Application for Disabled Person Placard or plates
advertisement

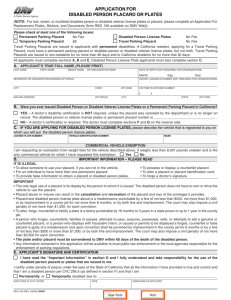
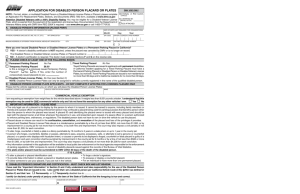
A Public Service Agency APPLICATION FOR DISAbLED PERSON PLACARD OR PLATES (NOTE: Forlost,stolen,ormutilateddisabledpersonordisabledveteranlicenseplatesorplacard,pleasecompleteanApplicationFor ReplacementPlates,Stickers,andDocuments[formREG156availableonDmVWeb]). Please check at least one of the following boxes: DisabledPersonLicensePlates No Fee No Fee NOTE:DisabledPersonlicenseplatescanonlybeassignedtovehicles currentlyregisteredinthenameofthequalifieddisabledperson. TemporaryParkingPlacard $6 TravelParkingPlacard No Fee TravelParkingPlacardsareissuedtoapplicantswithpermanentdisabilities.ACaliforniaresident,applyingforaTravelParkingPlacard, musthaveapermanentparkingplacardordisabledpersonordisabledveteranlicenseplates,butnotboth.TravelParkingPlacardsare issuedtonon-residentsfornomorethan90daysandtoCaliforniaresidentsfornomorethat30days. PermanentParkingPlacard AllapplicantsmustcompletesectionsA, bandE.DisabledPersonLicensePlateapplicantsmustalsocompletesectionC. A. APPLICANT’S TRuE FuLL NAME(PLEASE PRINT) LASTNAmE FIRSTNAmE mIDDLENAmE ORORGANIzATIONNAmE DATEOFbIRTh(NOTREqUIREDFORORGANIzATIONS) RESIDENCEORORGANIzATIONADDRESSAPT/SPACE DRIVERLICENSE/IDNUmbER(NOTREqUIREDFORORGANIzATIONS) CITY STATE zIPCODE DAYTImETELEPhONENUmbER mAILINGADDRESS APT/SPACE CITY month Day Year ( ) STATE zIPCODE b. WereyoueverissuedDisabledPersonorDisabledVeteranLicensePlatesoraPermanentParkingPlacardinCalifornia? yES –A doctor’s disability certification is NOT required, unless the placard was canceled by the department or is no longer on record.Thedisabledpersonorveteranlicenseplatesorpermanentplacardnumberis________________________________. NO –Adoctor’scertificationisrequired.ThedoctormustcompletesectionsF andGonthereverseside. C. IF yOu ARE APPLyING FOR DISAbLED PERSON LICENSE PLATES,pleasedescribethevehiclethatisregisteredtoyouon whichyouwillputthedisabledpersonlicenseplates: LICENSEPLATENUmbER VEhICLEIDENTIFICATIONNUmbER mAkE CoMMerCIaLVehICLeexeMPTIon Iamrequestinganexemptionfromweightfeesforthevehicledescribedabove.Itweighslessthan8,001poundsunladenandistheonly commercialvehicleforwhichIhaverequestedthisexemption. Yes No D. IMPORTANT INFORMATION – PLEASE READ IT IS ILLEGAL •Toallowsomeonetouseyourplacard,ifyouarenotinthevehicle. •Topossessordisplayacounterfeitplacard. •Foranindividualtohavemorethanonepermanentplacard. •Toalteraplacardorplacardidentificationcard. •Toprovidefalseinformationtoobtainaplacardordisabledpersonplates. •Toforgeadoctor’ssignature. IMPORTANT •Theonlylegaluseofaplacardisitsdisplaybythepersontowhomitisissued.Thedisabledpersondoesnothavetoownordrivethe vehicletousetheplacard. •Placardabuseormisusecanresultinthecancellation andrevocation oftheplacardandlossoftheprivilegesitprovides. •Placardanddisabledpersonlicenseplateabuseisamisdemeanorpunishablebyafineofnotlessthan$250,notmorethan$1,000,or byimprisonmentinacountyjailfornotmorethan6months,orbybothfineandimprisonment.Thecourtmayalsoimposeacivilpenalty ofnotmorethan$1,500,foreachconviction. •Toalter,forge,counterfeitorfalsifyaplateisafelonypunishableby16monthsto3yearsinastateprisonorupto1yearinthecountyjail. •Apersonwhoforges,counterfeits,falsifiesorpasses,attemptstopass,acquires,possesses,sells,orattemptstosellagenuineor counterfeitplacard,orapersonwhodisplayswithfraudulentintent,orcausesorpermitstobedisplayedaforged,counterfeitorfalse placardisguiltyofamisdemeanoranduponconvictionshallbepunishedbyimprisonmentinthecountyjailfor6monthsorbyafineof notlessthan$500ormorethan$1,000,orbybothfineandimprisonment.Thecourtmayalsoimposeacivilpenaltyofnotmorethan $3,500foreachconviction. •Theplateand/orplacardmustbesurrenderedtoDMVwithin60daysofthedeathofthedisabledperson. •Anyinformationcontainedinthisapplicationwillbeavailabletolocalpubliclawenforcementorthelocalagenciesresponsibleforthe enforcementofparkingregulations. E. APPLICANT’S SIGNATuRE AND CERTIFICATION I have read the “Important Information” in section D and I fully understand and take responsibility for the use of the disabledpersonplacardorplatesthatareissuedtome. Icertify(ordeclare)underpenaltyofperjuryunderthelawsoftheStateofCaliforniathatalltheforegoingistrueandcorrect.Ialsocertify thatIamadisabledpersonperCVC295.5(asdefinedinsectionF)andthatIam Permanently or Temporarilydisableddueto:_____________________________________________________________. EXECUTEDAT(CITY,STATE) REG195(REV.8/2008) WWW DATE SIGNATUREOFAPPLICANT Clear Form Print F. DOCTOR’S CERTIFICATION OF DISAbILITy Afulllegibledescriptionoftheillnessordisabilitymustbeprovidedfornumbers3,4,5,6and7below.Alicensedphysician,surgeon, physician’sassistant,nursepractitioner,orcertifiednursemidwife,maycertifytoitems1–7,alicensedchiropractormaycertifytoitems 5–7only,andalicensedphysicianorsurgeonwhospecializesindiseasesoftheeyeoralicensedoptometristmayonlycertifytoitem8. mypatient___________________________________________meetstherequirementsofadisabledpersonfoundinCVC295.5ashe (PRINTEDNAmEOFPATIENT) orshesuffersfromthefollowing: 1. A lung disease to the extent that forced (respiratory) expiratory volume for one second when measured by spirometry is less thanoneliteror arterialoxygentension(pO2)islessthan60mm/hgonroomairwhilethepersonisatrest. 2. A cardiovascular disease to the extent that the person’s functional limitations are classified in severity as class III or class IV baseduponstandardsacceptedbytheAmericanheartAssociation. 3. Adiagnoseddiseaseordisorderwhichsubstantiallyimpairsorinterfereswithmobilitydueto(please print): Aseveredisabilityinwhichheorsheisunabletomovewithouttheaidofanassistivedevice,whichisdueto(please print): 4. ___________________________________________________________________________________________________. ___________________________________________________________________________________________________. 5. Asignificantlimitationintheuseoflowerextremitiesdueto(please print): ___________________________________________________________________________________________________. 6. Theloss,orlossoftheuseofoneormorelowerextremities.Lossofusedueto(please print): ___________________________________________________________________________________________________. 7. Theloss,orlossoftheuseof,bothhands.Lossofusedueto(please print): ___________________________________________________________________________________________________. 8. Centralvisualacuitydoesnotexceed20/200inthebettereye,withcorrectivelenses,asmeasuredbytheSnellentest,orvisual acuity that is greater than 20/200, but with a limitation in the field of vision such that the widest diameter of the visual field subtendsananglenotgreaterthan20degrees. Please check the appropriate box(es). PERMANENT PLACARD TEMPORARy PLACARD Validuntil:month____Day____Year_____ (Cannotexceed6months) G. aUThorIZeDMeDICaLProVIDer’SSIGnaTUreanDCerTIFICaTIon PRINTAUThORIzEDmEDICALPROVIDER’SLASTNAmEFIRSTNAmEmIDDLENAmE AUThORIzEDmEDICALPROVIDER’SADDRESS CITY TraVeLPLaCarD Validuntil:month____Day____Year_____ (Cannotexceed30daysforaCalifornia residentand90daysforanon-resident.) AUThORIzEDmEDICALPROVIDER’SDAYTImETELEPhONE# ( ) STATEzIPCODE I certify that I am a Physician Surgeon Chiropractor optometrist Physician’s assistant nurse Practitioner CertifiednurseMidwifeandIcertify(ordeclare)underpenaltyofperjuryunderthelawsoftheStateofCaliforniathat theforegoingistrueandcorrect.IalsocertifythatIwillretaininformationsufficienttosubstantiatethiscertificationandshallmakethat informationavailableforinspectionbythemedicalboardofCaliforniaatthedepartment’srequest.(CVCSection22511.55). EXECUTEDAT(CITY,STATE) DATE AUThORIzEDmEDICALPROVIDER’SSIGNATURE MEDICAL LICENSE NuMbER h. CerTIFICaTIonoFreaDILYoBSerVaBLeanDUnConTeSTeDPerManenTDISaBILITY(DMV USE ONLY) SIGNATUREOFDmVEmPLOYEE Whenthisformiscompleted,itmaybemailedto: LINEDATESTAmP DmVPlacard P.O.box942869 Sacramento,CA94269-0001 or submitted to your nearest DmV office. It is recommended that you make an appointment if submitting this form to your nearest DmVoffice,bycalling1-800-777-0133. REG195(REV.8/2008) WWW