Clinical Examination of Respiratory System by Dr. Shahab
advertisement

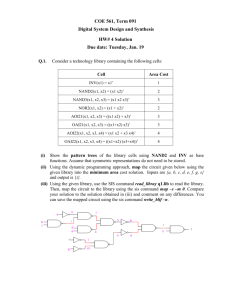
NOTES IN RESPIRATORY SYSTEM EXAMINATION BY DR. SHAHAB SHAIKH Examination of the Respiratory System Inspection: Co mf o rta b le a t re st . . . . ? B re a t h le ss . . . .? Cya n o sis . . . . . ? , 1 . Che s t w a l l a ppea ra nc e: a . S ha pe No rm a lly E llip so id B a rre l Ch e st - Hyp e re xp a n sio n (A -P d ia me t e r in crea sed ) e g. CO P D b. S ymme tr y c . S c a rs / Les i ons d. De formi t y: P e c tus c a ri na tum – st e rnu m b u lge s f o rwa rd s (‘p ige o n ch e st d ef o rm it y’) P e c tus e x ca va tu m – st e rnu m ca ve s in wa rd s (Fu n n e l ch e st d ef o rm it y) P e c tus c a ri na tum P e c tus e x ca va tu m K yphos i s is a n e xa gge ra t e d an t e rio r cu rva t u re of t h e sp in e S c ol i osi s is an e xa gge ra t e d la te ra l cu rva t u re of th e sp in e 2 . Che s t w a l l move me nt : a . E x pa ns i on b. S ymme tr y of mo ve me nt c . P a ra doxi c al move me nt : Ph re n ic ne rve p a ra lysis, Fla il ch e st 3 . Br e a thi ng: a . Re s pi ra tor y ra te : RR co u n t ed af t e r dive rt in g a t t e n t io n as if p re t en d in g to t a ke Pu lse T a ch yp n o ea is a re sp ira t o ry ra t e > 15 / m in a nd is cau sed b y in cre a se d ve n t ila t o ry d rive a s in f eve r, a st h ma an d CO P D, o r re d u ced ve n t ila t o ry ca p a cit y a s in p ne u mo n ia, pu lm on ary o e de ma an d int e rst it ia l lu n g d ise a se . A slo w re sp ira t o ry ra t e can o ccu r in asso cia t io n wit h o p io id t o xicit y, h yp o t h yro id ism , ra ised in t ra cra n ia l p re ssu re , h yp o t h a lam ic le sion s, an d h yp e rca p nia . b. Re s pi ra tor y de pt h c . Re s pi ra tor y Rh yt hm d. T ype of re s pi ra ti on: Norma l Kus s a mul: Hyp e rve n t ila t ion wit h d e ep , sigh in g re sp ira t io n s (Kü ssm a u l re sp ira t ion ) is a re spo n se t o t he re d u ce d a rt e ria l p H in m et ab o lic a cid o sis. T h is ca n o ccu r in a cut e re na l f a ilu re , la ct ic a cido sis, d iab e t ic ket oa cid o sis an d in sa li cyla t e a n d m et h an o l p o iso n in g. T h e p at ie n ts a p pe a r to ha ve 'a ir h u n ge r'. Che yne s trok e : Ch e yn e -S t o ke s b reat h in g, o r pe rio d ic re sp ira t io n , is ch a ra ct e rize d b y a p e rio d of in cre a sin g ra t e an d d e p th of b rea t h in g f o llo we d b y d im in ish in g re sp ira t o ry e f f o rt an d ra t e , u su a lly e n d ing in a p e riod of a pn o ea o r h yp op n oea . T h e cycle t h e n re pe a t s. Th is p at t e rn of b re a t h in g re la t e s to a n a lt e re d se n sit ivit y of t he re sp irat o ry ce n t re to chem ica l co n t ro l a n d d e la y in circu la t io n t im e b et we e n t h e lu n g a nd ch e mo re cep t o rs. I t is se e n mo st f re qu e n t ly in st ro ke invo l vin g t h e b ra in ste m, a nd in se ve re ca rd iac f a ilu re . Ho we ve r, it m a y b e n o rma l d u rin g sle ep in th e e ld e rly. e . Us e of a cc e ss or y mus c l es : T h e se inclu d e th e st e rn o cle ido ma st o id s, p lat ysm a an d pe ct o ra l m u scle s . Use of a cce s so ry m u scle s is ch a ra cte rist ic of p a t ie n t s wit h COP D wh o h a ve h yp e rinf la t ed lu n gs. 5 . Ne c k re gi on: a . P os i ti on of Tra c he a Ca us e s of trac hea l de vi a ti on Tow a rds the s i de of the l ung l e s i on Up p e r lo be o r lun g co lla p se Up p e r lo be f ib ro sis P n e umo n e ctom y Aw a y from the s i de of the l ung l esi on T en sio n p ne um o tho ra x Ma ssive p le u ra l ef f u sio n b. S upra c la vi c ul a r fos s a e c . V i s i ble pul sa ti on , J V P d. L ymph node s PALPATION: 1 . Te nde rne ss 2 . Te m pe ra ture 3 . P os i ti on of Tra c he a : Use on e o r t wo f in ge rs in sup ra st e rn a l no t ch ! 4 . Che s t E x pa ns i on: B o t h sid e s of th e th o ra x sh o u ld e xp an d e qu a lly d u rin g tid a l a nd m a xim a l in sp irat ion . Re d u ced e xp a n sion o n o ne sid e in d ica t e s a b no rm a lit y o n th a t sid e , e . g. p le u ra l ef f u sion , lu n g o r lob a r co lla p se , p n eum o th o ra x a n d u n ila t e ra l f ib ro sis. B ila t e ra l re du ct io n in ch e st wa ll m o ve m en t is co mm on in a d va n ced CO P D a n d d if f u se p u lmo n a ry f ib ro sis 5 . Ta c ti l e V oc al Fremi tus : T a ct ile vo ca l f re m it u s is t he t ran sm issio n of vo ice so u nd s f rom ce n t ra l a irwa ys t o t h e ch e st wa ll. I t is in cre a sed b y so lid lu n g, p ro vid e d t he a irwa ys su p p lyin g t h a t pa rt of t h e lu n g a re p a t en t . I t is im po rt an t to de cid e wh e t he r a rea s f ou n d t o b e d u ll t o p e rcu ssio n sh o w in cre a sed t a ct ile vo ca l f rem it u s (su gge st in g co n so lid at io n o r f ib ro sis) o r re d u ce d t a ct ile vo ca l f rem it u s (su gge st in g f lu id or co lla p se ) Du rin g a sse ssm ent of ta ct ile vo ca l f re m it u s, it is con ve n t io na l t o a sk t he pa t ie nt t o sa y 'n in e t y -n in e '. I n o th e r lan gu a ge s, o t he r n u mb e rs o r p h ra ses a re u se d . (T he in t e nt io n is t o p ro du ce a n a sa l 'o i' so u nd ). 6 . Ap e x be a t l oc a li za ti on : De via t io n of th e card ia c a pe x b e a t ind ica t e s sh if t of th e lo we r m e d ia st in um . Disp la ce me n t of the ca rd ia c im pu lse wit h o u t d e via t io n of t h e t ra ch e a is u sua lly d u e t o lef t ve n t ricula r e n la rge me n t b ut ca n a lso o ccu r in sco lio sis, kyp h o sco lio sis, o r se ve re p e c t u s e xca va t u m . T he ca rd ia c a pe x b e a t ma y b e d if f icu lt t o lo ca lize in ob e sit y, p e rica rd ia l ef f u sion , po o r lef t ve n t ricu la r f u n ct io n o r p at ie n t s wit h lu n g h yp e rin f la t io n a s in CO P D. Percussion: I d e a l site s f o r p e rcu ssio n a re a s sh own b e lo w The sounds heard in different condition are as mentioned: Type Condition R es onant Norm al l ung H yp err esonant P neum ot horax P ul m onar y consol i d at i on Dul l P ul m onar y col l aps e S evere pul m onar y fi brosi s 'S t on y dul l ' P l eural effusi on Auscultation: T he st et h o sco pe wa s in ve n t e d b y a Fre n ch ph ysicia n , La e nne c, in 1 8 19 . A u scu lt at e b o th sid e s a lte rn a te ly, co m p a rin g f ind in gs ove r a la rge n u mb e r of e qu iva le n t p o sit io n s t o e nsu re t ha t lo ca lize d a b no rma lit ie s a re n ot m isse d . T yp e s of so un d s on e m a y b e e xp e ct ed t o h ea r: Re s pi r a tor y (nor ma l ) s ounds o V e s ic ul a r s ounds o Bronc hi a l s ounds A )-Vesicular sounds Lower pitched, rustling Softer relatively Inspiration longer & Expiration shorter No Gap between Insp & Exp sounds Normally heard in lung parenchymal region (peripheral thorax) B )- Bronchial sounds Higher pitched, hollow or blowing quality Louder relatively Inspiration & Expiration equal Gap present between Insp & Exp sounds Normally heard only along tracheobronchial tree (central thorax) B ro n ch ia l so u nd s c a n be f o u nd in p erip h e ra l re gio n wh e n e ve r n o rm a l lu ng t issu e is re p la ce d b y u n if o rm ly co n duct in g t issu e , wh e t he r t h ro u gh c ons ol i da ti on , fi bros i s o r c ol la ps e . Ad ve nti ti ous ( Add e d) s ounds : Wheezes / Rhonchi Musical sounds produced by air passing through narrowed airways. e.g. asthma. Non-musical sounds mainly heard during inspiration caused by: 1) Reopening of occluded small airways. e.g. Crackles (Crepititions) fibrosing alveolitis and pulmonary edema 2) Air bubbling through secretions. e.g. bronchiectasis Leathery or creaking sounds produced by movement of roughened pleural surfaces. E.g. pleurisy caused by Pleural Friction rub pneumonia, pulmonary infarction. Usually associated with pleural pain. voc a l r e s ona nc e : Fin a lly, a sse ss vo ca l re so na n ce b y askin g t h e pa t ie nt to sa y 'o n e , on e , o ne '. I n th e n o rm a l lu ng a wh isp e re d n ote will n o t b e he a rd b u t o ve r co n so lid at e d lun g, a s in p neu m on ia , t h e so un d is t ra n sm it t ed p ro d u cin g 'w hi s peri ng pe c tori l oqu y' . SPIROMETRY: • Ba s i c s pi rome tr y te rmi nol og y 1 . Ti da l vol ume (TV ): vo lu me of a ir in ha le d o r e xh a le d in o n e n o rm a l b re a t h. 2 . I ns pi ra tor y re s e rve vol ume (I RV ): m a xim a l am ou n t of a ir t h a t ca n be in ha le d f o llo win g a n o rm a l inha la t io n. 3 . E x pi ra tor y re s e rve vol ume (E RV ): m a xim a l vo lu m e of a ir t h a t ca n be e xh a led f o llo win g a n o rma l e xh a la t ion . 4 . I ns pi ra tor y Ca pa c i t y (I C): m a xim a l am o un t of a ir a su b je ct can in h a le f o llo win g a n o rma l e xh a la t ion . 5 . V i ta l ca pa ci t y (V C ): ma xim a l am o un t of a ir th a t a sub ject ca n e xh a le af te r a m a xim a l in ha la t ion . 6 . Re s i dua l vol ume (RV ): vo lu m e of a ir re m a in in g in lu n gs af t e r m a xim a l e xh a la t ion . 7 . Func ti ona l re si dua l ca pa c i ty (FRC) : vo lu me of a ir lef t in lu n gs af t e r a n o rm a l e xh a la t io n. 8 . Tota l l ung c a pa c it y (TLC ): t o t a l vo lu m e of a ir t he lu n gs ca n h o ld . NO RM AL R ANG E : VARIOUS RESPIRATORY SIGNS & UNDERLYING PATHOLOGY Shape of the Chest Symmetry of the Chest Respiratory rate Mode of Breathing Trachea Reduced Chest Expansion Breathing Sounds Vocal Resonance Pigeon-shaped Barrel-shaped Asthma in childhood Rickets Emphysema Forward Bending Lateral Bending Kyphosis Scoliosis Increased Decreased Fever Acute Pulmonary Infections Pleural Pain Bronchial Asthma Pulmonary Edema Repiratory Failure Thoracic Abdominic Abdominal pain Ascites Gaseous Distension of the Intestines Large Ovarian Cyst Pregnancy Ankylosing Spondylitis Pleural Pain Intercostal Paralysis Pushed Pulled Pleural Effusion Pneumothorax Supramediastinal Mass Pulmonary Consolidation Lung Collapse Pulmonary fibrosis Bilateral Unilateral Bronchial Asthma Emphysema Pulmonary fibrosis Pleural Effusion Pleural thickening & fibrosis Pulmonary Collapse Pulmonary Consolidation Pneumothorax Diminished Vesicular Bronchial Breathing Emphysema Pleural effusion/thickening Thick Chest wall Pneumothorax Lung Collapse when large bronchi occluded Pulmonary Consolidation Large Superficial Lung Cavity Pulmonary Fibrosis Lung Collapse when large bronchi patent Increased Decreased Pulmonary Consolidation Lung Collapse when large bronchi patent Pleural Effusion Pneumothorax Lung Collapse when large bronchi occluded