyze the transfer of phosphate from ATP to a second substrate. Additional Resources for Teachers: Antibody Response Video clip http://www.youtube.com/user/nucleusanimation Atlas of Macromolecules, Protein Structure http://www.umass.edu/microbio/chime/pe_beta/pe/atlas/atlas.htm Cell Migration/Integrins http://student.biology.arizona.edu/honors2001/group08/intro/intro1.htm Western Blot Video Summary http://www.biosolutions.info/2008/07/western-blot.html# Western Blot Procedure Sheet http://www.bio.davidson.edu/courses/genomics/method/Westernblot.html References Todar, Kenneth PhD. 2011. “Todar’s Online Textbook of Bacteriology.” http://www.textbookofbacteriology.net/Anthrax.html Robinson, P; Fleming, E; Hack, C; Schneider, D; Gearhart, J (2010) "Biologically-Based Modeling of Anthrax Infection: Modulation of Macrophage MAPK Signaling Pathway by Lethal Toxin", JMedCBR 8, 4 September 2010, http://www.jmedcbr.org/issue_0801/PJRobinson/PJRobinson_09_10.html. Utah Education Resource: http://www.uen.org/Rubric/rubric.cgi?rubric_id=25 Images: Wikimedia commons images, or created by Melissa Guinta http://commons.wikimedia.org/wiki/File:Anthrax_spores.jpg http://commons.wikimedia.org/wiki/File:Bacillus_anthracis_Gram.jpg http://commons.wikimedia.org/wiki/File:Anthrax_-_inhalational.jpg http://commons.wikimedia.org/wiki/File:Anthrax_PHIL_2033.png http://commons.wikimedia.org/wiki/File:Plastic_microcentrifuge_tube_rack-04.jpg http://upload.wikimedia.org/wikipedia/commons/a/aa/200801large.jpg Lesson 1: In the Eye of Infection (TEACHER Instructions) Focus Students participate in a jigsaw strategy to analyze a scenario about the effects of a bioterrorist attack from the perspectives of government employees, healthcare workers, and laboratory technicians. Major Concepts Biotechnology has an important impact in regards to the individual, society, and the environment. When scientists are developing ideas, making inferences from observations and the content available to them helps lead them in the right direction. Objectives After completing this activity, students will Understand that scientific investigation affects public policy. Recognize the flow of scientific investigation from observation to testing. Understand the possible effects of Bacillus anthracis Be able to organize information to show understanding or relationships among facts, ideas, and events. Prerequisite Knowledge Scientific Method Time for Activity 1-2 Class periods (~45 minute class periods) Basic Science-Public Health Connection This opening activity is to introduce your students to the complicated relationship between government, scientists, and society and how these areas might interact during a health crisis. It is also a way to introduce students to the way scientists must systematically study an issue using the methods of science (for example, gathering and analyzing data). Materials & Preparations: Teachers will need to prepare the following materials before conducting this activity: (*based on time available for activity) Scenario 1: Narrator (per student) Scenario 2: News Release (per student) Scenario 3: Lab Personnel (1 for each student assigned this role) – optional* Scenario 3: Healthcare Administrators (1 for each student assigned this role)- optional* Scenario 3: Government Employees (1 for each student assigned this role) – optional* Access to computer, internet, and projector for multimedia simulation on Anthrax attack – optional* Procedure DAY ONE 1. Students should be placed in groups of three. Each group is assigned one of the roles on the following page. 2. Within the group, each student should receive a copy of Scenario 1. Using their own sheet of paper folded hot dog style, instruct them to read the passage individually. After allowing time to read the passage instruct students to discuss and record the important information provided in the scenario for their assigned role in a column called “What do you know” on the left side of the paper. Then instruct them to reflect and record information that would be helpful to them in the assigned role, and record on the side labeled “What do you need to know.” 3. Once completed, students are to be given scenario 2 and repeat the directions above to read, discuss and record “What do you know,” and “What do you need to know,” from the perspective of their assigned role. 4. Students should then be divided into groups containing one of each of the roles assigned. There they are to take three minutes to each present their role and the information they felt pertained to their role to the other two group members. 5. After each person has presented their perspective, students should be instructed to brainstorm what information is needed to know for future action, and record a list of options and suggestions for future investigations. DAY TWO 1. Students should be placed in their groups of three, each with a distinct perspective previously assigned. Provide students with Scenario Part 3 – SPECIFIC TO THEIR ROLE. Give students 15 – 20 minutes to read Part 3 and answer the questions that follow on their sheet of notebook paper. 2. Have each group discuss what their questions were and how they answered, and make a list of group suggestions for improving the response of the Federal Management Agency emergency. (15 minutes) 3. Play the NTI BW Terrorism Tutorial: Go right to the link labeled Conclusions, and open the class to a large group discussion comparing group suggestions to those provided on the site above. (10 minutes) http://www.nti.org/h_learnmore/bwtutorial/multimedia_02_02.html#pagetop (Multimedia flash animation of an Anthrax attack.) CDC/AMRIID, LAB RESEARCHERS LOCAL & FEDERAL EMERGENCY MANAGEMENT, GOVT. OFFICIALS HEALTHCARE PERSONNEL, HOPITAL ADMINISTRATORS CDC/AMRIID, LAB RESEARCHERS LOCAL & FEDERAL EMERGENCY MANAGEMENT, GOVT. OFFICIALS HEALTHCARE PERSONNEL, HOPITAL ADMINISTRATORS CDC/AMRIID, LAB RESEARCHERS LOCAL & FEDERAL EMERGENCY MANAGEMENT, GOVT. OFFICIALS HEALTHCARE PERSONNEL, HOPITAL ADMINISTRATORS CDC/AMRIID, LAB RESEARCHERS LOCAL & FEDERAL EMERGENCY MANAGEMENT, GOVT. OFFICIALS HEALTHCARE PERSONNEL, HOPITAL ADMINISTRATORS Scenario Part 1: (Narrator) On the evening of November 1, a professional football game is being played a Southeastern outdoor stadium before an audience of 74,000. The evening sky is overcast, the temperature warm, a breeze blows from east to west. Two days after the game, hundreds of people in and around the Southeast become ill with fever, cough, and in some cases shortness of breath and chest pain. Some of the sick self-administer over-the-counter cold remedies; some seek phone advice from physicians and nurses; others are seen in clinics, doctors' offices, and emergency departments throughout the city. Influenza cases had been seen in the Southeast 2 weeks before the game, and health-care providers seeing the new patients recommend bed rest and fluids for the presumed flu. Specimens are sent to confirm influenza. A few of the sickest patients get chest radiographs to exclude pneumonia. A few patients are hospitalized; some have blood cultures drawn. The 400 ill persons in the region are receiving care from many different sources so a health emergency is not detected. By November 4, nurses and physicians note the increased volume of serious upper respiratory illness, and some contact the city health department for treatment recommendations and a regional flu update. Blood cultures from the earliest patients grow gram-positive bacilli in seven laboratories around the city. The laboratories identify these as Bacillus species. No further identification is requested, and none is pursued. By the third day after the game, patients with the earliest symptoms are dying. The illness has been rapidly fatal, killing previously healthy young adults within 24 to 48 hours. Members of the medical community, now alarmed by these unexpected and unexplained deaths, urgently contact the state and city health departments. Health department officials contact the Centers for Disease Control and Prevention (CDC). By midnight November 4, 1,200 people around the city have fallen ill, 80 of whom have died. [Patient sample case: A 63 year old man was taken by his wife to the emergency room with a four day history of fever, myalgias, and malaise. His wife reported that he had a sore throat, rhinorrhea, or other respiratory tract symptoms. He awoke confused and disoriented the morning of admission. Medical history included mild hypertension and placement of a coronary stent for atherosclerotic heart disease. He had also attended the football game earlier in the week.] What do you know? (From your assigned perspective, re-read the above scenario and list the information that is important for you in your role) What do you need to know? (List any questions that relate to what is needed for future decisions you may have to make in your role): Scenario Part 2 (News Broadcast) "Previously healthy persons are dying of a rapidly fatal illness that spreads quickly among health-care providers in the state. Expert consultants reached by CBS have suggested potential diagnoses, including the new Spanish flu, Dengue Fever, Streptococcus, and many other infectious and noninfectious diseases. A survey completed by city emergency departments and health clinics finds that persons of all ages and from all sectors of the city continue to come down with similar illness. The numbers have doubled since the previous day, inundating many health-care facilities and straining an already decimated health care system.” “In related News, an anonymous official has stepped forward to inform CBS that they have knowledge that the Federal Bureau of Investigation (FBI) offices in five U.S. cities recently received warnings of an imminent bioterrorist attack. Each threat indicated that a "shower of anthrax would rain on U.S. cities," unless certain demands were met immediately. One of these calls was reported to be to a large city on the Eastern Seaboard. The threats were credible, but no information was relayed to city officials in Northeast or elsewhere. Could this be what is affecting our city?" What do you know? (From your assigned perspective, re-read the above scenario and list the information that is important for you in your role) What do you need to know? (List any questions that relate to what is needed for future decisions you may have to make in your role): Scenario Part 3: Government Response The mayor convenes an emergency meeting of leading medical experts and health officials as reporters gather outside city hall. Questions are how to proceed with the medical issues but issues of the financial impact to the city from a major illness are also concerns. The recommendations from all include isolation of all persons with fever, cough, or chest pain; expanded laboratory analyses; and rapid epidemiologic investigation. How to implement the recommendations are in question. It is decided to send blood and tissue specimens to CDC for urgent analysis and CDC investigators have been requested to arrive at the city as soon as possible. During a news conference, the mayor describes the city's response to what appears to be a serious influenza outbreak, appeals for public calm, and is surprised by questions about the possibility of bioterrorism. The mayor is outraged to learn that the FBI had not informed her of a credible anthrax threat to the Southeast. She is informed that an anthrax vaccine exists, but it is unclear whether any will be made available for civilian use. No one can yet estimate the probable scale of the epidemic or whether there has been a single or multiple attacks. The antibiotic recommendations are now being expanded to include all persons living or working within an area defined by 8 miles west and 1 mile north or south of the stadium on November 1. The mayor is told by her advisors that, in fact, no antibiotic arrivals are imminent. Some states report they have no antibiotics to give, some are refusing to send shipments, and the federal government reports that it will be at least another 6 hours before its antibiotic resources arrive. Despite assurances that anthrax is not contagious, people with the ability to do so flee to the North, causing traffic jams and increasing panic. Some train conductors, bus drivers, and pilots refuse to transport, citing personal safety concerns and threatening to walk off the job if forced. Businesses downwind of the stadium are shut down. The stadium is largely abandoned. Newspapers brand the area "the dead zone." The mayor holds a second press conference to address false allegations that anthrax vaccine is being administered to select individuals in the city. She reports that federal authorities will make available some vaccine for those deemed at highest risk. But due to a national shortage of vaccine and military concerns that this attack may herald further attacks, there is only a highly limited amount of vaccine available. For the most part, the city will have to manage with antibiotics alone. By midnight November 6, anthrax has sickened 3,200 people, 900 of whom have died. Scenario Part 3: Hospital Personnel The recommended isolation protocols quickly fall apart as hospital and clinic staffs struggle to cope with the surge of patients. Fears of a contagious disease prompt hospital staff to don protective positive-pressure hoods; the news shows physicians working in this gear and explains that there are only two dozen or so such hoods available per hospital. Hospitals around the city are then informed of the anthrax epidemic and warned to prepare for a new surge of patients in the wake of the mayor's forthcoming TV address. Recommendations for the care of infected patients are sent to hospitals and clinics around the region and they outline that the state is seeking assistance from state and federal agencies. The mayor tells the hospital staff that antibiotics must be taken by all those who attended the football game and have come in for treatment. For those who attended the game and remain well, arrangements are being made to distribute antibiotics at 20 police stations and schools around the city starting immediately. The mayor wants healthcare personnel to stress that anthrax is not contagious and appeals for calm. By noon November 5, intensive-care units and isolation beds across the city are full. Even patients receiving the most advanced medical care are dying. Patients are febrile, hypotensive, and seem to be in septic shock; some have meningitis. Still, there is no diagnosis for some. At some locations, the shock of rapid and unexplained deaths has created an atmosphere of desperation and confusion among hospital and clinic staff. There are patients with cutaneous infections (pustules on the skin), people with gastrointestinal anthrax infection from eating food exposed to spores, and inhalation anthrax the most deadly form. On the morning of November 6, the mayor announces that schools and homeless shelters will be opened to the ill because hospitals can no longer accommodate new patients. The National Guard will keep order. The Office of Emergency Preparedness, Department of Health and Human Services, and the Federal Emergency Management Agency will provide some logistical support. Federal shipments of antibiotics have begun to arrive by November 7. The distribution centers, now increased to 40, continue to be variably stocked with medicine. A heavy National Guard presence is now evident at distribution centers to prevent violence. At this point, there are effectively no antibiotics left in the city. Approximately 50,000 persons had obtained some quantity before supplies ran out, but there is no record of who has received them. Health-care facilities are unprepared to cope with the continually rising number of patients. By the early hours of November 6, 2,700 persons have become ill with anthrax, 300 of whom have died. Thousands more flood doctors' offices, clinics, and emergency departments, fearing that they are infected with anthrax. Scenario Part 3: Labs In the early evening of November 5, a university laboratory makes a preliminary diagnosis of anthrax from the blood culture of a young patient who died. The laboratory immediately notifies city and state health departments, which in turn notify CDC and FBI. The specimen is transferred to the U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID), where within hours experts report that rapid diagnostic tests support the preliminary diagnosis of anthrax. CDC, FBI, and USAMRIID have stated that the working assumptions are that the disease in Northeast is anthrax and that it is the result of a bioterrorist attack. Widespread exposure to an anthrax aerosol is feared. CDC is seeking news of similar syndromes in other locations around the country. The recommendations made to the mayor from the CDC are that to prevent death, antibiotics must be given before symptoms occur, or at the latest, in the earliest hours after symptoms begin. Patients with serious symptoms are likely to die, no matter what anyone does. Available information suggests that the local supply of needed antibiotics will soon be exhausted; many local pharmacies were already emptied of antibiotics as the initial news of a lethal epidemic spread through the city. Given this shortage of antibiotics, one senior advisor asks the mayor to consider a triage plan that uses all available antibiotics to protect the exposed who are not yet sick. In this plan, antibiotics would be kept from those already sick and thus likely to die, regardless of treatment. The mayor requests immediate federal assistance in obtaining and distributing large supplies of antibiotics. Antibiotic shipments from other states are also urgently requested. All that is known is that many (but not all) of the dying had been at the football game on November 1. At midday November 6, epidemiologists report that some anthrax patients had not attended the game, suggesting that exposure had occurred over a wider area. In addition, computer models show that wind patterns may have blown anthrax spores downwind of the stadium for some miles. The antibiotic recommendations are now being expanded to include all persons living or working within an area defined by 8 miles east and 1 mile north or south of the stadium on November 1. On televised interviews, families of the deceased promise legal action against the FBI for not revealing the threats, and against local and federal government for not supplying sufficient antibiotics and vaccine. Management of dead bodies becomes a growing crisis. Hospital and city mortuaries are full. Many funeral homes have closed. The state health department and CDC report that the deceased must be cremated. Some citizen and religious groups threaten that if cremation is enforced, there may not be full reporting of the dead, and private burial ceremonies would continue. By evening of Nov 7, a total of 4,800 persons have become ill; 2,400 have died. Scenario 3 Questions CDC/AMRIID/LAB RESEARCHERS 1. Should laboratory practices be changed to increase the chance of early detection of anthrax? 2. Based on the information regarding the fact that antibiotics are in short supply and are mostly not effective to those with severe symptoms, as a lab researcher, who do you recommend receive them first? 3. Should an anthrax vaccine be more widely available (take into account issues of production)? 4. How might health professionals and government officials interact with the media to best inform the public and avoid misunderstanding and panic? 5. What are some of the additional health issues that scientists may worry about during a crisis like this? GOVT. AGENCIES 1. Could communities have plans for rapid mass antibiotic acquisition and distribution? What are some of the problems they may have in doing so or doing without? 2. What should the community, hospitals, and professional societies be doing? 3. How might health professionals and government officials interact with the media to best inform the public and avoid misunderstanding and panic? 4. Could outcomes have changed if state and local health officials had prior notification of the anthrax threats? 5. Based on the information regarding the fact that antibiotics are in short supply and are mostly not effective to those with severe symptoms, as a government official, who do you recommend receive them first? HOSPITAL PERSONNEL 1. Should health-care workers become familiar with the early symptoms and signs of anthrax? 2. Could outcomes have changed if state and local health officials had prior notification of the anthrax threats? 3. Based on the information regarding the fact that antibiotics are in short supply and are mostly not effective to those with severe symptoms, as healthcare workers, who do you recommend receive them first? 4. What are some recommendations healthcare personnel can suggest for the future? 5. How can they organize the health response within the hospitals? Teacher Information: (The following is the original beginning of the scenario that may be used for further discussion.) On the evening of November 1, a professional football game is being played in Southeast's outdoor stadium before an audience of 74,000. The evening sky is overcast; the temperature mild, a breeze blows from west to east. During the first quarter of the game, an unmarked truck drives along a highway a mile upwind of the stadium. As it passes the stadium, the truck releases an aerosol of powdered anthrax over 30 seconds, creating an invisible, odorless anthrax cloud more than a third of a mile in breadth. The wind blows the cloud across the stadium parking lots, into and around the stadium, and onward for miles over the neighboring business and residential districts. After the anthrax release, the truck continues driving and is more than 100 miles away from the city by the time the game is finished. The anthrax release is detected by no one. Approximately 16,000 of the 74,000 fans are infected by the anthrax cloud; another 4,000 in the business and residential districts downwind of the stadium also are infected. After the game, the fans disperse to their homes in the greater southeast metropolitan area; some return to homes in neighboring states. A few are from other countries. The driver of the truck and his associates leave the country by plane that night. They will be many time zones away by the time the first symptoms of anthrax appear 2 days later. -------------------------------------------------------------------------------Inglesby, Thomas V. Anthrax: A Possible Case History. Special Issue CDC Emerging Infectious Diseases. http://www.cdc.gov/ncidod/EID/vol5no4/inglesby.htm Johns Hopkins School of Medicine, Baltimore, Maryland, USA Lesson 2: Identification of a Killer (TEACHER Instructions) ELISA SIMULATION LAB Focus Students will continue learning from the scenario introduced in Activity 1, by completing an ELISA simulation to diagnose whether those exposed to the Anthrax attack are exhibiting symptoms from Anthrax and/or other possible pathogens. Major Concepts ELISA is commonly used to test blood serum for the presence of antibodies against disease causing pathogens. Objectives After completing this activity, students will • understand the basic principles of antibody-mediated immunity • experience the steps involved in performing an ELISA • Understand how an ELISA is used as diagnostic tool by medical personnel • understand the disease-causing agent and transmission patterns of certain infectious diseases Prerequisite Knowledge The body produces antibodies in response to an infection. Basic Science-Public Health Connection This activity introduces the use of the ELISA as a way of gathering data about a patient’s illness. It exemplifies how scientific tests can be used to enhance public health. Time to Implement Approximately 45 minutes ELISA Background Information ELISA - Enzyme-Linked ImmunoSorbent Assay and is used in immunology to detect the presence of an antibody or an antigen in a sample. It is often used as a diagnostic tool in medicine. In our experiment today, we have known antigens from eight possible illnesses, fixed to the surface of microtitration plates. When a serum produced from a patient’s blood is applied to the plate, if there are antibodies present in for any of the illnesses being tested for the antibody will attach to the matching antigen. After treatment with the antibody, additional reagents are applied to enable a researcher to view the results. These reagents will react to where the antibodies have attached and fluoresce when UV light is applied. A similar procedure is possible using a plate pre-coated with an antibody which would react to an antigen present in a patient’s blood serum. Either of these plate types can be prepared by a researcher or purchased pre-made for repeated use. Flourogenic Substrate Detection Antibody Antibody Antigen Coated Plate Introduction Eight patients have been sequestered in the local Health Department after expressing the following symptoms: feeling light headed, sweating, coughing, malaise, and swollen lymph nodes. Due to the nature of their symptoms and residence near the Football stadium which was the site of the recent bioterrorist attack, an ELISA has been ordered to try and confirm infection by the bacterium, Bacillus anthracis in a patient’s blood serum. ELISA test plates have been prepared that have antigens for the following diseases pre-fixed in the assigned rows: A. Anthrax B. Pneumonia C. Mononucleosis D. Salmonella E. Influenza F. Streptococcus G. West Nile H. Dengue Fever Materials Required For Lab: 64 microcentrifuge tubes 8 Racks/Holders 8 Pre-treated ELISA plates 16 patient serum samples 8 Pipets 20 ul, plus tips (If use disposable pipets: Need 80, 10 for each station) UV light Paper towels Food coloring 16 Test tubes Permanent marker 16, 50 mL Beakers 1, 500mL Beaker Dish detergent 2, 1000 mL beakers To prepare the following simulated reagents for each group follow the instructions below: Positive controls: Make a 1 mL master solution of each and aliquot 100 ul of the master solutions into 8 microcentrifuge tubes Label each top with a permanent marker with the abbreviations below. Use water and a different color of food coloring to create reagent (suggested coloring below). Anthrax Pneumonia Mononucleosis Salmonella Influenza Streptococcus West Nile Dengue Fever +An +Pn +Mn +Sm +Flu +Stp +WN +Den Red Orange Blue Pink Purple Yellow Green Light blue Tween 20 Wash Buffer: Make a master solution of Wash Buffer using 1000 mL of water, 1 drop of blue food coloring, and 2.5 mL of dish detergent. Provide each group with a 50 mL beaker of solution. Fluorescent Tagged Antibodies: Make a master solution of reagent using 1000 mL of water, 1 drop of green food coloring, and 1 drop of yellow. Provide each group with a 50 mL beaker of solution. Patient Serum: Make a master solution of patient serum. Fill a beaker with 1000 mL of water and add 1 drop of yellow food coloring. Label 16 test tubes with numbers 1-16 and fill ¾ full with reagent. These are now your patient samples to be distributed with the correct ELISA plate. For example, Plate 1: patient 1 and 2; Plate 2: patient 3 and 4 and so on. Laboratory Safety: Gloves and goggles should be worn routinely throughout the experiment as good laboratory practice. Procedure Step 1: Place 20 ul of each positive control into the correct well. Change tips or disposable pipettes between different samples. Step 2: Place 20 ul of distilled water in each of the negative control wells. Step 3: Place 20 ul of the serum from your first patient into the wells 7,8, and 9, and note patient number on data sheet. Step 4: Place 20 ul of the serum from your second patient into the wells, 10, 11, and 12 and note patient number on data sheet. Step 5: Carefully place a small stack of paper towels on top of your ELISA plate and invert quickly to dispose of solutions. Place the plate upside down on paper towels and tap a few times to remove any remaining solutions. Step 6: Add 20 ul of the Wash Buffer (mild detergent called Tween 20) to every well. Step 7: Carefully place a small stack of paper towels on top of your ELISA plate and invert quickly to dispose of solutions. Place the plate upside down on paper towels and tap a few times to remove any remaining solutions. Step 8: Add 20 ul fluorescent tagged antibodies to each well. These antibodies will recognize any antibodies from an unknown serum. Step 9: Gently agitate plate on table to help facilitate binding. Step 10: Carefully place a small stack of paper towels on top of your ELISA plate and invert quickly to dispose of solutions. Place the plate upside down on paper towels and tap a few times to remove any remaining solutions. Step 11: Place the ELISA plate under a UV light to check fluorescence and record results on data sheet by shading in the circles that show up as positive after exposure. Teacher Key for patient infection (ELISA plates) Plate 1: Patient 1 = positive for exposure to Anthrax, Streptococcus. Patient 2 = positive for exposure to Mononucleosis, Influenza Plate 2: Patient 3 = positive for exposure to Salmonella, West Nile, Dengue Fever Patient 4 = positive for exposure to Anthrax Plate 3: Patient 5 = positive for exposure to Influenza, Steptococcus Patient 6 = positive for exposure to Anthrax, Pneumonia Plate 4: Patient 7 = positive for exposure to Anthrax, Influenza Patient 8 = positive for exposure to Salmonella, Influenza, Streptococcus Plate 5: Patient 9 = positive for exposure to Anthrax, Salmonella, Streptococcus, West Nile Patient 10 = positive for exposure to Anthrax, Mononucleosis Plate 6: Patient 11 = positive for exposure to Pneumonia, Mononucleosis, Salmonella, Influenza, Streptococcus Patient 12 = negative Plate 7: Patient 13 = positive for exposure to Mononucleosis, Salmonella, Influenza, Streptococcus Patient 14 = positive for exposure to Anthrax, and Streptococcus Plate 8: Patient 15 = positive for exposure to Influenza Patient 16 = positive for exposure to Anthrax, Mononucleosis Teacher Key for Lab Questions: 1. Why did you perform three identical tests for each control and patient sample? Each assay was performed in triplicate to ensure reproducibility of the results. 2. What might cause some positive results to be lighter in color than others? Weak positive results may be an indication that the patient’s blood serum carries few antibodies against the disease-causing agent. The patient’s exposure to the pathogen may be recent and the body may not have launched a full immune response yet. Alternatively, the infection may have occurred long ago, and the level of antibodies in the patient’s bloodstream is declining. (Note: Other explanations are possible and acceptable, but these are most likely.) 3. What is the function of the secondary antibody and fluorogen in an ELISA? Antigen-antibody complexes formed in the initial steps of an ELISA are not visible to the unaided eye. Therefore, a colorimetric detection system involving a secondary antibody and fluorogen is employed. The secondary antibody, which is conjugated to an enzyme, recognizes and binds to primary antibodies of antigen-antibody complexes, if they are present. Fluorogen substrate is then added. If present, the enzyme linked to the secondary antibody attaches to the substrate and causes it to fluoresce under UV light. 4. What basic principles of antibody-mediated immunity are utilized in an ELISA assay? ELISA assays are based on the principles that antibodies are produced in response to infection and that these antibodies are designed to specifically target particular antigens and bind tightly to them. 5. Why do you think we used a negative control? To ensure that our pre-treated plates would not react without antibodies applied. 6. Why might your patients have tested positive for more than one antibody? More than one positive result may be an indication that the patient’s blood serum carries antibodies against past disease-causing agents. The patient’s exposure to the pathogen may be recent or as a child and the body may have launched a full immune response causing the antibodies to still be present. Lesson 2: Identification of a Killer (STUDENT Instructions) ELISA SIMULATION LAB Objectives: After completing this activity, students will • understand the basic principles of antibody-mediated immunity • experience the steps involved in performing an ELISA • Understand how an ELISA is used as diagnostic tool by medical personnel • understand the disease-causing agent and transmission patterns of certain infectious diseases ELISA Background Information: ELISA stands for Enzyme –Linked ImmunoSorbent Assay and is used in immunology to detect the presence of an antibody or an antigen in a sample. It is often used as a diagnostic tool in medicine. In our experiment today, we have known antigens from eight possible illnesses, fixed to the surface of microtitration plates. When a serum produced from a patient’s blood is applied to the plate, if there are antibodies present in for any of the illnesses being tested for the antibody will attach to the matching antigen. After treatment with the antibody, additional reagents are applied to enable a researcher to view the results. These reagents will react to where the antibodies have attached and fluoresce when UV light is applied. A similar procedure is possible using a plate pre-coated with an antibody which would react to an antigen present in a patient’s blood serum. Either of these plate types can be prepared by a researcher or purchased pre-made for repeated use. Flourogenic Substrate Detection Antibody Antibody Antigen Coated Plate Introduction Eight patients have been sequestered in the local Health Department after expressing the following symptoms: feeling light headed, sweating, coughing, malaise, and swollen lymph nodes. Due to the nature of their symptoms and residence near the Football stadium which was the site of the recent bioterrorist attack, an ELISA has been ordered to try and confirm infection by the bacterium, Bacillus anthracis in a patient’s blood serum. ELISA test plates have been prepared that have antigens for the following diseases pre-fixed in the assigned rows: A. Anthrax B. Pneumonia C. Mononucleosis D. Salmonella E. Influenza F. Streptococcus G. West Nile H. Dengue Fever Materials (Make sure you have the following materials at your station): 8 positive controls labeled for each disease (microcentrifuge tubes) 1 Rack/Holder 1 Pre-treated ELISA plate 2 patient serum samples 1 Pipette 20 ul, plus tips (If use disposable pipettes: Need 10 each station) Access to a UV light Paper towel stack Laboratory Safety: Gloves and goggles should be worn routinely throughout the experiment as good laboratory practice. Procedure Step 1: Place 20 ul of each positive control into the correct well. Change tips or disposable pipettes between different samples. Step 2: Place 20 ul of distilled water in each of the negative control wells. Step 3: Place 20 ul of the serum from your first patient into the wells 7,8, and 9, and note patient number on data sheet. Step 4: Place 20 ul of the serum from your second patient into the wells, 10, 11, and 12 and note patient number on data sheet. Step 5: Carefully place a small stack of paper towels on top of your ELISA plate and invert quickly to dispose of solutions. Place the plate upside down on paper towels and tap a few times to remove any remaining solutions. Step 6: Add 20 ul of the Wash Buffer (mild detergent called Tween 20) to every well. Step 7: Carefully place a small stack of paper towels on top of your ELISA plate and invert quickly to dispose of solutions. Place the plate upside down on paper towels and tap a few times to remove any remaining solutions. Step 8: Add 20 ul fluorescent tagged antibodies to each well. These antibodies will recognize any antibodies from an unknown serum. Step 9: Gently agitate plate on table to help facilitate binding. Step 10: Carefully place a small stack of paper towels on top of your ELISA plate and invert quickly to dispose of solutions. Place the plate upside down on paper towels and tap a few times to remove any remaining solutions. Step 11: Place the ELISA plate under a UV light to check fluorescence and record results on data sheet by shading in the circles that show up as positive after exposure. Lab Questions: Complete the following on your own sheet of paper. 1. Why did you perform three identical tests for each control and patient sample? 2. What might cause some positive results to be lighter in color than others? 3. What is the function of the secondary antibody and flourogen in an ELISA? 4. What basic principles of antibody-mediated immunity are utilized in an ELISA assay? 5. Why do you think we used a negative control? 6. Why might your patients have tested positive for more than one antibody? Data Sheet: Shade the circles where color was detected after UV exposure. Record your Patient #’s and results below: Patient _____: _________________________________________________ Patient _____: _________________________________________________ Lesson 3: Zooming In: What in the toxin is causing cell death? (TEACHER Instructions) Western Blot Analysis Focus In this experiment, students will use a modified Western Blot to test hypothetical cells from the blood samples of patients with symptoms for Anthrax infection. Students are testing for the presence of phosphorylated p38, which would show that the patients are not infected with Anthrax. If the Anthrax lethal toxin is present in cells, it has been identified to block phosphorylation of p38 MAPK (mitogen activated protein kinase) in the signaling pathway that leads to macrophage activation. So instead of creating cells that can help defeat the infection, the apoptosis of cells is triggered and rapid cell death occurs in patients. Major Concepts Western Blot analysis is used for analysis of proteins and can be used by medical personnel to diagnose chronic infections. Cellular proteins are responsible for signal transduction and if not able to function properly can lead to cell death. Objectives Understand the concepts and methodology involved with completion of a Western Blot Analyze Western Blot Analysis as a strategy to detection and lead to treatment of communicable and chronic diseases. Understand that this technique is testing proteins because of their role in cell signaling Prerequisite Knowledge Students should be familiar with both macromolecule structure and function in the cell, and cell signaling transduction pathways. Basic Science-Health Connection This activity incorporates information from Activity 1 and 2 and introduces the students to more detailed techniques that researchers employ to assist doctors in understanding how an illness is affecting the cell. Time to Implement 3 or 4 - 45 minute class periods. May need adjustment Introduction (provided for students) Doctors in the scenario from Lesson 1 & 2 have sent a request to a CDC Lab to help them understand how the Anthrax toxin is affecting their patient’s cells. They are seeking a confirmation that the toxin is affecting cell signaling, in order to help guide them to potential treatment options. They sent over new patient samples that they believe are positive for Anthrax infection due to symptoms and they want the lab to test for the presence of phosphorylated p38. The sample group of patient serum they provided consists of three patients: 2 that were present at the football game where the bacteria was released, and 1 from the surrounding area. All are believed to have Anthrax infection due to the symptoms they are exhibiting. They believe that if non-phosphorylated p38 is present, this shows that the toxin is blocking the phosphorylation of p38 protein in a kinase signaling pathway, and instead of macrophage activation happening, this is the trigger for rapid cell death. LABORATORY SAFETY: Gloves and goggles should be worn routinely throughout the experiment as good laboratory practice. MATERIALS NEEDED (For 6 lab groups) EDVO-TEK KIT #275 Samples for Electrophoresis: Positive Control, Negative Control, 3 Patient Samples, Standard Molecular Weight Dye Markers UltraSpec-Protein Agarose™ 10x Tris-Glycine-SDS Buffer (Chamber Buffer) 10x Tris-Glycine Buffer (for gel preparation only) Practice Gel Loading Solution 1 ml Pipets 100 ml Graduated Cylinder (packaging for samples) Precut Western Blot Membranes (7 x 7 cm) Precut Blotting Filter Papers (7 x 7 cm) Western Blot Stain™ ADDITIONAL MATERIALS NEEDED • 6 Horizontal Gel Electrophoresis Apparatus • D.C. Power Supply (enough to run 6 gels) • Pipets with Tips • Microcentrifuge Tubes, 18-20 • Beakers • 12 Trays or Containers that can hold a 7 x 7 cm piece of membrane + 100 ml of liquid • Disposable Lab Gloves • Several Packs of Paper Towels • • • • • • • Plastic Wrap Scissors Metric Rulers 300 mL Methanol, 95-100% 6 , 50 mL graduated cylindars with tin foil as cover 25 mL Acetic Acid 1000 mL Distilled Water 6 pairs of Forceps 65 degree Celsius incubator Glass tray for the stain BACKGROUND INFORMATION: WESTERN BLOT ANALYSIS Western Blot Analysis involves the direct transfer of protein bands from an agarose or polyacrylamide gel to a charged nylon membrane for analysis. Following an electrophoresis experiment, the gel is removed from the tray and the nylon membrane is placed directly on the gel. Nylon membranes are much stronger and more pliable than gels and can undergo many manipulations without tearing. Protein bands are transferred to the surface of the nylon membrane and are adsorbed on the membrane by hydrophobic bonds. This transfer is achieved electrophoretically in specially designed chambers, by capillary flow or by the application of vacuum. If samples are not prepared separately, the procedure for sample preparation would begin by lysing the cells to release the proteins of interest. This solubilizes the proteins so they can migrate individually through a separating gel. As soon as lysis occurs, proteolysis, dephosphorylation and denaturation begin. These events can be slowed down tremendously if samples are kept on ice or at 4°C at all times and appropriate inhibitors are added fresh to the lysis buffer. Antibodies typically recognize a small portion of the protein of interest (referred to as the epitope) and this domain may reside within the 3D conformation of the protein. To enable access of the antibody to this portion it is necessary to unfold the protein, i.e. denature it. To denature, a loading buffer is used with the anionic denaturing detergent sodium dodecyl sulfate (SDS), and the mixture is boiled at 95-100°C for 5 minutes. Heating at 70°C for 5-10 minutes is also acceptable and may be preferable when studying multi-pass membrane proteins. These tend to aggregate when boiled and the aggregates may not enter the gel efficiently. SDS provides a uniform charge to all proteins so that they move through the gel based on size only. When SDS is used with proteins, all of the proteins become negatively charged by their attachment to the SDS anions. SDS denatures proteins by “wrapping around” the polypeptide backbone. SDS grade is of utmost importance: a protein stained background along individual gel tracts with indistinct or slightly distinct protein bands are indicative of old or poor quality SDS. The total protein transferred can then be visualized by staining the membrane with protein dyes. Visualizing a specific protein within a mixture of proteins is usually detected by immunochemical methods. For immunological detection of a specific protein, the unstained membrane is placed in a blocking buffer that contains detergent and protein that bind to all unoccupied sites on the nylon membrane. The membrane is then incubated in buffer that contains antibody to one (or more) of the blotted proteins. The antibody binds to the adsorbed protein (antigen) and subsequent washings removes unbound antibody. A second antibody that is covalently linked to an enzyme such as alkaline phosphatase or horseradish peroxidase is used for detection. The membrane is then incubated in a solution of the secondary antibody where it will bind selectively to the bound antigen-primary antibody complex. Following this treatment, the membrane is washed to remove the unbound secondary antibody-enzyme complex and is then incubated in a solution containing a phosphatase or peroxidase substrate. The products of the enzymatic reaction yield chromogenic (colored) products that are easily visible on the nylon membrane. PREPARATION OF AGAROSE GEL 1. To make 2.5% agarose in 1X gel buffer for a 7x7 cm size casting tray, add 0.5 gm of protein agarose powder to 20 mL volume of buffer. Swirl to disperse clumps. 2. With a marking pen, indicate the level of the solution volume on the outside of the flask. 3. Heat the mixture to dissolve the agarose powder. The final solution should be clear (like water) without any undissolved particles present. a. Microwave method: Cover flask loosely with plastic wrap to minimize evaporation. Do not cover tightly. Heat the mixture on High for 1 minute. Swirl the mixture and heat on High in bursts of 25 seconds until all the agarose is completely dissolved. b. Hot Plate method: Cover the flask with foil to minimize evaporation. Heat the mixture to boiling with occasional stirring. Boil until the agarose is completely dissolved. 4. Cool the agarose to 55°C with swirling to promote even dissipation of heat. If detectable evaporation has occurred, add hot distilled water to bring the volume of the solution up to the original volume as marked on the flask. 5. After the agarose solution has cooled to 55°C: Seal the ends of the gel tray with rubber dams or tape. Seal the tray with a bead of agarose if tape is used. 6. Pipet the cooled agarose solution into the bed. Make sure the bed is on a level surface. Place comb(s) in appropriate slots. 7. Allow the gel to solidify. It will become firm and ready for electrophoresis in approximately 20 minutes. PREPARATION OF MEMBRANES (Any time before the lab - required on DAY 1) Wear rinsed and dried lab gloves. Powders from gloves will interfere with the procedure. 1. Keep protective cover sheets around the membranes and make sure the cover sheets and membrane are all aligned. Keep the membrane covered this way during all the following steps. 2. Divide the covered membrane into six 7 x 7 cm squares by drawing pencil lines on the upper cover sheet. If you are using gels that are smaller or larger than 7 x 7 cm, you must adjust the dimensions of your membrane squares accordingly. You may also have to alter the sizes of the filter paper and towels the students prepare. Larger gels may necessitate fewer groups. 3. Cut the covered membranes on the lines to produce six squares. Make sure the sheets are aligned before cutting. PREPARATION OF BUFFERS AND STAINS (Required on DAY 1) Transfer Buffer 1. To 350 ml of distilled water, add 50 ml of 10X Tris-Glycine-SDS concentrate. 2. Add 100 ml of 95 - 100% methanol to the buffer. Mix. Keep tightly covered. Electrophoresis Buffer, Tris-glycine-SDS Buffer 1. Add 1 part EDVOTEK® 10X Tris-Glycine-SDS buffer to every 9 parts distilled water. 2. Make enough 1X buffer for all electrophoresis units used. Most of the standard electrophoresis units require between 300 - 400 ml (minimum) per unit. PREPARATION OF SAMPLES FOR ELECTROPHORESIS (Complete preparation on the day of the lab - Required first day) 1. Rehydrate the samples for electrophoresis (A-E) by adding 120 μl of distilled water to each tube. Incubate at room temperature for five minutes and vigorously mix. Use a waterresistant marker to label the tops of the tubes A-E in case the labels come off during boiling. 2. Wear safety goggles, in case the covers pop off due to heat. Make sure the tube caps are securely fastened. Suspend tubes A-E in a boiling water bath for 5 minutes. (It is not necessary to boil the markers, Component F.) Remove and let them cool to room temperature. Tap or briefly microcentrifuge to get condensate at the top of the tubes back into the sample. 3. Aliquot 20 μl of each sample (A-E) for each lab group. This experiment kit contains practice gel loading solution. If you are unfamiliar with gel electrophoresis, it is suggested that you practice loading the sample wells before performing the actual experiment. Do not use Methanol with acrylic materials. Methanol will destroy acrylic. Caution PREPARATION OF STAIN SOLUTION Make several days before the lab or on the day of the lab (required for DAY 3) 1. To 75 mL of distilled water, add 125 mL absolute methanol, 25 ml vinegar, and 25 mL Western Blot Stain™ concentrate. Mix thoroughly. 2. Pour the stain into a glass tray. Do not use acrylic. Day 1: Sample Preparation & Setting up the Electrophoresis. Day 2: Setting up the Western Blot (Capillary Action) Day 3: Processing and staining of the blot membrane, &bringing it all together. Teacher Assessment Lab report expanding on results and including future recommendations (graded by rubric). Teacher Expected Results • • • • • • A = Positive Control (phosphorylated p38) Normal cells = Positive/Band present B = Negative Control (non-phosphorylated p38) Anthrax treated cells = No Band C = Patient 1 (present at stadium) = Band Present/Negative for Infection *D = Patient 2 (10 miles of stadium) = No Band Present/Positive for Infection E = Patient 3 (present at stadium) = Band Present/Negative for Infection F = Standard Molecular Weight Dye Markers Students have shown that location and infection in this case are not necessarily related, however, the correlation between the lack of phosphorylated p38 protein in infected cells can be detected. A further confirmation of increased apoptosis in Patient 2 should be investigated. Science Lab Report Rubric Name: _______________________________ Excellent (20) Good (17) Satisfactory (15) Needs Improvement (12) Components of the Report All required All required elements are elements are present and present. additional elements that add to the report (e.g., thoughtful comments, graphics) have been added. One required Several required element is missing, elements are but additional missing. elements that add to the report (e.g., thoughtful comments, graphics) have been added. Question / Purpose The purpose of the lab or the question to be answered during the lab is clearly identified and stated. The purpose of the lab or the question to be answered during the lab is partially identified, and is stated in a somewhat unclear manner. Spelling, Punctuation, Grammar One or fewer errors in spelling, punctuation and grammar in the report. Drawings / Diagrams Clear, accurate diagrams are included and make the experiment easier to understand. Diagrams are labeled neatly and accurately. The purpose of the lab or the question to be answered during the lab is identified, but is stated in a somewhat unclear manner. Two or three errors in spelling, punctuation and grammar in the report. Four errors in spelling, punctuation and grammar in the report. Diagrams are Diagrams are included and are included and are labeled neatly and labeled. accurately. The purpose of the lab or the question to be answered during the lab is erroneous or irrelevant. More than four errors in spelling, punctuation and grammar in the report. Needed diagrams are missing OR are missing important labels. Error Analysis Experimental errors, their possible effects, and ways to reduce errors are discussed. Experimental errors and their possible effects are discussed. Summary Summary describes the skills learned, the information learned and future applications to real life situations. Summary describes the information learned and a possible application to a real life situation. Summary describes the information learned. No summary is written. Appearance / Organization Lab report is typed and uses headings and subheadings to visually organize the material. Lab report is neatly handwritten and uses headings to visually organize the material. Lab report is neatly written or typed, but formatting does not visually organize. Lab report is handwritten, looks sloppy with crossouts, multiple erasures and/or tears and creases. Background Sources Experimental errors are mentioned. There is no discussion of errors. Material is directly A few reputable A few background copied rather than background sources are used put into student's Several reputable sources are used and cited correctly, own words and/or background and cited but some are not background sources sources were used correctly. Material reputable sources. are cited incorrectly. and cited correctly. is translated into Material is Material is student's own translated into translated into words. student's own student's own words. words. Lesson 3: Zooming In: What in the toxin is causing cell death? (STUDENT Instructions) Western Blot Analysis Objectives: Understand the concepts and methodology involved with completion of a Western Blot Analyze Western Blot Analysis as a strategy to detection and lead to treatment of communicable and chronic diseases. Understand that this technique is testing proteins because of their role in cell signaling Introduction: Doctors in the scenario from Lesson 1 & 2 have sent a request to a CDC Lab to help them understand how the Anthrax toxin is affecting their patient’s cells. They are seeking a confirmation that the toxin is affecting cell signaling, in order to help guide them to potential treatment options. They sent over new patient samples that they believe are positive for Anthrax infection due to symptoms and they want the lab to test for the presence of phosphorylated p38. The sample group of patient serum they provided consists of three patients: 2 that were present at the football game where the bacteria was released, and 1 from the surrounding area. All are believed to have Anthrax infection due to the symptoms they are exhibiting. They believe that if non-phosphorylated p38 is present, this shows that the toxin is blocking the phosphorylation of p38 protein in a kinase signaling pathway, and instead of macrophage activation happening, this is the trigger for rapid cell death. LABORATORY SAFETY: Gloves and goggles should be worn routinely throughout the experiment as good laboratory practice. PROCEDURE: DAY ONE Part 1: Sample Preparation Take 5 of your microcentrifuge tubes and label them with permanent marker A – E. Aliquot 20 ul of each of the reagents A – E, that your teacher has prepared ahead of time, into each tube and put on ice. o A = Positive Control (phosphorylated p38) Normal cells o B = Negative Control (non-phosphorylated p38) Anthrax treated cells o C = Patient 1 (present at stadium) o D = Patient 2 (from within 10 miles of stadium) o E = Patient 3 (present at stadium) o F = Standard Molecular Weight Dye Markers Part 2: Setting up the Electrophoresis You will need the following at your lab station: o Protein Agarose 7x7 gel with wells (prepared by teacher) o Approximately 350 mL of 10x Tris-Glycine-SDS Buffer (Chamber Buffer) o 1, 10 ul micropipette with tips, or 8, 1 ml disposable Pipets o Electrophoresis Horizontal Apparatus and Power Supply o Samples from part 1 1. Remove 10 ul of sample A from the microcentrifuge tubes with your pipet. 2. Transfer the sample to the first well, taking care not to pierce the bottom of the well with the micropipet tip. Do not overload the wells. 3. Repeat the above procedure from left to right with remaining samples. Make sure to change tips on your pipet, or disposable pipets between samples! 4. Place your loaded gel, on a gel tray, in the center of the electrophoresis chamber. Position the well side of the gel near the negative electrode. 5. Add approximately 350 mL of Tris Buffer to the chamber until the level of buffer is 2mm above the top surface of the well. 6. Making sure that the cover and plugs are dry, slide the cover onto the electrophoresis chamber (red on +, black on -). 7. Making sure that the patch cords attached to the cover are dry, connect the red cord to the red electrode terminal on the power supply. Connect the black patch cord to the black electrode terminal on the power supply. 8. ONLY NOW, plug the cord in and run at 125 volts, 45 minutes if possible, or until the blue tracking dye has traveled at least 4 - 4.5 cm from the wells. 9. Unplug your apparatus, and carefully pour off buffer into waste container. Take out gel in case and wrap snugly in plastic wrap for use on day 2. DAY TWO Part 3: Setting up the Western Blot (Capillary Action) You will need the following at your lab station: o Gel from Day 1 o 1 Precut Western Blot Membrane (7 x 7 cm) o 2 Precut Blotting Filter Papers (7 x 7 cm) o Western Blot Stain™ o 20 mL of methanol in container with a cover o 2 trays that can hold up to 100 ml of liquid o Plastic wrap piece o Distilled water o Paper towels o 50 mL Diluted transfer buffer o Forceps o 1 mL disposable pipet o Pencil 1. Place a piece of plastic wrap on your bench top. Be sure it is smooth and flat. The filter paper, gel, membrane, and paper towels will be placed onto it to make the blotting sandwich. 2. Wearing gloves, carefully remove the cover sheets from the (white) Western Blot membrane. Using forceps, transfer the membrane to a plastic tray. 3. Pre-wet the membrane (7 x 7 cm) by immersing it in approximately 20 mL of 95-100% methanol for 10 seconds. Pour the methanol back in container to save. 4. Immediately pour 50 mL of distilled water onto membrane in tray and soak for about 5 minutes to remove the methanol (slightly agitate by sliding tray on table back and forth gently). 5. Pour off the water and immerse the membrane in 20 mL of diluted transfer buffer. Let the membrane sit until needed for the gel, at least 10 minutes. 6. Remove the gel from the plastic wrap and immerse into a separate tray that contains an additional 25 mL of transfer buffer. Soak for 10 to 15 minutes. 7. Saturate 1 piece of 7 x 7 cm filter paper with transfer buffer by dipping it into one of the trays. Place the filter paper on the plastic wrap on your bench. 8. Wear gloves and carefully remove the gel from the transfer buffer and place upside down on the filter paper. Roll a pencil over the surface to remove air bubbles that may be trapped under the gel. 9. Pipet 1 to 2 ml of transfer buffer over the top of the gel and place the Western Blot membrane over the gel. Roll a pencil over the surface to remove air bubbles. 10. Use a pencil to lightly trace the location of each of the bands in lane 6 onto the membrane. Beside each mark, indicate the color of the respective band. (B1 = Blue 1, B2 = Blue 2, P = Purple, and R = Red). 11. Saturate 1 piece of filter paper with transfer buffer by dipping it into one of the trays, and cover the membrane with the wet filter paper. Roll a pencil over the surface to remove air bubbles. 12. Add a second piece of dry filter paper to the top of the stack. Remove air bubbles. 13. Evenly place a stack of 7 x 7 cm paper towels 4 to 6 cm in thickness on top of the stack. 14. Place a plastic tray or plate on top of the stack. Place a light weight beaker (400 ml size) on top. Allow the protein transfer to proceed overnight or for a minimum of 4 hours. DAY THREE Part 4: Processing and staining of the blot membrane o 2 pieces of Filter paper o 20 mL of Methanol with cover o 100 mL Distilled water o Western blot stain o 2 Trays 1. Remove the tray, paper towels and filter paper from the top of the membrane. Leave the membrane in place on top of the gel. 2. Using a pencil, lightly trace the outline of each well and number according to loading sequence onto the membrane. (Remember the gel is upside down.) 3. Using forceps, remove the membrane from the gel and place it on a clean piece of filter paper. The side that was in contact with the gel should be facing up. 4. With a pencil, on one of the lower corners write “F” (for front). On the other corner, write your group number or initials. Place the membrane in a 65°C incubation oven for 10 minutes to fix the samples. 5. After 10 minutes, very briefly wet the membrane in methanol so that there are no dry areas. 6. Transfer the membrane to distilled water for about 5 minutes. 7. Immerse the membrane in the Western Blot Stain™ for 10-15 minutes with occasional agitation. 8. With forceps, transfer the membrane to a tray of Methanol and gently move the membrane in the alcohol to de-stain by sliding the tray gently back and forth on the table. Look for the positive control to appear. When the bands are evident, immediately transfer the membrane to a tray of distilled water. 9. After several minutes, remove membrane from the distilled water, lay on a piece of filter paper. 10. Compare the three patient results to the positive and negative controls. A B C D E F 140,000 110,000 90,000 70,000 Part 5: Setting a New Direction: Write a lab report according to class protocol, following the rubric provided. Research the following to include in your summary: o Role of p38 in the cell o Medications that may improve cell signaling o Ways available treat anthrax victims o Possibility of a vaccine production on a large scale o Suggestions for future research on Anthrax effects