© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
11
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 1
REPAIR OF INFRARENAL
ABDOMINAL AORTIC ANEURYSMS
Frank R. Arko, M.D., Stephen T. Smith, M.D., and Christopher K. Zarins, M.D., F.A.C.S.
An arterial aneurysm is defined as a permanent localized enlargement of an artery to a diameter more than 1.5 times its expected
diameter. Aneurysms are classified according to morphology, etiology, and anatomic site. The most common morphology is a
fusiform, symmetrical, circumferential enlargement that involves
all layers of the arterial wall. A saccular morphology is also seen,
in which aneurysmal degeneration affects only part of the arterial
circumference.
The most common cause of an arterial aneurysm is atherosclerotic degeneration of the arterial wall.The pathogenesis is a multifactorial process involving genetic predisposition, aging, atherosclerosis, inflammation, and localized activation of proteolytic
enzymes. Most aneurysms occur in elderly persons, and the prevalence rises with increasing age. Aneurysms also occur in genetically susceptible individuals with Ehlers-Danlos syndrome or Marfan
syndrome. Other causes include tertiary syphilis and localized
infection resulting in a mycotic aneurysm.
Aneurysms of the infrarenal aorta are by far the most common
arterial aneurysms encountered in clinical practice today: they are
three to seven times more common than thoracic aneurysms and
affect four times as many men as women.1 Abdominal aortic
aneurysms (AAAs) have a tendency to enlarge and rupture, causing death. In the United States, AAAs result in approximately
15,000 deaths each year and are thus the 13th leading cause of
death.2,3 The only way to reduce the death rate is to identify and
treat aortic aneurysms before they rupture [see 6:3 Pulsatile Abdominal Mass].
The relationship between aneurysm size and risk of rupture is
well known.The annual risk of rupture is 1% to 2% for aneurysms
less than 5 cm in diameter, 10% for aneurysms 5 to 6 cm in diameter, and 25% or higher for aneurysms larger than 6 cm.4 Although
large aneurysms are much more likely to rupture than small
aneurysms, small aneurysms can and do rupture on occasion.
The exact size at which an asymptomatic small AAA should be
treated remains unsettled. This issue was the subject of two
prospective, randomized clinical trials: the United Kingdom Small
Aneurysm Trial5 and the Aneurysm Detection And Management
(ADAM) Veterans Affairs (VA) Cooperative Study.6 Both trials
randomly assigned low-risk patients with small (4.0 to 5.4 cm)
AAAs to either open surgical repair or ultrasound surveillance.
Patients in the surveillance groups were closely monitored with
serial ultrasound examinations and underwent open surgical repair
if the aneurysm enlarged, became tender to palpation, or became
symptomatic. With respect to the primary end point—overall survival—the two trials came to similar conclusions: there was no difference in overall survival between the surgery group and the surveillance group.5,6 There was, however, a late survival benefit in the
surgery group in the U.K. Small Aneurysm Trial.7
Aneurysm rupture rates were low (1%) in both trials, leading
many clinicians to conclude that aneurysms smaller than 5.5 cm
need not be treated, because the risk of rupture is so low. Closer
examination of the data, however, reveals that more than 60% of
the patients in the surveillance groups underwent open surgical
repair during the two trials: 81% of patients with 5.0 to 5.4 cm
aneurysms in the ADAM trial underwent surgery, and almost all
patients in the U.K. trial ultimately required surgical management.
Thus, it is likely that the reason for the low rupture risk in these trials was that surgical treatment of the aneurysm was provided when
clinically indicated. This conclusion is supported by data from a
prospective study of patients from the VA hospitals involved in the
ADAM trial who were not eligible for randomization and did not
undergo operative repair. In these patients, the 1-year risk of rupture for slightly larger (5.5 to 5.9 cm) aneurysms was 9.4%.8
Furthermore, very close surveillance with ultrasound examinations every 3 to 6 months did not prevent aneurysm rupture in 1%
of patients. Thus, the decision whether to treat an aneurysm is
based on assessment of the risk of aneurysm rupture relative to the
risk associated with treatment rather than on an absolute size criterion or a surveillance protocol.
Open Repair
PREOPERATIVE EVALUATION
Identification of Risk Factors
For successful surgical reconstruction of AAAs, any significant
comorbidities that would increase the risk of operative repair must
be identified and managed at an early stage. Patients undergoing
the procedure usually are elderly and often have coexisting cardiac, pulmonary, cerebrovascular, renal, or peripheral vascular disease. The major anesthetic risk factors for elective resection of
AAAs are similar to those for other major intra-abdominal operations; in particular, they include inadequate cardiopulmonary and
renal function. Patients with unstable angina or angina at rest, a
cardiac ejection fraction of less than 25%, a serum creatinine concentration higher than 3 mg/dl, or pulmonary disease (manifested
by arterial oxygen tension < 50 mm Hg, elevated arterial carbon
dioxide tension, or both on room air) are considered to be at high
risk.9,10
Myocardial ischemia is the most common cause of perioperative
morbidity and mortality after arterial reconstruction of the aorta.
Optimization of preoperative medical management, perioperative
invasive monitoring, and long-term risk-factor modification are all
facilitated by an accurate preoperative cardiac evaluation. Such
evaluation may include transthoracic echocardiography, exercise
stress testing, myocardial scintigraphy, stress echocardiography,
and coronary angiography; each test has its own merits and limitations with regard to clinical risk assessment.
There has been considerable controversy over the potential benefit of preoperative coronary revascularization in this setting. This
issue was addressed by a clinical trial in which patients requiring
AAA or peripheral vascular surgery who had high-risk cardiac disease were randomly assigned to undergo either vascular surgery
without preoperative coronary revascularization or coronary revascularization followed by vascular surgery.11 There was no differ-
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 2
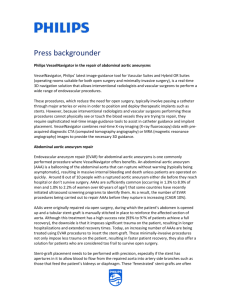
Figure 1 Duplex ultrasonography may be used as a screening
test and to determine the actual size of the aneurysm.
ence between the two groups with respect to the incidence of postoperative MI or overall mortality.The investigators concluded that
patients with stable coronary disease do not benefit from preoperative coronary revascularization. Patients with unstable severe
coronary disease may benefit from invasive cardiac evaluation and
preliminary coronary intervention.
To reduce the mortality associated with resection of AAAs, it is
necessary not only to identify high-risk groups but also to institute
appropriate preoperative, intraoperative, and postoperative alterations in patient care.With intensive perioperative monitoring and
support in place, resection of AAAs has been successfully performed even in high-risk patients, with operative mortalities of less
than 6%.12-14
lower-extremity occlusive disease. There are risks associated with
aortography that place some restrictions on its use. Among these
risks are the potential renal toxicity resulting from the use of contrast agents. In addition, manipulation of catheters through the
laminated mural thrombus increases the risk of distal embolization. Finally, local arterial complications may arise at the arterial
puncture site.
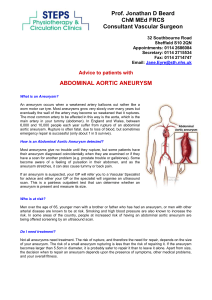
CT provides reliable information about the size of the entire
aorta, thereby allowing accurate determination of both the size
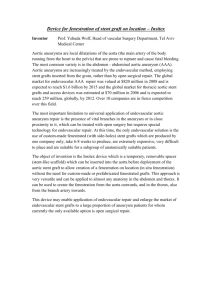
and the extent of the AAA [see Figure 2]. Spiral CT scanning permits identification of the visceral and renal arteries and their relationship to the aneurysm. The administration of I.V. contrast
material allows assessment of the aortic lumen, the amount and
location of mural thrombus, and the presence or absence of
retroperitoneal hematoma [see Figure 3]. Overall, spiral CT is currently the most useful imaging method for evaluation of the
abdominal aorta.
MRI is also useful in the preoperative evaluation of aortic
aneurysms.18,19 It employs radiofrequency energy and a magnetic
field to produce images in longitudinal, transverse, and coronal
planes.The advantages of MRI over CT are that no ionizing radiation is administered, multiplane images can be obtained, and no
nephrotoxic contrast agents are used.
Classification of Patients for Elective or Urgent Repair
Patients may usefully be classified into three categories according to how they present for repair: (1) elective patients, (2) symptomatic patients, and (3) patients with ruptured aneurysms.
Confirmation of Diagnosis and Determination of Aneurysm Size
Physical examination suffices for detection of most large
aneurysms. To determine the exact size of the aneurysm and to
identify smaller aneurysms, however, more objective methods are
available and should be used. Determination of the size of the
aneurysm is extremely important because size is the most important determinant of the likelihood of rupture and plays a crucial
role in subsequent management decisions. Imaging modalities
commonly employed to diagnose and measure aneurysms include
duplex ultrasonography (DUS), aortography, computed tomography, and magnetic resonance imaging.
The main advantages of DUS are its ready availability in both
inpatient and outpatient settings, its low cost, its safety, and its
good performance; many studies have documented the ability of
DUS to establish the diagnosis and accurately determine the size
of AAAs [see Figure 1].15-17 The primary limitations of DUS are
that imaging of the thoracic and suprarenal aorta is poor, that the
quality of the images is considerably lower in the presence of obesity or large amounts of intestinal gas, and that it must be performed by a skilled imaging technician.
Aortography yields excellent images of the contours of the aortic lumen, but it is not a reliable method for determining the diameter of an aneurysm or even for establishing its presence, because
the mural thrombus within the aneurysm tends to reduce the
lumen to near-normal size. Nonetheless, aortography can be helpful in determining the extent of an aneurysm (especially when
there is iliac or suprarenal involvement), defining associated arterial lesions involving the renal and visceral arteries, and detecting
Figure 2 Shown is a CT angiogram providing a three-dimensional reconstruction of an infrarenal AAA after endovascular
repair. Of particular interest is the relation of the graft to the
renal arteries and the hypogastric arteries distally.
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 3
Figure 3 CT scanning assesses the size of the aneurysm, the amount of mural thrombus present, and the relation of other intra-abdominal structures to the aneurysm.
Elective aneurysm repair is recommended for asymptomatic
patients who have aneurysms 5.0 cm in diameter or larger, who
have an acceptable level of operative risk, and who have a life
expectancy of 1 year or more. Furthermore, elective operation
should be considered for patients with aneurysms smaller than 5.0
cm who are not at high operative risk if they are hypertensive or live
in a remote area where proper medical care is not readily available.
Repair is also appropriate for aneurysms that are between 4.0 and
5.0 cm in diameter and have shown growth of more than 0.5 cm
on serial images in less than 6 to 12 months. Peripheral embolization originating from the aneurysm is an indication for repair,
regardless of the size of the aneurysm.
Urgent operation is indicated for patients with symptomatic
aneurysms, regardless of the size of the aneurysm. Such patients
typically present with abdominal or back pain. Sometimes, the
back pain radiates to the groin, much as in ureteral colic; this pain
may be elicited by palpating the aneurysm. In most cases, DUS,
CT, and MRI will reliably detect the presence of periaortic blood;
however, the absence of this finding should not delay operation,
because actual rupture of the aneurysm can occur at any time.
Emergency operation is indicated for almost all patients with
known or suspected rupture of an aneurysm.
aneurysm repair. Consideration of endovascular aneurysm repair
(EVAR) does introduce certain morphologic criteria into the
process of patient selection, in that stent grafting is appropriate
only for patients in whom the infrarenal neck and the iliac arteries
are suitable.
Given that the long-term outcome of endovascular grafting is
currently unknown, younger patients who are at low operative risk
and are expected to survive into the long term are typically better
served with open surgical repair. In addition, patients who require
additional abdominal or pelvic revascularization procedures, who
have small or diseased access vessels, or who have short (< 10 mm)
or tortuous infrarenal necks are not candidates for endovascular
grafting and should undergo open surgical repair instead.
Preoperative preparation to optimize cardiopulmonary function,
administration of preoperative antibiotics, and intraoperative hemodynamic monitoring with appropriate fluid management can significantly reduce the risks associated with AAA repair. Before aortic
cross-clamping, appropriate volume loading, combined with vasodilatation, is carried out to help prevent declamping hypotension.
OPERATIVE PLANNING
Open surgical repair of infrarenal AAAs is performed through a
transperitoneal or retroperitoneal exposure of the aorta with the
patient under general endotracheal anesthesia.The aneurysm may
be exposed through either a long midline incision (for the
transperitoneal approach) or an oblique flank incision (for the
retroperitoneal approach) [see Figure 4a]. An upper abdominal
transverse incision may also be used for either retroperitoneal or
transperitoneal exposure. The results with the two exposures are
equivalent. The transperitoneal approach is preferred when exposure of the right renal artery is required and when access to the distal right iliac system or to intra-abdominal organs is necessary.The
retroperitoneal exposure offers advantages when extensive peritoneal adhesions, an intestinal stoma, or severe pulmonary disease
is present and when there is a need for suprarenal exposure. Use
of the retroperitoneal approach has been associated with a shorter
Preoperative planning is essential for a successful outcome after
repair of an infrarenal AAA. Like the choice between elective and
urgent or emergency repair, operative planning is governed by the
presentation of the patient. In patients with ruptured aneurysms,
diagnosis is immediately followed by operative repair. In patients
with symptomatic aneurysms, the amount of preoperative imaging
done is balanced against the risk of impending rupture. In patients
presenting for elective repair, it is generally possible to perform
extensive imaging to determine whether the repair is best done via
an endovascular approach [see Endovascular Repair, below] or a
standard open approach. Current preoperative imaging methods
utilizing CT angiography (CTA) obviate several common pitfalls.
The availability of endovascular techniques for excluding an
aneurysm should not alter the patient selection criteria for
OPERATIVE TECHNIQUE
Step 1: Initial Incision and Choice of Approach
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 4
a
Renal Vein
b
Inferior
Mesenteric Vein
Inferior
Mesenteric
Artery
Ureter
Iliac Vein
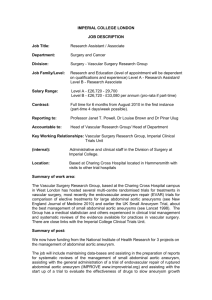
Figure 4 Open repair of infrarenal AAAs. (a) For the transabdominal approach to the abdominal aorta, a
midline or transverse incision is appropriate. For the retroperitoneal approach, an oblique flank incision
may be used. (b) The small intestine (including the duodenum) is retracted laterally after the ligament of
Treitz is mobilized, and the retroperitoneum is incised in the midline. The left renal vein is the landmark
for the infrarenal neck.
duration of postoperative ileus, a lower incidence of pulmonary
complications, and a reduction in length of stay in the ICU.
Step 2 (Transperitoneal Approach): Exposure and Control of
Aorta and Iliac Arteries
When the transperitoneal approach is taken, the small bowel
(including the duodenum) is retracted to the right, and the
retroperitoneum overlying the aneurysm is divided to the left of the
midline [see Figure 4b].The duodenum is completely mobilized, and
the left renal vein is identified and exposed. The normal infrarenal
neck, which is just below the left renal vein, is then exposed and
encircled for proximal control. Both common iliac arteries are
mobilized and controlled, with care taken to avoid the underlying
iliac veins and ureters that cross over at the iliac bifurcation [see
Figure 5]. If the common iliac arteries are aneurysmal, then both the
internal and the external iliac arteries are controlled. The inferior
mesenteric artery is then dissected out and controlled for possible
reimplantation into the graft after the aneurysm has been repaired.
Step 2 (Retroperitoneal Approach): Exposure and Control of
Aorta and Iliac Arteries
When the retroperitoneal approach is taken, a transverse left
abdominal or flank incision is made, and the peritoneum is reflected anteriorly. The left kidney usually is left in place but may be
mobilized anteriorly to expose the posterolateral aorta. Exposure
of the right iliac system can be achieved by dividing the inferior
mesenteric artery early in the course of dissection. The aorta and
the iliac arteries are controlled in essentially the same fashion
regardless of the type of incision used.
Step 3: Opening of Aneurysm and Creation of Proximal
Anastomosis
Systemic anticoagulation with I.V. heparin is then performed.
After sufficient time (3 to 5 minutes) has elapsed to permit adequate circulation, the infrarenal neck and the iliac arteries are
clamped. To prevent distal embolization, the distal clamps should
be applied before the proximal aortic clamp.The aneurysm is then
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 5
opened longitudinally, the mural thrombus is removed, and backbleeding lumbar arteries are oversewn. Depending on its degree of
backflow and on the patency of the hypogastric arteries, the inferior mesenteric artery may be either ligated or clamped and left with
a rim of aortic wall for subsequent reimplantation [see Troubleshooting, below].
The aortic neck is then partially or completely transected, and an
appropriately sized tubular or bifurcated graft is sutured to the aorta
with a continuous nonabsorbable monofilament suture [see Figure
6]. When the proximal aortic neck is very short, suprarenal aortic
clamping may be required for performance of the proximal anastomosis. If suprarenal clamping is necessary, the security of the proximal anastomosis should be verified, and the clamp should then be
moved onto the graft below the renal arteries as soon as possible to
minimize renal ischemia. If the aorta is especially weak or friable,
the anastomosis may be supported with Teflon-felt pledgets.
Step 4: Creation of Distal Anastomosis
When the aneurysm is confined to the aorta, the distal anastomosis is performed by suturing a straight tube graft to the aortic
a
b
c
Figure 5 Open repair of infrarenal AAAs. (a) Once the aneurysm is exposed, proximal control is obtained by encircling the proximal neck with an umbilical tape or heavy Silastic. The inferior mesenteric artery is identified and then
either clamped or ligated for possible reimplantation at the end of the procedure. (b) The iliac arteries are dissected
free, systemic heparin anticoagulation is instituted, and distal control is obtained, followed by proximal control to
prevent distal embolization. The aneurysm sac is then opened longitudinally. (c) All mural thrombus is removed, and
the proximal and distal necks of the aorta are incised.
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 6
a
c
b
d
e
bifurcation [see Figure 7]; straight tube graft reconstructions are
used about 30% of the time. Distally, the dissection should avoid
the fibroareolar tissue overlying the left common iliac artery
because this tissue contains branches of the inferior mesenteric
artery and the autonomic nerves that control sexual function in
men.
When the aneurysm extends into the common iliac arteries, the
distal anastomosis is accomplished by suturing a bifurcated graft to
the distal common iliac arteries or, in the case of significant occlusive disease, to the common femoral arteries. In these situations,
control of the iliac arteries is best achieved by mobilizing the external and internal arteries and clamping them individually [see Figure
8]. It is sometimes easier to control iliac artery back-bleeding by
using intraluminal balloon catheters and oversewing the common
iliac arteries from within the opened aortic or iliac aneurysms.
Care must be taken not to injure the accompanying venous structures or the ureters, which cross anterior to the iliac bifurcation.
Figure 6 Open repair of infrarenal AAAs.
(a) Back-bleeding lumbar arteries are
oversewn with figure-eight sutures to control bleeding. (b, c, d) The proximal anastomosis is sewn to the back wall of the aorta
with a continuous nonabsorbable monofilament suture. (e) If the aorta is weak or friable, Teflon-felt pledgets may be used for
additional support.
Every effort should be made to ensure perfusion of at least one
hypogastric artery to help minimize the risk of postoperative left
colon ischemia.
Declamping hypotension may occur after reperfusion of the
lower extremities. It is essential to maintain communication with
the anesthesiologist so that blood and fluid replacement can be
adjusted in anticipation of lower-extremity reperfusion. Even
though the graft and vessels are flushed and back-bled before distal flow is reestablished, it is preferable first to establish flow into
one of the hypogastric arteries so as to minimize the chances of distal embolization to the legs.
Before the abdomen is closed, adequate perfusion of the lower
extremities and the left colon should be ensured via either direct
inspection or noninvasive monitoring. The open aneurysm sac is
then sutured closed over the aortic graft to separate the graft from
the duodenum and the viscera [see Figure 9].This step reduces the
risk of aortoenteric fistula.
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 7
Troubleshooting
If the inferior mesenteric artery is small and back-bleeding is adequate, it may be ligated [see Figure 10a]; however, if the vessel is large
or back-bleeding is meager, it should be reimplanted. Reimplantation of the inferior mesenteric artery can be accomplished with relative ease by using the Carrel patch technique. After the graft has
been completely sewn to the aorta, a partial occluding clamp is
placed on the main body of the graft or on one of the limbs. An
opening in the graft is then created, and an end-to-side anastomosis
[see Figure 10b]—with an interposition graft added if necessary [see
Figure 10c]—is used to reconstruct the inferior mesenteric artery.
This anastomosis is created with a continuous monofilament suture.
SPECIAL CONSIDERATIONS
Concurrent Disease Processes
Figure 7 Open repair of infrarenal AAAs. When the aneurysm
does not extend into the iliac arteries, a straight tube graft is
used. The distal anastomosis is completed with a continuous
suture. Before completion of the anastomosis, the graft is flushed
by back-bleeding the iliac arteries and flushing the proximal
anastomosis.
a
At times, a concurrent disease process complicates repair of an
AAA.The most common problems encountered are hepatobiliary,
pancreatic, gastrointestinal, gynecologic, and genitourinary disorders. Careful evaluation of the situation is necessary to determine
whether to treat the two disease entities concurrently. As a rule, the
more life-threatening disorder is treated first.
There are three key points that should be remembered in the
management of patients with AAAs and concurrent diseases. First,
a careful preoperative diagnostic workup usually detects any concomitant disease processes. Second, in emergency situations such as
ruptured or symptomatic aneurysms, the aneurysm always takes
priority unless the other condition is life-threatening and the
aneurysm clearly is not the cause of the critical symptoms. Finally,
many concomitant intra-abdominal problems can be avoided by
taking an endovascular approach.
b
Figure 8 Open repair of infrarenal AAAs. When the common iliac arteries are aneurysmal, both the internal and the
external iliac arteries must be clamped individually (a), and a bifurcated graft is sewn to the iliac arteries bilaterally (b).
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 8
incidence is quite low. Left renal vein variants, such as retroaortic
left renal veins and circumaortic venous rings, are the most commonly seen venous anomalies.22 Azygous continuation of the inferior vena cava and bilateral inferior vena cava have also been noted.
Unnecessary bleeding can be prevented by means of careful dissection and meticulous technique.
Inflammatory Aneurysm
Approximately 5% of infrarenal AAAs are inflammatory.23 These
AAAs have a dense fibroinflammatory rind that typically adheres to
the fourth portion of the duodenum; they may also involve the inferior vena cava, the left renal vein, or the ureters. Patients with
inflammatory AAAs typically experience abdominal or flank pain
and may present with weight loss. The erythrocyte sedimentation
rate is usually elevated as well. Inflammatory aneurysms rarely rupture, because most are symptomatic and consequently are treated
before rupture can occur. Repair of inflammatory aneurysms poses technical problems because of the involvement of adjacent structures. A retroperitoneal approach is usually advocated for
these aneurysms.
Ruptured Aneurysm
Figure 9 Open repair of infrarenal AAAs. Once the anastomoses
have been completed and adequate flow to the lower extremities
and the left colon has been confirmed, the open aneurysm sac is
sutured closed over the aortic graft.
Anatomic Variants
Several anatomic variants may be encountered during repair of
AAAs, including horseshoe kidney, accessory renal arteries, and
venous anomalies.
Horseshoe kidney The incidence of horseshoe kidney in the
general population is less than 3%. Most patients with horseshoe
kidneys have between three and five renal arteries.20 To preserve
renal function, renal arteries arising from the aneurysm should be
reimplanted. In patients with horseshoe kidneys who have more
than five renal arteries, there often are multiple small accessory
arteries, some of which originate from the aneurysm, the iliac arteries, or both.
The presence of a horseshoe kidney may complicate—but does
not preclude—an anterior approach to repair of an infrarenal
AAA.21 In such cases, the left retroperitoneal approach provides
excellent exposure of the infrarenal aorta. This approach requires
that the surgeon dissect the space between the aneurysm and the
left portion and isthmus of the kidney; the kidney can then be
reflected to the right and the aneurysm fully exposed. The left
ureter crosses the iliac arteries from the right in this position, and
duplication of ureters may be noted.
Venous anomalies A number of different venous anomalies
may be observed in the course of AAA repair; however, the overall
Infrarenal AAAs can rupture freely into the peritoneal cavity or
into the retroperitoneum. Free rupture into the peritoneal cavity is
usually anterior and is typically accompanied by immediate hemodynamic collapse and a very high mortality. Retroperitoneal ruptures are usually posterior and may be contained by the psoas muscle and adjacent periaortic and perivertebral tissue. This type of
rupture may occur without significant blood loss initially, and the
patient may be hemodynamically stable.
When an aortic aneurysm ruptures, immediate surgical repair is
indicated. If the patient is unstable and either an abdominal aortic
aneurysm was previously diagnosed or a palpable abdominal mass
is present, no further evaluation is necessary and the patient should
be taken directly to the OR. If the patient is stable and the diagnosis is questionable, CT scanning may be performed to confirm the
presence of an aneurysm and determine its extent, the site of the
rupture, and the degree of iliac involvement. Bedside ultrasonography may also be used for quick confirmation of the presence of an
AAA.
Surgical repair of ruptured aneurysms is performed via a
transperitoneal approach. In cases of contained rupture, supraceliac control should be achieved before infrarenal dissection; once the
neck of the aneurysm has been dissected free, the aortic clamp may
be moved to the infrarenal level. In cases of free rupture, efforts to
obtain vascular control may include compression of the aorta at the
hiatus and infrarenal control with a clamp or an intraluminal balloon. Once proximal and distal control have been achieved, the
operation is conducted in much the same way as an elective repair.
OUTCOME EVALUATION
The mortality associated with repair of AAAs has been greatly
reduced by improvements in preoperative evaluation and perioperative care: leading centers currently report death rates ranging from
0% to 5%.24 Mortality after repair of inflammatory aneurysms and
after emergency repair of symptomatic nonruptured aneurysms
continues to be somewhat higher (5% to 10%), primarily as a consequence of less thorough preoperative evaluation.
Overall morbidity after elective aneurysm repair ranges from
10% to 30%. The most common complication is myocardial
ischemia, and MI is the most common cause of postoperative
death. Mild renal insufficiency is the second most frequent com-
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 9
c
a
b
Figure 10 Open repair of infrarenal AAAs. (a) A small, adequately back-bleeding inferior mesenteric artery may be ligated. (b) A large or meagerly back-bleeding inferior mesenteric artery should be reimplanted. A side-biting clamp is
applied to the graft, and an end-to-side anastomosis is created with a fine monofilament suture. (c) If the inferior mesenteric artery is not long enough for a direct anastomosis, an interposition graft—either a segment of a vein or a prosthetic
graft—may be used for added length.
plication, occurring after 6% of elective aneurysm repairs; however, severe renal failure necessitating dialysis is rare in this setting.
The third most common complication is pulmonary disease; the
incidence of postoperative pneumonia is approximately 5%.
Postoperative bleeding may occur as well. Common sources of
such bleeding include the anastomotic suture lines, inadequately
recognized venous injuries, and coagulopathies resulting from
intraoperative hypothermia or excessive blood loss. Any evidence of
ongoing bleeding is an indication for early exploration.
Lower-extremity ischemia may occur as a result of either emboli
or thrombosis of the graft and may necessitate reoperation and
thrombectomy. So-called trash foot may also develop when diffuse
microemboli are carried into the distal circulation.
Colon ischemia develops after 1% of elective aneurysm repairs.
Patients usually present with bloody diarrhea, abdominal pain, a
distended abdomen, and leukocytosis. The diagnosis is confirmed
by sigmoidoscopy, which reveals mucosal sloughing. In cases of
transmural colonic necrosis, colon resection and exteriorization of
stomas are warranted.
Paraplegia is rare after repair of infrarenal AAAs: the incidence is
only 0.2%. Most instances of paraplegia occur after repair of a ruptured aneurysm or when the pelvis has been devascularized. The
majority of patients recover at least some degree of neurologic
function.
Late complications (e.g., pseudoaneurysms at the suture lines,
graft or graft limb thrombosis, and graft infection) may occur but
are extremely rare. Graft infection may be associated with graftenteric fistula and is notoriously difficult to diagnose and treat.
Long-term survival in patients who have undergone successful
AAA repair is reduced in comparison with that in the general population. The 5-year survival rate after AAA repair is 67% (range,
49% to 84%), compared with 80% to 85% in age-matched control
subjects, and the mean duration of survival after AAA repair is 7.4
years. Part of the difference in survival can be attributed to associated coronary disease in patients with aneurysms. Late deaths
result primarily from cardiac causes.
Endovascular Repair
Endovascular repair was introduced during the 1990s as a less
invasive approach to treating infrarenal AAAs. In this approach, a
stent-graft is placed endoluminally via bilateral groin incisions;
thus, there is no need for a major abdominal incision and aortic
clamping. The results to date have been promising: blood loss is
decreased, hospital stay is shortened, and earlier return to function
is achieved. Not all patients are candidates for endovascular repair,
however. In September 1999, the Food and Drug Administration
approved two stent-graft devices for use in surgical management of
AAAs: the Ancure device (Guidant, Indianapolis, Indiana), which
is a balloon-expandable one-piece bifurcated stent-graft, and the
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 10
a
b
c
d
Figure 11 Endovascular repair of infrarenal AAAs. (a) The main bifurcated stent-graft
is advanced through the aortoiliac system under fluoroscopic guidance. (b) The sheath
over the stent-graft is retracted under fluoroscopic guidance. Controlled deployment
allows the graft to be gradually positioned directly below the renal arteries. (c) With the
main body of the stent-graft deployed, the contralateral limb is cannulated. Once this is
done, the contralateral limb is positioned within the junction gate and the common iliac
artery. (d) Shown is proper deployment of the stent-graft within the aortoiliac system,
with good proximal and distal fixation of the stent to the arterial wall.
AneuRx device (Medtronic AVE, Santa Rosa, California), which is
a self-expanding bifurcated modular device that is fully supported
externally by a nitinol stent. Subsequently, the FDA approved
three more devices for endovascular repair of AAAs: the Excluder
Bifurcated Endoprosthesis (W. L. Gore and Associates, Flagstaff,
Arizona), in November 2002, the Zenith AAA Endovascular Graft
(Cook Incorporated, Bloomington, Indiana), in May 2003, and
the Endologix Powerlink System (Endologix Incorporated, Irvine,
California), in November 2004. The Ancure device is no longer
available.
PREOPERATIVE PREPARATION
Precise preoperative evaluation that yields accurate measurements will result in proper planning and effective prevention of
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 11
problems. Both CTA and contrast biplane angiography are used
for this purpose. Of the two, spiral CTA is currently preferred.This
imaging modality is capable of obtaining high-quality images of
the vascular anatomy and reconfiguring them into detailed threedimensional images. For optimal evaluation, images should be
obtained at 1.5 to 3 mm intervals from the celiac artery to the
femoral arteries. Spiral CTA accurately defines the proximal and
distal characteristics of the AAA, as well as detects any significant
renal, visceral, or iliac occlusive disease. It is particularly helpful in
defining the infrarenal neck between the renal arteries and the
proximal portion of the aneurysm.
Angiography is employed as a complement to spiral CTA in this
setting. An arteriogram is useful in that it helps define renal,
mesenteric, and distal arterial anatomy; helps characterize tortuosity, calcification, and stenoses in access arteries; and helps determine the angles between the aorta, the proximal neck, and the
aneurysm.
Intravascular ultrasonography (IVUS) is a useful intraoperative
imaging adjunct in the process of sizing and selecting endograft
components. It can be used to measure vessel diameters and landing zone lengths, as well as to determine the amount of mural
thrombus in the aneurysm neck. In patients with severe renal
insufficiency, IVUS is used primarily to identify the renal and
hypogastric arteries, allowing the endograft to be deployed with
minimal or no resort to angiography.
Proper patient selection is mandatory for successful outcome.
The common femoral arteries must be large enough to accept a
delivery system larger than 21 French. The proximal infrarenal
aortic neck must be suitable for device implantation—that is, its
diameter must be between 16 and 28 mm, and its length should
be at least 15 mm. The common iliac artery implantation should
be carried out as close to the iliac bifurcation as possible to
increase the columnar strength of the implanted device. The iliac
artery diameter must be between 8 and 20 mm. In patients with
iliac artery aneurysms, it is possible to land the end of the stent in
the external iliac artery and thereby exclude one internal iliac
artery. Exclusion of both internal iliac arteries should be avoided
so as to prevent ischemic sequelae (e.g., buttock claudication,
colon ischemia, and erectile dysfunction). Coil embolization may
be performed in conjunction with EVAR to treat internal iliac
aneurysms. However, a waiting period of several weeks between
coil embolization of a hypogastric artery on one side and the same
procedure on the other side should be considered to allow recruitment of collateral vessels and reduce the incidence of pelvic
ischemia.
TECHNIQUE
The methods and technical principles we briefly describe here
derive from the personal experience of two surgeons (F.R.A and
C.K.Z) with more than 1,000 modular implants. The ensuing
technical description is not intended to be exhaustive, nor is it
meant as a substitute for the instructions provided by any of the
manufacturers.
The patient is placed under epidural or general anesthesia.
Bilateral femoral artery cutdowns are performed through transverse groin incisions to allow exposure of the common femoral
artery from the inguinal ligament to the femoral bifurcation.
Proximal control of the femoral arteries is obtained with umbilical
tapes. Systemic anticoagulation with I.V. heparin is instituted to
prolong the activated clotting time (ACT) to greater than 250 seconds.The ACT is monitored and maintained at this level throughout the procedure, and additional heparin is given as needed.
The femoral arteries are cannulated with an 18-gauge needle,
and 0.035-in. guide wires are placed bilaterally under fluoroscopic guidance; 10 French sheaths are then placed over the two guide
wires and advanced into the aneurysm under fluoroscopic guidance. A superstiff 0.035-in. guide wire 260 cm in length is inserted into the thoracic aorta, usually from the right limb. In the contralateral iliac artery, a pigtail catheter is placed just above the level
of the renal arteries, and an initial roadmapping aortogram is
obtained.The 10 French sheath in the right femoral artery is then
exchanged for the device, which is placed over the superstiff guide
wire and carefully advanced into the proximal infrarenal aorta
under fluoroscopic guidance, then into the perirenal aorta [see
Figure 11a]. A second aortogram is performed to verify the position of the renal arteries. Under fluoroscopic guidance, the stentgraft is then gradually deployed by retracting the outer sheath and
allowing the graft to expand, and it is positioned directly below the
level of the renal arteries [see Figure 11b].
Once the main bifurcation module has been deployed, the 10
French sheath in the contralateral iliac artery is pulled back, and a
0.035-in. angled hydrophilic wire and a guide catheter are inserted into the contralateral limb of the bifurcation module.The hydrophilic wire is then exchanged for a superstiff guide wire, over which
the contralateral limb is then advanced through the sheath into the
contralateral vessel and deployed [see Figure 11c]. A final aortogram is then performed to confirm that a satisfactory technical
result has been achieved [see Figure 11d]. Proximal and distal extender cuffs may be placed if necessary.The femoral arteriotomies
are repaired, and lower-extremity perfusion is reestablished.
OUTCOME EVALUATION
EVAR is significantly less invasive than open surgical repair and
consequently is associated with a significant reduction in major
procedure-related morbidity. Prospective clinical trials comparing
open AAA repair with EVAR have consistently found that patients
undergoing the latter experience less intraoperative blood loss,
need less postoperative ICU care, have shorter lengths of stay, and
regain normal function earlier.25,26 Procedure-related mortality
after EVAR is 1% to 2%, which is essentially equivalent to that
reported after open repair in prospective clinical trials but lower
than the 5% mortality reported after open repair in most multicenter studies.27,28
In the past few years, two randomized, controlled trials comparing EVAR with open AAA repair have been published. The
Dutch Randomized Endovascular Aneurysm Management
(DREAM) trial found EVAR to have a significant advantage in the
first 30 days, with reduced mortality and a lower incidence of
severe complications.29 This survival advantage was not sustained,
however, and at 1 year, there was no difference between EVAR and
open AAA repair. The EVAR 1 trial, carried out in the United
Kingdom, found EVAR to yield a similar reduction in 30-day mortality.30 Again, this survival advantage was not sustained, and at 4
years, there was no difference between EVAR and open repair in
terms of overall mortality or health-related quality of life. EVAR
did, however, have a significant advantage over open AAA repair
with regard to 4-year aneurysm-related mortality. The impact of
this advantage will continue to be assessed as this trial’s follow-up
period lengthens.
On occasion, EVAR fails to exclude blood flow from the
aneurysm sac completely.This condition, known as endoleak, may
arise from an incomplete seal at the site where the endograft is
affixed to the aortic neck or the iliac arteries (type I endoleak),
from retrograde flow into the aneurysm from the inferior mesenteric artery or the lumbar arteries (type II endoleak), or from the
graft or modular junction site (type III endoleak).Type I and type
© 2007 WebMD, Inc. All rights reserved.
6 VASCULAR SYSTEM
ACS Surgery: Principles and Practice
11 REPAIR OF INFRARENAL ABDOMINAL AORTIC ANEURYSMS — 12
III endoleaks call for secondary treatment to prevent possible
aneurysm rupture.The significance of type II endoleaks is less certain. There is no clear evidence that type II endoleaks lead to
aneurysm rupture; however, most such endoleaks are treated if
they are associated with aneurysm enlargement.
Although numerous studies have shown that endovascular AAA
repair results in less morbidity and perioperative mortality than
open repair,31-34 reports describing endograft migration over time,
aneurysm enlargement, and occasional aneurysm rupture have
raised questions about the long-term durability of the procedure.35,36 These adverse events, though uncommon, serve as
reminders that EVAR is still a new technology, one whose longterm outcome is unknown. Accordingly, close patient monitoring
and follow-up surveillance are warranted, and secondary treatments may be required (e.g., additional endovascular procedures
or, possibly, open surgical repair). New endovascular devices are
currently being designed and evaluated in clinical trials, and
endovascular treatment strategies continue to evolve and improve.
Clinical follow-up of patients treated during the initial prospective clinical trials now extends to more than 7 years, and EVAR
continues to show favorable results. The largest multicenter
endovascular clinical trial to date, involving 1,193 patients who
were followed for as long as 6 years, found that prevention of
aneurysm rupture (the primary objective) was achieved in 99% of
patients, whereas procedure-, aneurysm-, or graft-related death
was avoided in 97%.37,38 These results are consistent with the
favorable overall outcomes reported from a European registry of
EVAR using a variety of endovascular devices.39 Thus, the midterm
results of EVAR are favorable and support the consideration of this
approach for most patients who are candidates for the procedure.
References
1. Taylor LM, Porter JM: Basic data related to clinical decision-making in abdominal aortic aneurysms. Ann Vasc Surg 1:502, 1980
2. Bickerstaff LK, Hollier LH, Van Peenen HJ, et
al: Abdominal aortic aneurysm: the changing
natural history. J Vasc Surg 1:6, 1984
3. Melton L, Bickerstaff L, Hollier LH, et al: Changing incidence of abdominal aortic aneurysms: a
population based study. Am J Epidemiol 120:379,
1984
4. Finlayson SRG, Birkeyer JD, Fillinger MF, et al:
Should endovascular surgery lower the threshold
for abdominal aortic aneurysms? J Vasc Surg
29:973, 1999
5. The UK Small Aneurysm Trial Participants:
Mortality results for randomized controlled trial
of early elective surgery or ultrasonographic surveillance for small abdominal aortic aneurysms.
Lancet 352:1649, 1998
6. Lederle FA, Wilson SE, Johnson GR, et al:
Immediate repair compared with surveillance of
small abdominal aortic aneurysms. N Engl J
Med 346:1437, 2002
7. The United Kingdom Small Aneurysm Trial
Participants: Long-term outcomes of immediate
repair compared with surveillance for small
abdominal aortic aneurysms. N Engl J Med
346:1445, 2002
8. Lederle FA, Johnson GR, Wilson SE, et al: Rupture rate of large abdominal aortic aneurysms in
patients refusing or unfit for elective repair. JAMA
287:2968, 2002
9. Darling RC, Messina CR, Brewster DC, et al:
Autopsy study of unoperated aortic aneurysms.
Circulation 56(suppl 2):161, 1977
10. Thurmond AS, Semler JH: Abdominal aortic
aneurysm: incidence in a population at risk. J
Cardiovasc Surg 27:457, 1986
11. McFalls EO, Ward HB, Moritz TE, et al: Coronary-artery revascularization before elective major
vascular surgery. N Engl J Med 351:2795, 2004
ity and criteria of operability. Arch Surg
107:297, 1973
endovascular repair of open abdominal aortic
aneurysms. N Engl J Med 351:1607, 2004
15. Quill DS, Colgan MP, Summer DS: Ultrasonic
screening for the detection of abdominal aortic
aneurysms. Surg Clin North Am 69:713, 1989
30. EVAR trial participants. Endovascular aneurysm
repair versus open repair in patients with
abdominal aortic aneurysm (EVAR trial 1): randomised controlled trial. Lancet 365:2179, 2005
16. Bluth EI: Ultrasound of the abdominal aorta.
Arch Intern Med 144:377, 1994
17. Gomes MN, Choyke PL: Preoperative evaluation of abdominal aortic aneurysms: ultrasound
or computed tomography? J Cardiovasc Surg
28:159, 1987
18. Amparo EG, Hoddick WK, Hricak H, et al:
Comparison of magnetic resonance imaging and
ultrasonography in the evaluation of abdominal
aortic aneurysms. Radiology 154:451, 1985
19. Lee JKT, Ling D, Heiken JP, et al: Magnetic resonance imaging of abdominal aneurysms. Am J
Roentgenol 143:1197, 1984
20. Papin E: Chirurgie du rein. Anomalies du rein.
Paris, G. Doin, 1928, p 205
21. Zarins CK, Gewertz BL: Atlas of Vascular Surgery.
New York, Churchill Livingstone, 1988, p 56
22. Trigaux JP, Vandroogenbroek S, De Wispelaere
JF, et al: Congenital anomalies of the inferior
vena cava and left renal vein: evaluation with spiral CT. J Vasc Interv Radiol 9:339, 1998
23. Crawford JL, Stowe CL, Safi HJ, et al: Inflammatory aneurysms of the aorta. J Vasc Surg 2:133,
1985
24. Crawford ES, Saleh SA, Babb JW 3rd, et al:
Infrarenal abdominal aortic aneurysm: factors
influencing survival after operation performed
over a 25-year period. Ann Surg 193:699, 1981
25. Zarins CK, White RA, Schwarten D, et al:
AneuRx stent graft vs. open surgical repair of
abdominal aortic aneurysm: multicenter
prospective clinical trial. J Vasc Surg 29:292,
1999
26. Makaroun MS: The Ancure endografting system: an update. J Vasc Surg 33:S129, 2001
12. Whittemore AD, Clowes AW, Hechtman HB, et
al: Aortic aneurysm repair reduced operative
mortality associated with maintenance of optimal cardiac performance. Ann Surg 120:414,
1980
27. Nonruptured abdominal aortic aneurysm: sixyear follow-up results from the multicenter
prospective Canadian aneurysm study. Canadian
Society for Vascular Surgery Aneurysm Study
Group. J Vasc Surg 20:163, 1994
13. Pairolero PC: Repair of abdominal aortic
aneurysms in high-risk patients. Surg Clin North
Am 69:755, 1989
28. Zarins CK, Harris EJ: Operative repair of aortic
aneurysms: the gold standard. J Endovasc Surg
4:232, 1997
14. Stokes J, Butcher HR: Abdominal aortic
aneurysms: factors influencing operative mortal-
29. Prinssen M,Verhoeven ELG, Buth J, et al: A randomized trial comparing conventional and
31. Arko FR, Lee WA, Hill BB, et al: Aneurysmrelated death: primary endpoint analysis for
comparison of open and endovascular repair. J
Vasc Surg 36:297, 2002
32. Moore WS, Kashyap VS, Vescera CL, et al:
Abdominal aortic aneurysm: a 6 year comparison of endovascular versus transabdominal
repair. Ann Surg 230:298, 1999
33. Adriansen MEAPM, Bosch JL, Halpern EF, et
al: Elective endovascular versus open surgical
repair of abdominal aortic aneurysms: systematic review of short-term results. Radiology
224:739, 2002
34. Arko FR, Hill BB, Olcott C, et al: Endovascular
repair reduces early and late morbidity compared to open surgery for abdominal aortic
aneurysm. J Endovasc Ther 9:711, 2002
35. Cao P, Verzini F, Zannetti S, et al: Device migration after endoluminal abdominal aortic
aneurysm repair: analysis of 113 cases with a
minimum follow-up period of 2 years. J Vasc
Surg 35:229, 2002
36. Torsello GB, Klenk E, Kasprzak B, et al:
Rupture of abdominal aortic aneurysm previously treated by endovascular stent graft. J Vasc Surg
28:184, 1998
37. Zarins CK, White RA, Moll FL, et al: The
AneuRx stent graft: four-year results and worldwide experience 2000. J Vasc Surg 33:S135,
2001
38. The U.S. AneuRx Clinical Trial: 6-year clinical
update 2002. AneuRx Clinical Investigators. J
Vasc Surg 37:904, 2003
39. Harris PL, Vallabhaneni SR, Desgranges P, et al:
Incidence and risk factors of late rupture, conversion, and death after endovascular repair of
infrarenal aneurysms: the Eurostar experience. J
Vasc Surg 32:739, 2000
Acknowledgment
Figures 4 through 11 Susan Brust, C.M.I.